
A Comprehensive Review of the Neurological Manifestations of Celiac Disease and Its Treatment

 , , , and
, , , and 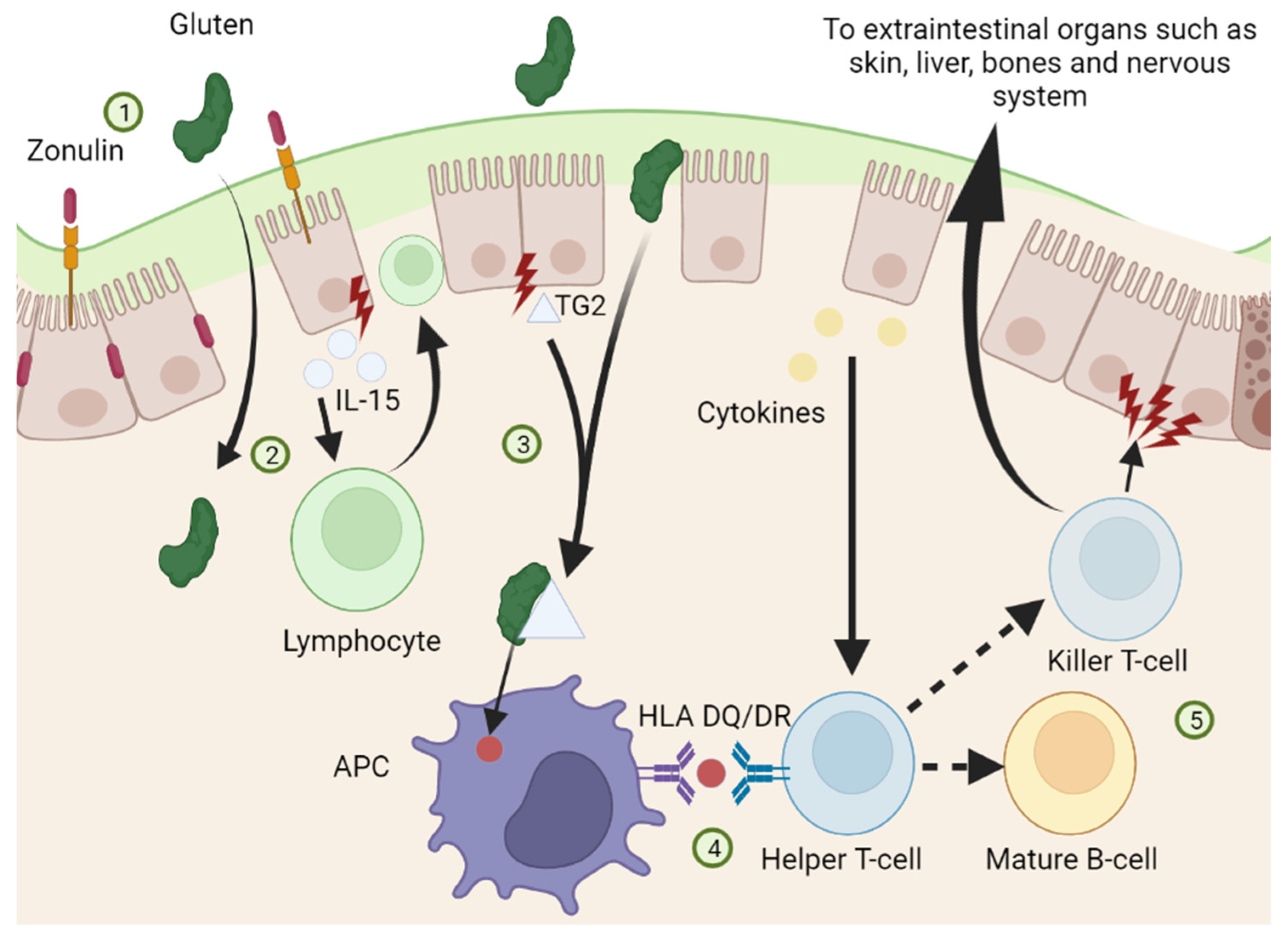{kind=link}
{kind=link}
Abstract
1. Celiac Disease
1.1. Introduction
1.2. Pathophysiology
1.3. Extraintestinal Manifestations
2. Neurological Manifestations of Celiac Disease
2.1. Introduction
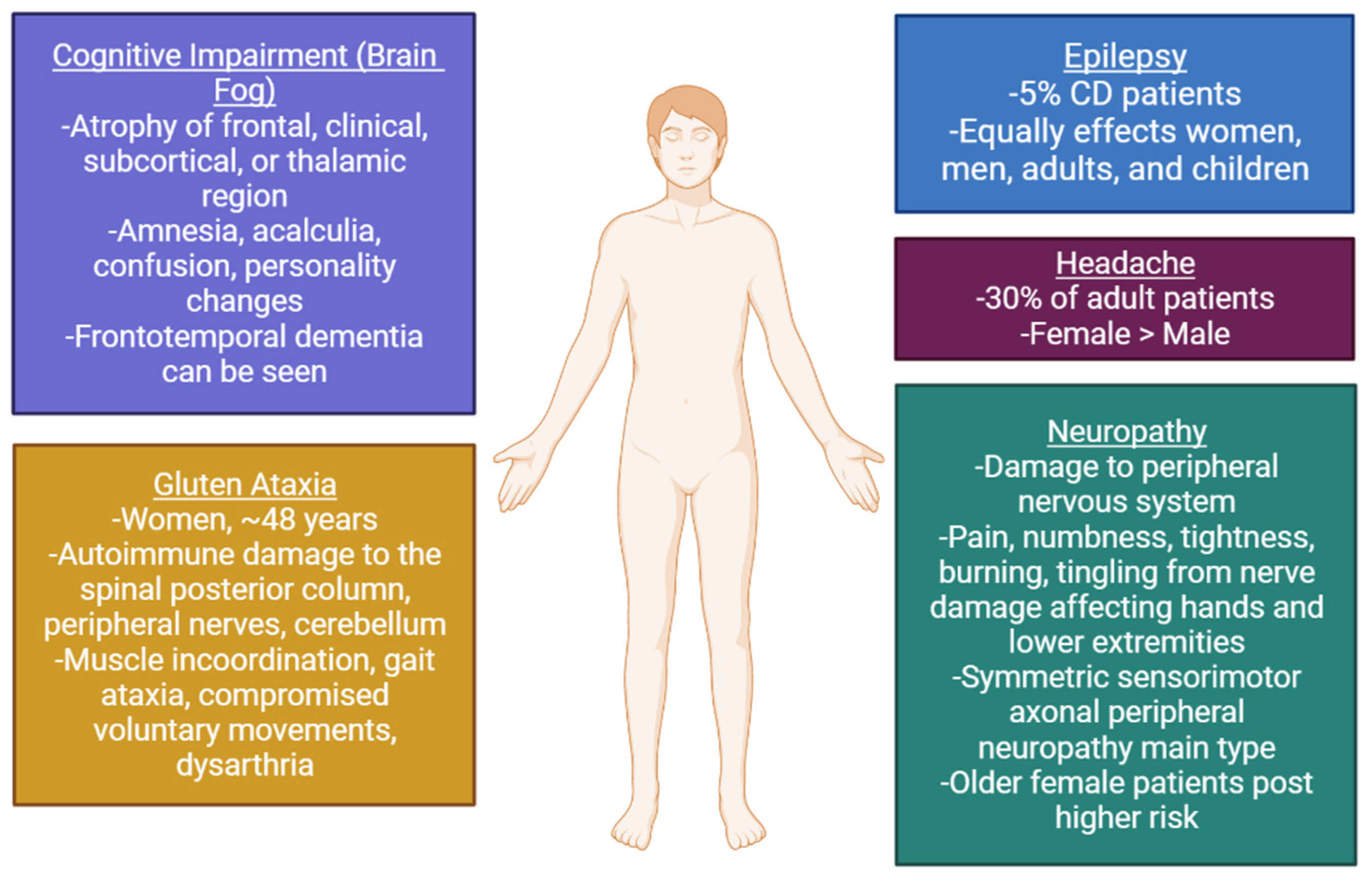
2.2. Gluten Ataxia
2.3. Epilepsy
2.4. Headache
2.5. Neuropathy
2.6. Cognitive Impairment (“Brain Fog”)
3. Treatment of Celiac Disease
3.1. Introduction
3.2. Tight Junction Integrity
3.3. Oral Enzyme Therapies
3.4. Transglutaminase 2 Inhibition
3.5. Immunotherapy and Vaccines
3.6. Treatment for Neurological Manifestations of Celiac Disease
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Husby, S.; Koletzko, S.; Korponay-Szabo, I.; Kurppa, K.; Mearin, M.L.; Ribes-Koninckx, C.; Shamir, R.; Troncone, R.; Auricchio, R.; Castillejo, G.; et al. European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 141–156. [Google Scholar] [CrossRef] [PubMed]
- Parzanese, I.; Qehajaj, D.; Patrinicola, F.; Aralica, M.; Chiriva-Internati, M.; Stifter, S.; Elli, L.; Grizzi, F. Celiac disease: From pathophysiology to treatment. World J. Gastrointest. Pathophysiol. 2017, 8, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Elli, L.; Branchi, F.; Tomba, C.; Villalta, D.; Norsa, L.; Ferretti, F.; Roncoroni, L.; Bardella, M.T. Diagnosis of gluten related disorders: Celiac disease, wheat allergy and non-celiac gluten sensitivity. World J. Gastroenterol. 2015, 21, 7110–7119. [Google Scholar] [CrossRef] [PubMed]
- Ehsani-Ardakani, M.J.; Rostami Nejad, M.; Villanacci, V.; Volta, U.; Manenti, S.; Caio, G.; Giovenali, P.; Becheanu, G.; Diculescu, M.; Pellegrino, S.; et al. Gastrointestinal and non-gastrointestinal presentation in patients with celiac disease. Arch. Iran. Med. 2013, 16, 78–82. [Google Scholar] [PubMed]
- Kreutz, J.M.; Adriaanse, M.P.M.; van der Ploeg, E.M.C.; Vreugdenhil, A.C.E. Narrative Review: Nutrient Deficiencies in Adults and Children with Treated and Untreated Celiac Disease. Nutrients 2020, 12, 500. [Google Scholar] [CrossRef]
- Tye-Din, J.A.; Galipeau, H.J.; Agardh, D. Celiac Disease: A Review of Current Concepts in Pathogenesis, Prevention, and Novel Therapies. Front. Pediatr. 2018, 6, 350. [Google Scholar] [CrossRef]
- Aronsson, C.A.; Lee, H.S.; Liu, E.; Uusitalo, U.; Hummel, S.; Yang, J.; Hummel, M.; Rewers, M.; She, J.X.; Simell, O.; et al. Age at gluten introduction and risk of celiac disease. Pediatrics 2015, 135, 239–245. [Google Scholar] [CrossRef]
- Marild, K.; Kahrs, C.R.; Tapia, G.; Stene, L.C.; Stordal, K. Infections and risk of celiac disease in childhood: A prospective nationwide cohort study. Am. J. Gastroenterol. 2015, 110, 1475–1484. [Google Scholar] [CrossRef]
- Loponen, J.; Sontag-Strohm, T.; Venalainen, J.; Salovaara, H. Prolamin hydrolysis in wheat sourdoughs with differing proteolytic activities. J. Agric. Food Chem. 2007, 55, 978–984. [Google Scholar] [CrossRef]
- Stadlmann, V.; Harant, H.; Korschineck, I.; Hermann, M.; Forster, F.; Missbichler, A. Novel avian single-chain fragment variable (scFv) targets dietary gluten and related natural grain prolamins, toxic entities of celiac disease. BMC Biotechnol. 2015, 15, 109. [Google Scholar] [CrossRef]
- Skovbjerg, H.; Koch, C.; Anthonsen, D.; Sjostrom, H. Deamidation and cross-linking of gliadin peptides by transglutaminases and the relation to celiac disease. Biochim. Biophys. Acta 2004, 1690, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Petersen, J.; Ciacchi, L.; Tran, M.T.; Loh, K.L.; Kooy-Winkelaar, Y.; Croft, N.P.; Hardy, M.Y.; Chen, Z.; McCluskey, J.; Anderson, R.P.; et al. T cell receptor cross-reactivity between gliadin and bacterial peptides in celiac disease. Nat. Struct. Mol. Biol. 2020, 27, 49–61. [Google Scholar] [CrossRef]
- Zanoni, G.; Navone, R.; Lunardi, C.; Tridente, G.; Bason, C.; Sivori, S.; Beri, R.; Dolcino, M.; Valletta, E.; Corrocher, R.; et al. In celiac disease, a subset of autoantibodies against transglutaminase binds toll-like receptor 4 and induces activation of monocytes. PLoS Med. 2006, 3, e358. [Google Scholar] [CrossRef] [PubMed]
