
Response Rate of the Third and Fourth Doses of the BNT162b2 Vaccine Administered to Cancer Patients Undergoing Active Anti-Neoplastic Treatments

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Determination of Anti-SARS-CoV-2 Antibodies Level
2.3. Statistical Analysis
3. Results
3.1. Study Population
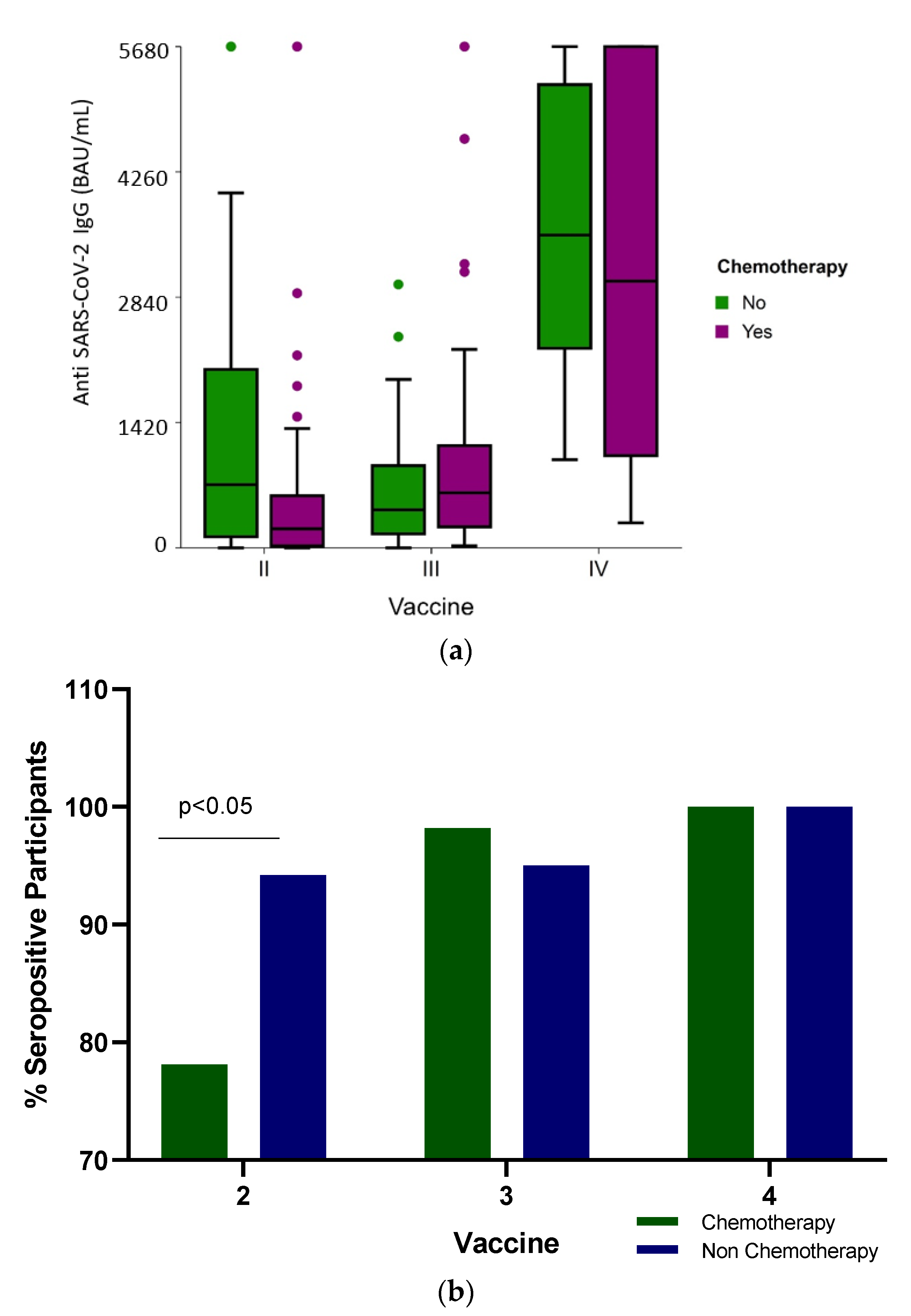
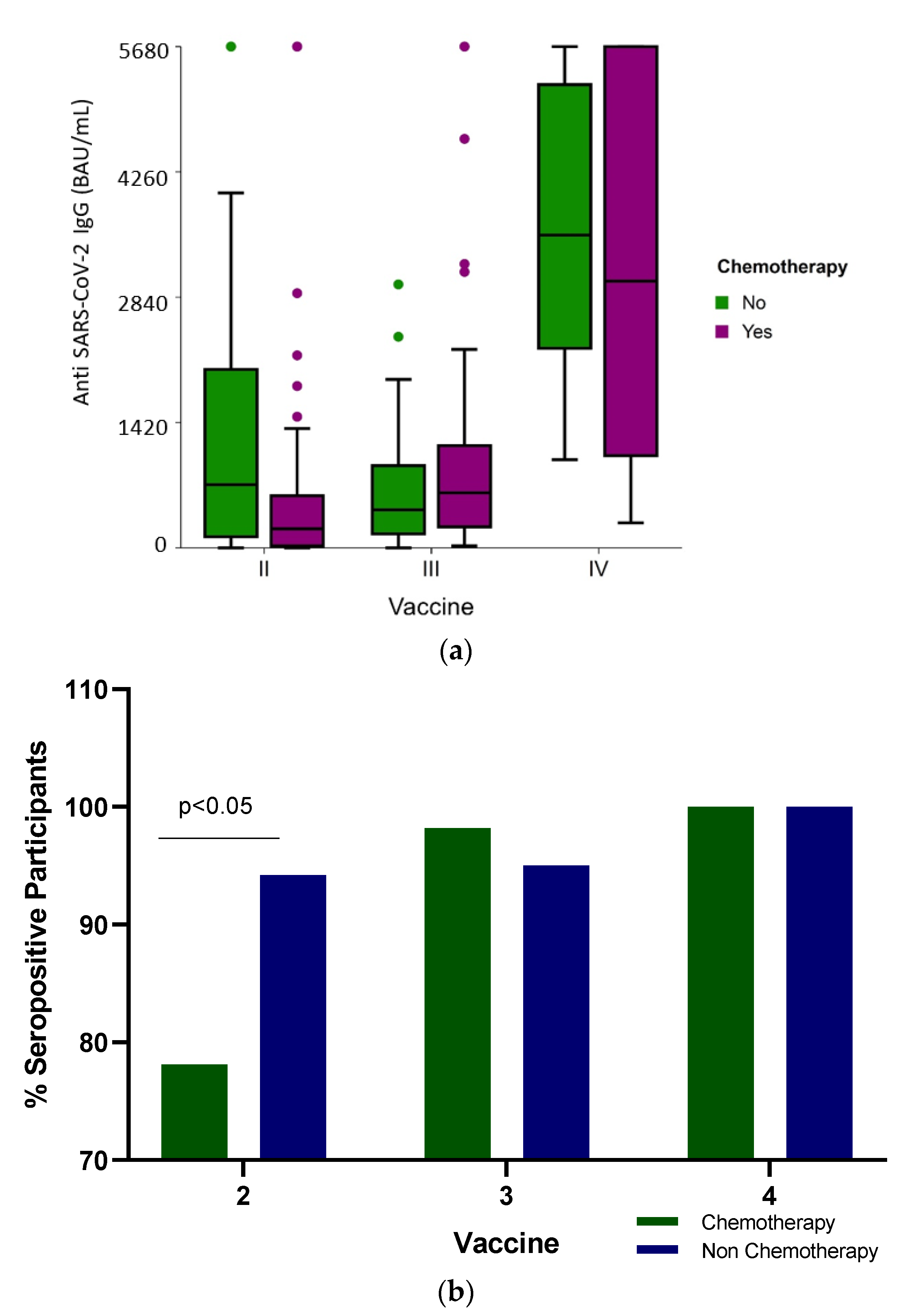
3.2. Antibody Levels and Seropositivity Response to BNT162b2 Vaccine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: http://covid19.who.int (accessed on 19 May 2023).
- Ciotti, M.; Ciccozzi, M.; Terrinoni, A.; Jiang, W.C.; Wang, C.B.; Bernardini, S. The COVID-19 pandemic. Crit. Rev. Clin. Lab. Sci. 2020, 57, 365–388. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, T.; Krammer, F.; Iwasaki, A. The first 12 months of COVID-19: A timeline of immunological insights. Nat. Rev. Immunol. 2021, 21, 245–256. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Director-General’s Opening Remarks at the Medica Briefing COVID-19. 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-themedia-briefing-on-covid-19-11-march-2020 (accessed on 19 May 2023).
