
A Multi-Pathogen Retrospective Study in Patients Hospitalized for Acute Gastroenteritis

 ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, T.; Klamer, S.; Jacquinet, S.; Catry, B.; Litzroth, A.; Mortgat, L.; Mamouris, P.; Rebolledo, J.; Vaes, B.; Van Cauteren, D.; et al. The health and economic impact of acute gastroenteritis in Belgium, 2010–2014. Epidemiol. Infect. 2019, 147, e146. [Google Scholar] [CrossRef] [PubMed]
- Barker, S.F.; Zomer, E.; O’Toole, J.; Sinclair, M.; Gibney, K.; Liew, D.; Leder, K. Cost of gastroenteritis in Australia: A healthcare perspective. PLoS ONE 2018, 13, e0195759. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 Diarrhoeal Disease Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the global burden of disease study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef]
- Schmidt, M.A.; Groom, H.C.; Rawlings, A.M.; Mattison, C.P.; Salas, S.B.; Burke, R.M.; Hallowell, B.D.; Calderwood, L.E.; Donald, J.; Balachandran, N.; et al. Incidence, Etiology, and Healthcare Utilization for Acute Gastroenteritis in the Community, United States. Emerg. Infect. Dis. 2022, 28, 2234–2242. [Google Scholar] [CrossRef]
- Graves, N.S. Acute gastroenteritis. Prim. Care 2013, 40, 727–741. [Google Scholar] [CrossRef]
- Raboni, S.M.; Damasio, G.A.C.; Ferreira, C.E.O.; Pereira, L.A.; Nogueira, M.B.; Vidal, L.R.; Cruz, C.R.; Almeida, S.M. Acute Gastroenteritis and Enteric Viruses in Hospitalised Children in Southern Brazil: Aetiology, Seasonality and Clinical Outcomes. Mem. Inst. Oswaldo Cruz 2014, 109, 428–435. [Google Scholar] [CrossRef]
- Guido, M.; Zizza, A.; Bredl, S.; Lindner, J.; De Donno, A.; Quattrocchi, M.; Grima, P.; Modrow, S.; Seroepidemiology Group. Seroepidemiology of human bocavirus in Apulia, Italy. Clin. Microbiol. Infect. 2012, 18, E74–E76. [Google Scholar] [CrossRef]
- Rose, T.C.; Adams, N.; Taylor-Robinson, D.C.; Barr, B.; Hawker, J.; O’Brien, S.; Violato, M.; Whitehead, M. Relationship between socioeconomic status and gastrointestinal infections in developed countries: A systematic review protocol. Syst. Rev. 2016, 5, 13. [Google Scholar] [CrossRef]
- Tate, J.E.; Burton, A.H.; Boschi-Pinto, C.; Steele, A.D.; Duque, J.; Parashar, U.D.; WHO-coordinated Global Rotavirus Surveillance Network. 2008 estimate of worldwide rotavirus-associated mortality in children younger than 5 years before the introduction of universal rotavirus vaccination programmes: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 136–141. [Google Scholar] [CrossRef]
- Lanata, C.F.; Fischer-Walker, C.L.; Olascoaga, A.C.; Torres, C.X.; Aryee, M.J.; Black, R.E.; Child Health Epidemiology Reference Group of the World Health Organization and UNICEF. Global causes of diarrheal disease mortality in children <5 years of age: A systematic review. PLoS ONE 2013, 8, e72788. [Google Scholar]