- Tuckova, L.; Tlaskalova-Hogenova, H.; Farre, M.A.; Karska, K.; Rossmann, P.; Kolinska, J.; Kocna, P. Molecular mimicry as a possible cause of autoimmune reactions in celiac disease? Antibodies to gliadin cross-react with epitopes on enterocytes. Clin. Immunol. Immunopathol. 1995, 74, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Rojas, M.; Restrepo-Jimenez, P.; Monsalve, D.M.; Pacheco, Y.; Acosta-Ampudia, Y.; Ramirez-Santana, C.; Leung, P.S.C.; Ansari, A.A.; Gershwin, M.E.; Anaya, J.M. Molecular mimicry and autoimmunity. J. Autoimmun. 2018, 95, 100–123. [Google Scholar] [CrossRef] [PubMed]
- Segal, Y.; Shoenfeld, Y. Vaccine-induced autoimmunity: The role of molecular mimicry and immune crossreaction. Cell. Mol. Immunol. 2018, 15, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Rampertab, S.D.; Pooran, N.; Brar, P.; Singh, P.; Green, P.H. Trends in the presentation of celiac disease. Am. J. Med. 2006, 119, 355.e9–355.e14. [Google Scholar] [CrossRef]
- Paez, M.A.; Gramelspacher, A.M.; Sinacore, J.; Winterfield, L.; Venu, M. Delay in Diagnosis of Celiac Disease in Patients Without Gastrointestinal Complaints. Am. J. Med. 2017, 130, 1318–1323. [Google Scholar] [CrossRef]
- Lucendo, A.J.; Garcia-Manzanares, A. Bone mineral density in adult coeliac disease: An updated review. Rev. Esp. Enferm. Dig. 2013, 105, 154–162. [Google Scholar] [CrossRef]
- Larussa, T.; Suraci, E.; Nazionale, I.; Abenavoli, L.; Imeneo, M.; Luzza, F. Bone mineralization in celiac disease. Gastroenterol. Res. Pract. 2012, 2012, 198025. [Google Scholar] [CrossRef]
- Daron, C.; Soubrier, M.; Mathieu, S. Occurrence of rheumatic symptoms in celiac disease: A meta-analysis: Comment on the article “Osteoarticular manifestations of celiac disease and non-celiac gluten hypersensitivity” by Dos Santos and Liote. Joint Bone Spine 2016, doi:10.1016/j.jbspin.2016.09.007. Jt. Bone Spine 2017, 84, 645–646. [Google Scholar] [CrossRef]
- Gorog, A.; Antiga, E.; Caproni, M.; Cianchini, G.; De, D.; Dmochowski, M.; Dolinsek, J.; Drenovska, K.; Feliciani, C.; Hervonen, K.; et al. S2k guidelines (consensus statement) for diagnosis and therapy of dermatitis herpetiformis initiated by the European Academy of Dermatology and Venereology (EADV). J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1251–1277. [Google Scholar] [CrossRef] [PubMed]
- Bottaro, G.; Cataldo, F.; Rotolo, N.; Spina, M.; Corazza, G.R. The clinical pattern of subclinical/silent celiac disease: An analysis on 1026 consecutive cases. Am. J. Gastroenterol. 1999, 94, 691–696. [Google Scholar] [CrossRef]
- Collin, P.; Huhtala, H.; Virta, L.; Kekkonen, L.; Reunala, T. Diagnosis of celiac disease in clinical practice: Physician’s alertness to the condition essential. J. Clin. Gastroenterol. 2007, 41, 152–156. [Google Scholar] [CrossRef]
- Popp, A.; Maki, M. Changing Pattern of Childhood Celiac Disease Epidemiology: Contributing Factors. Front. Pediatr. 2019, 7, 357. [Google Scholar] [CrossRef]
- Virta, L.J.; Saarinen, M.M.; Kolho, K.L. Declining trend in the incidence of biopsy-verified coeliac disease in the adult population of Finland, 2005–2014. Aliment. Pharmacol. Ther. 2017, 46, 1085–1093. [Google Scholar] [CrossRef]
- Ungprasert, P.; Wijarnpreecha, K.; Kittanamongkolchai, W. Psoriasis and Risk of Celiac Disease: A Systematic Review and Meta-analysis. Indian J. Dermatol. 2017, 62, 41–46. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Lindelof, B.; Rashtak, S.; Rubio-Tapia, A.; Murray, J.A. Does urticaria risk increase in patients with celiac disease? A large population-based cohort study. Eur. J. Dermatol. 2013, 23, 681–687. [Google Scholar] [CrossRef]
- Rodrigo, L.; Beteta-Gorriti, V.; Alvarez, N.; Gomez de Castro, C.; de Dios, A.; Palacios, L.; Santos-Juanes, J. Cutaneous and Mucosal Manifestations Associated with Celiac Disease. Nutrients 2018, 10, 800. [Google Scholar] [CrossRef]
- Persechino, F.; Galli, G.; Persechino, S.; Valitutti, F.; Zenzeri, L.; Mauro, A.; Corleto, V.D.; Parisi, P.; Ziparo, C.; Evangelisti, M.; et al. Skin Manifestations and Coeliac Disease in Paediatric Population. Nutrients 2021, 13, 3611. [Google Scholar] [CrossRef]
