
Postoperative Coagulation Changes in Patients after Epicardial Left Atrial Appendage Occlusion Varies Based on the Left Atrial Appendage Size

 ,
,  , ,
, ,
Abstract
:1. Introduction
1.1. Atrial Fibrillation Epidemiology, Complications and Treatment
1.2. The Left Atrial Appendage Occlusion Procedures
1.3. The Left Atrial Appendage Systemic Impact
1.4. The Aim of the Study
2. Materials and Methods
2.1. Characteristics of the Patients
2.2. Laboratory Tests
2.3. Left Atrial Appendage Occlusion Procedure
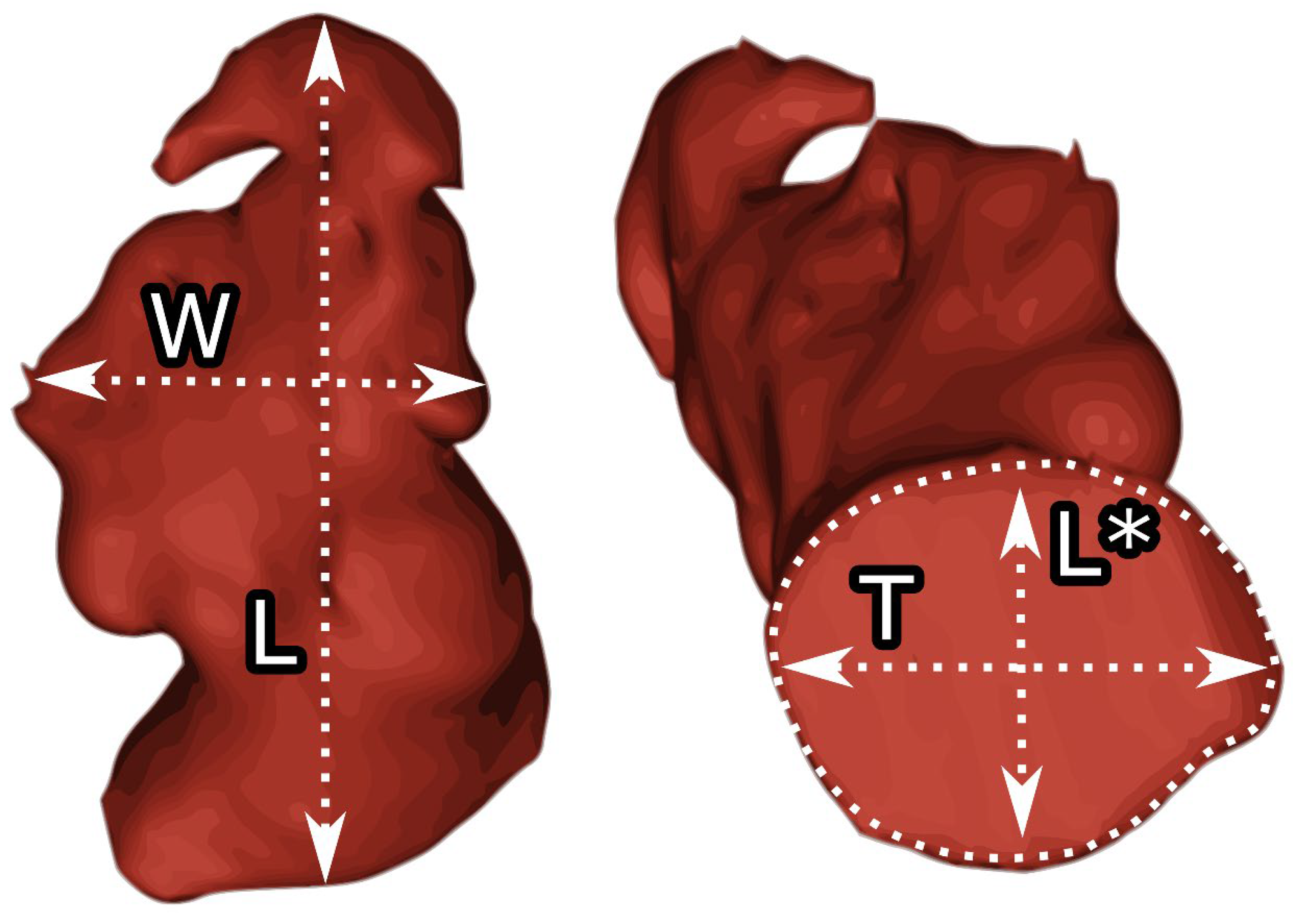
2.4. Image Processing and Analysis
2.5. Statistical Analysis
3. Results
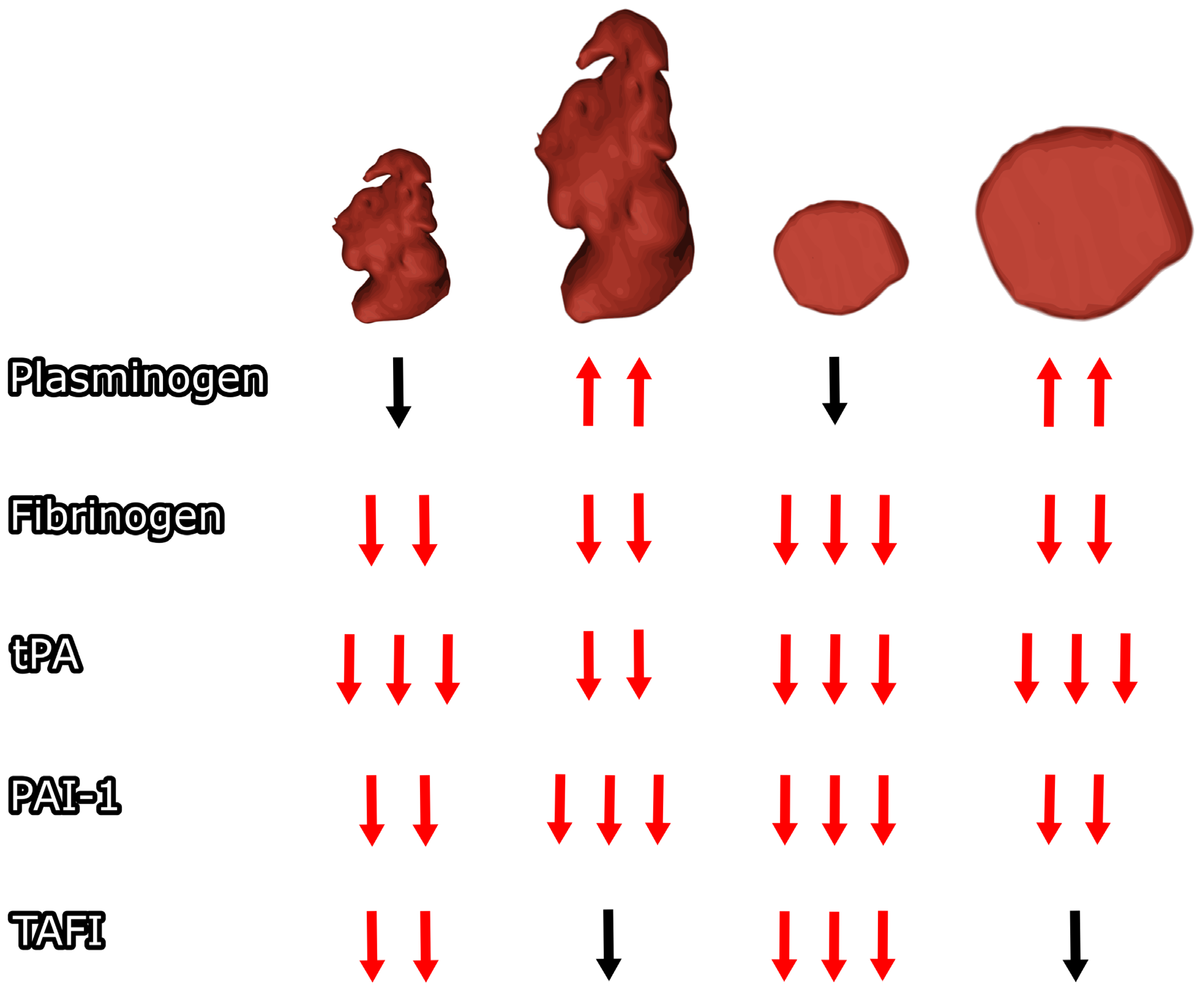
3.1. LAA Body Size Coagulation Impact
3.2. Effect of LAA Orifice Size on Coagulation
4. Discussion
4.1. LAA Subtypes Impact on Postoperative Coagulation Changes
4.2. Does Left Atrial Appendage Type Matter?
4.3. Molecular Findings Patophysiological Association
4.4. Coagulation and Fibrynolitic Factors
4.5. Enlarged Left Atrial Appendage—How to Determine?
4.6. Clinical Impact of the Left Atrial Appendage Anatomy
4.7. Endocardial Left Atrial Appendage Closure Coagulation Impact
4.8. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variable | Patients (n = 22) |
|---|---|
| Age, years (Mean ± SD) | 66.2 ± 8.7 |
| Female | 59.1% (n = 13) |
| BMI (Mean ± SD) [kg/m2] | 26.4 ± 2.4 |
| CHADS2 score (Mean ± SD) | 2.8 ± 1.0 |
| CHA2DS2-VASc score (Mean ± SD) | 3.9 ± 1.5 |
| HAS-BLED score (Mean ± SD) | 3.6 ± 1.2 |
| Congestive heart failure | 13.6% (n = 3) |
| Hypertension | 86.4% (n = 19) |
| Hyperlipidemia | 54.5% (n = 12) |
| Diabetes mellitus type 2 | 31.8% (n = 7) |
| Previous ischemic stroke/TIA | 68.2% (n = 15) |
| Hemorrhagic stroke | 59.1% (n = 13) |
| Myocardial infarction | 9.1% (n = 2) |
| Vascular disease | 13.6% (n = 3) |
| Alcoholism | 4.5% (n = 1) |
| Preprocedural OAC | |
| 13.6% (n = 3) 50.0% (n = 11) 13.6% (n = 3) 22.7% (n = 5) |
| n (%)/Mean ± SD | ||
|---|---|---|
| LAA type | chicken wing | 9 (40.9%) |
| cauliflower | 2 (9.1%) | |
| arrowhead | 11 (50%) | |
| LAA additional lobes | 0 | 11 (50%) |
| 1 | 9 (40.9%) | |
| 2 | 2 (9.1%) | |
