
Neutrophil to Lymphocyte Ratio as a Predictor of Postoperative Outcomes in Traumatic Brain Injury: A Systematic Review and Meta-Analysis

 , , ,
, , , 
Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Screening of Studies
2.3. Qualitative Analysis
2.4. Data Charting Process and Data Items
2.5. Statistical Analysis
3. Results
3.1. Qualitative Assessment
3.2. Demographics
3.3. Symptomatic Presentations
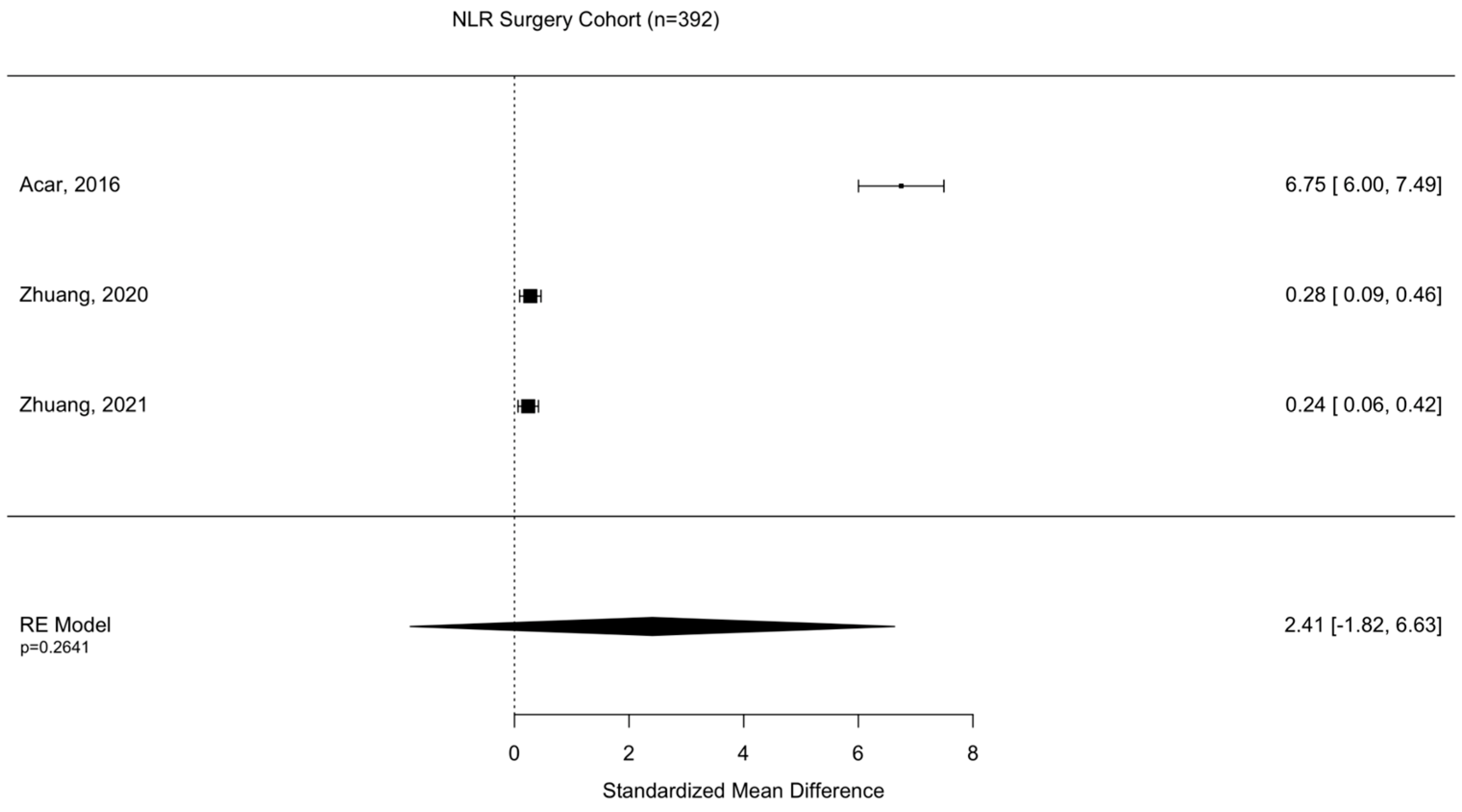
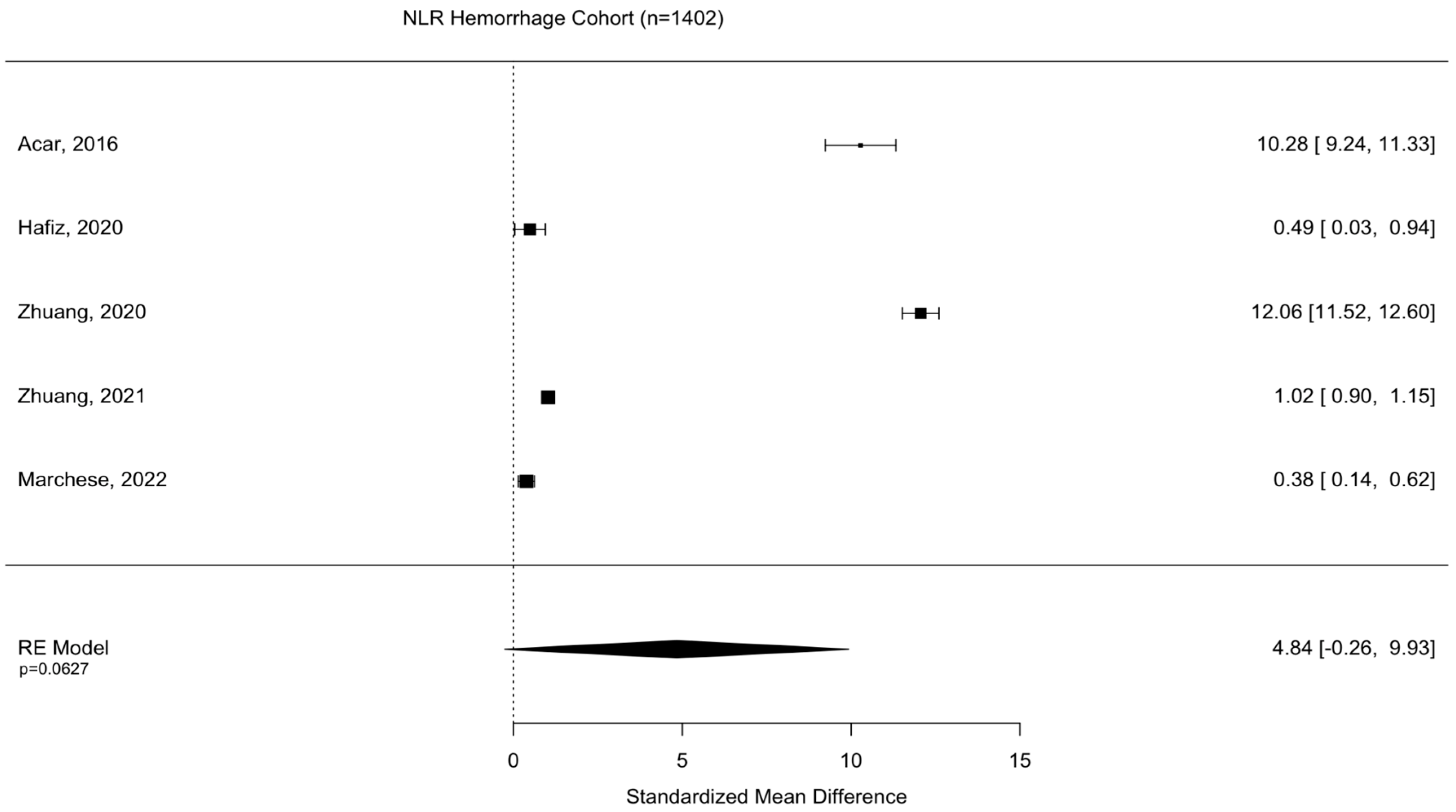
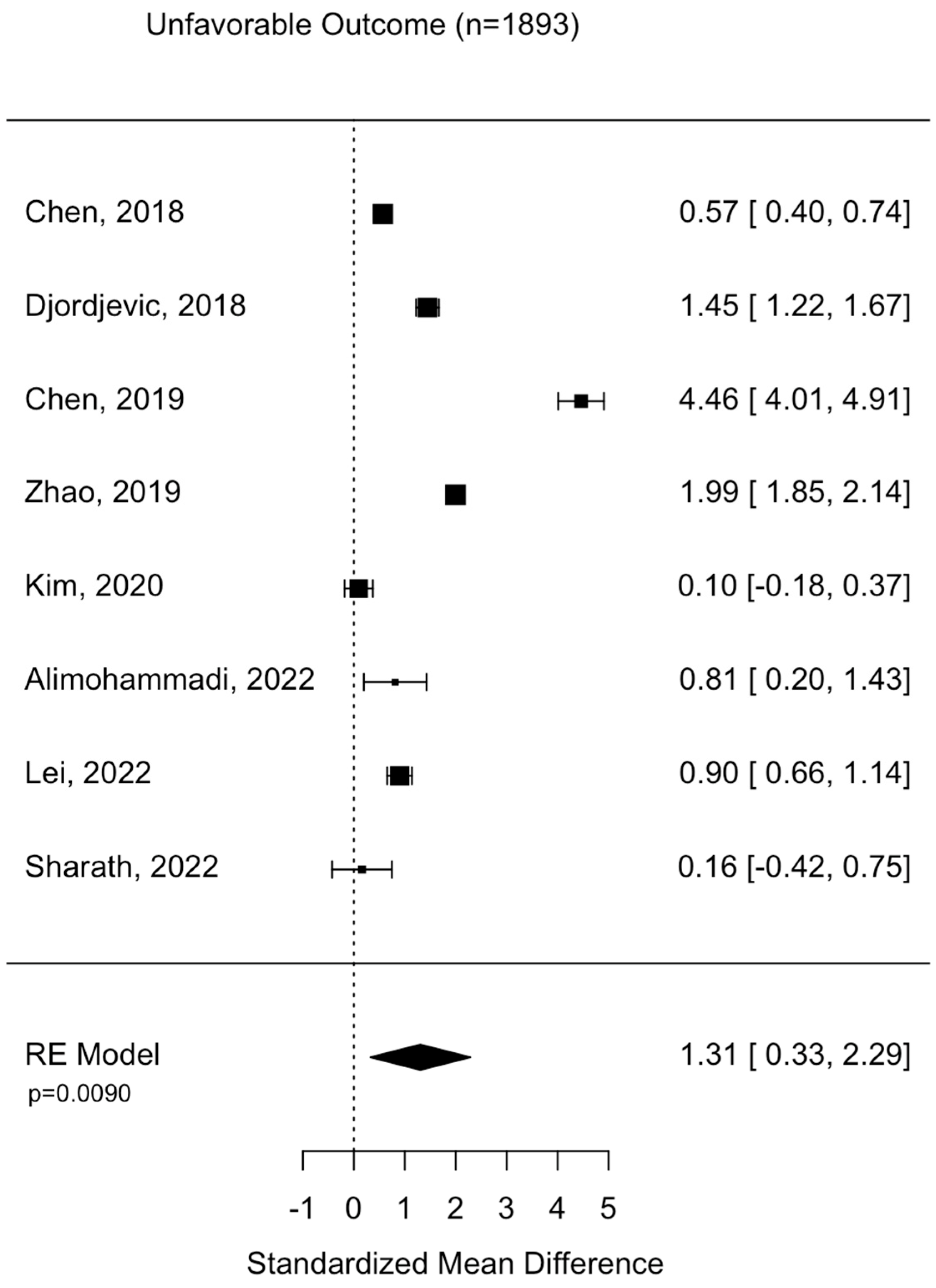
3.4. Surgical Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Galgano, M.; Toshkezi, G.; Qiu, X.; Russell, T.; Chin, L.; Zhao, L.R. Traumatic Brain Injury: Current Treatment Strategies and Future Endeavors. Cell Transplant. 2017, 26, 1118–1130. [Google Scholar] [CrossRef] [PubMed]
- Popescu, C.; Anghelescu, A.; Daia, C.; Onose, G. Actual data on epidemiological evolution and prevention endeavours regarding traumatic brain injury. J. Med. Life 2015, 8, 272–277. [Google Scholar] [PubMed]
- (CDC) CfDCaP. Report to Congress: Traumatic Brain Injury in the United States. Available online: https://www.cdc.gov/traumaticbraininjury/pubs/tbi_report_to_congress.html (accessed on 30 December 2022).
- Werner, C.; Engelhard, K. Pathophysiology of traumatic brain injury. Br. J. Anaesth. 2007, 99, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Dash, H.H.; Chavali, S. Management of traumatic brain injury patients. Korean J. Anesthesiol. 2018, 71, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Vella, M.A.; Crandall, M.L.; Patel, M.B. Acute Management of Traumatic Brain Injury. Surg. Clin. N. Am. 2017, 97, 1015–1030. [Google Scholar] [CrossRef]
- Rowley, G.; Fielding, K. Reliability and accuracy of the Glasgow Coma Scale with experienced and inexperienced users. Lancet 1991, 337, 535–538. [Google Scholar] [CrossRef]
- Defort, P.; Retkowska-Tomaszewska, N.; Kot, M.; Jarmuzek, P.; Tylutka, A.; Zembron-Lacny, A. Inflammatory Predictors of Prognosis in Patients with Traumatic Cerebral Haemorrhage: Retrospective Study. J. Clin. Med. 2022, 11, 705. [Google Scholar] [CrossRef]
- Zahorec, R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl. Lek. Listy 2021, 122, 474–488. [Google Scholar] [CrossRef]
- Toori, K.U.; Qureshi, M.A.; Chaudhry, A.; Safdar, M.F. Neutrophil to lymphocyte ratio (NLR) in COVID-19: A cheap prognostic marker in a resource constraint setting. Pak. J. Med. Sci. 2021, 37, 1435–1439. [Google Scholar] [CrossRef]
- Kilic, M.O.; Gundogdu, S.B.; Ozden, S.; Saylam, B.; Tez, M. The prognostic value of different node staging systems in patients with </=15 lymph nodes following surgery for gastric adenocarcinoma. Acta Chir. Belg. 2018, 118, 1–6. [Google Scholar] [CrossRef]
- Bartlett, E.K.; Flynn, J.R.; Panageas, K.S.; Ferraro, R.A.; Sta Cruz, J.M.; Postow, M.A.; Coit, D.G.; Ariyan, C.E. High neutrophil-to-lymphocyte ratio (NLR) is associated with treatment failure and death in patients who have melanoma treated with PD-1 inhibitor monotherapy. Cancer 2020, 126, 76–85. [Google Scholar] [CrossRef]