- Molteni, N.; Bardella, M.T.; Bianchi, P.A. Obstetric and gynecological problems in women with untreated celiac sprue. J. Clin. Gastroenterol. 1990, 12, 37–39. [Google Scholar] [CrossRef] [PubMed]
- Saccone, G.; Berghella, V.; Sarno, L.; Maruotti, G.M.; Cetin, I.; Greco, L.; Khashan, A.S.; McCarthy, F.; Martinelli, D.; Fortunato, F.; et al. Celiac disease and obstetric complications: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2016, 214, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Laurikka, P.; Nurminen, S.; Kivela, L.; Kurppa, K. Extraintestinal Manifestations of Celiac Disease: Early Detection for Better Long-Term Outcomes. Nutrients 2018, 10, 1015. [Google Scholar] [CrossRef] [PubMed]
- Moleski, S.M.; Lindenmeyer, C.C.; Veloski, J.J.; Miller, R.S.; Miller, C.L.; Kastenberg, D.; DiMarino, A.J. Increased rates of pregnancy complications in women with celiac disease. Ann. Gastroenterol. 2015, 28, 236–240. [Google Scholar]
- Tersigni, C.; Castellani, R.; de Waure, C.; Fattorossi, A.; De Spirito, M.; Gasbarrini, A.; Scambia, G.; Di Simone, N. Celiac disease and reproductive disorders: Meta-analysis of epidemiologic associations and potential pathogenic mechanisms. Hum. Reprod. Update 2014, 20, 582–593. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Montgomery, S.M.; Ekbom, A. Celiac disease and risk of adverse fetal outcome: A population-based cohort study. Gastroenterology 2005, 129, 454–463. [Google Scholar] [CrossRef]
- Sethi, G.R.; Singhal, K.K.; Puri, A.S.; Mantan, M. Benefit of gluten-free diet in idiopathic pulmonary hemosiderosis in association with celiac disease. Pediatr. Pulmonol. 2011, 46, 302–305. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; James, S.; Askling, J.; Stenestrand, U.; Ingelsson, E. Nationwide cohort study of risk of ischemic heart disease in patients with celiac disease. Circulation 2011, 123, 483–490. [Google Scholar] [CrossRef]
- Emilsson, L.; Smith, J.G.; West, J.; Melander, O.; Ludvigsson, J.F. Increased risk of atrial fibrillation in patients with coeliac disease: A nationwide cohort study. Eur. Heart J. 2011, 32, 2430–2437. [Google Scholar] [CrossRef]
- Emilsson, L.; Andersson, B.; Elfstrom, P.; Green, P.H.; Ludvigsson, J.F. Risk of idiopathic dilated cardiomyopathy in 29,000 patients with celiac disease. J. Am. Heart Assoc. 2012, 1, e001594. [Google Scholar] [CrossRef]
- Mollazadegan, K.; Kugelberg, M.; Lindblad, B.E.; Ludvigsson, J.F. Increased risk of cataract among 28,000 patients with celiac disease. Am. J. Epidemiol. 2011, 174, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Mollazadegan, K.; Kugelberg, M.; Tallstedt, L.; Ludvigsson, J.F. Increased risk of uveitis in coeliac disease: A nationwide cohort study. Br. J. Ophthalmol. 2012, 96, 857–861. [Google Scholar] [CrossRef] [PubMed]
- Volta, U.; Tovoli, F.; Caio, G. Clinical and immunological features of celiac disease in patients with Type 1 diabetes mellitus. Expert Rev. Gastroenterol. Hepatol. 2011, 5, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Volta, U.; Caio, G.; Stanghellini, V.; De Giorgio, R. The changing clinical profile of celiac disease: A 15-year experience (1998–2012) in an Italian referral center. BMC Gastroenterol. 2014, 14, 194. [Google Scholar] [CrossRef]
- O’Leary, C.; Walsh, C.H.; Wieneke, P.; O’Regan, P.; Buckley, B.; O’Halloran, D.J.; Ferriss, J.B.; Quigley, E.M.; Annis, P.; Shanahan, F.; et al. Coeliac disease and autoimmune Addison’s disease: A clinical pitfall. QJM 2002, 95, 79–82. [Google Scholar] [CrossRef]
- Volta, U.; De Franceschi, L.; Molinaro, N.; Cassani, F.; Muratori, L.; Lenzi, M.; Bianchi, F.B.; Czaja, A.J. Frequency and significance of anti-gliadin and anti-endomysial antibodies in autoimmune hepatitis. Dig. Dis. Sci. 1998, 43, 2190–2195. [Google Scholar] [CrossRef]
- Panetta, F.; Nobili, V.; Sartorelli, M.R.; Papa, R.E.; Ferretti, F.; Alterio, A.; Diamanti, A. Celiac disease in pediatric patients with autoimmune hepatitis: Etiology, diagnosis, and management. Paediatr. Drugs 2012, 14, 35–41. [Google Scholar] [CrossRef]
