1. Introduction
Multidrug-resistant bacteria (MDR) is one of the major public health problems of the 21st century. The most comprehensive and latest published data regarding worldwide antimicrobial resistance reported more than 5 million deaths in 2019 attributed to resistance, and more than 1.25 million people had a death directly linked to multidrug-resistant bacteria (MDR) [
1]. Many other studies proved that MDR bacteria increase mortality and morbidity [
2,
3,
4,
5,
6]. On the other hand, the rise of antibiotic resistance is associated with increased economic burn, hospitalization, and higher disability-adjusted life-years [
1,
2]. In the face of all these implications, one should constantly assess and evaluate the regional antibiotic resistance patterns to identify possible solutions to reduce MDR mortality and economic impact [
1].
Real data regarding antimicrobial resistance rates of positive urine cultures from Romania are scarce and the focus was mainly on female patients [
7,
8,
9,
10,
11,
12].
Escherichia coli was the leading bacteria to generate a urinary tract infection followed by
Klebsiella and
Proteus. These bacteria remained the most commonly identified pathogens in patients with diabetes mellitus from the Western part of Romania who developed UTI [
13,
14].
Data from Romania report different antimicrobial resistance rates in patients with UTI [
9,
10,
11,
12,
13]. For instance,
E. coli resistance to quinolones varies from 30 to 72%, and penicillin’s between 14 and 66% [
7,
9]. For
E. coli, Petca et al. reported the highest resistance rate to ciprofloxacin (30%) and only 14% to amoxicillin–clavulanic acid in females [
7], much lower than Chibelean et al., who reported a 72% resistance to quinolones and 66% to penicillin-amines in males [
9]. In an analysis of six East European countries,
E. coli presented the highest resistance rate to ampicillin (39.6%) and trimethoprim (23.8%), and around 15% to ciprofloxacin [
15]. These differences in resistances are consistent with other bacteria, like
Klebsiella,
Enterobacter, or
Pseudomonas [
7,
8,
9,
10,
11]. These heterogeneous results are the consequence of the empirical antibiotic therapy used in treating UTIs. Even though there are European guidelines recommending a “safe” use of an antibiotic if the resistance is lower than 20%, real-life data show that it is impossible for a continental guideline to be adequate.
In the face of such scattered data regarding antibiotic resistance, and the lack of national guidelines for antibiotic treatment of UTI, there is an imperative need to assess the antimicrobial resistance rates depending on the geographic area before the physician can prescribe an empirical treatment for UTI. Otherwise, the ascending trend of improper use of certain antibiotics will influence antimicrobial resistance rates, especially in patients with multiple UTIs. Nevertheless, every region could have a different approach regarding the type of antibiotics used in treating infections, if there is enough information regarding the local antimicrobial resistance.
Studies from the western part of Romania on UTI bacteria are scarce and they evaluate specific populations like children or patients with diabetes mellitus [
13,
14,
16].
There is a known fact that most of the bacteria responsible for UTIs are the Gram-negative ones [
7,
8,
9,
10,
11,
12]. Nevertheless, the incidence of UTIs generated by Gram-positive bacteria can be up to 30% [
9]. On the other hand, some bacteria strains are more common in UTI, as presented earlier.
To fill this gap, we performed a retrospective cross-sectional analysis in the largest hospital in the western part of Romania on positive urine cultures identified during 2021 in a mixed adult population. We aimed to evaluate the bacterial resistance to the most used antibiotics, to identify differences in resistance, and to determine the incidence of MDR bacteria. In our analysis, we included the positive urine cultures obtained from inpatients and outpatients as a comparative focus. Due to different antibiotic susceptibility, we classified bacteria according to Gram classification in Gram-positive and Gram-negative. In addition, we explored the differences regarding antibiotic resistance for most common bacteria.
