Increased Salivary IL-1 Beta Level Is Associated with Poor Sleep Quality in University Students

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Study Sample
2.3. Information Collection Procedure
2.4. Evaluation of Sleep Quality
2.5. Evaluation of Stress, Depression and Anxiety Symptoms, and Self-Perceived Health
2.6. Other Factors Influencing Sleep Quality
2.7. Saliva Collection and Cytokines Analysis
2.8. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics of the Study Sample
3.2. Sleep Quality
3.3. Stress, Anxiety and Depression Symptoms, Self-Perceived Health, and Their Association with Sleep Quality
3.4. Factors Affecting Sleep and Their Association with Sleep Quality
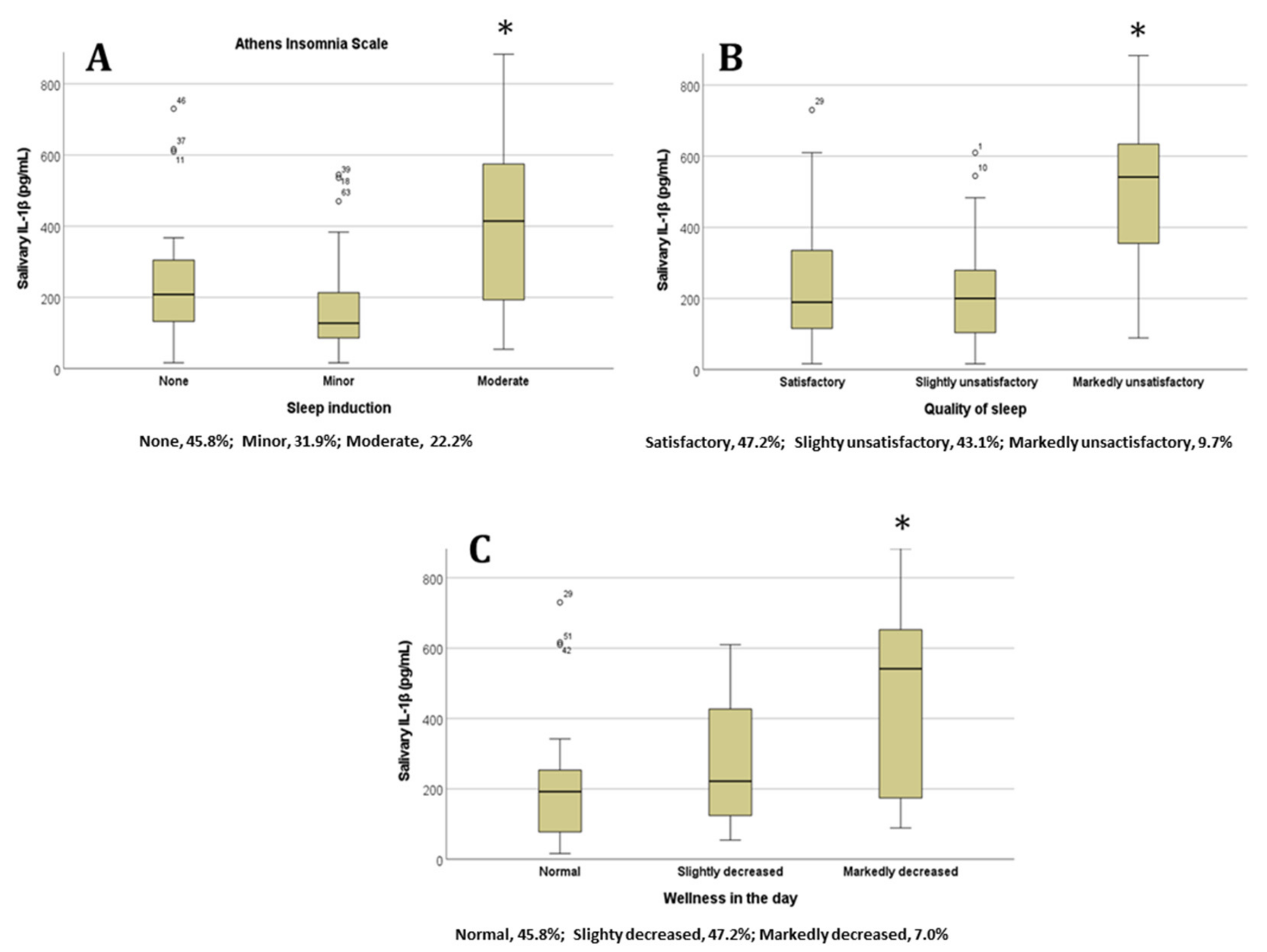
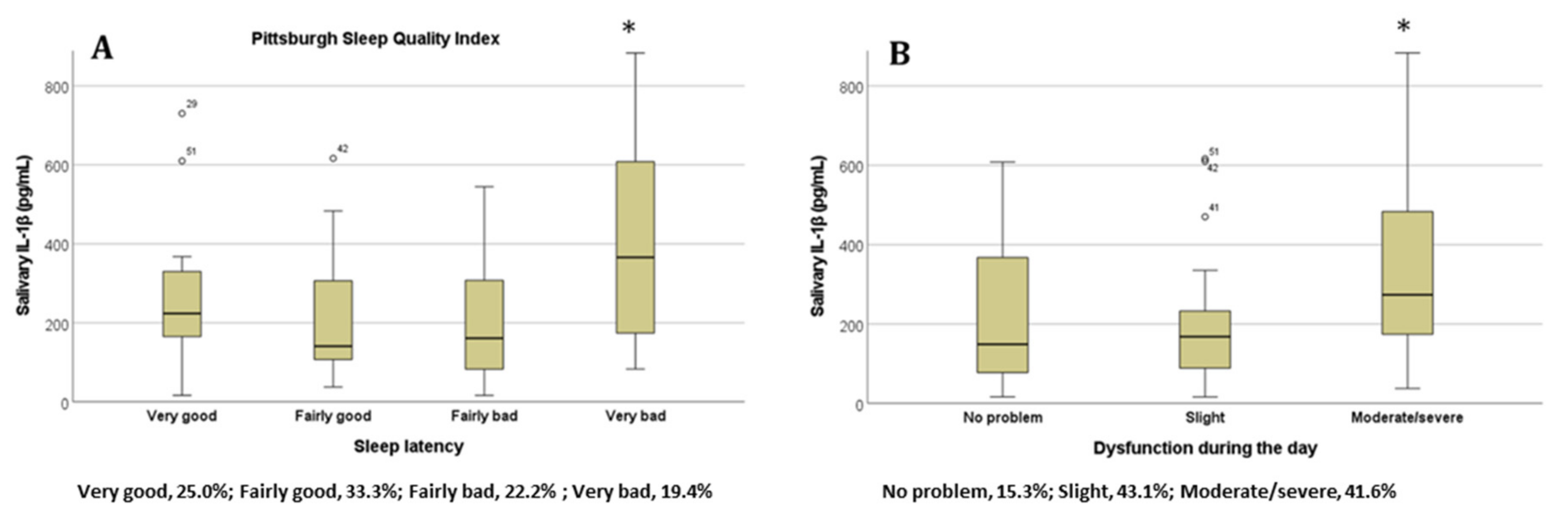
3.5. Salivary Cytokines and Their Association with Sleep Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smith, M.T.; Perlis, M.L.; Park, A.; Smith, M.S.; Pennington, J.; Giles, D.E.; Buysse, D.J. Comparative meta-analysis of pharmacotherapy and behavior therapy for persistent insomnia. Am. J. Psychiatry 2002, 159, 5–11. [Google Scholar] [CrossRef]
- American Psychiatric Association, DSM-5 Task Force. Diagnostic and Statistical Manual of Mental Disorders: DSM-5™, 5th ed.; American Psychiatric Publishing, Inc.: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Paúl, C.; Ribeiro, O.; Teixeira, L. Active Ageing: An Empirical Approach to the WHO Model. Curr. Gerontol. Geriatr. Res. 2012, 2012, 382972. [Google Scholar] [CrossRef]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef]
- Suardiaz-Muro, M.; Morante-Ruiz, M.; Ortega-Moreno, M.; Ruiz, M.A.; Martín-Plasencia, P.; Vela-Bueno, A. Sueño y rendimiento académico en estudiantes universitarios: Revisión sistemática [Sleep and academic performance in university students: A systematic review]. Rev. Neurol. 2020, 71, 43–53. [Google Scholar] [CrossRef]