- Odineal, D.D.; Gershwin, M.E. The Epidemiology and Clinical Manifestations of Autoimmunity in Selective IgA Deficiency. Clin. Rev. Allergy Immunol. 2020, 58, 107–133. [Google Scholar] [CrossRef]
- Haggard, L.; Glimberg, I.; Lebwohl, B.; Sharma, R.; Verna, E.C.; Green, P.H.R.; Ludvigsson, J.F. High prevalence of celiac disease in autoimmune hepatitis: Systematic review and meta-analysis. Liver Int. 2021, 41, 2693–2702. [Google Scholar] [CrossRef]
- Villavicencio Kim, J.; Wu, G.Y. Celiac Disease and Elevated Liver Enzymes: A Review. J. Clin. Transl. Hepatol. 2021, 9, 116–124. [Google Scholar] [CrossRef]
- Volta, U.; Rodrigo, L.; Granito, A.; Petrolini, N.; Muratori, P.; Muratori, L.; Linares, A.; Veronesi, L.; Fuentes, D.; Zauli, D.; et al. Celiac disease in autoimmune cholestatic liver disorders. Am. J. Gastroenterol. 2002, 97, 2609–2613. [Google Scholar] [CrossRef] [PubMed]
- Gale, L.; Wimalaratna, H.; Brotodiharjo, A.; Duggan, J.M. Down’s syndrome is strongly associated with coeliac disease. Gut 1997, 40, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Pavlovic, M.; Berenji, K.; Bukurov, M. Screening of celiac disease in Down syndrome—Old and new dilemmas. World J. Clin. Cases 2017, 5, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Ostermaier, K.K.; Weaver, A.L.; Myers, S.M.; Stoeckel, R.E.; Katusic, S.K.; Voigt, R.G. Incidence of Celiac Disease in Down Syndrome: A Longitudinal, Population-Based Birth Cohort Study. Clin. Pediatr. 2020, 59, 1086–1091. [Google Scholar] [CrossRef] [PubMed]
- Bonamico, M.; Pasquino, A.M.; Mariani, P.; Danesi, H.M.; Culasso, F.; Mazzanti, L.; Petri, A.; Bona, G.; Italian Society of Pediatric Gastroenterology and Hepatology (SIGEP); Italian Study Group for Turner Syndrome (ISGTS). Prevalence and clinical picture of celiac disease in Turner syndrome. J. Clin. Endocrinol. Metab. 2002, 87, 5495–5498. [Google Scholar] [CrossRef]
- Giannotti, A.; Tiberio, G.; Castro, M.; Virgilii, F.; Colistro, F.; Ferretti, F.; Digilio, M.C.; Gambarara, M.; Dallapiccola, B. Coeliac disease in Williams syndrome. J. Med. Genet. 2001, 38, 767–768. [Google Scholar] [CrossRef] [PubMed]
- Nikpour, S. Neurological manifestations, diagnosis, and treatment of celiac disease: A comprehensive review. Iran. J. Neurol. 2012, 11, 59–64. [Google Scholar]
- Collin, P.; Salmi, T.T.; Hervonen, K.; Kaukinen, K.; Reunala, T. Dermatitis herpetiformis: A cutaneous manifestation of coeliac disease. Ann. Med. 2017, 49, 23–31. [Google Scholar] [CrossRef]
- Leeds, J.S.; Hopper, A.D.; Hurlstone, D.P.; Edwards, S.J.; McAlindon, M.E.; Lobo, A.J.; Donnelly, M.T.; Morley, S.; Sanders, D.S. Is exocrine pancreatic insufficiency in adult coeliac disease a cause of persisting symptoms? Aliment. Pharmacol. Ther. 2007, 25, 265–271. [Google Scholar] [CrossRef]
- Metso, S.; Hyytia-Ilmonen, H.; Kaukinen, K.; Huhtala, H.; Jaatinen, P.; Salmi, J.; Taurio, J.; Collin, P. Gluten-free diet and autoimmune thyroiditis in patients with celiac disease. A prospective controlled study. Scand. J. Gastroenterol. 2012, 47, 43–48. [Google Scholar] [CrossRef]
- Duggan, J.M.; Duggan, A.E. Systematic review: The liver in coeliac disease. Aliment. Pharmacol. Ther. 2005, 21, 515–518. [Google Scholar] [CrossRef] [PubMed]
- Emilsson, L.; Carlsson, R.; Holmqvist, M.; James, S.; Ludvigsson, J.F. The characterisation and risk factors of ischaemic heart disease in patients with coeliac disease. Aliment. Pharmacol. Ther. 2013, 37, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, M.L.; Bardella, M.T. Bone in celiac disease. Osteoporos. Int. 2008, 19, 1705–1716. [Google Scholar] [CrossRef] [PubMed]
- Alaedini, A.; Green, P.H. Narrative review: Celiac disease: Understanding a complex autoimmune disorder. Ann. Intern. Med. 2005, 142, 289–298. [Google Scholar] [CrossRef]
- Wills, A.J. The neurology and neuropathology of coeliac disease. Neuropathol. Appl. Neurobiol. 2000, 26, 493–496. [Google Scholar] [CrossRef]
- Mearns, E.S.; Taylor, A.; Thomas Craig, K.J.; Puglielli, S.; Leffler, D.A.; Sanders, D.S.; Lebwohl, B.; Hadjivassiliou, M. Neurological Manifestations of Neuropathy and Ataxia in Celiac Disease: A Systematic Review. Nutrients 2019, 11, 380. [Google Scholar] [CrossRef]