| Orientation of main lobe | superior anterolateral | 13 (59.1%) |
| superior posterolateral | 5 (22.7%) | |
| superior lateral | 4 (18.2%) | |
| LAA width [mm] | 21.6 ± 7.2 | |
| LAA length [mm] | 47.1 ± 10.1 | |
| LAA body index [mm2] | 1025.8 ± 462.0 | |
| Ostium transverse dimension [mm] | 28.1 ± 6.2 | |
| Ostium longitudinal dimension [mm] | 23 ± 5.9 | |
| LAA ostium area [mm2] | 532.5 ± 243.4 | |
| LAA origin angle to LA [º] | 70.0 ± 19.0 | |
References
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- Magnussen, C.; Niiranen, T.J.; Ojeda, F.M.; Gianfagna, F.; Blankenberg, S.; Njølstad, I.; Vartiainen, E.; Sans, S.; Pasterkamp, G.; Hughes, M.; et al. Sex Differences and Similarities in Atrial Fibrillation Epidemiology, Risk Factors, and Mortality in Community Cohorts. Circulation 2017, 136, 1588–1597. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J.G.M. Refining Clinical Risk Stratification for Predicting Stroke and Thromboembolism in Atrial Fibrillation Using a Novel Risk Factor-Based Approach. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.G.M.; Lip, G.Y.H. A Novel User-Friendly Score (HAS-BLED) To Assess 1-Year Risk of Major Bleeding in Patients with Atrial Fibrillation. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef]
- Steffel, J.; Collins, R.; Antz, M.; Cornu, P.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; Rowell, N.; et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. EP Europace 2021, 23, 1612–1676. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Çınar, T.; Hayıroğlu, M.İ.; Selçuk, M.; Çiçek, V.; Doğan, S.; Kılıç, Ş.; Yavuz, S.; Babaoğlu, M.; Uzun, M.; Orhan, A.L. Association of Whole Blood Viscosity with Thrombus Presence in Patients Undergoing Transoesophageal Echocardiography. Int. J. Cardiovasc. Imaging 2022, 38, 601–607. [Google Scholar] [CrossRef]
- Cinar, T.; Hayiroğlu, M.İ.; Çiçek, V.; Asal, S.; Atmaca, M.M.; Keser, N.; Orhan, A.L. Predictors of Left Atrial Thrombus in Acute Ischemic Stroke Patients without Atrial Fibrillation: A Single-Center Cross-Sectional Study. Rev. Assoc. Med. Bras. 2020, 66, 1437–1443. [Google Scholar] [CrossRef]