- Moo, J.; Rosado, C.; Yañez, A.; Valencia, M. Types of insomnia and physical activity in college students. Sleep Med. Rev. 2013, 14, e117. [Google Scholar] [CrossRef]
- Vera, V.; Oñate, G.; Fernández, M.; Valladares, M.; Crovetto, M.; Espinoza, V.; Mena, F.; Agüero, S.D. Tobacco consumption in Chilean university students and associations with anthropometry, eating habits and sleep quality multicentric study. J. Prev. Med. Hyg. 2021, 62, E430–E438. [Google Scholar] [CrossRef]
- Seoane, H.A.; Moschetto, L.; Orliacq, F.; Orliacq, J.; Serrano, E.; Cazenave, M.I.; Vigo, D.E.; Perez-Lloret, S. Sleep disruption in medicine students and its relationship with impaired academic performance: A systematic review and meta-analysis. Sleep Med. Rev. 2020, 53, 101333. [Google Scholar] [CrossRef]
- Romero-Blanco, C.; Hernández-Martínez, A.; Parra-Fernández, M.L.; Onieva-Zafra, M.D.; Prado-Laguna, M.D.C.; Rodríguez-Almagro, J. Food Addiction and Lifestyle Habits among University Students. Nutrients 2021, 13, 1352. [Google Scholar] [CrossRef]
- Taylor, D.J.; Bramoweth, A.D.; Grieser, E.A.; Tatum, J.I.; Roane, B.M. Epidemiology of insomnia in college students: Relationship with mental health, quality of life, and substance use difficulties. Behav. Ther. 2013, 44, 339–348. [Google Scholar] [CrossRef]
- Zielinski, M.R.; Gibbons, A.J. Neuroinflammation, Sleep, and Circadian Rhythms. Front. Cell. Infect. Microbiol. 2022, 12, 853096. [Google Scholar] [CrossRef]
- Irwin, M.R.; Olmstead, R.; Carroll, J.E. Sleep Disturbance, Sleep Duration, and Inflammation: A Systematic Review and Meta-Analysis of Cohort Studies and Experimental Sleep Deprivation. Biol. Psychiatry 2016, 80, 40–52. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, N.C.; Vgontzas, A.N.; Kritikou, I.; Chrousos, G. HPA Axis and Sleep. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2020. [Google Scholar]
