

Progress and Perspectives in Colon Cancer Pathology, Diagnosis, and Treatments




Abstract
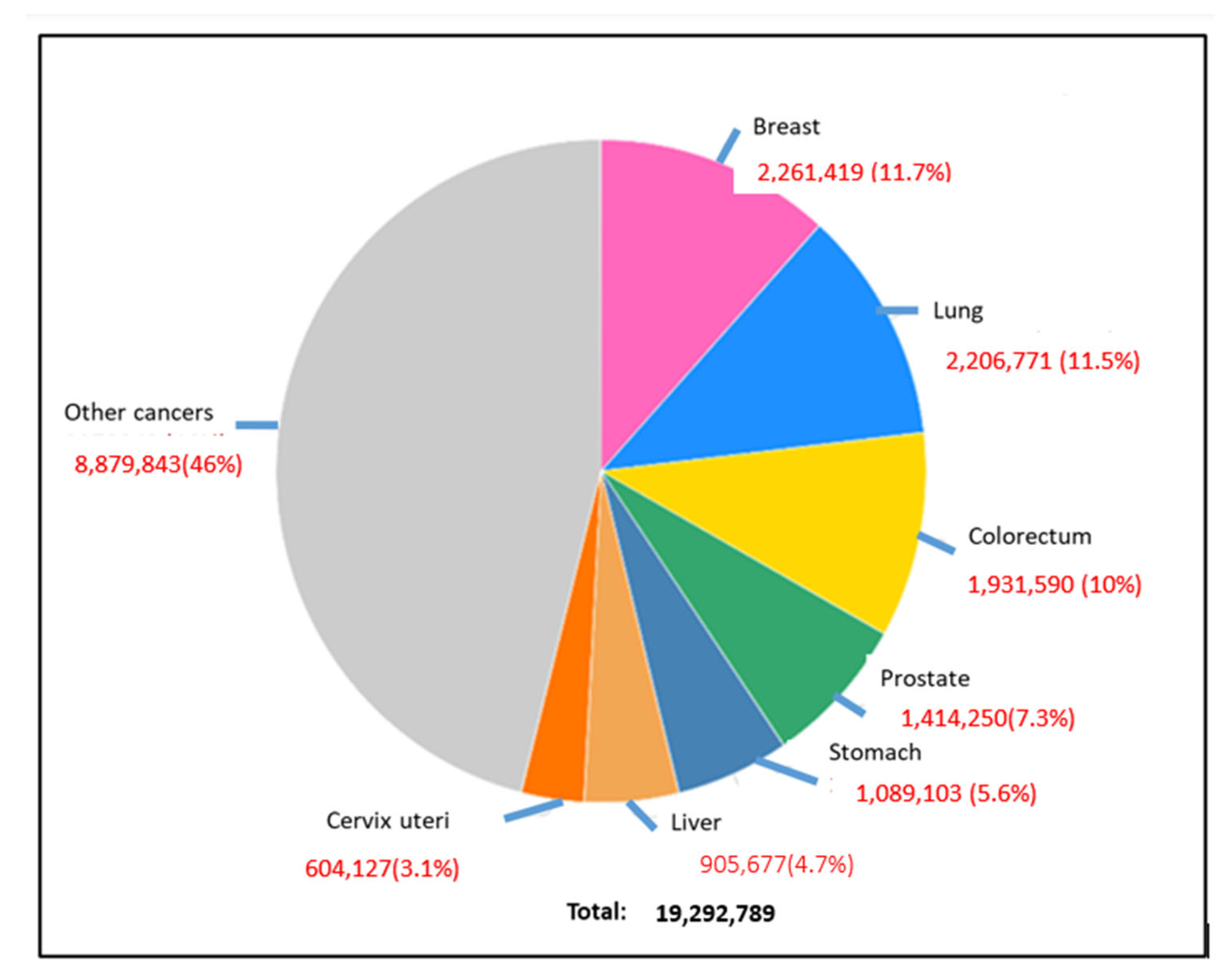
:1. Introduction
2. Risk Factors for CRC Development
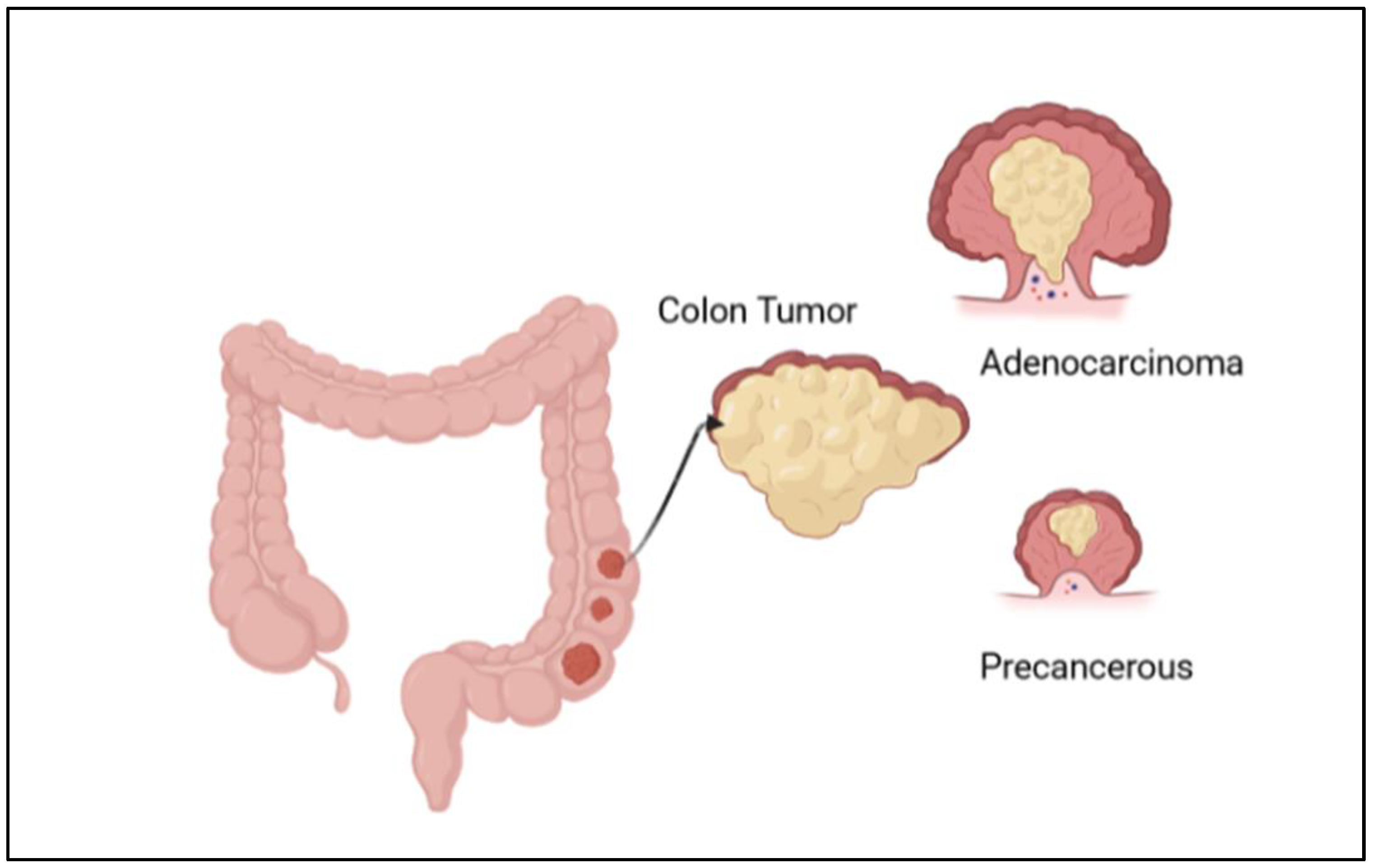
3. Developmental Stages of CRC
4. Diagnostic Strategies for CRC
4.1. Symptoms of CRC
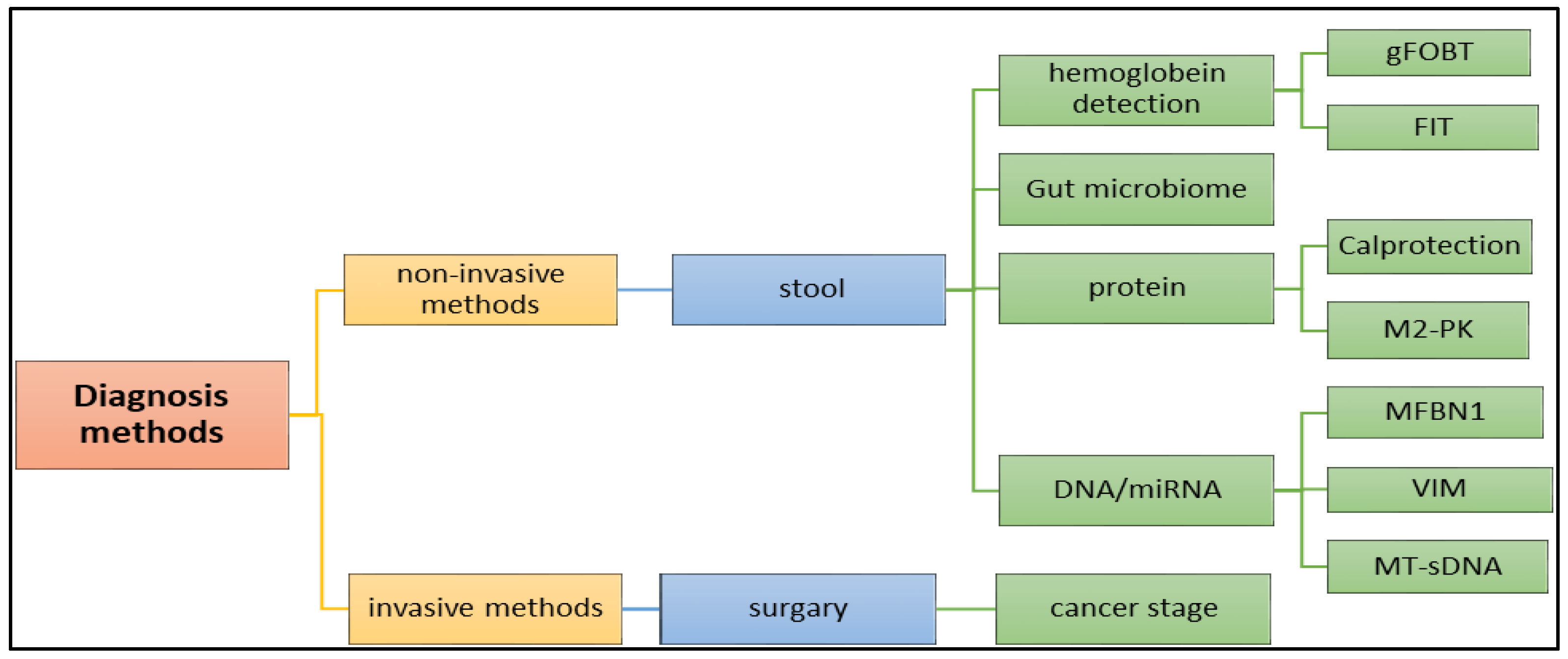
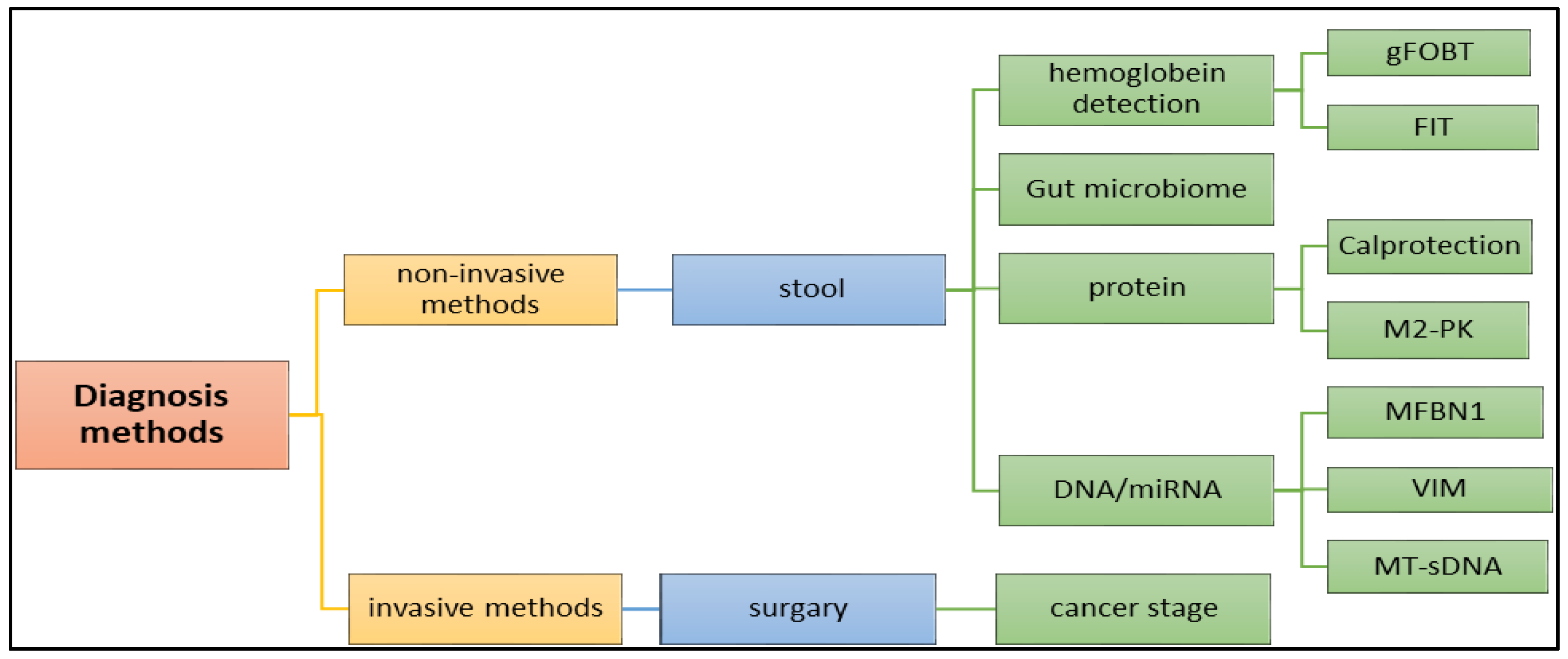
4.2. Methods of CRC Diagnosis
4.2.1. Biochemical and Molecular Biomarkers
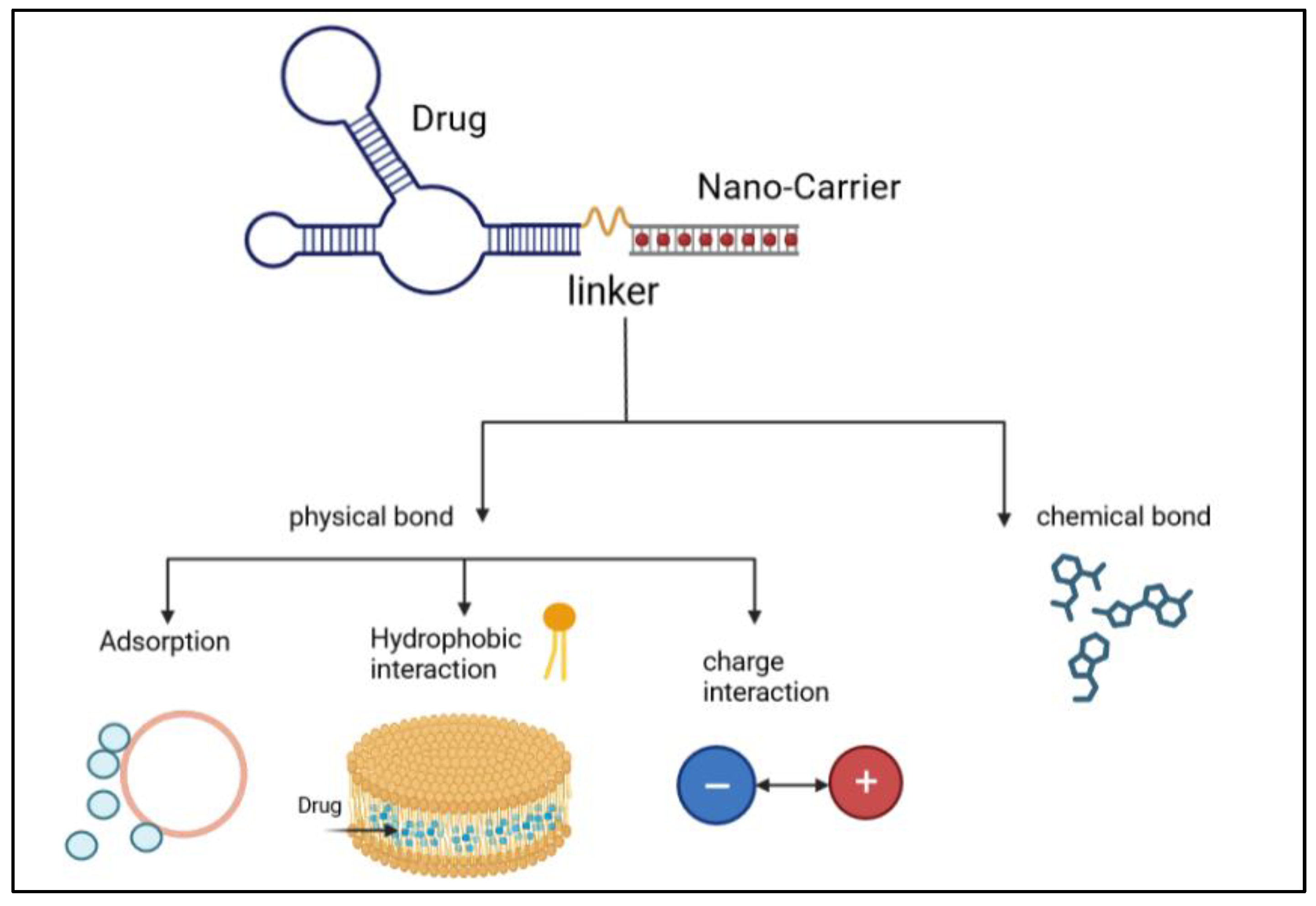
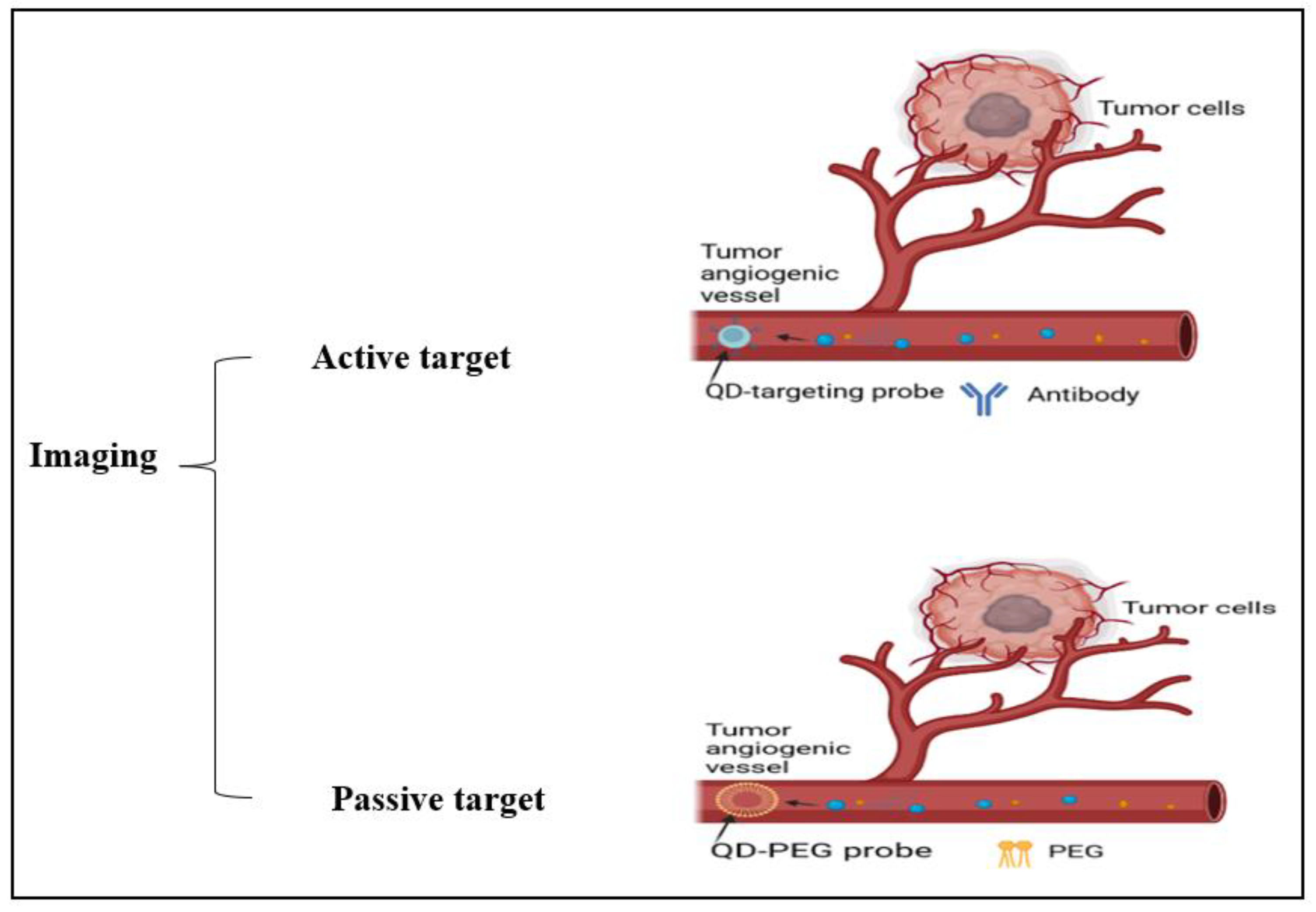
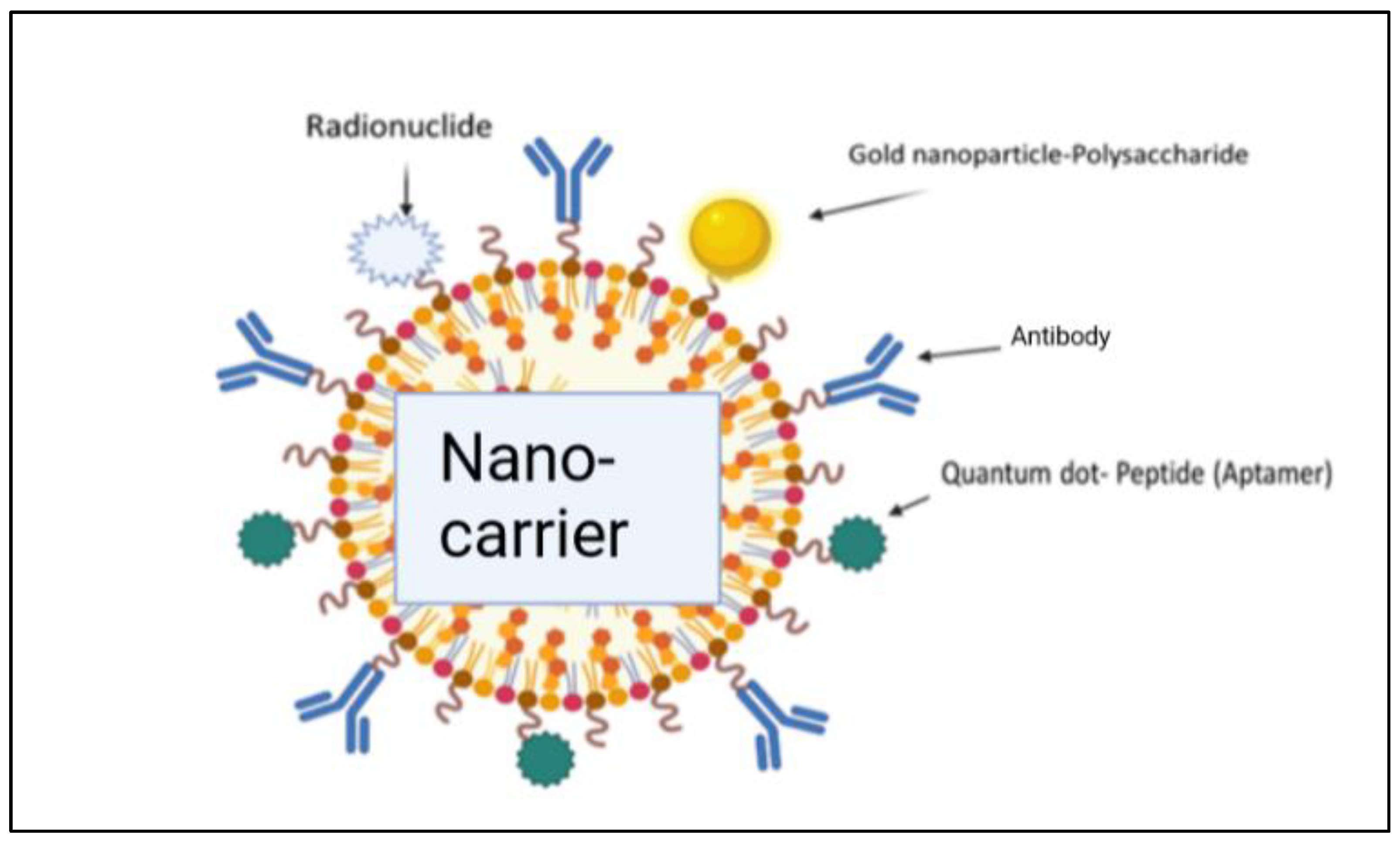
4.2.2. CRC Diagnosis via the Nano-Molecular Approach
4.2.3. Chromosomal Biomarkers for CRC
4.2.4. Fecal Metagenomics
4.3. Other Biomarkers
4.4. Imaging
4.5. Colonoscopy
4.6. Capsule Endoscopy
4.7. CT Colonography
4.8. The Multi-Target Stool DNA Test
4.9. Diagnostic Strategy in Colorectal Cancer
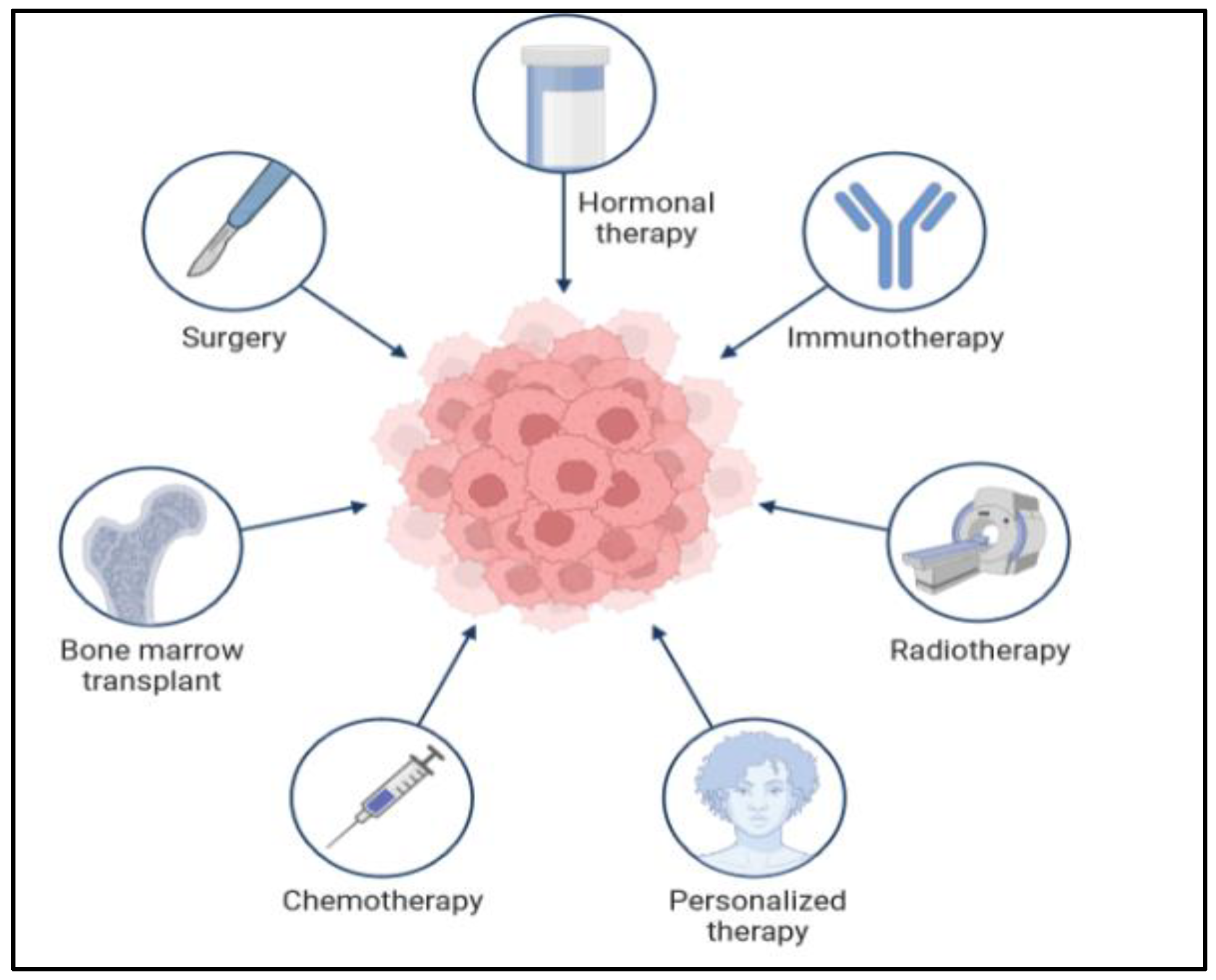
5. Cancer Treatments
5.1. Colon Surgery
5.2. Chemotherapy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nanoparticles | Active Molecules | Application | Result | References |