- Zhang, Y.; Lu, J.J.; Du, Y.P.; Feng, C.X.; Wang, L.Q.; Chen, M.B. Prognostic value of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in gastric cancer. Medicine 2018, 97, e0144. [Google Scholar] [CrossRef]
- Li, W.; Hou, M.; Ding, Z.; Liu, X.; Shao, Y.; Li, X. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in Stroke: A Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 686983. [Google Scholar] [CrossRef]
- Siwicka-Gieroba, D.; Malodobry, K.; Biernawska, J.; Robba, C.; Bohatyrewicz, R.; Rola, R.; Dabrowski, W. The Neutrophil/Lymphocyte Count Ratio Predicts Mortality in Severe Traumatic Brain Injury Patients. J. Clin. Med. 2019, 8, 1453. [Google Scholar] [CrossRef]
- Levochkina, M.; McQuillan, L.; Awan, N.; Barton, D.; Maczuzak, J.; Bianchine, C.; Trombley, S.; Kotes, E.; Wiener, J.; Wagner, A.; et al. Neutrophil-to-Lymphocyte Ratios and Infections after Traumatic Brain Injury: Associations with Hospital Resource Utilization and Long-Term Outcome. J. Clin. Med. 2021, 10, 4365. [Google Scholar] [CrossRef]
- Chen, J.; Qu, X.; Li, Z.; Zhang, D.; Hou, L. Peak Neutrophil-to-Lymphocyte Ratio Correlates with Clinical Outcomes in Patients with Severe Traumatic Brain Injury. Neurocrit. Care 2019, 30, 334–339. [Google Scholar] [CrossRef]
- von Leden, R.E.; Parker, K.N.; Bates, A.A.; Noble-Haeusslein, L.J.; Donovan, M.H. The emerging role of neutrophils as modifiers of recovery after traumatic injury to the developing brain. Exp. Neurol. 2019, 317, 144–154. [Google Scholar] [CrossRef]
- Clausen, F.; Lorant, T.; Lewen, A.; Hillered, L. T lymphocyte trafficking: A novel target for neuroprotection in traumatic brain injury. J. Neurotrauma 2007, 24, 1295–1307. [Google Scholar] [CrossRef]
- Sabouri, E.; Majdi, A.; Jangjui, P.; Rahigh Aghsan, S.; Naseri Alavi, S.A. Neutrophil-to-Lymphocyte Ratio and Traumatic Brain Injury: A Review Study. World Neurosurg. 2020, 140, 142–147. [Google Scholar] [CrossRef]
- Ghozy, S.; El-Qushayri, A.E.; Varney, J.; Kacimi SE, O.; Bahbah, E.I.; Morra, M.E.; Shah, J.; Kallmes, K.M.; Abbas, A.S.; Elfil, M.; et al. The prognostic value of neutrophil-to-lymphocyte ratio in patients with traumatic brain injury: A systematic review. Front. Neurol. 2022, 13, 1021877. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Acar, E.; Demir, A.; Alatas, Ö.D.; Beydilli, H.; Yıldırım, B.; Kırlı, U.; Hazer, D.B.; Kılınç, M.R.; Karagöz, Ü.; Derin, S.; et al. Evaluation of hematological markers in minor head trauma in the emergency room. Eur. J. Trauma Emerg. Surg. 2016, 42, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Yang, J.; Li, B.; Peng, G.; Li, T.; Li, L.; Wang, S. Neutrophil to lymphocyte ratio as a novel predictor of outcome in patients with severe traumatic brain injury. J. Head Trauma Rehabil. 2018, 33, E53–E59. [Google Scholar] [CrossRef] [PubMed]
- Djordjevic, D.; Rondovic, G.; Surbatovic, M.; Stanojevic, I.; Udovicic, I.; Andjelic, T.; Zeba, S.; Milosavljevic, S.; Stankovic, N.; Abazovic, D.; et al. Neutrophil-to-Lymphocyte Ratio, Monocyte-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, and Mean Platelet Volume-to-Platelet Count Ratio as Biomarkers in Critically Ill and Injured Patients: Which Ratio to Choose to Predict Outcome and Nature of Bacteremia? Mediators Inflamm. 2018, 2018, 3758068. [Google Scholar] [CrossRef]