- Toale, C.; Fitzmaurice, G.J.; Eaton, D.; Lyne, J.; Redmond, K.C. Outcomes of Left Atrial Appendage Occlusion Using the AtriClip Device: A Systematic Review. Interact. Cardiovasc. Thorac. Surg. 2019, 29, 655–662. [Google Scholar] [CrossRef]
- Burysz, M.; Litwinowicz, R.; Bryndza, M.; Skowronek, R.; Ogorzeja, W.; Bartus, K. Percutaneous Left Atrial Appendage Closure Using the LAmbre Device. First Clinical Results in Poland. Adv. Intervent. Cardiol. 2019, 15, 251–254. [Google Scholar] [CrossRef]
- Litwinowicz, R.; Burysz, M.; Mazur, P.; Kapelak, B.; Bartus, M.; Lakkireddy, D.; Lee, R.J.; Malec-Litwinowicz, M.; Bartus, K. Endocardial versus Epicardial Left Atrial Appendage Exclusion for Stroke Prevention in Patients with Atrial Fibrillation: Midterm Follow-up. J. Cardiovasc. Electrophysiol. 2021, 32, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Batko, J.; Rams, D.; Filip, G.; Bartoszcze, A.; Kapelak, B.; Bartuś, K.; Litwinowicz, R. Left Atrial Appendage Morphology and Course of the Circumflex Artery: Anatomical Implications for Left Atrial Appendage Occlusion Procedures. Innovat. Technol. Techniq. Cardiothorac. Vasc. Surg. 2022, 17, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Fauchier, L.; Cinaud, A.; Brigadeau, F.; Lepillier, A.; Pierre, B.; Abbey, S.; Fatemi, M.; Franceschi, F.; Guedeney, P.; Jacon, P.; et al. Device-Related Thrombosis After Percutaneous Left Atrial Appendage Occlusion for Atrial Fibrillation. J. Am. Coll. Cardiol. 2018, 71, 1528–1536. [Google Scholar] [CrossRef] [PubMed]
- Simard, T.; Jung, R.G.; Lehenbauer, K.; Piayda, K.; Pracoń, R.; Jackson, G.G.; Flores-Umanzor, E.; Faroux, L.; Korsholm, K.; Chun, J.K.R.; et al. Predictors of Device-Related Thrombus Following Percutaneous Left Atrial Appendage Occlusion. J. Am. Coll. Cardiol. 2021, 78, 297–313. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Ganta, N.; Filice, G.; Richard, I.; Acquah, F.; Alnabwani, D.; Patel, H.B. Embolic Cerebrovascular Accident Secondary to Device-Related Thrombus Post WATCHMAN Device Implantation. Cureus 2022, 14, e26892. [Google Scholar] [CrossRef] [PubMed]