- Ahmed, S.M.; Hall, A.J.; Robinson, A.E.; Verhoef, L.; Premkumar, P.; Parashar, U.D.; Koopmans, M.; Lopman, B.A. Global prevalence of norovirus in cases of gastroenteritis: A systematic review and meta-analysis. Lancet Infect. Dis. 2014, 14, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.P.; Zhou, S.X.; Wang, X.; Lu, Q.B.; Shi, L.S.; Ren, X.; Zhang, H.Y.; Wang, Y.F.; Lin, S.H.; Zhang, C.H. Etiological, epidemiological, and clinical features of acute diarrhea in China. Nat. Commun. 2021, 12, 2464. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Amodio, E.; Vitale, F. Impact on Rotavirus Gastro-Enteritis Hospitalisation during the First Year of Universal Vaccination in Sicily. Paediatr. Int. Child. Health 2015, 35, 342–343. [Google Scholar] [CrossRef]
- Khagayi, S.; Omore, R.; Otieno, G.P.; Ogwel, B.; Ochieng, J.B.; Juma, J.; Apondi, E.; Bigogo, G.; Onyango, C.; Ngama, M.; et al. Effectiveness of Monovalent Rotavirus Vaccine Against Hospitalization with Acute Rotavirus Gastroenteritis in Kenyan Children. Clin. Infect. Dis. 2020, 70, 2298–2305. [Google Scholar] [CrossRef]
- Kobayashi, M.; Miyazaki, M.; Ogawa, A.; Tatsumi, M. Sustained reduction in rotavirus-coded hospitalizations in children aged <5 years after introduction of self-financed rotavirus vaccines in Japan. Hum. Vaccines Immunother. 2020, 16, 132–137. [Google Scholar]
- Muhsen, K.; Rubenstein, U.; Kassem, E.; Goren, S.; Schachter, Y.; Kremer, A.; Shulman, L.M.; Ephros, M.; Cohen, D. A significant and consistent reduction in rotavirus gastroenteritis hospitalization of children under 5 years of age, following the introduction of universal rotavirus immunization in Israel. Hum. Vaccines Immunother. 2015, 11, 2475–2482. [Google Scholar] [CrossRef]
- Baker, J.M.; Tate, J.E.; Steiner, C.A.; Haber, M.J.; Parashar, U.D.; Lopman, B.A. Longer-Term Direct and Indirect Effects of Infant Rotavirus Vaccination Across All Ages in the United States in 2000–2013: Analysis of a Large Hospital Discharge Data Set. Clin. Infect. Dis. 2019, 68, 976–983. [Google Scholar] [CrossRef]
- Operario, D.J.; Platts-Mills, J.A.; Nadan, S.; Page, N.; Seheri, M.; Mphahlele, J.; Praharaj, I.; Kang, G.; Araujo, I.T.; Leite, J.P.G.; et al. Etiology of Severe Acute Watery Diarrhea in Children in the Global Rotavirus Surveillance Network Using Quantitative Polymerase Chain Reaction. J. Infect. Dis. 2017, 216, 220–227. [Google Scholar] [CrossRef]
- Payne, D.C.; Vinjé, J.; Szilagyi, P.G.; Edwards, K.M.; Staat, M.A.; Weinberg, G.A.; Hall, C.B.; Chappell, J.; Bernstein, D.I.; Curns, A.T.; et al. Norovirus and medically attended gastroenteritis in U.S. children. N. Engl. J. Med. 2013, 368, 1121–1130. [Google Scholar] [CrossRef]
- Kotloff, K.L. Bacterial diarrhoea. Curr. Opin. Pediatr. 2022, 34, 147–155. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA); European Centre for Disease Prevention and Control (ECDC). The European Union One Health 2022 Zoonoses Report. EFSA J. 2023, 21, e8442. [Google Scholar]
- WHO. PDVAC Executive Summary 2020: Update on Development of Enterotoxigenic E. coli (ETEC) Vaccines. Available online: https://www.who.int/publications/m/item/pdvac-agenda-2020-update-on-development-of-etec-vaccines (accessed on 6 May 2024).
- WHO. WHO Preferred Product Characteristics for Vaccines against Shigella. Available online: https://www.who.int/publications/i/item/9789240036741 (accessed on 6 May 2024).
