
Impact of Cardiovascular–Kidney–Metabolic Syndrome Staging on Myocardial Infarction Outcomes: A Retrospective Analysis of 2.7 Million Patients
 , , and
, , and 
Abstract
1. Introduction
2. Methods
2.1. Data Source
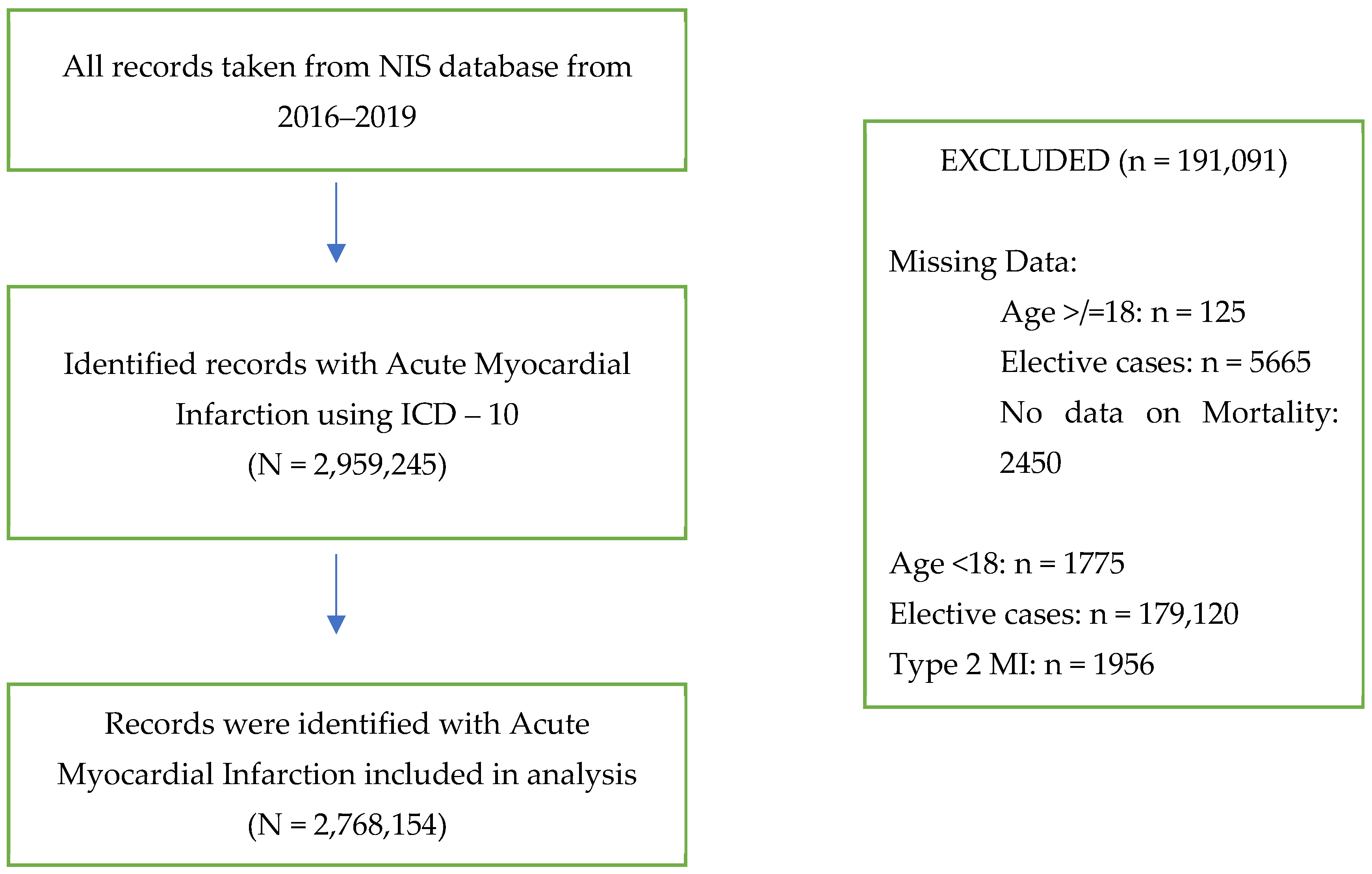
2.2. Study Design and Population
2.3. Outcomes
2.4. Statistical Analysis
3. Results
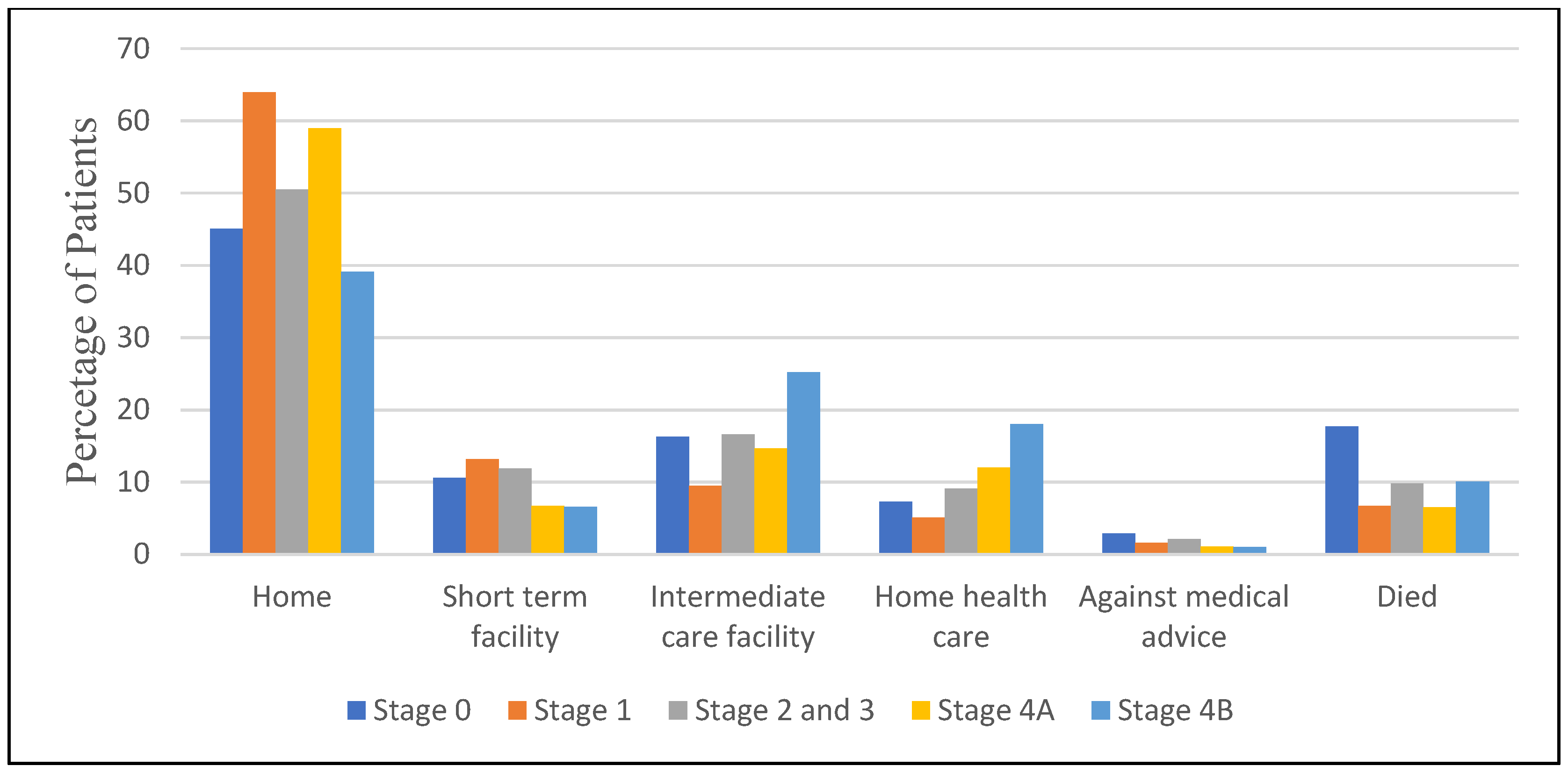
3.1. In-Hospital Procedures and Outcomes
Crude Rates
3.2. Adjusted Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mechanic, O.J.; Gavin, M.; Grossman, S.A. Acute Myocardial Infarction. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar] [PubMed]
- Ndumele, C.E.; Rangaswami, J.; Chow, S.L.; Neeland, I.J.; Tuttle, K.R.; Khan, S.S.; Coresh, J.; Mathew, R.O.; Baker-Smith, C.M.; Carnethon, M.R.; et al. Cardiovascular-Kidney-Metabolic Health: A Presidential Advisory from the American Heart Association. Circulation 2023, 148, 1606–1635, Erratum in Circulation 2024, 149, e1023. [Google Scholar] [CrossRef] [PubMed]
- Minhas, A.M.K.; Mathew, R.O.; Sperling, L.S.; Nambi, V.; Virani, S.S.; Navaneethan, S.D.; Shapiro, M.D.; Abramov, D. Prevalence of the Cardiovascular-Kidney-Metabolic Syndrome in the United States. J. Am. Coll. Cardiol. 2024, 83, 1824–1826. [Google Scholar] [CrossRef] [PubMed]
- HCUP, National Inpatient Sample (NIS), Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality, Rockville, MD. 2012. Available online: www.hcup-us.ahrq.gov/nisoverview.jsp (accessed on 1 December 2024).
- Francula-Zaninovic, S.; Nola, I.A. Management of Measurable Variable Cardiovascular Disease’ Risk Factors. Curr. Cardiol. Rev. 2018, 14, 153–163. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rus, M.; Crisan, S.; Andronie-Cioara, F.L.; Indries, M.; Marian, P.; Pobirci, O.L.; Ardelean, A.I. Prevalence and Risk Factors of Metabolic Syndrome: A Prospective Study on Cardiovascular Health. Medicina 2023, 59, 1711. [Google Scholar] [CrossRef] [PubMed]