- Pracoń, R.; Zieliński, K.; Bangalore, S.; Konka, M.; Kruk, M.; Kępka, C.; Trochimiuk, P.; Dębski, M.; Przyłuski, J.; Kaczmarska, E.; et al. Residual Stroke Risk after Left Atrial Appendage Closure in Patients with Prior Oral Anticoagulation Failure. Int. J. Cardiol. 2022, 354, 17–21. [Google Scholar] [CrossRef]
- Bartus, K.; Elbey, M.A.; Kanuri, S.H.; Lee, R.; Litwinowicz, R.; Natorska, J.; Zabczyk, M.; Bartus, M.; Kapelak, B.; Malecki, M.T.; et al. Metabolic Effects of the Left Atrial Appendage Exclusion (the Heart Hormone Study). J. Cardiovasc. Electrophysiol. 2022, 33, 2064–2071. [Google Scholar] [CrossRef]
- Dar, T.; Afzal, M.R.; Yarlagadda, B.; Kutty, S.; Shang, Q.; Gunda, S.; Samanta, A.; Thummaluru, J.; Arukala, K.S.; Kanmanthareddy, A.; et al. Mechanical Function of the Left Atrium Is Improved with Epicardial Ligation of the Left Atrial Appendage: Insights from the LAFIT-LARIAT Registry. Heart Rhythm. 2018, 15, 955–959. [Google Scholar] [CrossRef]
- Fanton, Y.; Robic, B.; Rummens, J.-L.; Daniëls, A.; Windmolders, S.; Willems, L.; Jamaer, L.; Dubois, J.; Bijnens, E.; Heuts, N.; et al. Cardiac Atrial Appendage Stem Cells Engraft and Differentiate into Cardiomyocytes in Vivo: A New Tool for Cardiac Repair after MI. Int. J. Cardiol. 2015, 201, 10–19. [Google Scholar] [CrossRef]
- Krul, S.P.J.; Berger, W.R.; Smit, N.W.; van Amersfoorth, S.C.M.; Driessen, A.H.G.; van Boven, W.J.; Fiolet, J.W.T.; van Ginneken, A.C.G.; van der Wal, A.C.; de Bakker, J.M.T.; et al. Atrial Fibrosis and Conduction Slowing in the Left Atrial Appendage of Patients Undergoing Thoracoscopic Surgical Pulmonary Vein Isolation for Atrial Fibrillation. Circ. Arrhythm. Electrophysiol. 2015, 8, 288–295. [Google Scholar] [CrossRef]
- Nesapiragasan, V.; Hayıroğlu, M.İ.; Sciacca, V.; Sommer, P.; Sohns, C.; Fink, T. Catheter Ablation Approaches for the Treatment of Arrhythmia Recurrence in Patients with a Durable Pulmonary Vein Isolation. Balkan Med. J. 2023, 40, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Bartus, K.; Litwinowicz, R.; Natorska, J.; Zabczyk, M.; Undas, A.; Kapelak, B.; Lakkireddy, D.; Lee, R.J. Coagulation Factors and Fibrinolytic Activity in the Left Atrial Appendage and Other Heart Chambers in Patients with Atrial Fibrillation: Is There a Local Intracardiac Prothrombotic State? (HEART-CLOT Study). Int. J. Cardiol. 