4. Discussion
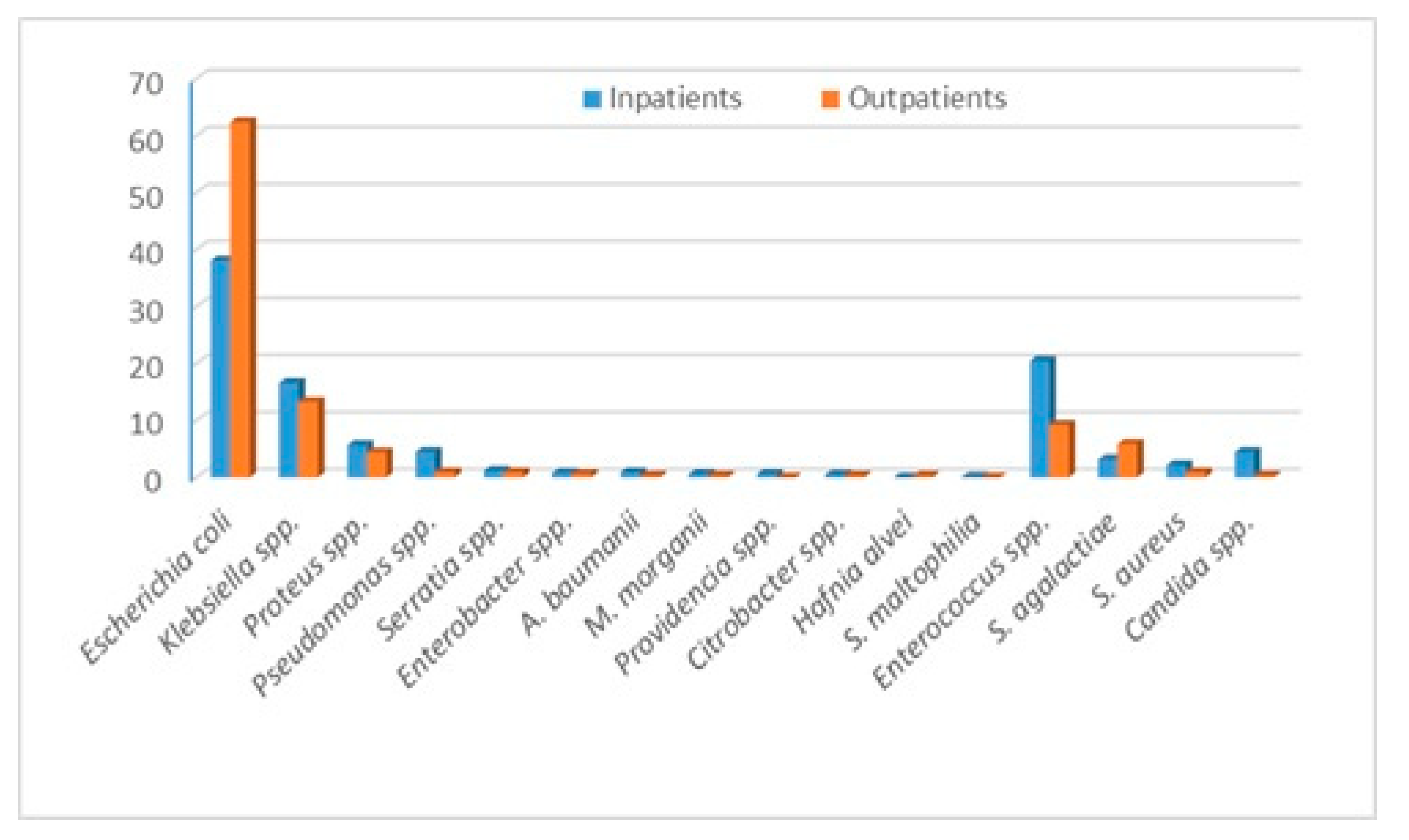
Our study is the first one to evaluate bacteria and the antibiotic resistance rate identified in a mixed adult population stratified by in and outpatients from the Western part of Romania. The most commonly identified bacteria is E. coli, followed by Enterococcus spp., Klebsiella spp., and Proteus spp. Outpatients presented a slightly different pattern, with E. coli representing almost two-thirds of identified bacteria, followed by Klebsiella spp. and Enterococcus spp.