|---|---|---|---|---|
| Mesoporous silica (MSN) | 5-fluorouracil (5-FU) | Oral treatment of colon cancer | Better targeting of colon cancer cells | [47] |
| Dextran sulphate sodium | 17-AAG | Orally administrated NP-PEG-FA/17-AAG | Better cancer therapy while reducing systemic exposure | [48] |
| Liposomes, cyclodextrin, nano gels, AuNPs, polymers, lipids, and micelles | Curcumin | Applied to colon cancer cell C26, HCT116 | Enhances the internalization to inhibit tumor progression | [2] |
| Liposome-mesoporous silica NPs, lipid-core nanocapsules, and AuNPs | Resveratrol | CRC cells | Better cancer cell internalization and penetration | |
| PEGylated silica NPs | Genistein | CRC cells | Better anticancer activity |
5.3. The Targeted Therapies for CRC
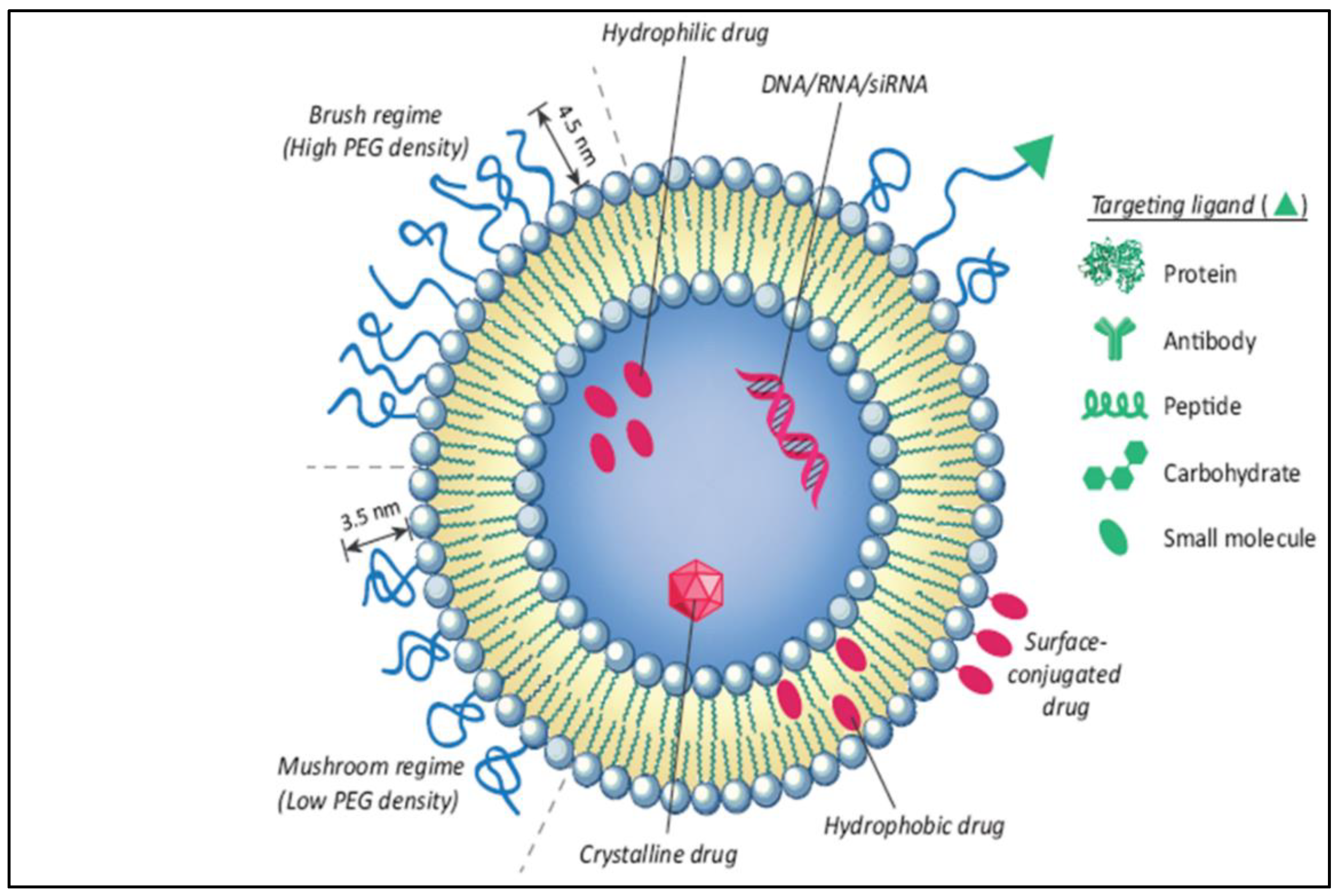
5.4. Application of Phototherapeutic-Based Nanoparticles in Colorectal Cancer
5.5. Female Hormones: Prospective Avenues for CRC as a Nano Therapy
5.6. Adjuvant Therapy and Neoadjuvant Therapy in Cancer
5.7. Future Prospects of Colorectal Treatment