- Ge, X.; Zhu, L.; Li, M.; Li, W.; Chen, F.; Li, Y.; Zhang, J.; Lei, P. A Novel Blood Inflammatory Indicator for Predicting Deterioration Risk of Mild Traumatic Brain Injury. Front. Aging Neurosci. 2022, 14, 878484. [Google Scholar] [CrossRef]
- Zhao, J.L.; Du, Z.Y.; Yuan, Q.; Yu, J.; Sun, Y.R.; Wu, X.; Li, Z.-L.; Wu, X.H.; Hu, J. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in Predicting the 6-Month Outcome of Patients with Traumatic Brain Injury: A Retrospective Study. World Neurosurg. 2019, 124, e411–e416. [Google Scholar] [CrossRef]
- Alexiou, G.A.; Lianos, G.D.; Tzima, A.; Sotiropoulos, A.; Nasios, A.; Metaxas, D.; Zigouris, A.; Zika, J.; Mitsis, M.; Voulgaris, S. Neutrophil to lymphocyte ratio as a predictive biomarker for computed tomography scan use in mild traumatic brain injury. Biomark. Med. 2020, 14, 1085–1090. [Google Scholar] [CrossRef]
- Kim, N.Y.; Lim, J.; Lee, S.; Kim, K.; Hong, J.H.; Chun, D.H. Hematological factors predicting mortality in patients with traumatic epidural or subdural hematoma undergoing emergency surgical evacuation: A retrospective cohort study. Medicine 2020, 99, e22074. [Google Scholar] [CrossRef]
- Kusuma, G.F.P.; Mahadewa, T.G.B.; Senapathi, T.G.A.; Lestari, A.A.W.; Muliarta, I.M. Neutrophil-to-lymphocyte Ratio and Platelet-to-lymphocyte Ratio Correlations with C-reactive Protein and Erythrocyte Sedimentation Rate in Traumatic Brain Injury. Open Access Maced. J. Med. Sci. 2020, 8, 574–583. [Google Scholar] [CrossRef]
- Hafiz MZ, A.; Saanin, S.; Ningsih, H.L. Comparison of Lymphocyte Neutrophil Ratio in Head Injury Patients with Blood and without Intracranial Bleeding in Dr. M. Djamil Hospital. Biomed. J. Indones. 2021, 7, 164–180. [Google Scholar] [CrossRef]
- Sharath, M.; Siddegowda, R.B.; Lonimath, A.; Cheluvaiah, J.D. An Elevated Neutrophil-to-Lymphocyte Ratio Predicts In-Hospital Mortality in Stroke Patients: A Prospective Cohort Study. Cureus 2022, 14, e31372. [Google Scholar] [CrossRef]
- Zhuang, D.; Sheng, J.; Peng, G.; Li, T.; Cai, S.; Ding, F.; Li, L.; Huang, M.; Tian, F.; Li, K.; et al. Neutrophil-to-Lymphocyte Ratio at Hospital Admission as a Novel Predictor of Early Growth of Intraprenchymal Haemorrhage in Patients with Traumatic Brain Injury. Res. Square 2020. [Google Scholar] [CrossRef]
- Le Bail, A.; Jardine, C.G.; Cottenceau, V.; Petit, L.; Matthieu, B.; Carrie, C. Ability of neutrophil-to-lymphocyte ratio to predict secondary neurological impairment in patients with mild to moderate head injury. A retrospective study. Am. J. Emerg. Med. 2021, 50, 46–50. [Google Scholar] [CrossRef]
- Chen, Y.; Tian, J.; Chi, B.; Zhang, S.; Wei, L.; Wang, S. Factors Associated with the Development of Coagulopathy after Open Traumatic Brain Injury. J. Clin. Med. 2021, 11, 185. [Google Scholar] [CrossRef]