- Abramov, D.; Kobo, O.; Mohamed, M.; Roguin, A.; Osman, M.; Patel, B.; Parwani, P.; Alraies, C.; Sauer, A.J.; Van Spall, H.G.C.; et al. Management and outcomes of acute myocardial infarction in patients with preexisting heart failure: An analysis of 2 million patients from the national inpatient sample. Expert. Rev. Cardiovasc. Ther. 2022, 20, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Bucholz, E.M.; Rathore, S.S.; Reid, K.J.; Jones, P.G.; Chan, P.S.; Rich, M.W.; Spertus, J.A.; Krumholz, H.M. Body mass index and mortality in acute myocardial infarction patients. Am. J. Med. 2012, 125, 796–803. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Keller, K.; Münzel, T.; Ostad, M.A. Sex-specific differences in mortality and the obesity paradox of patients with myocardial infarction ages >70 y. Nutrition 2018, 46, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Figtree, G.A.; Vernon, S.T.; Hadziosmanovic, N.; Sundström, J.; Alfredsson, J.; Arnott, C.; Delatour, V.; Leósdóttir, M.; Hagström, E. Mortality in STEMI patients without standard modifiable risk factors: A sex-disaggregated analysis of SWEDEHEART registry data. Lancet 2021, 397, 1085–1094, Erratum in Lancet 2021, 397, 1182. [Google Scholar] [CrossRef] [PubMed]
- Bharadwaj, A.; Potts, J.; Mohamed, M.O.; Parwani, P.; Swamy, P.; Lopez-Mattei, J.C.; Rashid, M.; Kwok, C.S.; Fischman, D.L.; Vassiliou, V.S.; et al. Acute myocardial infarction treatments and outcomes in 6.5 million patients with a current or historical diagnosis of cancer in the USA. Eur. Heart J. 2020, 41, 2183–2193. [Google Scholar] [CrossRef] [PubMed]