- Clinton, J.M.; Davis, C.J.; Zielinski, M.R.; Jewett, K.A.; Krueger, J.M. Biochemical regulation of sleep and sleep biomarkers. J. Clin. Sleep Med. 2011, 7, S38–S42. [Google Scholar] [CrossRef] [PubMed]
- Mullington, J.M.; Simpson, N.S.; Meier-Ewert, H.K.; Haack, M. Sleep loss and inflammation. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Mills, P.J.; Loredo, J.S.; Adler, K.A.; Dimsdale, J.E. The association between interleukin-6, sleep, and demographic characteristics. Brain Behav. Immun. 2005, 19, 165–172. [Google Scholar] [CrossRef]
- Vgontzas, A.N.; Papanicolaou, D.A.; Bixler, E.O.; Lotsikas, A.; Zachman, K.; Kales, A.; Prolo, P.; Wong, M.L.; Licinio, J.; Gold, P.W.; et al. Circadian interleukin-6 secretion and quantity and depth of sleep. J. Clin. Endocrinol. Metab. 1999, 84, 2603–2607. [Google Scholar] [CrossRef]
- Zhai, S.; Tao, S.; Wu, X.; Zou, L.; Yang, Y.; Xie, Y.; Li, T.; Zhang, D.; Qu, Y.; Tao, F. Associations of Sleep Insufficiency and Chronotype with Inflammatory Cytokines in College Students. Nat. Sci. Sleep 2021, 13, 1675–1685. [Google Scholar] [CrossRef]
- Dimitrov, S.; Besedovsky, L.; Born, J.; Lange, T. Differential acute effects of sleep on spontaneous and stimulated production of tumor necrosis factor in men. Brain Behav. Immun. 2015, 47, 201–210. [Google Scholar] [CrossRef]
- Riis, J.L.; Out, D.; Dorn, L.D.; Beal, S.J.; Denson, L.A.; Pabst, S.; Jaedicke, K.; Granger, D.A. Salivary cytokines in healthy adolescent girls: Intercorrelations, stability, and associations with serum cytokines, age, and pubertal stage. Dev. Psychobiol. 2014, 56, 797–811. [Google Scholar] [CrossRef]
- La Fratta, I.; Tatangelo, R.; Campagna, G.; Rizzuto, A.; Franceschelli, S.; Ferrone, A.; Patruno, A.; Speranza, L.; De Lutiis, M.A.; Felaco, M.; et al. The plasmatic and salivary levels of IL-1β, IL-18 and IL-6 are associated to emotional difference during stress in young male. Sci. Rep. 2018, 8, 3031. [Google Scholar] [CrossRef]