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Olovo, C.V.; Huang, X.; Zheng, X. Faecal microbial biomarkers in early diagnosis of colorectal cancer. J. Cell. Mol. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Pavitra, E.; Dariya, B.; Srivani, G.; Kang, S.M.; Alam, A.; Sudhir, P.R.; Kamal, M.A.; Raju, G.S.R.; Han, Y.K.; Lakkakula, B.V.K.S.; et al. Engineered nanoparticles for imaging and drug delivery in colorectal cancer. Semin. Cancer Biol. 2021. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer (IARC-WHO) Cancer Today. Data visualization Tools for Exploring the Global Cancer Burden in 2020. Available online: https://gco.iarc.fr/today/ (accessed on 30 July 2023).
- Yu, J.; Zhang, J.; Peng, T.; Fei, Z.; Jin, L.; Yang, M. Predictive Value of Circulating Tumor Cells in Prognosis of Stage III/IV Colorectal Cancer after Oxaliplatin-based First-line Chemotherapy. In Vivo 2022, 36, 806–813. [Google Scholar] [CrossRef] [PubMed]
- The American Cancer Society Medical and Editorial Content Team (ACSMECT). American Cancer Society. Cancer.Org. Available online: https://www.cancer.org/cancer/colon-rectal-cancer/causes-risks-prevention/risk-factors.html (accessed on 29 June 2020).