- Zhuang, D.; Sheng, J.; Peng, G.; Li, T.; Cai, S.; Din, F.; Li, L.; Huang, M.; Tian, F.; Li, K.; et al. Neutrophil to lymphocyte ratio predicts early growth of traumatic intracerebral haemorrhage. Ann. Clin. Transl. Neurol. 2021, 8, 1601–1609. [Google Scholar] [CrossRef]
- Alimohammadi, E.; Foroushani, A.Z.; Moradi, F.; Ebrahimzadeh, K.; Nadersepahi, M.J.; Asadzadeh, S.; Amiri, A.; Hosseini, S.; Eden, S.V.; Bagheri, S.R. Dynamics of neutrophil-to-lymphocyte ratio can be associated with clinical outcomes of children with moderate to severe traumatic brain injury: A retrospective observational study. Injury 2022, 53, 999–1004. [Google Scholar] [CrossRef]
- Marchese, P.; Lardone, C.; Canepele, A.; Biondi, S.; Roggi, C.; Massart, F.; Bonuccelli, A.; Peroni, D.G.; Lucifero, A.G.; Luzzi, S.; et al. Pediatric traumatic brain injury: A new relation between outcome and neutrophil-to-lymphocite ratio. Acta Biomed. 2022, 92, e2021417. [Google Scholar] [CrossRef]
- Lei, J.; Zhang, X.; Tan, R.; Li, Y.; Zhao, K.; Niu, H. Levels of lncRNA GAS5 in Plasma of Patients with Severe Traumatic Brain Injury: Correlation with Systemic Inflammation and Early Outcome. J. Clin. Med. 2022, 11, 3319. [Google Scholar] [CrossRef]
- Forget, P.; Khalifa, C.; Defour, J.P.; Latinne, D.; Van Pel, M.C.; De Kock, M. What is the normal value of the neutrophil-to-lymphocyte ratio? BMC Res. Notes 2017, 10, 12. [Google Scholar] [CrossRef]
- Wang, J. Neutrophils in tissue injury and repair. Cell Tissue Res. 2018, 371, 531–539. [Google Scholar] [CrossRef]
- Kimball, R.; Shachar, E.; Eyerly-Webb, S.; Patel, D.M.; Spader, H. Using the neutrophil-to-lymphocyte ratio to predict outcomes in pediatric patients with traumatic brain injury. Clin. Neurol. Neurosurg. 2020, 193, 105772. [Google Scholar] [CrossRef] [PubMed]
- Butterfield, T.A.; Best, T.M.; Merrick, M.A. The dual roles of neutrophils and macrophages in inflammation: A critical balance between tissue damage and repair. J. Athl. Train. 2006, 41, 457–465. [Google Scholar] [PubMed]
- Watanabe, S.; Alexander, M.; Misharin, A.V.; Budinger, G.R.S. The role of macrophages in the resolution of inflammation. J. Clin. Investig. 2019, 129, 2619–2628. [Google Scholar] [CrossRef]
- Schuijs, M.J.; Hammad, H.; Lambrecht, B.N. Professional and ‘Amateur’ Antigen-Presenting Cells In Type 2 Immunity. Trends Immunol. 2019, 40, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.D.; Nedjai, B.; Hurst, T.; Pennington, D.J. Cytokines and chemokines: At the crossroads of cell signalling and inflammatory disease. Biochim. Biophys. Acta. 2014, 1843, 2563–2582. [Google Scholar] [CrossRef]
- Berger, A. Th1 and Th2 responses: What are they? BMJ 2000, 321, 424. [Google Scholar] [CrossRef]
- Yunna, C.; Mengru, H.; Lei, W.; Weidong, C. Macrophage M1/M2 polarization. Eur. J. Pharmacol. 2020, 877, 173090. [Google Scholar] [CrossRef]
- McHugh, R.S.; Shevach, E.M. The role of suppressor T cells in regulation of immune responses. J. Allergy Clin. Immunol. 2002, 110, 693–702. [Google Scholar] [CrossRef]
- Burn, G.L.; Foti, A.; Marsman, G.; Patel, D.F.; Zychlinsky, A. The Neutrophil. Immunity 2021, 54, 1377–1391. [Google Scholar] [CrossRef]