- Parkin, G.M.; Kim, S.; Mikhail, A.; Malhas, R.; McMillan, L.; Hollearn, M.; Granger, D.A.; Mapstone, M.; Yassa, M.A.; Thomas, E.A. Associations between saliva and plasma cytokines in cognitively normal, older adults. Aging Clin. Exp. Res. 2023, 35, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Martínez, R.; Chover-Sierra, E.; Colomer-Pérez, N.; Vlachou, E.; Andriuseviciene, V.; Cauli, O. Sleep quality and its association with substance abuse among university students. Clin. Neurol. Neurosurg. 2020, 188, 105591. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Gavurova, B.; Khouri, S.; Ivankova, V.; Rigelsky, M.; Mudarri, T. Internet Addiction, Symptoms of Anxiety, Depressive Symptoms, Stress Among Higher Education Students During the COVID-19 Pandemic. Front. Public Health 2022, 10, 893845. [Google Scholar] [CrossRef]
- Pieh, C.; Dale, R.; Plener, P.L.; Humer, E.; Probst, T. Stress levels in high-school students after asemester of home-schooling. Eur. Child Adolesc. Psychiatry 2022, 31, 1847–1849. [Google Scholar] [CrossRef]
- Jurewicz, J.; Kaleta, D. Correlates of Poor Self-Assessed Health Status among Socially Disadvantaged Populations in Poland. Int. J. Environ. Res. Public Health 2020, 17, 1372. [Google Scholar] [CrossRef]
- Machón, M.; Vergara, I.; Dorronsoro, M.; Vrotsou, K.; Larrañaga, I. Self-perceived health in functionally independent older people: Associated factors. BMC Geriatr. 2016, 16, 66. [Google Scholar] [CrossRef]
- Ministry of Health of Spain. Límites de Consumo de Bajo Riesgo de Alcohol. Actualización del Riesgo Relacionado Con Los Niveles de Consumo de Alcohol, el Patrón de Consumo y el Tipo de Bebida. Ministerio de Sanidad Española. 2020. Available online: https://www.sanidad.gob.es/profesionales/saludPublica/prevPromocion/Prevencion/alcohol/docs/Limites_Consumo_Bajo_Riesgo_Alcohol_Actualizacion.pdf (accessed on 4 September 2023).
