
Life-Threatening Ventricular Arrhythmia Identification Based on Multiple Complex Networks


Abstract
1. Introduction
2. Materials and Methods
2.1. Database and Preprocessing
2.1.1. Benchmark Datasets
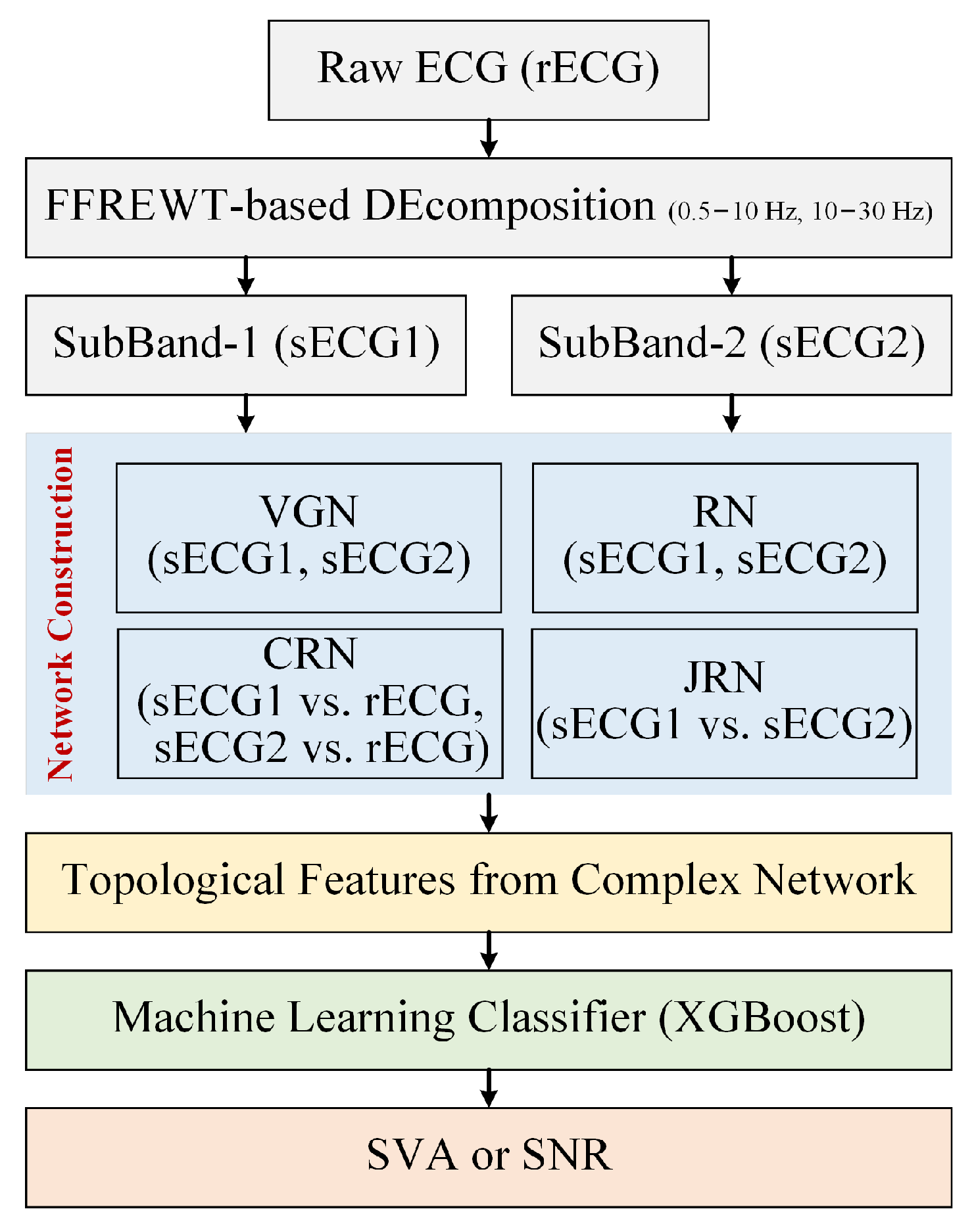
2.1.2. Signal Processing
2.2. Complex Network Construction
2.2.1. Weighted Multi-Scale Visibility Graph
2.2.2. Recurrence Network
2.2.3. Cross-Recurrence Network
2.2.4. Joint Recurrence Network
2.3. Topological Feature Extraction from Complex Network
2.4. Machine Learning Classifier and Evaluation Metrics
3. Results
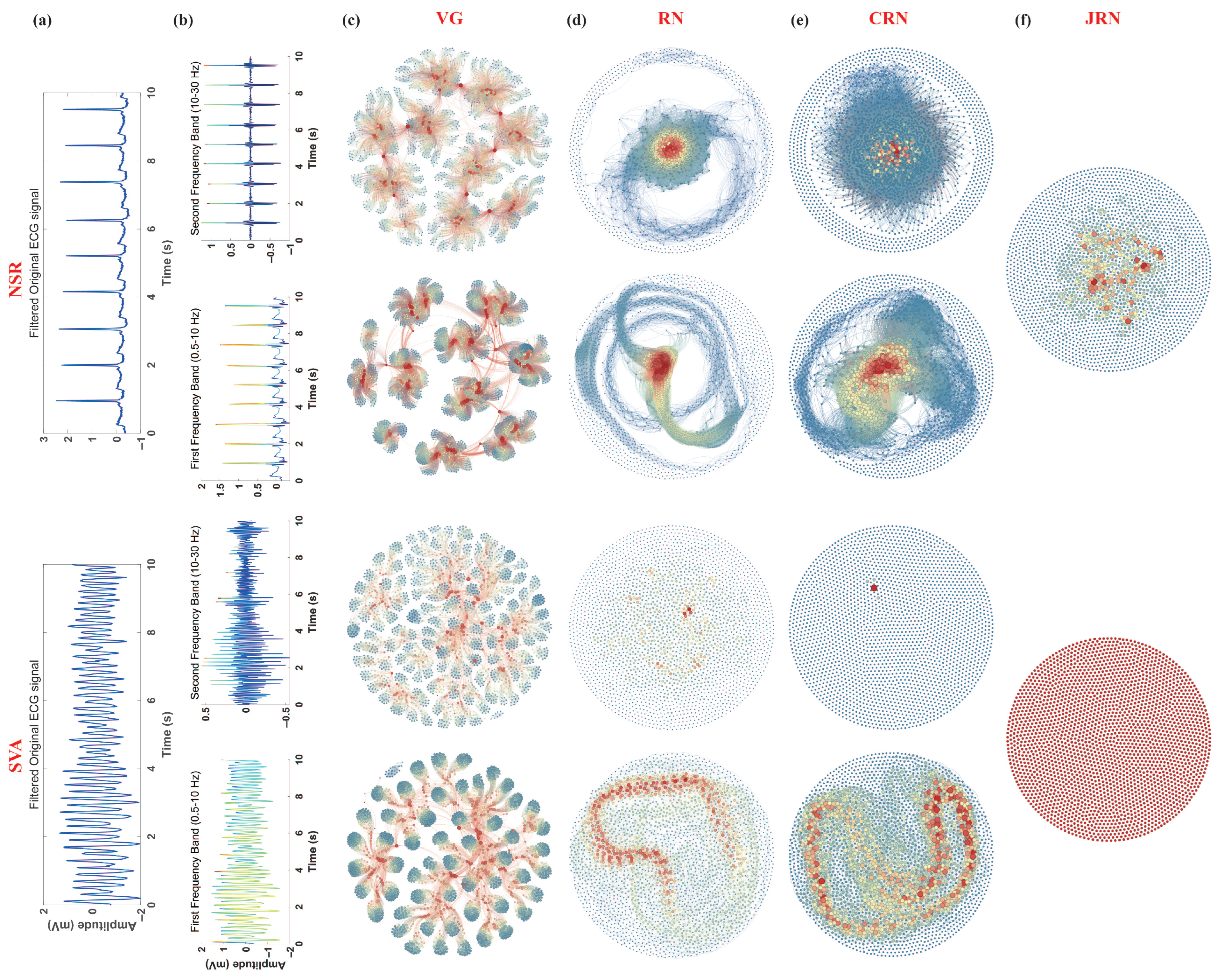
3.1. Complex Network Comparison for SVA/NSR Segments
3.1.1. VGN
3.1.2. RN
3.1.3. CRN
3.1.4. JRN
3.2. Investigation of Frequency Band Significance
3.3. Ablation Experiment for Complex Network Importance Evaluation
3.4. Performance of the Proposed Method on Short-Term ECG
3.5. Mobile Deployment of the Proposed Model
4. Discussion
4.1. Comparison with Existing Methods
4.2. Influence of Frequency Band Characteristics on Detection Performance
4.3. Effect of ECG Segment Length on Detection Accuracy
4.4. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marijon, E.; Narayanan, K.; Smith, K.; Barra, S.; Basso, C.; Blom, M.T.; Crotti, L.; D’Avila, A.; Deo, R.; Dumas, F.; et al. The Lancet Commission to Reduce the Global Burden of Sudden Cardiac Death: A Call for Multidisciplinary Action. Lancet 2023, 402, 883–936. [Google Scholar] [CrossRef]
- Deyell, M.W.; Krahn, A.D.; Goldberger, J.J. Sudden Cardiac Death Risk Stratification. Circ. Res. 2015, 116, 1907–1918. [Google Scholar] [CrossRef]