- McMillan, T.; Wilson, L.; Ponsford, J.; Levin, H.; Teasdale, G.; Bond, M. The Glasgow Outcome Scale—40 years of application and refinement. Nat. Rev. Neurol. 2016, 12, 477–485. [Google Scholar] [CrossRef]
- Yamal, J.M.; Hannay, H.J.; Gopinath, S.; Aisiku, I.P.; Benoit, J.S.; Robertson, C.S. Glasgow Outcome Scale Measures and Impact on Analysis and Results of a Randomized Clinical Trial of Severe Traumatic Brain Injury. J. Neurotrauma 2019, 36, 2484–2492. [Google Scholar] [CrossRef]
- Wilson, J.T.; Pettigrew, L.E.; Teasdale, G.M. Emotional and cognitive consequences of head injury in relation to the glasgow outcome scale. J. Neurol. Neurosurg Psychiatry 2000, 69, 204–209. [Google Scholar] [CrossRef]
- Profaci, C.P.; Munji, R.N.; Pulido, R.S.; Daneman, R. The blood-brain barrier in health and disease: Important unanswered questions. J. Exp. Med. 2020, 217, e20190062. [Google Scholar] [CrossRef]
- Daneman, R.; Prat, A. The blood-brain barrier. Cold Spring Harb. Perspect. Biol. 2015, 7, a020412. [Google Scholar] [CrossRef]
- Rauf, A.; Badoni, H.; Abu-Izneid, T.; Olatunde, A.; Rahman, M.M.; Painuli, S.; Semwal, P.; Wilairatana, P.; Mubarak, M.S. Neuroinflammatory Markers: Key Indicators in the Pathology of Neurodegenerative Diseases. Molecules 2022, 27, 3194. [Google Scholar] [CrossRef]
- George-Gay, B.; Parker, K. Understanding the complete blood count with differential. J. Perianesth. Nurs. 2003, 18, 96–114; quiz 115–1157. [Google Scholar] [CrossRef]
- Abbott, N.J.; Patabendige, A.A.; Dolman, D.E.; Yusof, S.R.; Begley, D.J. Structure and function of the blood-brain barrier. Neurobiol. Dis. 2010, 37, 13–25. [Google Scholar] [CrossRef]
- Obermeier, B.; Daneman, R.; Ransohoff, R.M. Development, maintenance and disruption of the blood-brain barrier. Nat. Med. 2013, 19, 1584–1596. [Google Scholar] [CrossRef]
- Candelario-Jalil, E.; Dijkhuizen, R.M.; Magnus, T. Neuroinflammation, Stroke, Blood-Brain Barrier Dysfunction, and Imaging Modalities. Stroke 2022, 53, 1473–1486. [Google Scholar] [CrossRef]
- Hariri, R.J. Cerebral edema. Neurosurg. Clin. N. Am. 1994, 5, 687–706. [Google Scholar] [CrossRef]
- Zheng, H.; Chen, C.; Zhang, J.; Hu, Z. Mechanism and Therapy of Brain Edema after Intracerebral Hemorrhage. Cerebrovasc. Dis. 2016, 42, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Papayannopoulos, V. Neutrophil extracellular traps in immunity and disease. Nat. Rev. Immunol. 2018, 18, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Manda-Handzlik, A.; Demkow, U. The Brain Entangled: The Contribution of Neutrophil Extracellular Traps to the Diseases of the Central Nervous System. Cells 2019, 8, 1477. [Google Scholar] [CrossRef] [PubMed]
- Monson, K.L.; Converse, M.I.; Manley, G.T. Cerebral blood vessel damage in traumatic brain injury. Clin. Biomech. 2019, 64, 98–113. [Google Scholar] [CrossRef]
- Mehta, V.; Harward, S.C.; Sankey, E.W.; Nayar, G.; Codd, P.J. Evidence based diagnosis and management of chronic subdural hematoma: A review of the literature. J. Clin. Neurosci. 2018, 50, 7–15. [Google Scholar] [CrossRef]
- Cooper, P.R. Delayed traumatic intracerebral hemorrhage. Neurosurg. Clin. N. Am. 1992, 3, 659–665. [Google Scholar] [CrossRef]