- O’Connell, J.B.; Maggard, M.A.; Ko, C.Y. Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J. Natl. Cancer Inst. 2004, 96, 1420–1425. [Google Scholar] [CrossRef] [PubMed]
- Alana Biggers, M.M.B. Signs and Symptoms of Colon Cancer (Also Known as Colorectal Cancer); Healthline: San Francisco, CA, USA, 2021. [Google Scholar]
- Noone, A.M.; Howlader, N.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. SEER Cancer Statistics Review (CSR) 1975–2015; National Cancer Institute: Bethesda, MD, USA, 2019. Available online: https://seer.cancer.gov/archive/csr/1975_2017/ (accessed on 30 July 2023).
- Sawicki, T.; Ruszkowska, M.; Danielewicz, A.; Niedźwiedzka, E.; Arłukowicz, T.; Przybyłowicz, K.E. A Review of Colorectal Cancer in Terms of Epidemiology, Risk Factors, Development, Symptoms and Diagnosis. Cancers 2021, 13, 2025. [Google Scholar] [CrossRef]
- Shin, A.; Joo, J.; Bak, J.; Yang, H.R.; Kim, J.; Park, S.; Nam, B.H. Site-specific risk factors for colorectal cancer in a Korean population. PLoS ONE 2011, 6, e23196. [Google Scholar] [CrossRef] [PubMed]