- Giersing, B.K.; Vekemans, J.; Nava, S.; Kaslow, D.C.; Moorthy, V. Report from the World Health Organization’s third Product Development for Vaccines Advisory Committee (PDVAC) meeting, Geneva, 8–10th June 2016. Vaccine 2019, 37, 7315–7327. [Google Scholar] [CrossRef] [PubMed]
- Seo, H.; Duan, Q.; Zhang, W. Vaccines against gastroenteritis, current progress and challenges. Gut Microbes 2020, 11, 1486–1517. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.; Kaminski, R.W.; Porter, C.; Choy, R.K.M.; White, J.A.; Fleckenstein, J.M.; Cassels, F.; Bourgeois, L. Vaccines for Protecting Infants from Bacterial Causes of Diarrheal Disease. Microorganisms 2021, 9, 1382. [Google Scholar] [CrossRef]
- Luo, L.F.; Qiao, K.; Wang, X.G.; Ding, K.Y.; Su, H.L.; Li, C.Z.; Yan, H.J. Acute gastroenteritis outbreak caused by a GII.6 norovirus. World J. Gastroenterol. 2015, 21, 5295–5302. [Google Scholar] [CrossRef]
- Zhao, X.; Ni, B.; Wang, Y.; Shen, X.; Zhang, C.; Liu, J.; Li, S. Aetiological characteristics of adult acute diarrhoea in a general hospital of Shanghai. Epidemiol. Infect. 2017, 145, 545–552. [Google Scholar] [CrossRef]
- Patel, M.M.; Pitzer, V.E.; Alonso, W.J.; Vera, D.; Lopman, B.; Tate, J.; Viboud, C.; Parashar, U.D. Global seasonality of rotavirus disease. Pediatr. Infect. Dis. J. 2013, 32, e134–e147. [Google Scholar] [CrossRef]
- Patel, M.M.; Hall, A.J.; Vinjé, J.; Parashar, U.D. Noroviruses: A comprehensive review. J. Clin. Virol. 2009, 44, 1–8. [Google Scholar] [CrossRef]
- Ahmed, S.M.; Lopman, B.A.; Levy, K. A systematic review and meta-analysis of the global seasonality of norovirus. PLoS ONE 2013, 8, e75922. [Google Scholar] [CrossRef]
- Elliott, E.J. Acute gastroenteritis in children. BMJ 2007, 334, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Duzova, A.; Bakkaloglu, A.; Kalyoncu, M.; Poyrazoglu, H.; Delibas, A.; Ozkaya, O.; Peru, H.; Alpay, H.; Soylemezoglu, O.; Gur-Guven, A.; et al. Etiology and outcome of acute kidney injury in children. Pediatr. Nephrol. 2010, 25, 1453–1461. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, S.M.; Ji, J.; Sheikhi, F.H.; Widen, E.; Tian, L.; Alexander, S.R.; Ling, X.B. AKI in hospitalized children: Epidemiology and clinical associations in a national cohort. Clin. J. Am. Soc. Nephrol. 2013, 8, 1661–1669. [Google Scholar] [CrossRef] [PubMed]
- Mammen, C.; Al Abbas, A.; Skippen, P.; Nadel, H.; Levine, D.; Collet, J.P.; Matsell, D.G. Long-term risk of CKD in children surviving episodes of acute kidney injury in the intensive care unit: A prospective cohort study. Am. J. Kidney Dis. 2012, 59, 523–530. [Google Scholar] [CrossRef]
- Coca, S.G.; Singanamala, S.; Parikh, C.R. Chronic kidney disease after acute kidney injury: A systematic review and meta-analysis. Kidney Int. 2012, 81, 442–448. [Google Scholar] [CrossRef]
- Stanyevic, B.; Sepich, M.; Biondi, S.; Baroncelli, G.I.; Peroni, D.; Di Cicco, M. The evolving epidemiology of acute gastroenteritis in hospitalized children in Italy. Eur. J. Pediatr. 2022, 181, 349–358. [Google Scholar] [CrossRef]
- Biscaro, V.; Piccinelli, G.; Gargiulo, F.; Ianiro, G.; Caruso, A.; Caccuri, F.; De Francesco, M.A. Detection and molecular characterization of enteric viruses in children with acute gastroenteritis in Northern Italy. Infect. Genet. Evol. 2018, 60, 35–41. [Google Scholar] [CrossRef]
- Regione Puglia. Protocollo Operativo “Sorveglianza delle Gastroenteriti Emorragiche in Età Pediatrica” Prot. AOO_005_000221 del 21 Giugno 2018. Available online: https://www.sanita.puglia.it/documents/20182/26606314/Protocollo+Operativo_Sorveglianza+Gastroenteriti+emorragiche+in+et%C3%A0+pediatrica.pdf/dc372a68-bcf3-465e-bf25-cee20a892da8 (accessed on 13 June 2024).
- Schnadower, D.; Finkelstein, Y.; Freedman, S.B. Ondansetron and probiotics in the management of pediatric acute gastroenteritis in developed countries. Curr. Opin. Gastroenterol. 2015, 31, 1–6. [Google Scholar] [CrossRef]
- Mattei, A.; Sbarbati, M.; Fiasca, F.; Angelone, A.M.; Mazzei, M.C.; di Orio, F. Temporal trends in hospitalization for rotavirus gastroenteritis: A nationwide study in Italy, 2005–2012. Hum. Vaccines Immunother. 2016, 12, 534–539. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation. Deaths Diarrheal Diseases. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 6 March 2024).