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with cancer appear more vulnerable to SARS-CoV-2: A multicenter study during the COVID-19 outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Stainer, A.; Amati, F.; Suigo, G.; Simonetta, E.; Gramegna, A.; Voza, A.; Aliberti, S. COVID-19 in Immunocompromised Patients: A Systematic Review. Semin. Respir. Crit. Care Med. 2021, 42, 839–858. [Google Scholar] [CrossRef]
- Sengar, M.; Chinnaswamy, G.; Ranganathan, P.; Ashok, A.; Bhosale, S.; Biswas, S.; Chaturvedi, P.; Dhamne, C.; Divatia, J.; D’Sa, K.; et al. Outcomes of COVID-19 and risk factors in patients with cancer. Nat. Cancer 2022, 3, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Russell, B.; Moss, C.L.; Shah, V.; Ko, T.K.; Palmer, K.; Sylva, R.; Geogre, G.; Monroy-Iglesias, M.J.M.; Patten, P.; Ceesay, M.M.; et al. Risk of COVID-19 death in cancer patients: An analysis from Guy’s Cancer Centre and King’s College Hospital in London. Br. J. Cancer 2021, 125, 939–947. [Google Scholar] [CrossRef]
- Seth, G.; Sethi, S.; Bhattarai, S.; Saini, G.; Bhushan-Singh, C.; Aneja, R. SARS-CoV-2 Infection in Cancer Patients: Effects on Disease Outcomes and Patient Prognosis. Cancers 2020, 12, 3266. [Google Scholar] [CrossRef]
- Hiam-Galvez, K.J.; Allen, B.M.; Spitzer, M.H. Systemic immunity in cancer. Nat. Rev. Cancer 2021, 21, 345–359. [Google Scholar] [CrossRef]
- Norris, J.; Tumors Disrupt the Immune System Throughout the Body. University of California, San Francisco. 2020. Available online: https://www.ucsf.edu/news/2020/06/417666/tumors-disrupt-immune-system-throughout-body (accessed on 19 May 2023).
- Teo, S.P. Review of COVID-19 mRNA Vaccines: BNT162b2 and mRNA-1273. J. Pharm. Pract. 2022, 35, 947–951. [Google Scholar] [CrossRef]
- The Food and Drug Administration. Coronavirus (COVID-19) Update: FDA Authorizes Additional Vaccine Dose for Certain Immunocompromised Individuals. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-additional-vaccine-dose-certain-immunocompromised (accessed on 21 May 2023).
- Rahav, G.; Lustig, Y.; Lavee, J.; Benjamini, O.; Magen, H.; Hod, T.; Shem-Tov, N.; Shacham Shmueli, E.; Merkel, D.; Ben-Ari, Z.; et al. BNT162b2 mRNA COVID-19 vaccination in immunocompromised patients: A prospective cohort study. eClinicalMedicine 2021, 41, 101158. [Google Scholar] [CrossRef]
- Massarweh, A.; Eliakim-Raz, N.; Stemmer, A.; Levy-Barda, A.; Yust-Katz, S.; Zer, A.; Benouaich-Amiel, A.; Ben-Zvi, H.; Moskovits, N.; Brenner, B.; et al. Evaluation of Seropositivity Following BNT162b2 Messenger RNA Vaccination for SARS-CoV-2 in patients Undergoing Treatment for Cancer. JAMA Oncol. 2021, 7, 1133–1140. [Google Scholar] [CrossRef]
- Uaprasert, N.; Pitakkitnukun, P.; Tangcheewinsirikul, N.; Chiasakul, T.; Rojnuckarin, P. Immunogenicity and risks associated with impaired immune responses following SARS-CoV-2 vaccination and booster in hematologic malignancy patients: An updated meta-analysis. Blood Cancer J. 2022, 12, 173. [Google Scholar] [CrossRef]
- Oosting, S.F.; van der Veldt, A.A.M.; GeurtsvanKessel, C.H.; Fehrmann, R.S.N.; van Binnendijk, R.S.; Dingemans, A.C.; Smit, E.F.; Hiltermann, T.J.N.; den Hartog, G.; Jalving, M.; et al. mRNA-1273 COVID-19 vaccination in patients receiving chemotherapy, immunotherapy, or chemoimmunotherapy for solid tumours: A prospective, multicentre, non-inferiority trial. Lancet Oncol. 2021, 22, 1681–1691. [Google Scholar] [CrossRef]
- Stampfer, S.D.; Goldwater, M.S.; Jew, S.; Bujarski, S.; Regidor, B.; Daniely, D.; Chen, H.; Xu, N.; Li, M.; Green, T.; et al. Response to mRNA vaccination for COVID-19 among patients with multiple myeloma. Leukemia 2021, 35, 3534–3541. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Epten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Eng. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Leshem, E.; Wilder-Smith, A. COVID-19 vaccine impact in Israel and a way out of the pandemic. Lancet 2021, 397, 1783–1785. [Google Scholar] [CrossRef] [PubMed]
- Jeffay, N. COVID Vaccine Effective for 90% of Cancer Patients, Israeli Study Finds. The Times of Israel. 2021. Available online: https://www.timesofisrael.com/covid-vaccine-effective-for-90-of-cancer-patients-israeli-study-finds/ (accessed on 23 May 2023).