- Kobo, O.; Moledina, S.M.; Raisi-Estabragh, Z.; Shanmuganathan, J.W.D.; Chieffo, A.; Al Ayoubi, F.; Alraies, M.C.; Biondi-Zoccai, G.; Elgendy, I.Y.; Mohamed, M.O.; et al. Emergency department cardiovascular disease encounters and associated mortality in patients with cancer: A study of 20.6 million records from the USA. Int. J. Cardiol. 2022, 363, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Sedhom, R.; Mohammad, A.; Khedr, M.; Megaly, M.; Waldman, C.; Bharadwaj, A.S.; Kobo, O.; Sayed, A.; Abramov, D. Characteristics and outcomes of myocardial infarction among patients with bleeding or hypercoagulable disorders: A nationwide analysis. Cardiovasc. Revasc. Med. 2024. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Sedhom, R.; Khedr, M.; Beshai, R.; Brilakis, E.S.; Basir, M.B.; Alaswad, K.; Stoletniy, L.; Abramov, D.; Bharadwaj, A.; Megaly, M. Characteristics and outcomes of myocardial infarction among burn patients: A nationwide analysis. Burns 2025, 51, 107313. [Google Scholar] [CrossRef] [PubMed]
- Kobo, O.; Leiba, R.; Avizohar, O.; Karban, A. Relative fat mass (RFM) as abdominal obesity criterion for metabolic syndrome. Eur. J. Intern. Med. 2019, 63, e9–e11. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| CKM Stage | ||||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 and 3 | 4A | 4B | p-Value | |
| NIS discharge weight | 68,680 | 33,095 | 255,570 | 1,695,070 | 715,145 | |
| Mean age | 58.9 | 56.7 | 66.2 | 67.2 | 73.1 | <0.001 |
| Female, % | 45.3% | 52% | 50.30% | 39.4% | 40.6% | <0.001 |
| Ethnicity | <0.001 | |||||
| White | 75.1% | 70% | 67.6% | 77.3% | 69% | |
| Black | 11.4% | 16.1% | 16.6% | 10.2% | 16.5% | |
| Hispanic | 7.9% | 9% | 9.5% | 7% | 8.3% | |
| Asian | 2.3% | 1.7% | 3.1% | 2.2% | 3.2% | |
| Native | 0.6% | 0.4% | 0.5% | 0.5% | 0.5% | |
| Other | 2.8% | 2.80% | 2.90% | 2.80% | 2.5% | |
| Hospital region | <0.001 | |||||
| Northeast | 24.1% | 22.2% | 22.4% | 20.5% | 20.6% | |
| Midwest or North Central | 20.6% | 23.9% | 22% | 24.5% | 24.6% | |
| South | 39% | 37% | 39.7% | 40.6% | 39.9% | |
| West | 16.3% | 16.80% | 15.90% | 14.4% | 14.9% | |