- Chironna, M.; Loconsole, D.; Centrone, F.; Giordano, M. Sorveglianza Regionale delle Gastroenteriti Emorragiche in età Pediatrica. Report sulle Attività Svolte dal 21/06/2018 30/11/2021. Report Regione Puglia 2021. Available online: https://www.sanita.puglia.it/documents/20182/26606314/Report+GE+Puglia+2021_DEF.pdf/a3f002e6-c54a-4a9f-850b-217f74de1fe0 (accessed on 19 June 2024).
- Zizza, A.; Recchia, V.; Aloisi, A.; Guido, M. Clinical features of COVID-19 and SARS epidemics. A literature review. J. Prev. Med. Hyg. 2021, 62, E13–E24. [Google Scholar]
- Di Martino, G.; Cedrone, F.; Di Giovanni, P.; Tognaccini, L.; Trebbi, E.; Romano, F.; Staniscia, T. The Burden of HPV-Related Hospitalizations: Analysis of Hospital Discharge Records from the Years 2015–2021 from a Southern Italian Region. Pathogens 2023, 12, 725. [Google Scholar] [CrossRef] [PubMed]
- Cedrone, F.; Montagna, V.; Del Duca, L.; Camplone, L.; Mazzocca, R.; Carfagnini, F.; Fortunato, V.; Di Martino, G. The Burden of Streptococcus pneumoniae-Related Admissions and In-Hospital Mortality: A Retrospective Observational Study between the Years 2015 and 2022 from a Southern Italian Province. Vaccines 2023, 11, 1324. [Google Scholar] [CrossRef] [PubMed]
- Thwiny, H.T.; Alsalih, N.J.; Saeed, Z.F.; Al-Yasari, A.M.R.; Al-Saadawe, M.A.A.; Alsaadawi, M.A.E. Prevalence and seasonal pattern of enteric viruses among hospitalized children with acute gastroenteritis in Samawah, Iraq. J. Med. Life 2022, 15, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Gu, Y.; Wang, X.; Zhang, Y.; Zhan, L.; Liu, J.; Yan, H.; Liu, Y.; Zhen, S.; Chen, X.; et al. Epidemiological and clinical differences between sexes and pathogens in a three-year surveillance of acute infectious gastroenteritis in Shanghai. Sci. Rep. 2019, 9, 9993. [Google Scholar] [CrossRef]
- Olaimat, A.N.; Taybeh, A.O.; Al-Nabulsi, A.; Al-Holy, M.; Hatmal, M.M.; Alzyoud, J.; Aolymat, I.; Abughoush, M.H.; Shahbaz, H.; Alzyoud, A.; et al. Common and Potential Emerging Foodborne Viruses: A Comprehensive Review. Life 2024, 14, 190. [Google Scholar] [CrossRef]
- Summa, M.; Tuutti, E.; Al-Hello, H.; Huttunen, L.M.; Rimhanen-Finne, R. Norovirus GII.17 Caused Five Outbreaks Linked to Frozen Domestic Bilberries in Finland, 2019. Food Environ. Virol. 2024, 16, 180–187. [Google Scholar] [CrossRef]
- Li, F.; Guo, L.; Li, Q.; Xu, H.; Fu, Y.; Huang, L.; Feng, G.; Liu, G.; Chen, X.; Xie, Z. Changes in the epidemiology and clinical characteristics of viral gastroenteritis among hospitalized children in the Mainland of China: A retrospective study from 2016 to 2020. BMC Pediatr. 2024, 24, 303. [Google Scholar] [CrossRef]
- Farfán-García, A.E.; Imdad, A.; Zhang, C.; Arias-Guerrero, M.Y.; Sánchez-Álvarez, N.T.; Iqbal, J.; Hernández-Gamboa, A.E.; Slaughter, J.C.; Gómez-Duarte, O.G. Etiology of acute gastroenteritis among children less than 5 years of age in Bucaramanga, Colombia: A case-control study. PLoS Negl. Trop. Dis. 2020, 14, e0008375. [Google Scholar] [CrossRef]
- Amodio, E.; De Grazia, S.; Genovese, D.; Bonura, F.; Filizzolo, C.; Collura, A.; Di Bernardo, F.; Giammanco, G.M. Clinical and Epidemiologic Features of Viral Gastroenteritis in Hospitalized Children: An 11-Year Surveillance in Palermo (Sicily). Viruses 2022, 15, 41. [Google Scholar] [CrossRef]
- Posovszky, C.; Buderus, S.; Classen, M.; Lawrenz, B.; Keller, K.M.; Koletzko, S. Acute Infectious Gastroenteritis in Infancy and Childhood. Dtsch. Arztebl. Int. 2020, 117, 615–624. [Google Scholar] [CrossRef]
- Gounden, V.; Bhatt, H.; Jialal, I. Renal Function Tests. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK507821/ (accessed on 7 June 2024).