- Agbarya, A.; Sarel, I.; Ziv-Baran, T.; Agranat, S.; Schwartz, O.; Shai, A.; Nordheimer, S.; Fenig, S.; Shechtman, Y.; Kozlener, E.; et al. Efficacy of the mRNA-Based BNT162b2 COVID-19 Vaccine in Patients with Solid Malignancies Treated with Anti-Neoplastic Drugs. Cancers 2021, 13, 4191. [Google Scholar] [CrossRef] [PubMed]
- Isasi, F.; Naylor, M.D.; Skorton, D.; Grabowski, D.C.; Hernández, S.; Montomery Rice, V. Patients, Families, and Communities COVID-19 Impact Assessment: Lessons Learned and Compelling Needs. NAM Perspect. 2021, 2021. [Google Scholar] [CrossRef] [PubMed]
- Koc, H.C.; Xiao, J.; Liu, W.; Chen, G. Long COVID and its management. Int. J. Biol. Sci. 2022, 18, 4768–4780. [Google Scholar] [CrossRef]
- World Health Organization. Chapter 2. Current Context: The COVID-19 Pandemic and Continuing Challenges to Global Health. Available online: https://www.who.int/about/funding/invest-in-who/investment-case-2.0/challenges: (accessed on 24 May 2023).
- Fekadu, G.; Bekele, F.; Tolossa, T.; Fetensa, G.; Turi, E.; Getachew, M.; Abdisa, E.; Assefa, L.; Afeta, M.; Demisew, W.; et al. Impact of COVID-19 pandemic on chronic diseases care follow-up and current perspectives in low resource settings: A narrative review. Int. J. Physiol. Pathophysiol. Pharmacol. 2021, 13, 86–93. [Google Scholar]
- Kang, S.J.; Jung, S.I. Age related Morbidity and mortalities among Patients with COVID-19. Infect Chemother. 2020, 52, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Tassone, D.; Thompson, A.; Connell, W.; Lee, T.; Ungaro, R.; An, P.; Ding, Y.; Ding, N.S. Immunosuppression as a risk factor for COVID-19: A meta-analysis. Intern. Med. J. 2021, 51, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.K.; Liu, C.; Dadwal, S.S. Infectious Disease Complications in Cancer Patients. Crit Care Clin. 2021, 37, 69–84. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.H.J.; Sparks, J.A. Immunosuppression and SARS-CoV-2 breakthrough infections. Lancet Rheumatology. 2022, 4, e379–e380. [Google Scholar] [CrossRef] [PubMed]
- Trapani, D.; Curlgliano, G. COVID-19 vaccines in patients with cancer. Lancet Oncol. 2021, 22, 738–739. [Google Scholar] [CrossRef] [PubMed]
- Monin, L.; Laing, A.G.; Munoz-Ruiz, M.; McKenzie, D.R.; del Molino del Barrio, I.; Alaguthurai, T.; Domingo-Vila, C.; Hayday, T.S.; Graham, C.; Seow, J.; et al. Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: Interim analysis of a prospective observational study. Lancet Oncol. 2021, 22, 765–778. [Google Scholar] [CrossRef]
- Guven, D.C.; Sahin, T.K.; Klickap, S.; Uckun, F.M. Antibody Responses to COVID-19 Vaccination in Cancer: A Systematic Review. Front. Oncol. 2021, 11, 2021. [Google Scholar] [CrossRef]
- Fendler, A.; de Vries, E.G.E.; GeurtsvanKessel, C.H.; Haanen, J.B.; Wörmann, B.; Turajlic, S.; von Lilienfeld-Toal, M. COVID-19 vaccines in patients with cancer: Immunogenicity, efficacy and safety. Nat. Rev. Clin. Oncol. 2022, 19, 385–401. [Google Scholar] [CrossRef]
- Kamar, N.; Abravenel, F.; Narion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA COVID-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier, G.; Perrin, P.; Olagne, J.; Cognard, N.; Fafi-Kremer, S.; Caillard, S. Antibody Response After a Third dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients with Minimal Serologic Response to 2 Doses. JAMA 2021, 326, 1063–1065. [Google Scholar] [CrossRef]
- Rüthrich, M.M.; Giesen, N.; Mellinghoff, S.C.; Rieger, C.T.; von Lilienfeld-Toal, N. Cellular Immune Response after Vaccination in Patients with Cancer-Review on Past and Present Experiences. Vaccines 2022, 10, 182. [Google Scholar] [CrossRef] [PubMed]