- Léger, D.; Roscoat, E.D.; Bayon, V.; Guignard, R.; Pâquereau, J.; Beck, F. Short sleep in young adults: Insomnia or sleep debt? Prevalence and clinical description of short sleep in a representative sample of 1004 young adults from France. Sleep Med. 2011, 12, 454–462. [Google Scholar] [CrossRef]
- Ahn, S.Y.; Kim, Y.J. The influence of smartphone use and stress on quality of sleep among nursing students. Indian J. Sci. Technol. 2015, 8, 85943. [Google Scholar] [CrossRef]
- Van Dongen, H.P.; Vitellaro, K.M.; Dinges, D.F. Individual differences in adult human sleep and wakefulness: Leitmotif for a research agenda. Sleep 2005, 28, 479–496. [Google Scholar] [CrossRef] [PubMed]
- Gellis, L.A.; Park, A.; Stotsky, M.T.; Taylor, D.J. Associations between sleep hygiene and insomnia severity in college students: Cross-sectional and prospective analyses. Behav. Ther. 2014, 45, 806–816. [Google Scholar] [CrossRef]
- Alimoradi, Z.; Lin, C.Y.; Broström, A.; Bülow, P.H.; Bajalan, Z.; Griffiths, M.D.; Ohayon, M.M.; Pakpour, A.H. Internet addiction and sleep problems: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 47, 51–61. [Google Scholar] [CrossRef]
- Riera-Sampol, A.; Rodas, L.; Martínez, S.; Moir, H.J.; Tauler, P. Caffeine Intake among Undergraduate Students: Sex Differences, Sources, Motivations, and Associations with Smoking Status and Self-Reported Sleep Quality. Nutrients 2022, 14, 1661. [Google Scholar] [CrossRef] [PubMed]
- Yin, F.; Chen, C.; Song, S.; Chen, Z.; Jiao, Z.; Yan, Z.; Yin, G.; Feng, Z. Factors Affecting University Students’ Sleep Quality during the Normalisation of COVID-19 Epidemic Prevention and Control in China: A Cross-Sectional Study. Sustainability 2022, 14, 10646. [Google Scholar] [CrossRef]
- Krueger, J.M.; Majde, J.A. Humoral links between sleep and the immune system: Research issues. Ann. N. Y. Acad. Sci. 2003, 992, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Zielinski, M.R.; Kim, Y.; Karpova, S.A.; McCarley, R.W.; Strecker, R.E.; Gerashchenko, D. Chronic sleep restriction elevates brain interleukin-1 beta and tumor necrosis factor-alpha and attenuates brain-derived neurotrophic factor expression. Neurosci. Lett. 2014, 580, 27–31. [Google Scholar] [CrossRef]
- Zefferino, R.; Di Gioia, S.; Conese, M. Molecular links between endocrine, nervous and immune system during chronic stress. Brain Behav. 2021, 11, e01960. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Janicki-Deverts, D.; Doyle, W.J.; Miller, G.E.; Frank, E.; Rabin, B.S.; Turner, R.B. Chronic stress, glucocorticoid receptor resistance, inflammation, and disease risk. Proc. Natl. Acad. Sci. USA 2012, 109, 5995–5999. [Google Scholar] [CrossRef]
- Irwin, M.R.; Cole, S.W. Reciprocal regulation of the neural and innate immune systems. Nat. Rev. Immunol. 2011, 11, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.; Thompson, J.; Miller, C.; Gillin, J.C.; Ziegler, M. Effects of sleep and sleep deprivation on catecholamine and interleukin-2 levels in humans: Clinical implications. J. Clin. Endocrinol. Metab. 1999, 84, 1979–1985. [Google Scholar] [CrossRef]
- Owens, H.; Christian, B.; Polivka, B. Sleep behaviors in traditional-age college students: A state of the science review with implications for practice. J. Am. Assoc. Nurse Pract. 2017, 29, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Qiu, L.; Gong, F.; Wu, J.; You, D.; Zhao, Y.; Xu, L.; Cao, X.; Bao, F. Exercise Interventions Improved Sleep Quality through Regulating Intestinal Microbiota Composition. Int. J. Environ. Res. Public Health 2022, 19, 12385. [Google Scholar] [CrossRef]