- Chung, I.-M.; Subramanian, U.; Thirupathi, P.; Venkidasamy, B.; Samynathan, R.; Gangadhar, B.H.; Rajakumar, G.; Thiruvengadam, M. Resveratrol nanoparticles: A promising therapeutic advancement over native resveratrol. Processes 2020, 8, 458. [Google Scholar] [CrossRef]
- Board Cancer Net Editorial. Cancer.Net. Knowledge Conquers Cancer. 2022. Available online: https://www.cancer.net/cancer-types/colorectal-cancer/stages (accessed on 28 July 2023).
- Haraldsdottir, S.; Einarsdottir, H.M.; Smaradottir, A.; Gunnlaugsson, A.; Halfdanarson, T.R. Krabbamein í ristli og endaþarmi [Colorectal cancer—review]. Laeknabladid 2014, 100, 75–82. (In Icelandic) [Google Scholar] [CrossRef]
- Howlader, N.; Noone, A.M.; Krapcho, M.; Neyman, N.; Aminou, R.; Waldron, W.; Altekruse, S.F.; Kosary, C.L.; Ruhl, J.; Tatalovich, Z.; et al. SEER Cancer Statistics Review, 1975–2009 (Vintage 2009 Populations); National Cancer Institute: Bethesda, MD, USA, 2012. Available online: https://seer.cancer.gov/csr/1975_2009_pops09/ (accessed on 28 July 2023).