2020, 301, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Janga, P.; Pamulapati, H.; Kanmanthareddy, A.; Vallakati, A.; Gunda, S.; Bommana, S.; Jaeger, M.; Yeruva, M.R.; Lakkireddy, D. State of the Art in Left Atrial Appendage Ligation—The Lariat. J. Atr. Fibrillation 2014, 7, 1073. [Google Scholar] [PubMed]
- Ren, Z.; Zheng, Y.; Zhang, J.; Yang, H.; Wu, J.; Li, H.; Guo, R.; Meng, W.; Zhang, J.; Sun, H.; et al. Patients with Larger Left Atrial Appendage Orifice Presented Worse Prognosis Contributed by Acute Heart Failure after Left Atrial Appendage Closure. J. Am. Heart Assoc. 2022, 11, e026309. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.; Shapiro, A.D. Plasminogen Deficiency. Haemophilia 2008, 14, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Della-Morte, D.; Pacifici, F.; Ricordi, C.; Massoud, R.; Rovella, V.; Proietti, S.; Iozzo, M.; Lauro, D.; Bernardini, S.; Bonassi, S.; et al. Low Level of Plasminogen Increases Risk for Mortality in COVID-19 Patients. Cell Death Dis. 2021, 12, 773. [Google Scholar] [CrossRef]
- Jung, R.G.; Motazedian, P.; Ramirez, F.D.; Simard, T.; Di Santo, P.; Visintini, S.; Faraz, M.A.; Labinaz, A.; Jung, Y.; Hibbert, B. Association between Plasminogen Activator Inhibitor-1 and Cardiovascular Events: A Systematic Review and Meta-Analysis. Thromb. J. 2018, 16, 12. [Google Scholar] [CrossRef]
- Slodowska, K.M.; Batko, J.; Holda, J.P.; Dudkiewicz, D.; Koziej, M.; Litwinowicz, R.; Bartus, K.; Holda, M.K. Morphometrical Features of Left Atrial Appendage in the AF Patients Subjected to Left Atrial Appendage Closure. Folia Morphol. 2023, 82, 814–821. [Google Scholar] [CrossRef]
- Keragala, C.B.; Medcalf, R.L. Plasminogen: An Enigmatic Zymogen. Blood 2021, 137, 2881–2889. [Google Scholar] [CrossRef]
- Sillen, M.; Declerck, P.J. Thrombin Activatable Fibrinolysis Inhibitor (TAFI): An Updated Narrative Review. Int. J. Mol. Sci. 2021, 22, 3670. [Google Scholar] [CrossRef]