- Gauchan, E.; Malla, K.K. Relationship of Renal Function Tests and Electrolyte Levels with Severity of Dehydration in Acute Diarrhea. J. Nepal Health Res. Counc. 2015, 13, 84–89. [Google Scholar] [PubMed]
- Tutay, G.J.; Capraro, G.; Spirko, B.; Garb, J.; Smithline, H. Electrolyte profile of pediatric patients with hypertrophic pyloric stenosis. Pediatr. Emerg. Care 2013, 29, 465–468. [Google Scholar] [CrossRef] [PubMed]
- Grassi, T.; De Donno, A.; Guido, M.; Gabutti, G.; Collaborative Group for the Surveillance of Rotavirus Infection. The epidemiology and disease burden of rotavirus infection in the Salento peninsula, Italy. Turk. J. Pediatr. 2008, 50, 132–136. [Google Scholar] [PubMed]
- Soares-Weiser, K.; Bergman, H.; Henschke, N.; Pitan, F.; Cunliffe, N. Vaccines for preventing rotavirus diarrhoea: Vaccines in use. Cochrane Database Syst. Rev. 2019, 2019, CD008521. [Google Scholar] [PubMed]
- Pindyck, T.; Tate, J.E.; Parashar, U.D. A decade of experience with rotavirus vaccination in the United States—Vaccine uptake, effectiveness, and impact. Expert Rev. Vaccines 2018, 17, 593–606. [Google Scholar] [CrossRef]
- Shah, M.P.; Dahl, R.M.; Parashar, U.D.; Lopman, B.A. Annual changes in rotavirus hospitalization rates before and after rotavirus vaccine implementation in the United States. PLoS ONE 2018, 13, e0191429. [Google Scholar] [CrossRef]
- Italian Ministry of Health. Vaccinazioni Dell’età Pediatrica e Dell’adolescenza—Coperture Vaccinali. Available online: https://www.salute.gov.it/imgs/C_17_tavole_20_11_0_file.pdf (accessed on 12 June 2024).