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2012. CA Cancer J. Clin. 2012, 62, 10–29. [Google Scholar] [CrossRef]
- Alexiusdottir, K.K.; Möller, P.H.; Snaebjornsson, P.; Jonasson, L.; Olafsdottir, E.J.; Björnsson, E.S.; Tryggvadottir, L.; Jonasson, J.G. Association of symptoms of colon cancer patients with tumor location and TNM tumor stage. Scand. J. Gastroenterol. 2012, 47, 795–801. [Google Scholar] [CrossRef]
- Winawer, S.J.; Zauber, A.G.; Gerdes, H.; O’Brien, M.J.; Gottlieb, L.S.; Sternberg, S.S.; Bond, J.H.; Waye, J.D.; Schapiro, M.; Panish, J.F.; et al. Risk of colorectal cancer in the families of patients with adenomatous polyps. N. Engl. J. Med. 1996, 334, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Atkin, W.S.; Morson, B.C.; Cuzick, J. Long-term risk of colorectal cancer after excision of rectosigmoid adenomas. N. Engl. J. Med. 1992, 326, 658–662. [Google Scholar] [CrossRef] [PubMed]
- Farraye, F.A.; Odze, R.D.; Eaden, J.; Itzkowitz, S.H. AGA technical review on the diagnosis and management of colorectal neoplasia in inflammatory bowel disease. Gastroenterology 2010, 138, 746–774. [Google Scholar] [CrossRef] [PubMed]
- Botteri, E.; Iodice, S.; Bagnardi, V.; Raimondi, S.; Lowenfels, A.B.; Maisonneuve, P. Smoking and colorectal cancer: A meta-analysis. JAMA 2008, 300, 2765–2778. [Google Scholar] [CrossRef]
- Botteri, E.; Støer, N.C.; Sakshaug, S.; Graff-Iversen, S.; Vangen, S.; Hofvind, S.; de Lange, T.; Bagnardi, V.; Ursin, G.; Weiderpass, E. Menopausal hormone therapy and colorectal cancer: A linkage between nationwide registries in Norway. BMJ Open 2017, 7, e017639. [Google Scholar] [CrossRef]
- Rothwell, P.M.; Wilson, M.; Price, J.F.; Belch, J.F.; Meade, T.W.; Mehta, Z. Effect of daily aspirin on risk of cancer metastasis: A study of incident cancers during randomized controlled trials. Lancet 2012, 379, 1591–1601. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Leitzmann, M.F.; Subar, A.F.; Hollenbeck, A.; Schatzkin, A. Dairy food, calcium, and risk of cancer in the NIH-AARP Diet and Health Study. Arch. Intern. Med. 2009, 169, 391–401. [Google Scholar] [CrossRef]
- Selchick, F. MaryAnn De Pietro, CRT; Healthline: San Francisco, CA, USA, 2022; Available online: https://www.healthline.com/health/colorectal-cancer/stages-of-colon-cancer (accessed on 28 July 2023).
- Villéger, R.; Lopès, A.; Veziant, J.; Gagnière, J.; Barnich, N.; Billard, E.; Boucher, D.; Bonnet, M. Microbial markers in colorectal cancer detection and/or prognosis. World J. Gastroenterol. 2018, 24, 2327. [Google Scholar] [CrossRef]
- Zygulska, A.L.; Pierzchalski, P. Novel Diagnostic Biomarkers in Colorectal Cancer. Int. J. Mol. Sci. 2022, 23, 852. [Google Scholar] [CrossRef]
- Lech, G.; Słotwiński, R.; Słodkowski, M.; Krasnodębski, I.W. Colorectal cancer tumour markers and biomarkers: Recent therapeutic advances. World J. Gastroenterol. 2016, 22, 1745–1755. [Google Scholar] [CrossRef]
- Shajari, E.; Mollasalehi, H. Ribonucleic-acid-biomarker candidates for early-phase group detection of common cancers. Genomics 2020, 112, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Bresalier, R.S.; Grady, W.M.; Markowitz, S.D.; Nielsen, H.J.; Batra, S.K.; Lampe, P.D. Biomarkers for Early Detection of Colorectal Cancer: The Early Detection Research Network, a Framework for Clinical Translation. Cancer Epidemiol. Biomark. Prev. 2020, 29, 2431–2440. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Verma, M.; Henson, D.E. Biomarkers for Early Detection of Colon Cancer. Clin. Cancer Res. 2001, 7, 1118–1126. [Google Scholar] [PubMed]
- Kim, V.N. MicroRNA biogenesis: Coordinated cropping and dicing. Nat. Rev. Mol. Cell Biol. 2005, 6, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Marcuello, M.; Vymetalkova, V.; Neves, R.P.L.; Duran-Sanchon, S.; Vedeld, H.M.; Tham, E.; Gironella, M. Circulating biomarkers for early detection and clinical management of colorectal cancer. Mol. Asp. Med. 2019, 69, 107–122. [Google Scholar] [CrossRef] [PubMed]
- Bartley, A.N.; Yao, H.; Barkoh, B.A.; Ivan, C.; Mishra, B.M.; Rashid, A.; Hamilton, S.R. Complex Patterns of Altered MicroRNA Expression during the Adenoma-Adenocarcinoma Sequence for Microsatellite-Stable Colorectal Cancer. Clin. Cancer Res. 2011, 17, 7283–7293. [Google Scholar] [CrossRef] [PubMed]
- Danese, E.; Montagnana, M.; Brentegani, C.; Lippi, G. Short-term stability of free metanephrines in plasma and whole blood. Clin. Chem. Lab. Med. 2020, 58, 753–757. [Google Scholar] [CrossRef]
- Ogino, S.; Nosho, K.; Irahara, N.; Shima, K.; Baba, Y.; Kirkner, G.J.; Fuchs, C.S. Prognostic Significance and Molecular Associations of 18q Loss of Heterozygosity: A Cohort Study of Microsatellite Stable Colorectal Cancers. J. Clin. Oncol. 2009, 27, 4591–4598. [Google Scholar] [CrossRef]
- Boyle, T.; Keegel, T.; Bull, F.; Heyworth, J.; Fritschi, L. Physical Activity and Risks of Proximal and Distal Colon Cancers: A Systematic Review and Meta-analysis. J. Natl. Cancer Inst. 2012, 104, 1548–1561. [Google Scholar] [CrossRef]
- Bahari, A. Characteristics of Fe3O4, α-Fe2O3, and γ-Fe2O3 Nanoparticles as Suitable Candidates in the Field of Nanomedicine. J. Supercond. Nov. Magn. 2017, 30, 2165–2174. [Google Scholar] [CrossRef]
- Li, X.; Liu, L.; Li, S.; Wan, Y.; Chen, J.-X.; Tian, S.; Huang, Z.; Xiao, Y.-F.; Cui, X.; Xiang, C.; et al. Biodegradable π-Conjugated Oligomer Nanoparticles with High Photothermal Conversion Efficiency for Cancer Theranostics. ACS Nano 2019, 13, 12901–12911. [Google Scholar] [CrossRef] [PubMed]
- Mayo Clinic Team. Mayo Foundation for Medical Education and Research (MFMER). 1998–2022. Myoclonic. Available online: https://www.mayoclinic.org/diseases-conditions/colon-cancer/symptoms-causes/syc-20353669 (accessed on 30 July 2023).
- Nakajima, F.; Furumatsu, Y.; Yurugi, T.; Amari, Y.; Iida, T.; Fukui, T.; Kuramoto, T. Investigation of small intestinal lesions in dialysis patients using capsule endoscopy. Hemodial. Int. 2019, 23, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Obaro, A.E.; Burling, D.N.; Plumb, A.A. Colon cancer screening with CT colonography: Logistics, cost-effectiveness, efficiency and progress. Br. J. Radiol. 2018, 91, 20180307. [Google Scholar] [CrossRef] [PubMed]
- Kleinschmidt, T.K.; Clements, A.; Parker, M.A.; Scarcliff, S.D. Retrospective Review of Multitarget Stool DNA as a Screening Test for Colorectal Cancer. Am. Surg. 2023, 89, 603–606. [Google Scholar] [CrossRef] [PubMed]
- Body, A.; Prenen, H.; Latham, S.; Lam, M.; Tipping-Smith, S.; Raghunath, A.; Segelov, E. The Role of Neoadjuvant Chemotherapy in Locally Advanced Colon Cancer. Cancer Manag. Res. 2021, 13, 2567–2579. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed]
- Ramos, E.K.; Hoffmann, A.D.; Gerson, S.L.; Liu, H. New opportunities and challenges to defeat cancer stem cells. Trends Cancer 2017, 3, 780–796. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Colorectal Cancer—Patient Version. Available online: https://www.cancer.gov/types/colorectal (accessed on 30 July 2023).