| Hospital bed size | <0.001 | |||||
| Small | 19.5% | 20.5% | 20.7% | 16.6% | 17.6% | |
| Medium | 29.4% | 30% | 31.2% | 29.8% | 30.1% | |
| Large | 51.1% | 49.5% | 48% | 53.7% | 52.3% | |
| Hospital location/teaching status | <0.001 | |||||
| Rural | 10.3% | 8.4% | 8% | 8.3% | 8.3% | |
| Urban non-teaching | 25.6% | 25.4% | 23.9% | 23.5% | 23.5% | |
| Teaching | 64.1% | 66.1% | 68.1% | 68.2% | 68.2% | |
| Median ZIP income | <0.001 | |||||
| 1st quartile | 31.9% | 30.8% | 33.2% | 30.5% | 32.4% | |
| 2nd quartile | 27.6% | 26.7% | 26.9% | 27.8% | 27.2% | |
| 3rd quartile | 22.4% | 24.4% | 22.3% | 23.5% | 23% | |
| 4th quartile | 18% | 18.2% | 17.5% | 18.3% | 17.3% | |
| Primary expected payer | <0.001 | |||||
| Medicare | 40.4% | 33% | 56% | 57.6% | 79.5% | |
| Medicaid | 18.1% | 15.9% | 12.2% | 9.6% | 6.4% | |
| Private insurance | 29.5% | 41.1% | 24% | 25.1% | 10.6% | |
| Self-pay | 7.9% | 6.4% | 4.7% | 4.6% | 1.5% | |
| No charge | 0.6% | 0.7% | 0.5% | 0.4% | 0.1% | |
| Other | 3.5% | 2.9% | 2.% | 2.7% | 1.9% | |
| Record characteristics | ||||||
| STEMI | 21.6% | 18.2% | 17.9% | 26.4% | 11.7% | <0.001 |
| NSTEMI | 78.4% | 81.8% | 82.1% | 73.6% | 88.3% | <0.001 |
| Cardiac arrest | 7.80% | 3.9% | 4.4% | 3.6% | 4.1% | <0.001 |
| Ventricular fibrillation | 3.70% | 2.4% | 1.7% | 3.3% | 1.9% | <0.001 |
| Ventricular tachycardia | 4.50% | 4.1% | 3.3% | 7% | 6.7% | <0.001 |
| Comorbidities | ||||||
| Valvular heart disease | 4.9% | 5% | 6.9% | 13.4% | 20.9% | <0.001 |
| Smoking | 39.7% | 46.3% | 40.8% | 49.9% | 39.4% | <0.001 |
| Dementia | 6.8% | 2.5% | 10.2% | 6.5% | 10.4% | <0.001 |
| Anemia | 22.2% | 16.3% | 23.8% | 21.1% | 48.8% | <0.001 |
| Thrombocytopenia | 8.3% | 5.5% | 6.2% | 5.7% | 9.1% | <0.001 |
| Coagulopathy | 6.2% | 3.2% | 3.0% | 2.1% | 3.0% | <0.001 |
| Chronic liver disease | 1.1% | 0.8% | 1.1% | 0.7% | 1.2% | <0.001 |