- Trancuccio, A.; Kukavica, D.; Sugamiele, A.; Mazzanti, A.; Priori, S.G. Prevention of Sudden Death and Management of Ventricular Arrhythmias in Arrhythmogenic Cardiomyopathy. Card. Electrophysiol. Clin. 2023, 15, 349–365. [Google Scholar] [CrossRef] [PubMed]
- Hammad, M.; Iliyasu, A.M.; Subasi, A.; Ho, E.S.L.; El-Latif, A.A.A. A Multitier Deep Learning Model for Arrhythmia Detection. IEEE Trans. Instrum. Meas. 2021, 70, 1–9. [Google Scholar] [CrossRef]
- Kolk, M.Z.H.; Frodi, D.M.; Langford, J.; Jacobsen, P.K.; Risum, N.; Andersen, T.O.; Tan, H.L.; Hastrup Svendsen, J.; Knops, R.E.; Diederichsen, S.Z.; et al. Artificial Intelligence-Enhanced Wearable Technology Enables Ventricular Arrhythmia Prediction. Eur. Heart J.—Digit. Health 2024, ztae069. [Google Scholar] [CrossRef]
- Lee, S.; Park, D. Improved Dynamic Programming in Local Linear Approximation Based on a Template in a Lightweight ECG Signal-Processing Edge Device. J. Inf. Process. Syst. 2022, 18, 97–114. [Google Scholar] [CrossRef]
- Matsuura, N.; Kuwabara, K.; Ogasawara, T. Lightweight Heartbeat Detection Algorithm for Consumer Grade Wearable ECG Measurement Devices and Its Implementation. In Proceedings of the 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, Scotland, UK, 11–15 July 2022; pp. 4299–4302. [Google Scholar] [CrossRef]
- Shen, Q.; Li, J.; Cui, C.; Wang, X.; Gao, H.; Liu, C.; Chen, M. A Wearable Real-Time Telemonitoring Electrocardiogram Device Compared with Traditional Holter Monitoring. J. Biomed. Res. 2021, 35, 238. [Google Scholar] [CrossRef]