- Mitoma, H.; Manto, M.; Hampe, C.S. Immune-mediated Cerebellar Ataxias: Practical Guidelines and Therapeutic Challenges. Curr. Neuropharmacol. 2019, 17, 33–58. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Grunewald, R.A.; Sanders, D.S.; Shanmugarajah, P.; Hoggard, N. Effect of gluten-free diet on cerebellar MR spectroscopy in gluten ataxia. Neurology 2017, 89, 705–709. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Grunewald, R.A.; Chattopadhyay, A.K.; Davies-Jones, G.A.; Gibson, A.; Jarratt, J.A.; Kandler, R.H.; Lobo, A.; Powell, T.; Smith, C.M. Clinical, radiological, neurophysiological, and neuropathological characteristics of gluten ataxia. Lancet 1998, 352, 1582–1585. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Sanders, D.D.; Aeschlimann, D.P. Gluten-related disorders: Gluten ataxia. Dig. Dis. 2015, 33, 264–268. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Grunewald, R.; Sharrack, B.; Sanders, D.; Lobo, A.; Williamson, C.; Woodroofe, N.; Wood, N.; Davies-Jones, A. Gluten ataxia in perspective: Epidemiology, genetic susceptibility and clinical characteristics. Brain 2003, 126, 685–691. [Google Scholar] [CrossRef]
- Thomas, H.; Beck, K.; Adamczyk, M.; Aeschlimann, P.; Langley, M.; Oita, R.C.; Thiebach, L.; Hils, M.; Aeschlimann, D. Transglutaminase 6: A protein associated with central nervous system development and motor function. Amino Acids 2013, 44, 161–177. [Google Scholar] [CrossRef]
- Cervio, E.; Volta, U.; Verri, M.; Boschi, F.; Pastoris, O.; Granito, A.; Barbara, G.; Parisi, C.; Felicani, C.; Tonini, M.; et al. Sera of patients with celiac disease and neurologic disorders evoke a mitochondrial-dependent apoptosis in vitro. Gastroenterology 2007, 133, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Hadjivassiliou, M. Advances in Therapies of Cerebellar Disorders: Immune-mediated Ataxias. CNS Neurol. Disord. Drug Targets 2019, 18, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Hadjivassiliou, M.; Davies-Jones, G.A.; Sanders, D.S.; Grunewald, R.A. Dietary treatment of gluten ataxia. J. Neurol. Neurosurg. Psychiatry 2003, 74, 1221–1224. [Google Scholar] [CrossRef]
- Chapman, R.W.; Laidlow, J.M.; Colin-Jones, D.; Eade, O.E.; Smith, C.L. Increased prevalence of epilepsy in coeliac disease. Br. Med. J. 1978, 2, 250–251. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Zingone, F.; Tomson, T.; Ekbom, A.; Ciacci, C. Increased risk of epilepsy in biopsy-verified celiac disease: A population-based cohort study. Neurology 2012, 78, 1401–1407. [Google Scholar] [CrossRef]
- Casciato, S.; Morano, A.; Albini, M.; Fanella, M.; Lapenta, L.; Fattouch, J.; Carni, M.; Colonnese, C.; Manfredi, M.; Giallonardo, A.T.; et al. Cryptogenic focal epilepsy and “hidden” celiac disease in adulthood: A causal or accidental link? Int. J. Neurosci. 2015, 125, 913–917. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.M.; Dale, R.C.; Wienholt, L.; Hadjivassiliou, M.; Aeschlimann, D.; Lawson, J.A. Coeliac disease, epilepsy, and cerebral calcifications: Association with TG6 autoantibodies. Dev. Med. Child Neurol. 2013, 55, 90–93. [Google Scholar] [CrossRef]
- Lea, M.E.; Harbord, M.; Sage, M.R. Bilateral occipital calcification associated with celiac disease, folate deficiency, and epilepsy. AJNR Am. J. Neuroradiol. 1995, 16, 1498–1500. [Google Scholar]
- Dimitrova, A.K.; Ungaro, R.C.; Lebwohl, B.; Lewis, S.K.; Tennyson, C.A.; Green, M.W.; Babyatsky, M.W.; Green, P.H. Prevalence of migraine in patients with celiac disease and inflammatory bowel disease. Headache 2013, 53, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Zis, P.; Julian, T.; Hadjivassiliou, M. Headache Associated with Coeliac Disease: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 1445. [Google Scholar] [CrossRef] [PubMed]
- Fanaeian, M.M.; Alibeik, N.; Ganji, A.; Fakheri, H.; Ekhlasi, G.; Shahbazkhani, B. Prevalence of migraine in adults with celiac disease: A case control cross-sectional study. PLoS ONE 2021, 16, e0259502. [Google Scholar] [CrossRef] [PubMed]
- Ameghino, L.; Farez, M.F.; Wilken, M.; Goicochea, M.T. Headache in Patients with Celiac Disease and Its Response to the Gluten-Free Diet. J. Oral Facial Pain Headache 2019, 33, 294–300. [Google Scholar] [CrossRef]