| Intracerebral hemorrhage | 1.8% | 1.1% | 1.2% | 0.6% | 0.5% | <0.001 |
| Hematologic malignancy | 2.0% | 1.2% | 1.6% | 1.2% | 1.9% | <0.001 |
| Solid malignancy | 7.3% | 3.3% | 4.9% | 3.0% | 3.3% | <0.001 |
| Metastatic malignancy | 5.4% | 2% | 3% | 1.4% | 1.3% | <0.001 |
| CKM Stage | ||||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 and 3 | 4A | 4B | p-Value | |
| NIS discharge weight | 68,680 | 33,095 | 255,570 | 1,695,070 | 715,145 | |
| In-Hospital Procedures | ||||||
| Coronary Angiography | 30.5% | 46.6% | 34.2% | 66.7% | 43.4% | <0.001 |
| PCI | 14.1% | 23.2% | 19.3% | 42.6% | 22.8% | <0.001 |
| CABG | 0.6% | 0% | 0.5% | 7.7% | 5.6% | <0.001 |
| Thrombolysis | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | <0.001 |
| Mechanical Ventilation | 22.7% | 11.7% | 11.9% | 9.8% | 12.2% | <0.001 |
| Circulatory support (inc. IABP, LV assist device and ECMO). | 1.8% | 0.9% | 1.0% | 4.6% | 3.6% | <0.001 |
| In-Hospital Outcomes | ||||||
| MACCE | 21.4% | 9.10% | 13.4% | 11% | 14.1% | <0.001 |
| Mortality | 17.7% | 6.7% | 9.80% | 6.50% | 10.1% | <0.001 |
| Acute CVA | 4.3% | 1.9% | 4% | 2.7% | 2.9% | <0.001 |
| Major Bleeding | 7.4% | 3.9% | 5.3% | 4.2% | 6.3% | <0.001 |
| Length of stay, days, mean | 5.72 | 4.05 | 4.6 | 5.06 | 7 | <0.001 |
| Total charge, USD, mean | USD 89,890.11 | USD 71,472.06 | USD 70,846.81 | USD 96,495.32 | USD 101,842.68 | <0.001 |
| CKM Stage 1 | CKM Stage 2 and 3 | CKM Stage 4A | CKM Stage 4B | |||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| CA | 1.97 (1.91–2.02) | <0.001 | 1.68 (1.64–1.71) | <0.001 | 6.86 (6.73–6.99) | <0.001 | 3.87 (3.80–3.95) | <0.001 |
| PCI | 1.90 (1.83–1.97) | <0.001 | 1.97 (1.91–2.02) | <0.001 | 5.93 (5.79–6.08) | <0.001 | 4.14 (4.04–4.24) | <0.001 |
| CABG | 0.76 (0.62–0.93) | 0.009 | 1.07 (0.96–1.21) | 0.223 | 20.70 (18.71–22.91) | <0.001 | 8.49 (7.67–9.40) | <0.001 |