- Velasquez-Portocarrero, D.E.; Wang, X.; Cortese, M.M.; Snider, C.J.; Anand, A.; Costantini, V.P.; Yunus, M.; Aziz, A.B.; Haque, W.; Parashar, U.; et al. Head-to-head comparison of the immunogenicity of RotaTeq and Rotarix rotavirus vaccines and factors associated with seroresponse in infants in Bangladesh: A randomised, controlled, open-label, parallel, phase 4 trial. Lancet Infect. Dis. 2022, 22, 1606–1616. [Google Scholar] [CrossRef]
- Osborne, C.M.; Montano, A.C.; Robinson, C.C.; Schultz-Cherry, S.; Dominguez, S.R. Viral gastroenteritis in children in Colorado 2006–2009. J. Med. Virol. 2015, 87, 931–939. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | All Patients (n = 103) | Group 1 (<5 Years) (n = 59) | Group 2 (≥5 Years) (n = 44) | p |
|---|---|---|---|---|
| Age, median years (IQR) | 3 (1–8) | 1 (1–2) | 9 (6–12.25) | 0.0001 ^ |
| Male, n. (%) | 60 (58.25) | 33 (55.9) | 27 (61.36) | 0.5803 ** |
| Hospital admission year, n. (%) | ||||
| - 2021, n. (%) | 20 (18.69) | 12 (20.34) | 8 (18.18) | |
| - 2022, n. (%) | 61 (57.01) | 39 (66.10) | 22 (40.00) | |
| - 2023, n. (%) | 26 (24.30) | 8 (13.56) | 14 (31.82) | 0.0782 ** |
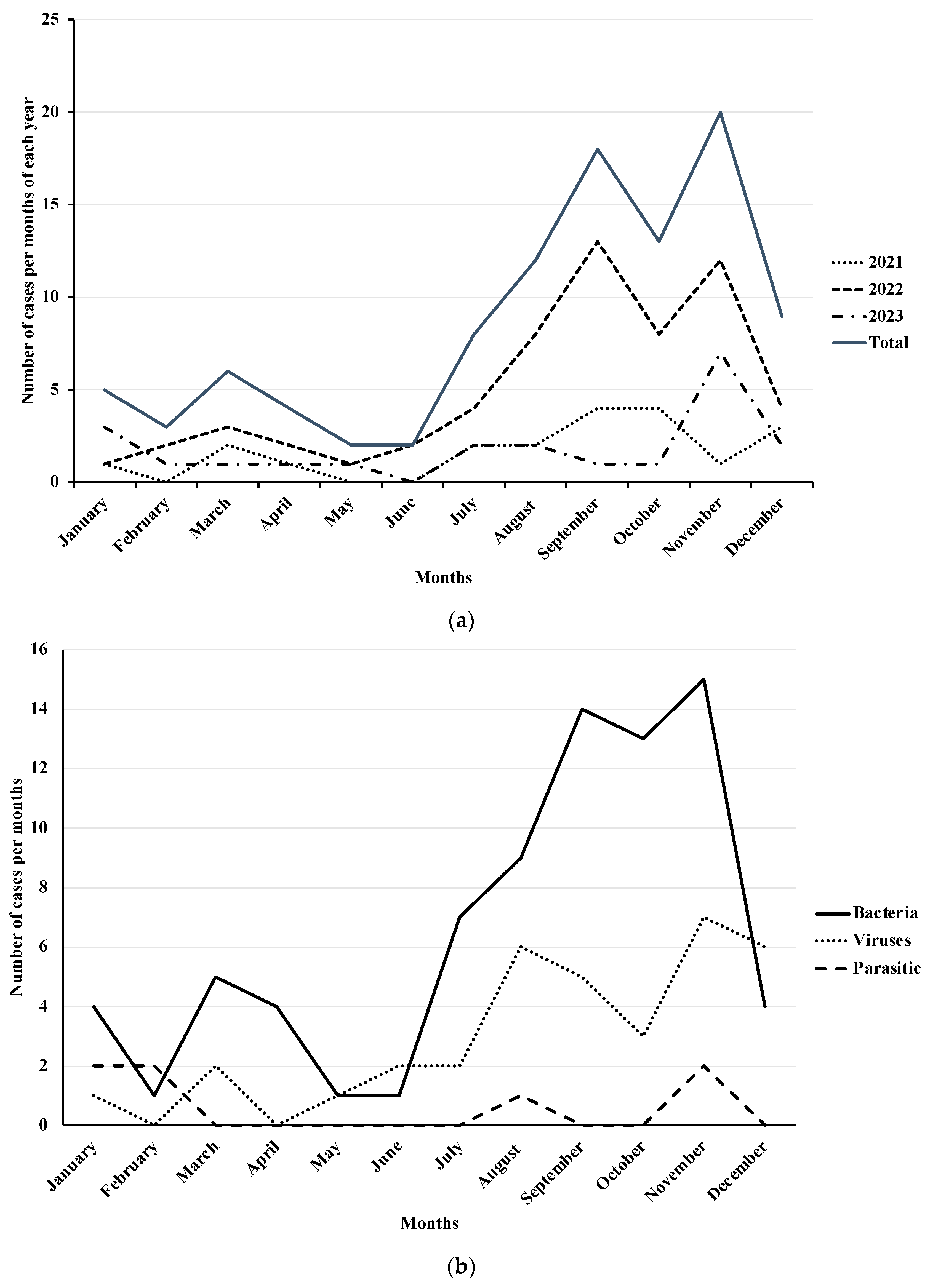
| Hospital admission season (2021–2023), n. (%) | ||||
| - Summer, n. (%) | 37 (35.92) | 20 (33.90) | 17 (38.64) | |
| - Autumn, n. (%) | 39 (37.86) | 26 (44.07) | 13 (29.55) | |
| - Winter, n. (%) | 19 (18.45) | 10 (16.95) | 9 (20.45) | |
| - Spring, n. (%) | 8 (7.77) | 3 (5.08) | 5 (11.36) | 0.3903 ** |
| Hospital length of stay in days, median (IQR) | 5 (4–6) | 5 (4–6) | 5 (4–7) | 0.2762 ^ |
| Diagnosis | Group 1 (<5 Years) (n = 59) | Group 2 (≥5 Years) (n = 44) | p |
|---|---|---|---|
| Method | |||
| Coproculture, n. (%) | 4 (6.78) | 1 (4.54) | |
| Multiplex PCR, n. (%) | 55 (93.22) | 43 (97.72) | 0.3898 * |
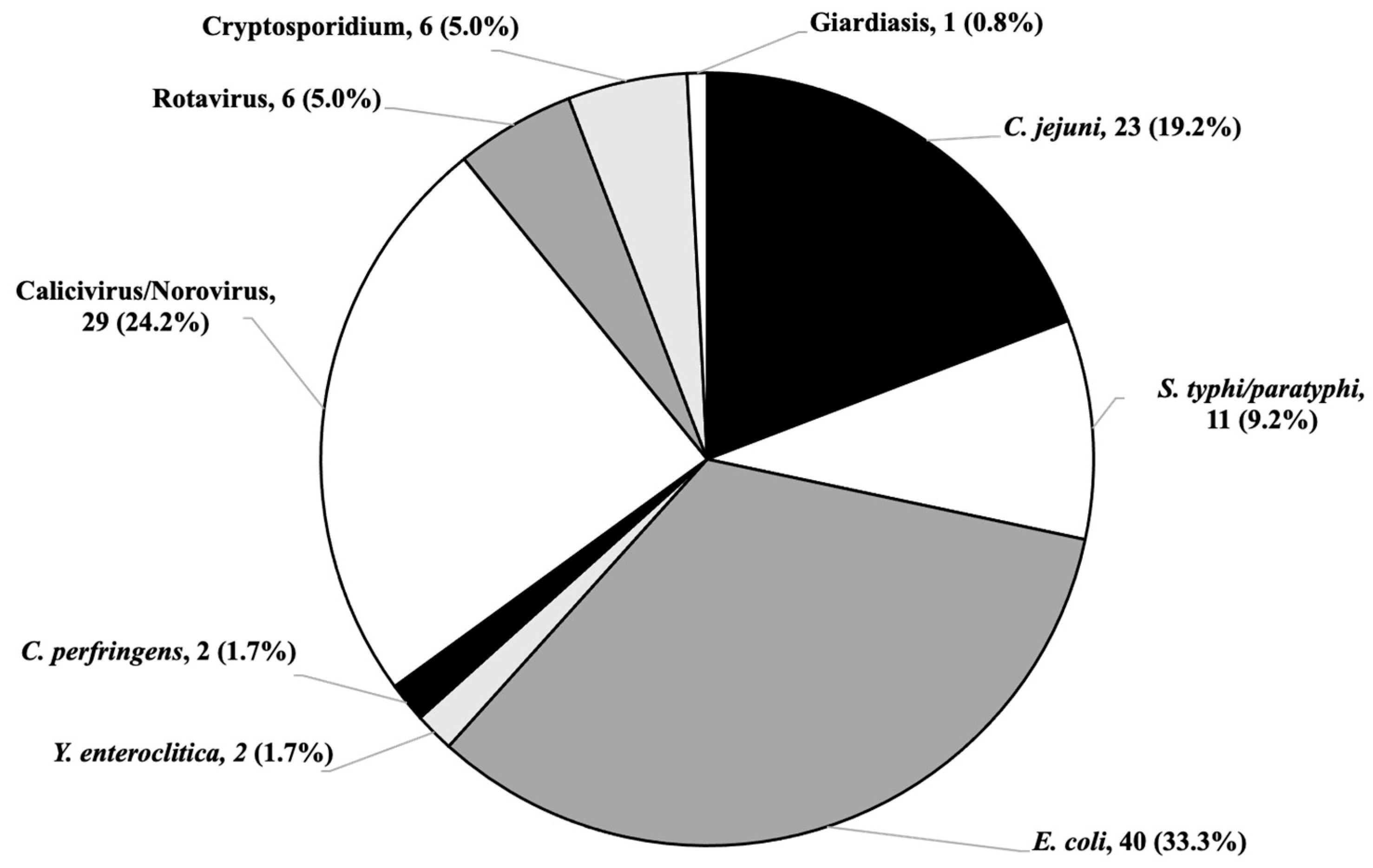