- Shi, J.; Ma, Z.; Pan, H.; Liu, Y.; Chu, Y.; Wang, J.; Chen, L. Biofilm-encapsulated nano drug delivery system for the treatment of colon cancer. J. Microencapsul. 2020, 37, 481–491. [Google Scholar] [CrossRef]
- Yang, M.; Zhang, F.; Yang, C.; Wang, L.; Sung, J.; Garg, P.; Zhang, M.; Merlin, D. Oral Targeted Delivery by Nanoparticles Enhances Efficacy of an Hsp90 Inhibitor by Reducing Systemic Exposure in Murine Models of Colitis and Colitis-Associated Cancer. J. Crohns Colitis 2020, 14, 130–141. [Google Scholar] [CrossRef]
- Gangane, N.M. Chapter 13—Nanotherapeutics for colon cancer. In Photophysics and Nanophysics in Therapeutics; Gangane, N.M., Ed.; Elsevier: Amsterdam, The Netherlands, 2022; pp. 251–268. [Google Scholar]
- Koushki, M.; Amiri-Dashatan, N.; Ahmadi, N.; Abbaszadeh, H.; Rezaei-Tavirani, M. Resveratrol: A miraculous natural compound for diseases treatment. Food Sci. Nutr. 2018, 6, 2473–2490. [Google Scholar] [CrossRef]
- Ji, J.; Sundquist, J.; Sundquist, K. Use of hormone replacement therapy improves the prognosis in patients with colorectal cancer: A population-based study in Sweden. Int. J. Cancer 2018, 142, 2003–2010. [Google Scholar] [CrossRef] [PubMed]
- Bhaskara, V.K.; Mittal, B.; Mysorekar, V.V.; Amaresh, N.; Simal-Gandara, J. Resveratrol, cancer and cancer stem cells: A review on past to future. Curr. Res. Food Sci. 2020, 3, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.; Zhou, M.; Huang, D.; Wasan, H.S.; Zhang, K.; Sun, L.; Huang, H.; Ma, S.; Shen, M.; Ruan, S. Resveratrol inhibits the invasion and metastasis of colon cancer through reversal of epithelial mesenchymal transition via the AKT/GSK3β/Snail signaling pathway. Mol. Med. Rep. 2019, 20, 2783–2795. [Google Scholar] [PubMed]
- Li, D.; Wang, G.; Jin, G.; Yao, K.; Zhao, Z.; Bie, L.; Guo, Y.; Li, N.; Deng, W.; Chen, X.; et al. Resveratrol suppresses colon cancer growth by targeting the AKT/STAT3 signaling pathway. Int. J. Mol. Med. 2019, 43, 630–640. [Google Scholar] [CrossRef] [PubMed]
- Sharifi-Rad, J.; Quispe, C.; Mukazhanova, Z.; Knut, E.; Turgumbayeva, A.; Kipchakbayeva, A.; Seitimova, G.; Mahomoodally, M.F.; Lobine, D.; Koay, A.; et al. Resveratrol-based nanoformulations as an emerging therapeutic strategy for cancer. Front. Mol. Biosci. 2021, 8, 649395. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, Z.; Mohammadinejad, R.; Ashrafizadeh, M. Drug delivery systems for resveratrol, a non-flavonoid polyphenol: Emerging evidence in last decades. J. Drug Deliv. Sci. Technol. 2019, 51, 591–604. [Google Scholar] [CrossRef]
- Yingchoncharoen, P.; Kalinowski, D.S.; Richardson, D.R. Lipid-based drug delivery systems in cancer therapy: What is available and what is yet to come. Pharmacol. Rev. 2016, 68, 701–787. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Su, K.; Sun, X.; Jiang, Y.; Wang, L.; Hu, C.; Zhang, C.; Lu, M.; Du, X.; Xing, B. Sec62 promotes stemness and chemoresistance of human colorectal cancer through activating Wnt/β-catenin pathway. J. Exp. Clin. Cancer Res. 2021, 40, 132. [Google Scholar] [CrossRef]
- Shen, C.; Wang, D.; Liu, X.; Gu, B.; Du, Y.; Song, B.; Lu, X.; Yang, Q.; Zhu, Q.; Hou, T.; et al. SET7/9 regulates cancer cell proliferation by influencing beta-catenin stability. FASEB J. 2015, 29, 4313–4323. [Google Scholar] [CrossRef]
- Çağdaş, M.; Sezer, A.D.; Bucak, S. Liposomes as Potential Drug Carrier Systems for Drug Delivery. Appl. Nanotechnol. Drug Deliv. 2014, 1, 1–50. [Google Scholar] [CrossRef]
- Zhang, P.; Hu, C.; Ran, W.; Meng, J.; Yin, Q.; Li, Y. Recent Progress in Light-Triggered Nanotheranostics for Cancer Treatment Theranostics. Theranostics 2016, 6, 948. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Wang, C.; Jiang, X.; Wei, Y.; Wang, Q.; Cui, K.; Xu, X.; Wang, F.; Zhang, L. Application of phototherapeutic-based nanoparticles in colorectal cancer. Int. J. Biol. Sci. 2021, 17, 1361. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zeng, Z.; Huang, L.; Luo, S.; Dong, J.; Zhou, F.H.; Zhou, K.; Wang, L.; Kang, L. Photothermal therapy technology of metastatic colorectal cancer. Am. J. Transl. Res. 2020, 12, 3089–3115. [Google Scholar] [PubMed]
- Xie, X.; Li, Z.; Zhang, Y.; Guo, S.; Pendharkar, A.I.; Lu, M.; Huang, L.; Huang, W.; Han, G. Emerging ≈ 800 nm Excited Lanthanide-Doped Upconversion Nanoparticles. Small 2017, 13, 1602843. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.M.; Oleinick, N.L. Dissociation of mitochondrial depolarization from cytochrome c release during apoptosis induced by photodynamic therapy. Br. J. Cancer 2001, 84, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- Barge, J.; Decréau, R.; Julliard, M.; Hubaud, J.; Sabatier, A.; Grob, J.; Verrando, P. Killing efficacy of a new silicon phthalocyanine in human melanoma cells treated with photodynamic therapy by early activation of mitochondrion-mediated apoptosis. Exp. Dermatol. 2004, 13, 33–44. [Google Scholar] [CrossRef]
- Chiu, S.-M.; Xue, L.-Y.; Lam, M.; Rodriguez, M.E.; Zhang, P.; Kenney, M.E.; Nieminen, A.-L.; Oleinick, N.L. A requirement for bid for induction of apoptosis by photodynamic therapy with a lysosome- but not a mitochondrion-targeted photosensitizer. Photochem. Photobiol. 2010, 86, 1161–1173. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.; Ding, L.; Xu, H.J.; Shen, Z.; Ju, H.; Jia, L.; Yu, J.S. Cell-specific and pH-activatable rubyrin-loaded nanoparticles for highly selective near-infrared photodynamic therapy against cancer. J. Am. Chem. Soc. 2013, 135, 18850–18858. [Google Scholar] [CrossRef]
- Igney, F.H.; Krammer, P.H. Death and anti-death: Tumour resistance to apoptosis. Nat. Rev. Cancer 2002, 2, 277–288. [Google Scholar] [CrossRef]
- Mori, M.; Kuroda, T.; Obana, A.; Sakata, I.; Hirano, T.; Nakajima, S.; Hikida, M.; Kumagai, T. In vitro plasma protein binding and cellular uptake of ATX-S10(Na), a hydrophilic chlorin photosensitizer. Jpn. J. Cancer Res. Gann 2000, 91, 845–852. [Google Scholar] [CrossRef]
- Gomer, C.J. Preclinical examination of first and second generation photosensitizers used in photodynamic therapy. Photochem. Photobiol. 1991, 54, 1093–1107. [Google Scholar] [CrossRef] [PubMed]
- Skinner, S.A.; Tutton, P.J.; O’Brien, P.E. Microvascular architecture of experimental colon tumors in the rat. Cancer Res. 1990, 50, 2411–2417. [Google Scholar] [PubMed]
- Henderson, B.W.; Waldow, S.M.; Mang, T.S.; Potter, W.R.; Malone, P.B.; Dougherty, T.J. Tumor destruction and kinetics of tumor cell death in two experimental mouse tumors following photodynamic therapy. Cancer Res. 1985, 45, 572–576. [Google Scholar] [PubMed]
- Li, J.; Li, X.L.; Yuan, Y.; Zhang, S.Z. Disputes and exploration of neoadjuvant and adjuvant therapy for colon cancer. Zhonghua Wei Chang. Wai Ke Za Zhi 2019, 22, 329–335. (In Chinese) [Google Scholar] [CrossRef] [PubMed]
- Barzi, A.; Lenz, A.M.; Labonte, M.J.; Lenz, H.J. Molecular Pathways: Estrogen Pathway in Colorectal Cancer Estrogen and Colorectal Cancer. Clin. Cancer Res. 2013, 19, 5842–5848. [Google Scholar] [CrossRef] [PubMed]