E. coli presented the highest resistance rate to amoxicillin–clavulanic acid, Enterococcus spp. to quinolones, Klebsiella spp. to cephalosporins, and Proteus spp. to trimethoprim–sulfamethoxazole. Inpatients presented the highest resistance rates for E. coli to ampicillin, ceftazidime, cefuroxime, gentamycin, ciprofloxacin, and trimethoprim/sulfamethoxazole, Klebsiella spp. to most cephalosporins, gentamycin and levofloxacin, Proteus spp. to gentamycin and Enterococcus spp. to gentamycin and all quinolones. The highest incidence of XDR bacteria was among Acinetobacter baumanii, followed by Pseudomonas sppand Serratia spp. Almost half of Klebsiella spp. strains produce ESBL but only 4.8% XDR. MRSA incidence was 35.3%.
The female gender is associated with a higher risk of urinary tract infection (UTI) especially before the age of 50 years old [
20]. In the elderly, it seems that both females and males have the same risk of UTI, especially due to the urological-associated pathology in males [
21,
22]. Even with a relatively advanced age (67), our cohort has a slight predominance of females (65.7%).
On the other hand, we identified some differences regarding the bacteria distribution in in- and outpatients. E. coli presented a higher percentage among outpatients (62.4% vs. 38.1%). In inpatients, Enterococcus spp. and Klebsiella spp. were the next most common bacteria, while in outpatients, this order was reversed. The inpatients present several risk factors that increase the risk of nosocomial infection, like older age, multiple comorbidities, urine catheters, multiple antibiotics administration, and invasive procedures. For instance, the fact that some of the inpatients presented urine catheters explains the higher incidence of Pseudomonas spp. in this group. These risk factors increase the risk of infection with MDR agents, and thus, one should expect a much higher incidence of these bacteria in the inpatients. All of these factors should influence the decision of empirical antibiotherapy. For outpatients, the doctors could choose from a larger number of antibiotics to treat a UTI, but for the inpatients, the treatment possibilities are lower due to a higher incidence of MDR bacteria.
Sorescu et al. recently evaluated bacteria distribution in urinary tract infections from patients with diabetes from the same hospital as ours [
14]. The trend was similar, with
E. coli being the leading pathogen, followed by
Klebsiella spp. and
Enteroccocus spp. [
14].
Several factors are involved in bacterial resistance development [
23]. In addition to the increased use of antibiotics in both people and animals, there is a link between resistance to different antibiotics and the most commonly prescribed antibacterial agents within different regions [
23].
Previously published data from Romania reported different susceptibilities in both males and females. For
E. coli, Petca et al. reported the highest resistance rate to ciprofloxacin (30%) and only 14% to amoxicillin–clavulanic acid in females [
7], much lower than Chibelean et al., who reported a 72% resistance to quinolones and 66% to penicillin amines in males [
9]. In an analysis of six East-European countries,
E. coli presented the highest resistance rate to ampicillin (39.6%) and trimethoprim (23.8%), and around 15% to ciprofloxacin [
15].
We report a higher resistance rate to levofloxacin for
Enterococcus spp. compared with current Romanian data—32% resistance to levofloxacin in females [
7] and 25% to levofloxacin in males [
9]. Petca et al. reported a resistance rate of 28% to amoxicillin–clavulanic acid and 15% to levofloxacin for
Klebsiella spp. in females [
7], while Chibelean et al. 59% to amoxicillin–clavulanic acid, 44% to levofloxacin and 38% to ceftazidime in males [
9], results different from ours. On the other hand, all of the aforementioned studies reported low resistances to carbapenems, similar to our results [
7,
9]. Regarding
Proteus spp. and
S. aureus, our results are in concordance with the current literature [
7,
9]. In Romania,
Pseudomonas spp. has been associated with different resistance rates: from 31 to 44% for levofloxacin, 14 to 32% for amikacin, and 24 to 26% for ceftazidime [
7,
9].