- Jilani, T.N.; Siddiqui, A.H. Tissue Plasminogen Activator. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Cesari, M.; Pahor, M.; Incalzi, R.A. Plasminogen Activator Inhibitor-1 (PAI-1): A Key Factor Linking Fibrinolysis and Age-Related Subclinical and Clinical Conditions. Cardiovasc. Ther. 2010, 28, e72–e91. [Google Scholar] [CrossRef] [PubMed]
- Veinot, J.P.; Harrity, P.J.; Gentile, F.; Khandheria, B.K.; Bailey, K.R.; Eickholt, J.T.; Seward, J.B.; Tajik, A.J.; Edwards, W.D. Anatomy of the Normal Left Atrial Appendage. Circulation 1997, 96, 3112–3115. [Google Scholar] [CrossRef] [PubMed]
- Batko, J.; Jakiel, R.; Krawczyk–Ożóg, A.; Litwinowicz, R.; Hołda, J.; Bartuś, S.; Bartuś, K.; Hołda, M.K.; Konieczyńska, M. Definition and Anatomical Description of the Left Atrial Appendage Neck. Clin. Anat. 2023, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Green, C.E.; Kelley, M.J.; Higgins, C.B. Etiologic Significance of Enlargement of the Left Atrial Appendage in Adults. Radiology 1982, 142, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Kelley, M.J.; Elliott, L.P.; Shulman, S.T.; Ayoub, E.M.; Victorica, B.E.; Gessner, I.H. The Significance of the Left Atrial Appendage in Rheumatic Heart Disease. Circulation 1976, 54, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Di Biase, L.; Horton, R.P.; Nguyen, T.; Morhanty, P.; Natale, A. Left Atrial Appendage Studied by Computed Tomography to Help Planning for Appendage Closure Device Placement. J. Cardiovasc. Electrophysiol. 2010, 21, 973–982. [Google Scholar] [CrossRef]
- Sherwood, M.; Bliden, K.P.; Ilkhanoff, L.; Venkataraman, G.; Strickberger, A.; Yazdani, S.; McSwain, R.; Rashid, H.; Navarese, E.P.; Plummer, T.; et al. Detailed Thrombogenicity Phenotyping and 1 Year Outcomes in Patients Undergoing WATCHMAN Implantation: (TARGET-WATCHMAN) a Case–Control Study. J. Thromb. Thrombolysis 2020, 50, 484–498. [Google Scholar] [CrossRef]
- Asmarats, L.; O’Hara, G.; Champagne, J.; Paradis, J.-M.; Bernier, M.; O’Connor, K.; Beaudoin, J.; Junquera, L.; Del Val, D.; Muntané-Carol, G.; et al. Short-Term Oral Anticoagulation Versus Antiplatelet Therapy Following Transcatheter Left Atrial Appendage Closure. Circ. Cardiovasc. Interv. 2020, 13, e009039. [Google Scholar] [CrossRef]