- Addolorato, G.; Capristo, E.; Ghittoni, G.; Valeri, C.; Masciana, R.; Ancona, C.; Gasbarrini, G. Anxiety but not depression decreases in coeliac patients after one-year gluten-free diet: A longitudinal study. Scand. J. Gastroenterol. 2001, 36, 502–506. [Google Scholar] [CrossRef]
- Kemper, R.H.; Meijler, W.J.; Korf, J.; Ter Horst, G.J. Migraine and function of the immune system: A meta-analysis of clinical literature published between 1966 and 1999. Cephalalgia 2001, 21, 549–557. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Croall, I.D.; Grunewald, R.A.; Trott, N.; Sanders, D.S.; Hoggard, N. Neurological Evaluation of Patients with Newly Diagnosed Coeliac Disease Presenting to Gastroenterologists: A 7-Year Follow-Up Study. Nutrients 2021, 13, 1846. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Sanders, D.S.; Grunewald, R.A.; Woodroofe, N.; Boscolo, S.; Aeschlimann, D. Gluten sensitivity: From gut to brain. Lancet Neurol. 2010, 9, 318–330. [Google Scholar] [CrossRef]
- Shen, T.C.; Lebwohl, B.; Verma, H.; Kumta, N.; Tennyson, C.; Lewis, S.; Scherl, E.; Swaminath, A.; Capiak, K.M.; DiGiacomo, D.; et al. Peripheral neuropathic symptoms in celiac disease and inflammatory bowel disease. J. Clin. Neuromuscul. Dis. 2012, 13, 137–145. [Google Scholar] [CrossRef]
- Mukherjee, R.; Egbuna, I.; Brar, P.; Hernandez, L.; McMahon, D.J.; Shane, E.J.; Bhagat, G.; Green, P.H. Celiac disease: Similar presentations in the elderly and young adults. Dig. Dis. Sci. 2010, 55, 3147–3153. [Google Scholar] [CrossRef]
- Thawani, S.P.; Brannagan, T.H., 3rd; Lebwohl, B.; Green, P.H.; Ludvigsson, J.F. Risk of Neuropathy Among 28,232 Patients With Biopsy-Verified Celiac Disease. JAMA Neurol. 2015, 72, 806–811. [Google Scholar] [CrossRef] [PubMed]
- Jericho, H.; Sansotta, N.; Guandalini, S. Extraintestinal Manifestations of Celiac Disease: Effectiveness of the Gluten-Free Diet. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Makhlouf, S.; Messelmani, M.; Zaouali, J.; Mrissa, R. Cognitive impairment in celiac disease and non-celiac gluten sensitivity: Review of literature on the main cognitive impairments, the imaging and the effect of gluten free diet. Acta Neurol. Belg. 2018, 118, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.T.; Murray, J.A.; Greenaway, M.C.; Parisi, J.E.; Josephs, K.A. Cognitive impairment and celiac disease. Arch. Neurol. 2006, 63, 1440–1446. [Google Scholar] [CrossRef]
- Longarini, G.; Richly, P.; Temprano, M.P.; Costa, A.F.; Vazquez, H.; Moreno, M.L.; Niveloni, S.; Lopez, P.; Smecuol, E.; Mazure, R.; et al. A Prospective Study on Cognitive Impairment in Middle-aged Adults With Newly Diagnosed Celiac Disease. J. Clin. Gastroenterol. 2019, 53, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Collin, P.; Pirttila, T.; Nurmikko, T.; Somer, H.; Erila, T.; Keyrilainen, O. Celiac disease, brain atrophy, and dementia. Neurology 1991, 41, 372–375. [Google Scholar] [CrossRef] [PubMed]
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac disease: A comprehensive current review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef] [PubMed]
- Bascunan, K.A.; Vespa, M.C.; Araya, M. Celiac disease: Understanding the gluten-free diet. Eur. J. Nutr. 2017, 56, 449–459. [Google Scholar] [CrossRef]
- Welstead, L. The Gluten-Free Diet in the 3rd Millennium: Rules, Risks and Opportunities. Diseases 2015, 3, 136–149. [Google Scholar] [CrossRef]
- Zarkadas, M.; Cranney, A.; Case, S.; Molloy, M.; Switzer, C.; Graham, I.D.; Butzner, J.D.; Rashid, M.; Warren, R.E.; Burrows, V. The impact of a gluten-free diet on adults with coeliac disease: Results of a national survey. J. Hum. Nutr. Diet. 2006, 19, 41–49. [Google Scholar] [CrossRef]
- Osorio, C.E.; Mejías, J.H.; Rustgi, S. Gluten Detection Methods and Their Critical Role in Assuring Safe Diets for Celiac Patients. Nutrients 2019, 11, 2920. [Google Scholar] [CrossRef]
- Cohen, I.S.; Day, A.S.; Shaoul, R. Gluten in Celiac Disease-More or Less? Rambam Maimonides Med. J. 2019, 10, e0007. [Google Scholar] [CrossRef]