- Capers, P.L.; Fobian, A.D.; Kaiser, K.A.; Borah, R.; Allison, D.B. A systematic review and meta-analysis of randomized controlled trials of the impact of sleep duration on adiposity and components of energy balance. Obes. Rev. 2015, 16, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Hepsomali, P.; Groeger, J.A. Examining the role of systemic chronic inflammation in diet and sleep relationship. J. Psychopharmacol. 2022, 36, 1077–1086. [Google Scholar] [CrossRef]
- You, Y.; Chen, Y.; Fang, W.; Li, X.; Wang, R.; Liu, J.; Ma, X. The association between sedentary behavior, exercise, and sleep disturbance: A mediation analysis of inflammatory biomarkers. Front. Immunol. 2023, 13, 1080782. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.; Yang, E. Sleep, physical activity, and sedentary behaviors as factors related to depression and health-related quality of life among older women living alone: A population-based study. Eur. Rev. Aging Phys. Act. 2023, 20, 6. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Jiang, C.; Yang, Y.; Dzierzewski, J.M.; Spruyt, K.; Zhang, B.; Huang, M.; Ge, H.; Rong, Y.; Ola, B.A.; et al. Depression and Anxiety Mediate the Association between Sleep Quality and Self-Rated Health in Healthcare Students. Behav. Sci. 2023, 13, 82. [Google Scholar] [CrossRef] [PubMed]
- Gardani, M.; Bradford, D.R.R.; Russell, K.; Allan, S.; Beattie, L.; Ellis, J.G.; Akram, U. A systematic review and meta-analysis of poor sleep, insomnia symptoms and stress in undergraduate students. Sleep Med. Rev. 2022, 61, 101565. [Google Scholar] [CrossRef]
- Wu, S.; Wang, R.; Zhao, Y.; Ma, X.; Wu, M.; Yan, X.; He, J. The relationship between self-rated health and objective health status: A population-based study. BMC Public Health 2013, 13, 320. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Su, H.; Zou, Y.; Chen, J.; Wu, J.; Chang, W. Self-rated health of Chinese adolescents: Distribution and its associated factors. Scand. J. Caring Sci. 2011, 25, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Lekander, M.; Elofsson, S.; Neve, I.M.; Hansson, L.O.; Undén, A.L. Self-rated health is related to levels of circulating cytokines. Psychosom. Med. 2004, 66, 559–563. [Google Scholar] [CrossRef]
- Bautmans, I.; Njemini, R.; Predom, H.; Lemper, J.C.; Mets, T. Muscle endurance in elderly nursing home residents is related to fatigue perception, mobility, and circulating tumor necrosis factor-alpha, interleukin-6, and heat shock protein 70. J. Am. Geriatr. Soc. 2008, 56, 389–396. [Google Scholar] [CrossRef]
- He, D.; Yuan, M.; Dang, W.; Bai, L.; Yang, R.; Wang, J.; Ma, Y.; Liu, B.; Liu, S.; Zhang, S.; et al. Long term neuropsychiatric consequences in COVID-19 survivors: Cognitive impairment and inflammatory underpinnings fifteen months after discharge. Asian J. Psychiatry 2023, 80, 103409. [Google Scholar] [CrossRef] [PubMed]
- Abduljabbar, T.; Vohra, F.; Ullah, A.; Alhamoudi, N.; Khan, J.; Javed, F. Relationship between self-rated pain and peri-implant clinical, radiographic and whole salivary inflammatory markers among patients with and without peri-implantitis. Clin. Implant. Dent. Relat. Res. 2019, 21, 1218–1224. [Google Scholar] [CrossRef]