- Duthoit, G.; Silvain, J.; Marijon, E.; Ducrocq, G.; Lepillier, A.; Frere, C.; Dimby, S.-F.; Popovic, B.; Lellouche, N.; Martin-Toutain, I.; et al. Reduced Rivaroxaban Dose Versus Dual Antiplatelet Therapy After Left Atrial Appendage Closure. Circ. Cardiovasc. Interv. 2020, 13, e008481. [Google Scholar] [CrossRef]
| Normal LAA Body | Enlarged LAA Body | p | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| LAA Width [mm] | 16.7 ± 2.8 | 26.5 ± 6.9 | <0.001 |
| LAA Length [mm] | 44.5 ± 10.9 | 49.6 ± 9.0 | 0.116 |
| LAA body index [mm2] | 727.1 ± 146 | 1324.5 ± 480.2 | <0.001 |
| Ostium transverse dimension [mm] | 24.1 ± 5.2 | 32.1 ± 4.3 | 0.001 |
| ostium longitudinal dimension [mm] | 20.3 ± 4.3 | 25.8 ± 6.1 | 0.034 |
| LAA ostium area [mm2] | 398.3 ± 164.9 | 666.7 ± 240.0 | 0.010 |
| LAA origin angle to LA [º] | 64.8 ± 24.6 | 75.2 ± 9.5 | 0.748 |
| Normal LAA Body | Enlarged LAA Body | |||||
|---|---|---|---|---|---|---|
| Baseline (Mean ± SD) | 6-Month Follow-Up (Mean ± SD) | Baseline vs. 6-Month Follow-Up p | Baseline (Mean ± SD) | 6-Month Follow-Up (Mean ± SD) | Baseline vs. 6-Month Follow-Up p | |
| Plasminogen (%) | 109.1 ± 30 | 97.7 ± 14.6 | 0.181 | 89.5 ± 12.0 | 105.2 ± 14.6 | 0.007 |
| Fibrinogen g/L | 4.4 ± 0.9 | 2.9 ± 0.8 | 0.020 | 3.9 ± 0.9 | 2.6 ± 0.7 | 0.003 |
| tPA conc. (ng/mL) | 10.6 ± 3.6 | 5.8 ± 2.1 | 0.003 | 10.5 ± 6.8 | 6.8 ± 4.9 | 0.007 |
| PAI-1 (ng/mL) | 3.8 ± 2.6 | 2.3 ± 1.5 | 0.003 | 4.9 ± 3.1 | 2.3 ± 1.5 | 0.007 |
| TAFI (%) | 101.1 ± 12.2 | 82.7 ± 12.5 | 0.003 | 105.2 ± 19.6 | 96 ± 17.6 | 0.108 |
| Normal LAA Orifice | Enlarged LAA Orifice | p | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| LAA Width [mm] | 19.1 ± 5.6 | 24.2 ± 7.9 | 0.116 |
| LAA Length [mm] | 43.1 ± 11.1 | 51.0 ± 7.6 | 0.034 |
| LAA body index [mm2] | 791.6 ± 207.5 | 1260 ± 533.3 | 0.016 |
| Ostium transverse dimension [mm] | 23.7 ± 4.6 | 32.6 ± 4.2 | <0.001 |
| ostium longitudinal dimension [mm] | 18.2 ± 1.6 | 27.8 ± 4.4 | <0.001 |
| LAA ostium area [mm2] | 344.0 ± 93.8 | 720.9 ± 193.7 | <0.001 |
| LAA origin angle to LA [º] | 66.9 ± 26.3 | 73.1 ± 6.7 | 0.300 |
| Normal LAA Orifice | Enlarged LAA Orifice | |||||