- Zarmehri, B.; Shahi, B.; Rahmani, S.; Dehghan Tafti, F.; Foroughian, M. Association of platelet count and mean platelet volume (MPV) index with types of stroke. Caspian J. Int. Med. 2020, 11, 398–402. [Google Scholar] [CrossRef]
- Yuan, B.; Yang, T.; Yan, T.; Cheng, W.; Bu, X. Relationships Between D-Dimer Levels and Stroke Risk as Well as Adverse Clinical Outcomes After Acute Ischemic Stroke or Transient Ischemic Attack: A Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 670730. [Google Scholar] [CrossRef]
- Qu, D.; Li, W.; Zhang, S.; Li, R.; Wang, H.; Chen, B. Traumatic Brain Injury Is Associated With Both Hemorrhagic Stroke and Ischemic Stroke: A Systematic Review and Meta-Analysis. Front. Neurosci. 2022, 16, 2. [Google Scholar] [CrossRef]
- Sezer, C.; Gokten, M.; Acıkalın, R. Troponin I New Biomarker in Traumatic Brain Injury. Indian J. Surg. 2022, 85, 120–126. [Google Scholar] [CrossRef]
- Karibe, H.; Hayashi, T.; Hirano, T.; Kameyama, M.; Nakagawa, A.; Tominaga, T. Surgical management of traumatic acute subdural hematoma in adults: A review. Neurol. Med. Chir. 2014, 54, 887–894. [Google Scholar] [CrossRef]
- Mendelow, A.D.; Gregson, B.A.; Rowan, E.N.; Francis, R.; McColl, E.; McNamee, P.; Chambers, I.R.; Unterberg, A.; Boyers, D.; Mitchell, P.M.; et al. Early Surgery versus Initial Conservative Treatment in Patients with Traumatic Intracerebral Hemorrhage (STITCH[Trauma]): The First Randomized Trial. J. Neurotrauma 2015, 32, 1312–1323. [Google Scholar] [CrossRef]
- Kellner, C.P.; Schupper, A.J.; Mocco, J. Surgical Evacuation of Intracerebral Hemorrhage: The Potential Importance of Timing. Stroke 2021, 52, 3391–3398. [Google Scholar] [CrossRef]
- Kirkman, M.A.; Smith, M. Intracranial pressure monitoring, cerebral perfusion pressure estimation, and ICP/CPP-guided therapy: A standard of care or optional extra after brain injury? Br. J. Anaesth. 2014, 112, 35–46. [Google Scholar] [CrossRef]
- Marin, B.S.; Cesena, F.; Laurinavicius, A.G.; Santos, R.D.; Bittencourt, M.S. Neutrophil-To-Lymphocyte Ratio and Abdominal Aortic Atherosclerosis among Asymptomatic Individuals. Arq. Bras. Cardiol. 2022, 118, 729–734. [Google Scholar] [CrossRef]
- Ferrucci, L.; Fabbri, E. Inflammageing: Chronic inflammation in ageing, cardiovascular disease, and frailty. Nat. Rev. Cardiol. 2018, 15, 505–522. [Google Scholar] [CrossRef]
- Herrero-Cervera, A.; Soehnlein, O.; Kenne, E. Neutrophils in chronic inflammatory diseases. Cell. Mol. Immunol. 2022, 19, 177–191. [Google Scholar] [CrossRef]
- Yeatts, S.D.; Martin, R.H.; Meurer, W.; Silbergleit, R.; Rockswold, G.L.; Barsan, W.G.; Korley, F.K.; Wright, D.W.; Gajewski, B.J. Sliding Scoring of the Glasgow Outcome Scale-Extended as Primary Outcome in Traumatic Brain Injury Trials. J. Neurotrauma 2020, 37, 2674–2679. [Google Scholar] [CrossRef]
- Sharon DYeatts, Y.Y.P.; Temkin, N. Chapter 9—Biostatistical issues in TBI clinical trials. In Handbook of Neuroemergency Clinical Trials, 2nd ed.; Academic Press: Cambridge, MA, USA, 2018; pp. 167–185. [Google Scholar]