- Gardner, A.; Carpenter, G.; So, P.W. Salivary Metabolomics: From Diagnostic Biomarker Discovery to Investigating Biological Function. Metabolites 2020, 10, 47. [Google Scholar] [CrossRef]
- Okuma, N.; Saita, M.; Hoshi, N.; Soga, T.; Tomita, M.; Sugimoto, M.; Kimoto, K. Effect of masticatory stimulation on the quantity and quality of saliva and the salivary metabolomic profile. PLoS ONE 2017, 12, e0183109. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez-Del Valle, V.; Navarro-Martínez, R.; Ballestar-Tarin, M.L.; Cauli, O. Salivary Inflammatory Molecules as Biomarkers of Sleep Alterations: A Scoping Review. Diagnostics 2021, 11, 278. [Google Scholar] [CrossRef] [PubMed]
- Riis, J.L.; Granger, D.A.; DiPietro, J.A.; Bandeen-Roche, K.; Johnson, S.B. Salivary cytokines as a minimally-invasive measure of immune functioning in young children: Correlates of individual differences and sensitivity to laboratory stress. Dev. Psychobiol. 2015, 57, 153–167. [Google Scholar] [CrossRef]
- DeSantis, A.S.; DiezRoux, A.V.; Hajat, A.; Aiello, A.E.; Golden, S.H.; Jenny, N.S.; Seeman, T.E.; Shea, S. Associations of salivary cortisol levels with inflammatory markers: The Multi-Ethnic Study of Atherosclerosis. Psychoneuroendocrinology 2012, 37, 1009–1018. [Google Scholar] [CrossRef]
- Cole, S.W. Social regulation of leukocyte homeostasis: The role of glucocorticoid sensitivity. Brain Behav. Immun. 2008, 22, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.H.; Silverman, M.N.; Sternberg, E.M. Glucocorticoid dysregulations and their clinical correlates: From receptors to therapeutics. Ann. N. Y. Acad. Sci. 2009, 1179, 1–18. [Google Scholar] [CrossRef]
- DeRijk, R.; Michelson, D.; Karp, B.; Petrides, J.; Galliven, E.; Deuster, P.; Paciotti, G.; Gold, P.W.; Sternberg, E.M. Exercise and circadian rhythm-induced variations in plasma cortisol differentially regulate interleukin-1 beta (IL-1 beta), IL-6, and tumor necrosis factor-alpha (TNF alpha) production in humans: High sensitivity of TNF alpha and resistance of IL-6. J. Clin. Endocrinol. Metab. 1997, 82, 2182–2191. [Google Scholar] [CrossRef]
- Dagmara, D.; Frances, L.C.; Patrick, M. The role of environmental factors on sleep patterns and school performance in adolescents. Front. Psychol. 2015, 6, 17–24. [Google Scholar]
- Demirci, K.; Akgönül, M.; Akpinar, A. Relationship of smartphone use severity with sleep quality, depression, and anxiety in university students. J. Behav. Addict. 2015, 4, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Sohn, S.Y.; Rees, P.; Wildridge, B.; Kalk, N.J.; Carter, B. Prevalence of problematic smartphone usage and associated mental health outcomes amongst children and young people: A systematic review, meta-analysis and GRADE of the evidence. BMC Psychiatry 2019, 19, 356–360. [Google Scholar] [CrossRef]
- Rafique, N.; Al-Asoom, L.I.; Alsunni, A.A.; Saudagar, F.N.; Almulhim, L.; Alkaltham, G. Effects of Mobile Use on Subjective Sleep Quality. Nat. Sci. Sleep 2020, 12, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Rathakrishnan, B.; Bikar Singh, S.S.; Kamaluddin, M.R.; Yahaya, A.; Mohd Nasir, M.A.; Ibrahim, F.; Ab Rahman, Z. Smartphon Addiction and Sleep Quality on Academic Performance of University Students: An Exploratory Research. Int. J. Environ. Res. Public Health 2021, 18, 8291. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Items of the AIS Scale | No | Slight | Moderate | Severe |