|---|---|---|---|---|---|---|
| Baseline (Mean ± SD) | 6-Month Follow-Up (Mean ± SD) | Baseline vs. 6-Month Follow-Up p | Baseline (Mean ± SD) | 6-Month Follow-Up (Mean ± SD) | Baseline vs. 6-Month Follow-Up p | |
| Plasminogen (%) | 111.9 ± 28.3 | 103.1 ± 9.9 | 0.422 | 86.7 ± 10.3 | 99.8 ± 18.9 | 0.007 |
| Fibrinogen g/L | 4.2 ± 0.9 | 2.7 ± 0.8 | 0.003 | 4.0 ± 0.8 | 2.8 ± 0.8 | 0.020 |
| tPA conc. (ng/mL) | 9.4 ± 1.3 | 5.6 ± 1.1 | 0.004 | 11.6 ± 7.4 | 7 ± 5.2 | 0.006 |
| PAI-1 (ng/mL) | 4.5 ± 3.4 | 2.2 ± 1.6 | 0.007 | 4.2 ± 2.3 | 2.4 ± 1.4 | 0.003 |
| TAFI (%) | 104.2 ± 13.4 | 80.2 ± 11.5 | 0.003 | 102 ± 19.0 | 98.4 ± 15.7 | 0.284 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batko, J.; Rusinek, J.; Słomka, A.; Litwinowicz, R.; Burysz, M.; Bartuś, M.; Lakkireddy, D.R.; Lee, R.J.; Natorska, J.; Ząbczyk, M.; et al. Postoperative Coagulation Changes in Patients after Epicardial Left Atrial Appendage Occlusion Varies Based on the Left Atrial Appendage Size. Diseases 2024, 12, 8. https://doi.org/10.3390/diseases12010008
Batko J, Rusinek J, Słomka A, Litwinowicz R, Burysz M, Bartuś M, Lakkireddy DR, Lee RJ, Natorska J, Ząbczyk M, et al. Postoperative Coagulation Changes in Patients after Epicardial Left Atrial Appendage Occlusion Varies Based on the Left Atrial Appendage Size. Diseases. 2024; 12(1):8. https://doi.org/10.3390/diseases12010008
Chicago/Turabian StyleBatko, Jakub, Jakub Rusinek, Artur Słomka, Radosław Litwinowicz, Marian Burysz, Magdalena Bartuś, Dhanunjaya R. Lakkireddy, Randall J. Lee, Joanna Natorska, Michał Ząbczyk, and et al. 2024. "Postoperative Coagulation Changes in Patients after Epicardial Left Atrial Appendage Occlusion Varies Based on the Left Atrial Appendage Size" Diseases 12, no. 1: 8. https://doi.org/10.3390/diseases12010008
APA StyleBatko, J., Rusinek, J., Słomka, A., Litwinowicz, R., Burysz, M., Bartuś, M., Lakkireddy, D. R., Lee, R. J., Natorska, J., Ząbczyk, M., Kapelak, B., & Bartuś, K. (2024). Postoperative Coagulation Changes in Patients after Epicardial Left Atrial Appendage Occlusion Varies Based on the Left Atrial Appendage Size. Diseases, 12(1), 8. https://doi.org/10.3390/diseases12010008