- Negahdaripour, M.; Shafiekhani, M.; Iman Moezzi, S.M.; Amiri, S.; Rasekh, S.; Bagheri, A.; Mosaddeghi, M.; Vazin, A. Administration of COVID-19 vaccines in immunocompromised patients. Int. Immunopharmacol. 2021, 99, 10802. [Google Scholar] [CrossRef] [PubMed]
- Cohen, I.; Campisi-Pfinto, S.; Rozenberg, O.; Colodner, R.; Bar-Sela, G. The Humoral Response of Patients with Cancer to Breakthrough COVID-19 Infection or the Fourth BNT162b2 Vaccine dose. Oncologist 2023, 28, e225–e227. [Google Scholar] [CrossRef] [PubMed]
- Magen, O.; Waxman, J.G.; Makov-Assif, M.; Vered, R.; Dicker, D.; Hernán, M.A.; Lipsitch, M.; Reis, B.Y.; Balicer, R.D.; Dagan, N. Fourth Dose of BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2022, 386, 1603–1614. [Google Scholar] [CrossRef]
- Curlin, M.E.; Bates, T.A.; Guzman, G.; Schoen, D.; McBride, S.K.; Carpenter, S.D.; Tafesse, F.G. Omicron neutralizing antibody response following booster vaccination compared with breakthrough infection. medRxiv 2022. [Google Scholar] [CrossRef]
- Lasagna, A.; Bergami, F.; Lilleri, D.; Percivalle, E.; Quaccini, M.; Alessio, N.; Comolli, G.; Sarasini, A.; Sammartino, J.C.; Ferrari, A.; et al. Immunogenicity and safety after the third dose of BNT162b2 anti-SARS-CoV-2 vaccine in patients with solid tumors on active treatment: A prospective cohort study. ESMO Open 2022, 7, 100458. [Google Scholar] [CrossRef]
- Di Noia, V.; Pimpinelli, F.; Renna, D.; Campo, F.; Cosimati, A.; Torchia, A.; Marcozzi, B.; Massacci, A.; Pallocca, M.; Pellini, R.; et al. Duration of humoral response to the third dose of BNT162b2 vaccine in patients with solid cancer: Is fourth dose urgently needed? Eur. J. Cancer 2022, 176, 164–167. [Google Scholar] [CrossRef]
- Shroff, R.T.; Chalasani, P.; Wei, R.; Pennington, D.; Quirk, G.; Schoenle, M.V.; Peyton, K.L.; Uhrlaub, J.L.; Ripperger, T.J.; Jergovic, M.; et al. Immune responses to two and three doses of the BNT162b mRNA vaccine in adults with solid tumors. Nat. Med. 2021, 27, 2002–2011. [Google Scholar] [CrossRef]
- Shacham Shmueli, E.; Lawrence, Y.R.; Rahav, G.; Itay, A.; Lustig, Y.; Halpern, N.; Boursi, B.; Margalit, O. Serological response to a third booster dose of BNT162b2 COVID-19 vaccine among seronegative cancer patients. Cancer Rep. 2022, 5, e1645. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 COVID-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Terpos, E.; Karalis, V.; Ntanasis-Stathopoulos, I.; Gavariatopoulou, M.; Gumeni, S.; Malandrakis, P.; Papanagnou, E.-D.; Kastritis, E.; Trougakos, I.P.; Dimopoulus, M.A. Robust Neutralizing Antibody Responses 6 Months post Vaccination with BNT162b2: A Prospective study in 308 Health Individuals. Life 2021, 11, 1077. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, Y.; Mandel, M.; Bar-on, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.R.Y.B.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; et al. Efficacy of COVID-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ. 2022, 376, e068632. [Google Scholar] [CrossRef] [PubMed]
- Campos, G.R.; Almeida, N.B.F.; Filgueiras, P.S.; Corsini, C.A.; Gomes, S.V.C.; de Miranda, D.A.P.; de Assis, J.V.; de Souza Silva, T.B.; Alves, P.A.; da Rocha Fernandes, G.; et al. Booster dose of BNT162b2 after two doses of CoronaVac improves neutralization of SARS-CoV-2 Omicron variant. Commun. Med. 2022, 2, 76. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against COVID-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef]
- Falsey, A.R.; Frenck, R.W.; Walsh, E.E.; Kitchin, N.; Abslon, J.; Gurtman, A.; Lockhart, S.; Bailey, R.; Swanson, K.A.; Xu, X.; et al. SARS-CoV-2 Neutralization with BNT162b2 Vaccine Dose 3. N. Engl. J. Med. 2021, 385, 1627–1629. [Google Scholar] [CrossRef]