| Microbiological pathogen detected | |||
| Bacterial infection, n. (%) | 40 (67.80) | 42 (95.45) | 0.0004 * |
| C. jejuni, n. (%) | 8 (13.56) | 15 (34.09) | 0.1332 ** |
| S. typhi/Paratyphi, n. (%) | 5 (8.47) | 6 (13.64) | 0.4014 ** |
| E. coli, n. (%) | 25 (42.37) | 15 (34.09) | 0.3936 ** |
| Y. enterocolitica, n. (%) | 1 (1.69) | 1 (2.27) | 1.0000 * |
| C. perfringens, n. (%) | 1 (1.69) | 1 (2.27) | 1.0000 * |
| Viral infection, n. (%) | 26 (44.07) | 9 (20.45) | 0.0123 ** |
| Norovirus, n. (%) | 23 (38.98) | 6 (13.63) | 0.0047 ** |
| Rotavirus, n. (%) | 3 (5.08) | 3 (6.81) | 0.6989 * |
| Parasitic infection, n. (%) | 3 (5.08) | 5 (11.36) | 0.2820 * |
| Cryptosporidium, n. (%) | 3 (5.08) | 4 (9.09) | 0.4567 * |
| Giardiasis, n. (%) | 0 (-) | 1 (2.27) | 0.4272 * |
| Co-infections, n. (%) | 10 (16.95) | 7 (15.91) | 0.8881 ** |
| Hematology and Serum Chemistry Value | Group 1 (<5 Years) (n = 59) | Group 2 (≥5 Years) (n = 44) | p |
|---|---|---|---|
| Decreased Hematocrit | 22 (37.29) | 17 (38.63) | 0.8890 ** |
| Increased Lymphocytes | 22 (37.29) | 27 (61.36) | 0.0155 ** |
| Increased Neutrophils | 40 (67.80) | 29 (65.90) | 0.9918 ** |
| Increased CRP | 36 (61.02) | 29 (65.90) | 0.3605 ** |
| Decreased Sodium | 23 (38.98) | 22 (50.00) | 0.3605 ** |
| Decreased Potassium | 9 (15.25) | 3 (6.82) | 0.2274 * |
| Increased Creatinine | 20 (33.90) | 4 (8.33) | 0.0000 * |
| Increased AST | 3 (5.08) | 0 (-) | 0.2587 * |
| Increased ALT | 1 (1.69) | 0 (-) | 1.0000 * |
| Increased γ-GT | 0 (-) | 0 (-) | 1.0000 * |
| Increased Total bilirubin | 0 (-) | 0 (-) | 1.0000 * |
| Mixed Pathogens | All Patients (n = 103) | Group 1 (<5 Years) (n = 59) | Group 2 (≥5 Years) (n = 44) |
|---|---|---|---|
| Bacterial | |||