- Vaquero, L.; Bernardo, D.; Leon, F.; Rodriguez-Martin, L.; Alvarez-Cuenllas, B.; Vivas, S. Challenges to drug discovery for celiac disease and approaches to overcome them. Expert Opin. Drug Discov. 2019, 14, 957–968. [Google Scholar] [CrossRef] [PubMed]
- Valitutti, F.; Trovato, C.M.; Montuori, M.; Cucchiara, S. Pediatric Celiac Disease: Follow-Up in the Spotlight. Adv. Nutr. 2017, 8, 356–361. [Google Scholar] [CrossRef]
- Hoilat, G.J.; Altowairqi, A.K.; Ayas, M.F.; Alhaddab, N.T.; Alnujaidi, R.A.; Alharbi, H.A.; Alyahyawi, N.; Kamal, A.; Alhabeeb, H.; Albazee, E.; et al. Larazotide acetate for treatment of celiac disease: A systematic review and meta-analysis of randomized controlled trials. Clin. Res. Hepatol. Gastroenterol. 2021, 46, 101782. [Google Scholar] [CrossRef]
- Lahdeaho, M.L.; Kaukinen, K.; Laurila, K.; Vuotikka, P.; Koivurova, O.P.; Karja-Lahdensuu, T.; Marcantonio, A.; Adelman, D.C.; Maki, M. Glutenase ALV003 attenuates gluten-induced mucosal injury in patients with celiac disease. Gastroenterology 2014, 146, 1649–1658. [Google Scholar] [CrossRef] [PubMed]
- Schuppan, D.; Maki, M.; Lundin, K.E.A.; Isola, J.; Friesing-Sosnik, T.; Taavela, J.; Popp, A.; Koskenpato, J.; Langhorst, J.; Hovde, O.; et al. A Randomized Trial of a Transglutaminase 2 Inhibitor for Celiac Disease. N. Engl. J. Med. 2021, 385, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Daveson, A.J.M.; Ee, H.C.; Andrews, J.M.; King, T.; Goldstein, K.E.; Dzuris, J.L.; MacDougall, J.A.; Williams, L.J.; Treohan, A.; Cooreman, M.P.; et al. Epitope-Specific Immunotherapy Targeting CD4-Positive T Cells in Celiac Disease: Safety, Pharmacokinetics, and Effects on Intestinal Histology and Plasma Cytokines with Escalating Dose Regimens of Nexvax2 in a Randomized, Double-Blind, Placebo-Controlled Phase 1 Study. EBioMedicine 2017, 26, 78–90. [Google Scholar] [CrossRef]
- Khaleghi, S.; Ju, J.M.; Lamba, A.; Murray, J.A. The potential utility of tight junction regulation in celiac disease: Focus on larazotide acetate. Ther. Adv. Gastroenterol. 2016, 9, 37–49. [Google Scholar] [CrossRef]
- Slifer, Z.M.; Krishnan, B.R.; Madan, J.; Blikslager, A.T. Larazotide acetate: A pharmacological peptide approach to tight junction regulation. Am. J. Physiol. Gastrointest. Liver Physiol. 2021, 320, G983–G989. [Google Scholar] [CrossRef]
- Paterson, B.M.; Lammers, K.M.; Arrieta, M.C.; Fasano, A.; Meddings, J.B. The safety, tolerance, pharmacokinetic and pharmacodynamic effects of single doses of AT-1001 in coeliac disease subjects: A proof of concept study. Aliment. Pharmacol. Ther. 2007, 26, 757–766. [Google Scholar] [CrossRef]
- Leffler, D.A.; Kelly, C.P.; Abdallah, H.Z.; Colatrella, A.M.; Harris, L.A.; Leon, F.; Arterburn, L.A.; Paterson, B.M.; Lan, Z.H.; Murray, J.A. A randomized, double-blind study of larazotide acetate to prevent the activation of celiac disease during gluten challenge. Am. J. Gastroenterol. 2012, 107, 1554–1562. [Google Scholar] [CrossRef] [PubMed]
- Leffler, D.A.; Kelly, C.P.; Green, P.H.; Fedorak, R.N.; DiMarino, A.; Perrow, W.; Rasmussen, H.; Wang, C.; Bercik, P.; Bachir, N.M.; et al. Larazotide acetate for persistent symptoms of celiac disease despite a gluten-free diet: A randomized controlled trial. Gastroenterology 2015, 148, 1311–1319.e6. [Google Scholar] [CrossRef]
- Kelly, C.P.; Green, P.H.; Murray, J.A.; Dimarino, A.; Colatrella, A.; Leffler, D.A.; Alexander, T.; Arsenescu, R.; Leon, F.; Jiang, J.G.; et al. Larazotide acetate in patients with coeliac disease undergoing a gluten challenge: A randomised placebo-controlled study. Aliment. Pharmacol. Ther. 2013, 37, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Stern, M.; Ciclitira, P.J.; van Eckert, R.; Feighery, C.; Janssen, F.W.; Mendez, E.; Mothes, T.; Troncone, R.; Wieser, H. Analysis and clinical effects of gluten in coeliac disease. Eur. J. Gastroenterol. Hepatol. 2001, 13, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Wei, G.; Helmerhorst, E.J.; Darwish, G.; Blumenkranz, G.; Schuppan, D. Gluten Degrading Enzymes for Treatment of Celiac Disease. Nutrients 2020, 12, 2095. [Google Scholar] [CrossRef] [PubMed]