- Ligumsky, H.; Dor, H.; Etan, T.; Golomb, I.; Nikolaevski-Berlin, A.; Greenberg, I.; Halperin, T.; Angel, Y.; Henig, O.; Spitzer, A.; et al. Immunogenicity and safety of BNT162b2 mRNA vaccine booster in actively treated patients with cancer. Lancet Oncol. 2021, 23, 193–195. [Google Scholar] [CrossRef]
- Vietri, M.T.; Albanese, L.; Passariello, L.; D’Elia, G.; Caliendo, G.; Molinari, A.M.; Angelillo, I.F. Evaluation of neutralizing antibodies after vaccine BNT162b2: Preliminary data. J. Clin. Virol. 2022, 146, 105057. [Google Scholar] [CrossRef]
- Vietri, M.T.; DeElia, G.; Caliendo, G.; Passariello, L.; Albanese, L.; Molinari, A.M.; Angelillo, I.F. Antibody levels after BNT162b2 vaccine booster and SARS-CoV-2 Omicron infection. Vaccine 2022, 40, 5726–5731. [Google Scholar] [CrossRef]
- Gray-Gaillard, S.L.; Solis, S.; Monteiro, C.; Chen, H.M.; Ciabattoni, G.; Samanovic, M.I.; Cornelius, A.R.; Williams, T.; Geesey, E.; Rodriguez, M.; et al. Molecularly distinct memory CD4+ T cells are induced by SARS-CoV-2 infection and mRNA vaccination. bioRxiv 2022. [Google Scholar] [CrossRef]
- Fiorino, F.; Ciabattini, A.; Sicuranza, A.; Pastore, G.; Santoni, A.; Simoncelli, M.; Polvere, J.; Galimberti, S.; Baratè, C.; Sammartano, V.; et al. The third dose of mRNA SARS-CoV-2 vaccines enhances the spike-specific antibody and memory B cell response in myelofibrosis patients. Front. Immunol. 2022, 13, 1017863. [Google Scholar] [CrossRef] [PubMed]
- Vallejo, A.; Vizcarra, P.; Martin-Hondarza, A.; Gómez-Maldonado, S.; Haemmerle, J.; Velasco, H.; Casado, J.L. Impact of SARS-CoV-2-specific memory B cells on the immune response after mRNA-based Comirnaty vaccine in seronegative health care workers. Front. Microbiol. 2022, 13, 1002748. [Google Scholar] [CrossRef] [PubMed]
- Ciabattini, A.; Pastore, G.; Fiorino, F.; Polvere, J.; Lucchesi, S.; Pettini, E.; Auddino, S.; Rancen, I.; Durante, M.; Miscia, M.; et al. Evidence of SARS-CoV-Specific Memory B Cells Six months after vaccination With the BNT162b2 mRNA Vaccine. Front. Immunol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Henig, I.; Isenberg, J.; Yehudai-Ofir, D.; Leiba, R.; Ringelstein-Harlev, S.; Ram, R.; Avni, B.; Amit, O.; Grisariu, S.; Azoulay, T.; et al. Third BNT162b2 mRNA SARS-CoV-2 Vaccine Dose Significantly Enhances Immunogenicity in Recipients of Allogeneic Hematopoietic Stem Cell Transplantation. Vaccines 2023, 11, 775. [Google Scholar] [CrossRef]
- Watanabe, M.; Yakushijin, K.; Funakoshi, Y.; Ohji, G.; Ichikawa, H.; Sakai, H.; Hojo, W.; Saeki, M.; Hirakawa, Y.; Marsumoto, S.; et al. A Third Dose COVID-19 Vaccination in Allogeneic Hematopoietic Stem Cell Transplantation Patients. Vaccines 2022, 10, 1830. [Google Scholar] [CrossRef]
- Steensels, D.; Pierlet, N.; Penders, J.; Mesotten, D.; Heylen, L. Comparison of SARS-CoV-2 Antibody Response Following Vaccination with BNT162b2 and mRNA-1273. JAMA 2021, 326, 1533–1535. [Google Scholar] [CrossRef]
- Dickerman, B.A.; Gerlovin, H.; Madenci, A.L.; Kurgansky, K.E.; Ferolito, B.R.; Figueroa Muñiz, M.J.; Gagnon, D.R.; Gaziano, M.; Cho, K.; Casas, J.P.; et al. Comparative Effective ness of BNT162b2 and mRNA-1273 Vaccines in U.S. Veterans. N. Engl. J. Med. 2022, 386, 105–115. [Google Scholar] [CrossRef]
- Moderna’s COVID-19 Vaccine May Be More Effective for Cancer Patients—Cancer Therapy Advisor. Available online: https://www.cancertherapyadvisor.com/home/cancer-topics/general-oncology/cancer-moderna-covid19-vaccine-may-be-more-effective/ (accessed on 9 June 2023).