- Caiazza, F.; Ryan, E.J.; Doherty, G.; Winter, D.C.; Sheahan, K. Estrogen receptors and their implications in colorectal carcinogenesis. Front. Oncol. 2015, 5, 19. [Google Scholar] [CrossRef] [PubMed]
- Nanda, K.; Bastian, L.A.; Hasselblad, V.; Simel, D.L. Hormone replacement therapy and the risk of colorectal cancer: A meta-analysis. Obstet. Gynecol. 1999, 93, 880–888. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.C.; Huang, H.L.; Leung, C.Y. Association of hormone replacement therapy with mortality in colorectal cancer survivor: A systematic review and meta-analysis. BMC Cancer 2019, 19, 1199. [Google Scholar] [CrossRef]
- Symer, M.M.; Wong, N.Z.; Abelson, J.S.; Milsom, J.W.; Yeo, H.L. Hormone Replacement Therapy and Colorectal Cancer Incidence and Mortality in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. Clin. Color. Cancer 2018, 17, e281–e288. [Google Scholar] [CrossRef]
- Simin, J.; Khodir, H.; Fornes, R.; Tamimi, R.M.; Brusselaers, N. Association between menopausal hormone therapy use and mortality risk: A Swedish population-based matched cohort study. Acta Oncol. 2022, 61, 632–640. [Google Scholar] [CrossRef]
- Zhang, Y.L.; Wen, X.D.; Guo, X.; Huang, S.Q.; Wang, T.T.; Zhou, P.T.; Li, W.; Zhou, L.F.; Hu, Y.H. Progesterone suppresses the progression of colonic carcinoma by increasing the activity of the GADD45α/JNK/cJun signalling pathway. Oncol. Rep. 2021, 45, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Sasso, C.V.; Santiano, F.E.; Campo Verde Arboccó, F.; Zyla, L.E.; Semino, S.N.; Guerrero-Gimenez, M.E.; Pistone Creydt, V.; López Fontana, C.M.; Carón, R.W. Estradiol and progesterone regulate proliferation and apoptosis in colon cancer. Endocr. Connect. 2019, 8, 217–229. [Google Scholar] [CrossRef] [PubMed]
- Campbell-Thompson, M.; Lynch, I.J.; Bhardwaj, B. Expression of estrogen receptor (ER) subtypes and ERbeta isoforms in colon cancer. Cancer Res. 2001, 61, 632–640. [Google Scholar] [PubMed]
- Zhang, L.; Gao, X.; Men, K.; Wang, B.; Zhang, S.; Qiu, J.; Huang, M.; Gou, M.; Huang, N.; Qian, Z.; et al. Gene therapy for C-26 colon cancer using heparin-polyethyleneimine nanoparticle-mediated survivin T34A. Int. J. Nanomed. 2011, 6, 2419–2427. [Google Scholar] [CrossRef]
- Ortiz, R.; Prados, J.; Melguizo, C.; Rama, A.R.; Alvarez, P.J.; Rodríguez-Serrano, F.; Caba, O.; Boulaiz, H.; Aranega, A. Gef gene therapy enhances the therapeutic efficacy of cytotoxics in colon cancer cells. Biomed. Pharmacother. 2012, 66, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Tu, S.P.; Cui, J.T.; Liston, P.; Huajiang, X.; Xu, R.; Lin, M.C.; Zhu, Y.B.; Zou, B.; Ng, S.S.; Jiang, S.H.; et al. Gene therapy for colon cancer by adeno-associated viral vector-mediated transfer of survivin Cys84Ala mutant. Gastroenterology 2005, 128, 361–375. [Google Scholar] [CrossRef]
- Huang, Z.; Kaller, M.; Hermeking, H. CRISPR/Cas9-mediated inactivation of miR-34a and miR-34b/c in HCT116 colorectal cancer cells: Comprehensive characterization after exposure to 5-FU reveals EMT and autophagy as key processes regulated by miR-34. Cell Death Differ. 2023, 30, 2017–2034. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, I.; Dhar, R.; Pethusamy, K.; Seethy, A.; Srivastava, T.; Sah, R.; Sharma, J.; Karmakar, S. Exploring the Role of Gut Microbiome in Colon Cancer. Appl. Biochem. Biotechnol. 2021, 193, 1780–1799. [Google Scholar] [CrossRef]
- Bell, H.N.; Rebernick, R.J.; Goyert, J.; Singhal, R.; Kuljanin, M.; Kerk, S.A.; Huang, W.; Das, N.K.; Andren, A.; Solanki, S.; et al. Reuterin in the healthy gut microbiome suppresses colorectal cancer growth through altering redox balance. Cancer Cell 2022, 40, 185–200.e6. [Google Scholar] [CrossRef]
| Kind | Factor | Example |
|---|---|---|
| History | Genetic from family history and the medical history of the patient |
|
| Lifestyle | Lifestyle for the patient in the active and diet surgery |
|
| Molecular Marker | Description | Diagnostic Methods | Reference |
|---|---|---|---|
| CEA (carcinoembryonic antigen) | Protein in the blood. | Measured using a blood test. A high level of CEA indicates the presence of colon cancer. | [27] |
| Calprotectin | Protein in the stool. | A non-invasive screening tool. A higher level than normal in the stool can indicate the presence of CRC. | |
| M2-PK | This is an enzyme that is often elevated in the blood of patients with colon cancer. | Measured using a blood test. A high level of M2-PK indicates the presence of colon cancer. | |
| S100A12 | A protein in the blood. | Measured using a blood test. A high level of S100A12 can indicate the presence of colon cancer. | |
| Microsatellite instability (MSI) | This is a genetic change. | This genetic testing of tumor tissue. The presence of MSI can indicate a higher likelihood of colon cancer. | |
| KRAS mutation | This is a genetic changepresent in around 40% of colon cancer cases. | Diagnosed through genetic testing of tumor tissue. The presence of a KRAS mutation can indicate a higher likelihood of colon cancer. |
| Specimen | Chromosomal Location |
|---|---|
| Stool DNA | 5q21, 17p13, and 12p |
| Tissue | 17p13, 3p22, 2q31–33, 2p21, 18q21, 20q11, 18q21, 2p21, 7p22, and 3p21 |
| Colonic effluent and colonic DNA | 12p |
| Nanoparticles | Imaging Technique | Benefit | Result | Reference |
|---|---|---|---|---|
| Peanut agglutinin (PNA) | Florescence endoscopy | Early-stage small-sized CRC tissue | Better imaging of the CRC cell’s mucous | [2] |
| maghemite Fe2O3 and γ-Fe2O3 | SERS technique | Crucial target for diagnosing CRC | ||
| AuNPs | Raman spectroscopy (SERS) | Through the RS it differentiates between normal cells and cancerous serum | Better visibility and detection of cancerous serum | |
| Quantum dots (QDs) | Florescence | Emit from visible to infrared wavelengths upon excitation | Better cancer imaging | |
| Raman scattering (RS) and fiber optic probes | Hollow organs and diagnose CRC | Single-cell-based technique with better cancer imaging | ||
| H2O2 | Florescence | Circulating tumor cell detection | Better tumor targeting and imaging | [38] |
| Element barium | X-ray | Help to improve the quality of the X-ray images | Barium solution coats the lining of the colon | [7] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alrushaid, N.; Khan, F.A.; Al-Suhaimi, E.; Elaissari, A. Progress and Perspectives in Colon Cancer Pathology, Diagnosis, and Treatments. Diseases 2023, 11, 148. https://doi.org/10.3390/diseases11040148
Alrushaid N, Khan FA, Al-Suhaimi E, Elaissari A. Progress and Perspectives in Colon Cancer Pathology, Diagnosis, and Treatments. Diseases. 2023; 11(4):148. https://doi.org/10.3390/diseases11040148
Chicago/Turabian StyleAlrushaid, Noor, Firdos Alam Khan, Ebtesam Al-Suhaimi, and Abdelhamid Elaissari. 2023. "Progress and Perspectives in Colon Cancer Pathology, Diagnosis, and Treatments" Diseases 11, no. 4: 148. https://doi.org/10.3390/diseases11040148
APA StyleAlrushaid, N., Khan, F. A., Al-Suhaimi, E., & Elaissari, A. (2023). Progress and Perspectives in Colon Cancer Pathology, Diagnosis, and Treatments. Diseases, 11(4), 148. https://doi.org/10.3390/diseases11040148