|---|---|---|---|---|
| Sleep induction | 45.8 | 31.9 | 22.2 | 0 |
| Awakenings during the night | 44.4 | 43.1 | 12.5 | 0 |
| Final awakening earlier than desired | 56.9 | 36.1 | 6.9 | 0 |
| Total sleep duration | 31.9 | 47.2 | 20.8 | 0 |
| Overall quality of sleep | 47.2 | 43.1 | 9.7 | 0 |
| Sense of well-being during the day | 45.8 | 47.2 | 5.6 | 1.4 |
| Functioning (physical and mental) during the day | 63.9 | 31.9 | 4.2 | 0 |
| Sleepiness during the day | 23.6 | 59.7 | 16.7 | 0 |
| Very Good | Fairly Good | Fairly Bad | Very Bad | |
|---|---|---|---|---|
| Sleep quality | 29.2 | 41.7 | 22.2 | 6.9 |
| Sleep latency | 25.0 | 33.3 | 22.2 | 19.4 |
| Sleep duration | 20.8 | 43.1 | 31.9 | 4.2 |
| Habitual sleep efficiency | 73.6 | 9.7 | 8.3 | 8.3 |
| Sleep disturbance | 6.9 | 90.3 | 2.8 | 0 |
| Use of sleeping medication | 76.4 | 15.3 | 4.2 | 4.2 |
| Daytime dysfunction | 15.3 | 43.1 | 38.9 | 2.8 |
| Sleep Quality (PSQI) | Self-Perceived Stress (PSS) | Anxiety Symptoms (GADS) | Depression Symptoms (GADS) | Anxiety and Depression Symptoms (Total GADS Score) | Self-Perceived Health | |
|---|---|---|---|---|---|---|
| Sleep quality (AIS) | ||||||
| r | 0.723 | 0.441 | 0.670 | 0.478 | 0.673 | −0.355 |
| Sig | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.003 |
| Sleep quality (PSQI) | ||||||
| r | 0.531 | 0.498 | 0.366 | 0.505 | −0.318 | |
| Sig | <0.001 | <0.001 | 0.002 | <0.001 | 0.007 |
| Sleep Quality (AIS) | Sleep Quality (PSQI) | Self-Perceived Stress (PSS) | Anxiety Symptoms (GADS) | Depression Symptoms (GADS) | Anxiety and Depression Symptoms (Total GADS Score) | Self-Perceived Health | |
|---|---|---|---|---|---|---|---|
| lL-1β | |||||||
| r | 0.248 | 0.274 | 0.054 | 0.028 | 0.051 | 0.044 | −0.030 |
| p-value | 0.038 | 0.022 | 0.656 | 0.818 | 0.672 | 0.718 | 0.805 |
| IL-6 | |||||||
| r | −0.027 | −0.055 | −0.030 | −0.159 | 0.044 | −0.077 | 0.035 |
| p-value | 0.822 | 0.649 | 0.773 | 0.188 | 0.717 | 0.528 | 0.773 |
| TNFα | |||||||
| r | −0.024 | −0.035 | 0.088 | 0.039 | 0.117 | 0.085 | −0.259 |
| p-value | 0.842 | 0.778 | 0.470 | 0.752 | 0.337 | 0.490 | 0.033 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ballestar-Tarín, M.L.; Ibáñez-del Valle, V.; Mafla-España, M.A.; Cauli, O.; Navarro-Martínez, R. Increased Salivary IL-1 Beta Level Is Associated with Poor Sleep Quality in University Students. Diseases 2023, 11, 136. https://doi.org/10.3390/diseases11040136
Ballestar-Tarín ML, Ibáñez-del Valle V, Mafla-España MA, Cauli O, Navarro-Martínez R. Increased Salivary IL-1 Beta Level Is Associated with Poor Sleep Quality in University Students. Diseases. 2023; 11(4):136. https://doi.org/10.3390/diseases11040136
Chicago/Turabian StyleBallestar-Tarín, María Luisa, Vanessa Ibáñez-del Valle, Mayra Alejandra Mafla-España, Omar Cauli, and Rut Navarro-Martínez. 2023. "Increased Salivary IL-1 Beta Level Is Associated with Poor Sleep Quality in University Students" Diseases 11, no. 4: 136. https://doi.org/10.3390/diseases11040136
APA StyleBallestar-Tarín, M. L., Ibáñez-del Valle, V., Mafla-España, M. A., Cauli, O., & Navarro-Martínez, R. (2023). Increased Salivary IL-1 Beta Level Is Associated with Poor Sleep Quality in University Students. Diseases, 11(4), 136. https://doi.org/10.3390/diseases11040136