- Price, M.; Hertzberg, V.; Wright, D.W. Does the sliding dichotomy result in higher powered clinical trials for stroke and traumatic brain injury research? Clin. Trials. 2013, 10, 924–934. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Selection | Comparability | Outcome | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Cohort/Case Series | ||||||||||
| Author and Year | Study Type | Representativeness of the exposed cohort | Selection of the non-exposed cohort | Ascertainment of exposure | Demonstration that outcome of interest was not present at the start of the study | Comparability of cohorts on the basis of the design or analysis | Assessment of outcome | Was follow-up long enough for outcomes to occur | Adequacy of follow-up of cohorts | Total |
| Chen, 2018 [24] | RC | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| Djordevic, 2018 [25] | PC | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| Chen, 2019 [17] | RC | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| Ge, 2022 [26] | RC | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 5 |
| Zhao, 2019 [27] | RC | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| Alexiou, 2020 [28] | RC | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 6 |
| Kim, 2020 [29] | RC | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| Kusuma, 2020 [30] | CS | 1 | N/A | 1 | 1 | NA | 1 | 0 | 1 | 5 |
| Hafiz, 2020 [31] | RC | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 6 |
| Sharath, 2022 [32] | PC | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 5 |
| Zhuang, 2020 [33] | RC, PC | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 6 |
| Bail, 2021 [34] | RC | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 6 |
| Chen, 2021 [35] | RC | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 6 |
| Zhuang, 2021 [36] | RC | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 6 |
| Alimohammadi, 2022 [37] | RC | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 6 |
| Defort, 2022 [8] | RC | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 6 |
| Case-Control | ||||||||||
| Selection | Comparability | Outcome | ||||||||
| Author and Year | Study Type | Is the case definition adequate | Representativeness of the cases | Selection of Controls | Definition of Controls | Comparability of cases and controls on the basis of the design or analysis | Ascertainment of exposure | Same method of ascertainment for cases and controls | Non-Response rate | Total |
| Acar, 2016 [23] | CC | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| Marchese, 2022 [38] | CC | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| Lei, 2022 [39] | CC | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
| Author, Year | Study Design | Country | Age (Years) | Age SD | Male | Female |
|---|---|---|---|---|---|---|
| Acar, 2016 [23] | Case-control | Turkey | NA | NA | 151 | 49 |
| Chen, 2018 [24] | Retrospective Cohort | China | 45.4 | 14.85 | 557 | 131 |
| Djordevic, 2018 [25] | Prospective Cohort | Serbia | 53.67 | 18.26 | 236 | 156 |
| Chen, 2019 [17] | Retrospective Cohort | China | 56 | NA | 256 | 60 |