- Becker, M.; Cossmann, A.; Lürken, K.; Junker, D.; Gruber, J.; Juengling, J.; Morillas Ramos, G.; Beigel, A.; Wrenger, E.; Lonnemann, F.; et al. Longitudinal cellular and humoral immune responses after triple BNT162b2 and fourth full-dose mRNA-1273 vaccination in haemodialysis patients. Front. Immunol. 2022, 13, 1004045. [Google Scholar] [CrossRef]
- Alexopoulos, H.; Trougakos, I.P.; Dimopoulos, M.A.; Terpo, E. Clinical usefulness of testing for severe acute respiratory syndrome coronavirus 2 antibodies. Eur. J. Intern. Med. 2023, 107, 7–16. [Google Scholar] [CrossRef]
- Terpos, E.; Liontos, M.; Fiste, O.; Zagouri, F.; Briasoulis, A.; Sklirou, A.D.; Markellos, C.; Skafida, E.; Papatheodoridi, A.; Andrikopoulou, A.; et al. SARS-CoV-2 Neutralizing Antibodies Kinetics Postvaccination in Cancer Patients under Treatment with Immune Checkpoint Inhibition. Cancers 2022, 14, 2796. [Google Scholar] [CrossRef]
- Bergamaschi, C.; Pagoni, M.; Rosati, M.; Angel, M.; Tzannou, I.; Vlachou, M.; Darmani, I.; Ullah, A.; Bear, J.; Devasundaram, S.; et al. Reduced Antibodies and Innate Cytokine Changes in SARS-CoV-2 BNT162b2 mRNA Vaccinated Transplant Patients with Hematological Malignancies. Front. Immunol. 2022, 13, 899972. [Google Scholar] [CrossRef] [PubMed]
- Rosati, M.; Terpos, E.; Bear, J.; Burns, R.; Devasundaram, S.; Ntanasis-Stathopoulos, I.; Gavriatopoulou, M.; Kastritis, E.; Dimopoulos, M.-A.; Pavlakis, G.N.; et al. Low Spike Antibody Levels and Impaired BA.4/5 Neutralization in Patients with Multiple Myeloma or Waldenstrom’s Macroglobulinemia after BNT162b2 Booster Vaccination. Cancers 2022, 14, 5816. [Google Scholar] [CrossRef] [PubMed]
- Liatsou, E.; Ntanasis-Stathopoulos, I.; Lykos, S.; Ntanasis-Stathopoulos, A.; Gavriatopoulou, M.; Psaltopoulou, T.; Sergentanis, T.N.; Terpos, E. Adult Patients with Cancer Have Impaired Humoral Responses to Complete and Booster COVID-19 Vaccination, Especially Those with Hematologic Cancer on Active Treatment: A Systematic Review and Meta-Analysis. Cancers 2023, 15, 2266. [Google Scholar] [CrossRef] [PubMed]
- Longitudinal Study—An overview|ScienceDirect Topics. Available online: http://www.sciencedirect.com/topics/neuroscience/longtitudinal-study (accessed on 20 September 2023).