| MACCE | 0.47 (0.45–0.49) | <0.001 | 0.58 (0.56–0.59) | <0.001 | 0.44 (0.43–0.45) | <0.001 | 0.50 (0.49–0.52) | <0.001 |
| Mortality | 0.45 (0.43–0.48) | <0.001 | 0.46 (0.44–0.47) | <0.001 | 0.25 (0.25–0.26) | <0.001 | 0.34 (0.33–0.35) | <0.001 |
| Acute CVA | 0.56 (0.52–0.62) | <0.001 | 0.94 (0.90–0.98) | 0.007 | 1.05 (1.01–1.09) | 0.024 | 0.83 (0.80–0.87) | <0.001 |
| Major bleeding | 0.69 (0.64–0.73) | <0.001 | 0.74 (0.71–0.76) | <0.001 | 0.75 (0.73–0.78) | <0.001 | 0.61 (0.59–0.63) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shabtai, R.; Gatuz, M.V.; Folman, A.; Barel, M.S.; Abu-Fanne, R.; Abramov, D.; Mamas, M.A.; Roguin, A.; Kobo, O. Impact of Cardiovascular–Kidney–Metabolic Syndrome Staging on Myocardial Infarction Outcomes: A Retrospective Analysis of 2.7 Million Patients. Diseases 2025, 13, 97. https://doi.org/10.3390/diseases13040097
Shabtai R, Gatuz MV, Folman A, Barel MS, Abu-Fanne R, Abramov D, Mamas MA, Roguin A, Kobo O. Impact of Cardiovascular–Kidney–Metabolic Syndrome Staging on Myocardial Infarction Outcomes: A Retrospective Analysis of 2.7 Million Patients. Diseases. 2025; 13(4):97. https://doi.org/10.3390/diseases13040097
Chicago/Turabian StyleShabtai, Ronny, Marlon Villaga Gatuz, Adam Folman, Maguli S. Barel, Rami Abu-Fanne, Dmitry Abramov, Mamas A. Mamas, Ariel Roguin, and Ofer Kobo. 2025. "Impact of Cardiovascular–Kidney–Metabolic Syndrome Staging on Myocardial Infarction Outcomes: A Retrospective Analysis of 2.7 Million Patients" Diseases 13, no. 4: 97. https://doi.org/10.3390/diseases13040097
APA StyleShabtai, R., Gatuz, M. V., Folman, A., Barel, M. S., Abu-Fanne, R., Abramov, D., Mamas, M. A., Roguin, A., & Kobo, O. (2025). Impact of Cardiovascular–Kidney–Metabolic Syndrome Staging on Myocardial Infarction Outcomes: A Retrospective Analysis of 2.7 Million Patients. Diseases, 13(4), 97. https://doi.org/10.3390/diseases13040097