- Bethune, M.T.; Khosla, C. Oral enzyme therapy for celiac sprue. Methods Enzymol. 2012, 502, 241–271. [Google Scholar] [CrossRef] [PubMed]
- Gass, J.; Bethune, M.T.; Siegel, M.; Spencer, A.; Khosla, C. Combination enzyme therapy for gastric digestion of dietary gluten in patients with celiac sprue. Gastroenterology 2007, 133, 472–480. [Google Scholar] [CrossRef]
- Murray, J.A.; Kelly, C.P.; Green, P.H.R.; Marcantonio, A.; Wu, T.T.; Maki, M.; Adelman, D.C.; CeliAction Study Group of Investigators. No Difference Between Latiglutenase and Placebo in Reducing Villous Atrophy or Improving Symptoms in Patients With Symptomatic Celiac Disease. Gastroenterology 2017, 152, 787–798.e2. [Google Scholar] [CrossRef]
- Syage, J.A.; Murray, J.A.; Green, P.H.R.; Khosla, C. Latiglutenase Improves Symptoms in Seropositive Celiac Disease Patients While on a Gluten-Free Diet. Dig. Dis. Sci. 2017, 62, 2428–2432. [Google Scholar] [CrossRef]
- Wolf, C.; Siegel, J.B.; Tinberg, C.; Camarca, A.; Gianfrani, C.; Paski, S.; Guan, R.; Montelione, G.; Baker, D.; Pultz, I.S. Engineering of Kuma030: A Gliadin Peptidase That Rapidly Degrades Immunogenic Gliadin Peptides in Gastric Conditions. J. Am. Chem. Soc. 2015, 137, 13106–13113. [Google Scholar] [CrossRef] [PubMed]
- Molberg, Ø.; McAdam, S.; Lundin, K.E.A.; Kristiansen, C.; Arentz-Hansen, H.; Kett, K.; Sollid, L.M. T cells from celiac disease lesions recognize gliadin epitopes deamidated in situ by endogenous tissue transglutaminase. Eur. J. Immunol. 2001, 31, 1317–1323. [Google Scholar] [CrossRef]
- Hsu, T.C.; Huang, C.Y.; Chiang, S.Y.; Lai, W.X.; Tsai, C.H.; Tzang, B.S. Transglutaminase inhibitor cystamine alleviates the abnormality in liver from NZB/W F1 mice. Eur. J. Pharmacol. 2008, 579, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Jeitner, T.M.; Pinto, J.T.; Cooper, A.J.L. Cystamine and cysteamine as inhibitors of transglutaminase activity in vivo. Biosci. Rep. 2018, 38, BSR20180691. [Google Scholar] [CrossRef]
- Stamnaes, J.; Pinkas, D.M.; Fleckenstein, B.; Khosla, C.; Sollid, L.M. Redox regulation of transglutaminase 2 activity. J. Biol. Chem. 2010, 285, 25402–25409. [Google Scholar] [CrossRef]
- Badarau, E.; Collighan, R.J.; Griffin, M. Recent advances in the development of tissue transglutaminase (TG2) inhibitors. Amino Acids 2013, 44, 119–127. [Google Scholar] [CrossRef]
- Di Sabatino, A.; Lenti, M.V.; Corazza, G.R.; Gianfrani, C. Vaccine Immunotherapy for Celiac Disease. Front. Med. 2018, 5, 187. [Google Scholar] [CrossRef]
- Liang, L.; Pinier, M.; Leroux, J.C.; Subirade, M. Interaction of alpha-gliadin with polyanions: Design considerations for sequestrants used in supportive treatment of celiac disease. Biopolymers 2010, 93, 418–428. [Google Scholar] [CrossRef]
- Perlman, S.L. Update on the Treatment of Ataxia: Medication and Emerging Therapies. Neurotherapeutics 2020, 17, 1660–1664. [Google Scholar] [CrossRef]
- Liu, J.; Wang, L.N. The efficacy and safety of riluzole for neurodegenerative movement disorders: A systematic review with meta-analysis. Drug Deliv. 2018, 25, 43–48. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gala, D.; Scharf, S.; Kudlak, M.; Green, C.; Khowaja, F.; Shah, M.; Kumar, V.; Ullal, G. A Comprehensive Review of the Neurological Manifestations of Celiac Disease and Its Treatment. Diseases 2022, 10, 111. https://doi.org/10.3390/diseases10040111
Gala D, Scharf S, Kudlak M, Green C, Khowaja F, Shah M, Kumar V, Ullal G. A Comprehensive Review of the Neurological Manifestations of Celiac Disease and Its Treatment. Diseases. 2022; 10(4):111. https://doi.org/10.3390/diseases10040111
Chicago/Turabian StyleGala, Dhir, Shelbie Scharf, Megan Kudlak, Christian Green, Faisal Khowaja, Mili Shah, Vikash Kumar, and Gautam Ullal. 2022. "A Comprehensive Review of the Neurological Manifestations of Celiac Disease and Its Treatment" Diseases 10, no. 4: 111. https://doi.org/10.3390/diseases10040111
APA StyleGala, D., Scharf, S., Kudlak, M., Green, C., Khowaja, F., Shah, M., Kumar, V., & Ullal, G. (2022). A Comprehensive Review of the Neurological Manifestations of Celiac Disease and Its Treatment. Diseases, 10(4), 111. https://doi.org/10.3390/diseases10040111