| E. coli + S. typhi/Paratyphi, n. (%) | 2 (1.94) | 1 (1.69) | 1 (2.27) |
| E. coli + C. jejuni, n. (%) | 3 (2.91) | (-) | 3 (6.81) |
| Bacterial + viral | |||
| E. coli + Norovirus, n. (%) | 6 (5.82) | 5 (0.72) | 1 (2.27) |
| C. jejuni + Rotavirus, n. (%) | 1 (0.97) | 1 (1.69) | (-) |
| C. jejuni + Norovirus, n. (%) | 1 (0.97) | (-) | 1 (2.27) |
| Y. enterocolitica + Rotavirus, n. (%) | 1 (0.97) | 1 (1.69) | (-) |
| Bacterial + parasitic | |||
| E. coli + Cryptosporidium, n. (%) | 2 (1.94) | 2 (3.39) | (-) |
| S. typhi/Paratyphi + Cryptosporidium, n. (%) | 1 (0.97) | (-) | 1 (2.27) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zizza, A.; Guido, M.; Sedile, R.; Benelli, M.; Nuzzo, M.; Paladini, P.; Romano, A.; Grima, P. A Multi-Pathogen Retrospective Study in Patients Hospitalized for Acute Gastroenteritis. Diseases 2024, 12, 213. https://doi.org/10.3390/diseases12090213
Zizza A, Guido M, Sedile R, Benelli M, Nuzzo M, Paladini P, Romano A, Grima P. A Multi-Pathogen Retrospective Study in Patients Hospitalized for Acute Gastroenteritis. Diseases. 2024; 12(9):213. https://doi.org/10.3390/diseases12090213
Chicago/Turabian StyleZizza, Antonella, Marcello Guido, Raffaella Sedile, Marzia Benelli, Milva Nuzzo, Pasquale Paladini, Anacleto Romano, and Pierfrancesco Grima. 2024. "A Multi-Pathogen Retrospective Study in Patients Hospitalized for Acute Gastroenteritis" Diseases 12, no. 9: 213. https://doi.org/10.3390/diseases12090213
APA StyleZizza, A., Guido, M., Sedile, R., Benelli, M., Nuzzo, M., Paladini, P., Romano, A., & Grima, P. (2024). A Multi-Pathogen Retrospective Study in Patients Hospitalized for Acute Gastroenteritis. Diseases, 12(9), 213. https://doi.org/10.3390/diseases12090213