As we can see, there are differences and similarities regarding bacteria resistance to several antibiotics, within the same country. One of the major factors that generates these results is the empirical antibiotic prescription for treating UTIs. On the other hand, the studied population differs, with some studies evaluating only females and others only males [
7,
9].
The antibiotic resistance analysis for in and outpatients represents the highlight of our study. We identified that there are some differences regarding resistance to most commonly used antibiotics. First, the inpatients were older compared to outpatients and most likely presented higher comorbidity rates. An indirect proof of this is represented by the department distribution of identified positive urine cultures. Patients admitted to the urology department have urological problems and are prone to invasive procedures on the urinary tract. Neurological patients present a high rate of immobilization, are prone to dehydration, and have a higher incidence of urine catheters. Nevertheless, more than 10% of our patients present diabetes mellitus, a known risk factor for UTIs.
Secondly, inpatients present a higher risk of hospital-acquired infections (HAI) due to invasive procedures, prolonged hospitalization, and multiple antibiotic courses. HAI infections present a higher incidence of MDR bacteria; thus, one should expect higher resistance rates [
1,
2,
3,
4,
5]. We are aware that we did not evaluate the incidence of HAI in our cohort.
Worldwide, the trend of antimicrobial resistance of different uropathogens is rising. The downside seems to be a reduced susceptibility to the most common antibiotics for both community—and hospital-acquired UTIs [
1,
24,
25].
Antibiotic resistance represents a major world health problem with high morbidity and mortality [
1,
26]. The reported mortality associated with MDR bacteria is rising with an estimated mortality of 5 million deaths in 2019 and it is presumed to double by 2030 [
1,
2]. On the other hand, the estimated costs of treating MDR bacteria represent USD 12.61 billion in 2024, with an increase of 6.5% per year, up to USD 16.22 billion in 2028 [
27]. The published data regarding MDR bacteria and even the resistance to several antibiotics are not uniform, as most of the studies were conducted in developed countries [
1,
2,
3,
4,
5]. Nevertheless, due to the regional pattern of antibiotic resistance, one could not properly estimate bacteria resistance to a specific antibiotic not even in the same country. However, besides the economic burden and the high mortality rates, the importance of reporting antimicrobial resistance and MDR strains is highlighted by the necessity of broad-spectrum therapeutics [
28,
29].
As expected, the hospital bacteria presented the highest resistance rates.
Acinetobacter baumanii presented the highest incidences in most of the resistance patterns. It was the most common bacteria with an XDR pattern, followed by
Pseudomonas spp. and
Serratia spp. More than 20% of
E. coli strains were MDR and a third of
Klebsiella spp. A recent analysis of Petca regarding the MDR uropathogens in Romania showed an incidence of 4.5% of MDR bacteria [
8]. Nevertheless, in Petca’s study,
E. coli and
Klebsiella spp. represented the most common MDR bacteria, while in ours were
Klebsiella spp.,
Acinetobacter baumanii, and
Serratia spp.
Our study presents some limitations. The cross-sectional and retrospective type, without data regarding hospital stay, mortality, and other comorbidities, could limit the impact of our results. Unfortunately, molecular testing to identify antibiotic resistance genes or virulence genes was not performed. In future studies, we plan to evaluate isolates in this perspective as well. On the other hand, a relatively high number of evaluated positive urine cultures doubled by the evaluation of the MDR incidence and stratification on in and outpatients represents the strongest points. Our study is the first one from the western part of Romania, which analyzed the positive urine culture from a tertiary care hospital.


 ,
, 


{kind=link}
{kind=link}