{kind=link}
{kind=link}
| After 2nd Dose | After 3rd Dose | After 4th Dose | |
|---|---|---|---|
| Frequency (n) | 142 | 76 | 25 |
| Age, median years (IQR) | 67 (56.75–75) | 66.5 (57–74.75) | 72 (67.5–79) |
| Male (%) | 78 (54.9) | 43 (56.6) | 15 (60) |
| Time from last BNT162b2 dose, median days (IQR) | 35 (24.5–46.25) | 147 (130.5–160.8) | 18 (12–25) |
| Type of Cancer, n (%) | |||
| Gastrointestinal | 49 (34.5) | 42 (55.3) | 10 (40) |
| Breast | 30 (21.1) | 12 (15.8) | 3 (12) |
| Lung | 28 (19.7) | 10 (22.7) | 6 (24) |
| Urinary | 13 (9.2) | 3 (3.9) | 2 (8) |
| Melanoma | 7 (4.9) | 4 (5.3) | 3 (12) |
| Gynecological | 9 (6.3) | 2 (2.6) | 0 |
| Other types | 6 (4.2) | 3 (3.94) | 1 (4) |
| Treatment, n (%) | |||
| Chemotherapy 1 | 73 (51.4) | 56 (73.7) | 13 (52) |
| Non-chemotherapy 2 | 69 (48.6) | 20 (26.3) | 12 (48) |
| After 2nd | Vaccine | After 3rd | Vaccine | After 4th | Vaccine | |
|---|---|---|---|---|---|---|
| Chemo 1 | Non-Chemo 2 | Chemo | Non-Chemo | Chemo | Non-Chemo | |
| Frequency (n) | 73 | 69 | 56 | 20 | 13 | 12 |
| COVID-19 antibodies response, n (%) | ||||||
| Positive (>21.3 BAU) | 57 (78.1) | 65 | 55 (98.2) | 19 (95) | 13 (100) | 12 (100) |
| Borderline (>7.1 BAU, <21.3 BAU) | 4 (5.5) | 2 (2.9) | 1 (1.8) | 0 | 0 | 0 |
| Negative | 12 (16.4) | 2 (2.9) | 0 | 1 (5) | 0 | 0 |
| Anti-SARS-CoV-2 IgG (BAU/mL), median (IQR) | 316.8 | (63.2–1139.3) | 571.6 | (237.9–1119.5) | 3474 | (176.8–5680) |
| R2A3 | ||||||
| after each vaccine dose | 216.4 (25.3–593.2) | 716.4 (121.5–2023.5) | 620 (214.3–1153.9) | 434.6 (61.76–928.02) | 3019.2 (1043.3–5680) | 3544.5 (2261.3–5243.6) |
| Antibody levels comparison chemo/non-chemo (p) for each vaccine | <0.001 | 0.443 | 0.81 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agbarya, A.; Sarel, I.; Ziv-Baran, T.; Schwartz, O.; Shechtman, Y.; Kozlener, E.; Khoury, R.; Sheikh-Ahmad, M.; Saiegh, L.; Swaid, F.; et al. Response Rate of the Third and Fourth Doses of the BNT162b2 Vaccine Administered to Cancer Patients Undergoing Active Anti-Neoplastic Treatments. Diseases 2023, 11, 128. https://doi.org/10.3390/diseases11040128
Agbarya A, Sarel I, Ziv-Baran T, Schwartz O, Shechtman Y, Kozlener E, Khoury R, Sheikh-Ahmad M, Saiegh L, Swaid F, et al. Response Rate of the Third and Fourth Doses of the BNT162b2 Vaccine Administered to Cancer Patients Undergoing Active Anti-Neoplastic Treatments. Diseases. 2023; 11(4):128. https://doi.org/10.3390/diseases11040128
Chicago/Turabian StyleAgbarya, Abed, Ina Sarel, Tomer Ziv-Baran, Orna Schwartz, Yelena Shechtman, Ella Kozlener, Rasha Khoury, Mohammad Sheikh-Ahmad, Leonard Saiegh, Forat Swaid, and et al. 2023. "Response Rate of the Third and Fourth Doses of the BNT162b2 Vaccine Administered to Cancer Patients Undergoing Active Anti-Neoplastic Treatments" Diseases 11, no. 4: 128. https://doi.org/10.3390/diseases11040128
APA StyleAgbarya, A., Sarel, I., Ziv-Baran, T., Schwartz, O., Shechtman, Y., Kozlener, E., Khoury, R., Sheikh-Ahmad, M., Saiegh, L., Swaid, F., Ahmad, A. A., Janzic, U., & Brenner, R. (2023). Response Rate of the Third and Fourth Doses of the BNT162b2 Vaccine Administered to Cancer Patients Undergoing Active Anti-Neoplastic Treatments. Diseases, 11(4), 128. https://doi.org/10.3390/diseases11040128