| Zhao, 2019 [27] | Retrospective Cohort | China | 47.03 | 16.88 | 982 | 309 |
| Alexiou, 2020 [28] | Case-control | Greece | 61.6 | 19.9 | 85 | 45 |
| Kim, 2020 [29] | Retrospective Cohort | South Korea | 56.77 | NA | 155 | 45 |
| Kusuma, 2020 [30] | Cross-sectional | Indonesia | 38.89 | 15.27 | 66 | 19 |
| Hafiz, 2021 [29] | Retrospective Cohort | Indonesia | 32.34 | 21.67 | 64 | 64 |
| Zhuang, 2020 [30] | Mixed Retrospective and Prospective Cohort | China | 48.3 | NA | 764 | 239 |
| Bail, 2021 [34] | Retrospective Cohort | France | 54 | NA | 88 | 27 |
| Chen, 2021 [35] | Retrospective Cohort | China | 44.5 | NA | 113 | 19 |
| Zhuang, 2021 [36] | Retrospective Cohort | China | 48.63 | 17.92 | 815 | 262 |
| Alimohammadi, 2022 [37] | Retrospective Cohort | Iran | 7.37 | 3.11 | 197 | 197 |
| Defort, 2022 [8] | Retrospective Cohort | Poland | 46.37 | 18.7 | 79 | 16 |
| Ge, 2022 [26] | Retrospective Cohort | China | 53.27 | 16.27 | 663 | 329 |
| Lei, 2022 [39] | Case-control | China | 51.1 | 15.2 | 33 | 12 |
| Marchese, 2022 [38] | Case-control | Italy | 11.54 | 4.79 | 150 | 69 |
| Sharath, 2022 [32] | Prospective Cohort | India | 63.37 | NA | 31 | 29 |
| Total or Mean | 46.25 | 9.77 | 5487 | 2021 |
| Presenting Symptom | Percentage |
|---|---|
| Headache | 2.73% |
| Vomiting | 0.67% |
| Neurological Deficit | 11.46% |
| LOC | 3.23% |
| Amnesia | 3.11% |
| Psychomotor Agitation | 0.35% |
| Hypotension | 4.87% |
| Pupillary Abnormality | 16.30% |
| Seizure | 2.88% |
| Surgery | Bleed | Outcome (Unfavorable) | |
|---|---|---|---|
| Total/Average | 31.4% | 52.4% | 49.1% |
| Overall effect | SMD 2.41 95% CI −1.82 to 6.63 p = 0.2641 | SMD 4.84 95% CI −0.26 to 9.93 p = 0.0627 | SMD 1.31 95% CI 0.33 to 2.29 p = 0.0090 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, A.; Nguyen, A.; Hsu, T.I.; Lew, H.D.; Gupta, N.; Nguyen, B.; Mandavalli, A.; Diaz, M.J.; Lucke-Wold, B. Neutrophil to Lymphocyte Ratio as a Predictor of Postoperative Outcomes in Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Diseases 2023, 11, 51. https://doi.org/10.3390/diseases11010051
Nguyen A, Nguyen A, Hsu TI, Lew HD, Gupta N, Nguyen B, Mandavalli A, Diaz MJ, Lucke-Wold B. Neutrophil to Lymphocyte Ratio as a Predictor of Postoperative Outcomes in Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Diseases. 2023; 11(1):51. https://doi.org/10.3390/diseases11010051
Chicago/Turabian StyleNguyen, Andrew, Alexander Nguyen, Timothy I. Hsu, Harrison D. Lew, Nithin Gupta, Brandon Nguyen, Akhil Mandavalli, Michael J. Diaz, and Brandon Lucke-Wold. 2023. "Neutrophil to Lymphocyte Ratio as a Predictor of Postoperative Outcomes in Traumatic Brain Injury: A Systematic Review and Meta-Analysis" Diseases 11, no. 1: 51. https://doi.org/10.3390/diseases11010051
APA StyleNguyen, A., Nguyen, A., Hsu, T. I., Lew, H. D., Gupta, N., Nguyen, B., Mandavalli, A., Diaz, M. J., & Lucke-Wold, B. (2023). Neutrophil to Lymphocyte Ratio as a Predictor of Postoperative Outcomes in Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Diseases, 11(1), 51. https://doi.org/10.3390/diseases11010051