- Rauf, S.; Bilal, R.M.; Li, J.; Vaseem, M.; Ahmad, A.N.; Shamim, A. Fully Screen-Printed and Gentle-to-Skin Wet ECG Electrodes with Compact Wireless Readout for Cardiac Diagnosis and Remote Monitoring. ACS Nano 2024, 18, 10074–10087. [Google Scholar] [CrossRef]
- Pantelidis, P.; Dilaveris, P.; Ruipérez-Campillo, S.; Goliopoulou, A.; Giannakodimos, A.; Theofilis, P.; De Lucia, R.; Katsarou, O.; Zisimos, K.; Kalogeras, K.; et al. Hearts, Data, and Artificial Intelligence Wizardry: From Imitation to Innovation in Cardiovascular Care. Biomedicines 2025, 13, 1019. [Google Scholar] [CrossRef]
- Page, R.L.; Joglar, J.A.; Caldwell, M.A.; Calkins, H.; Conti, J.B.; Deal, B.J.; Estes, N.M.; Field, M.E.; Goldberger, Z.D.; Hammill, S.C.; et al. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia. J. Am. Coll. Cardiol. 2016, 67, e27–e115. [Google Scholar] [CrossRef]
- Aktaa, S.; Tzeis, S.; Gale, C.P.; Ackerman, M.J.; Arbelo, E.; Behr, E.R.; Crotti, L.; d’Avila, A.; De Chillou, C.; Deneke, T.; et al. European Society of Cardiology Quality Indicators for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. EP Eur. 2023, 25, 199–210. [Google Scholar] [CrossRef]
- Niu, Y.; Wang, H.; Wang, H.; Zhang, H.; Jin, Z.; Guo, Y. Diagnostic Validation of Smart Wearable Device Embedded with Single-Lead Electrocardiogram for Arrhythmia Detection. Digit. Health 2023, 9, 20552076231198682. [Google Scholar] [CrossRef]
- Kim, D.; Min, J.; Ko, S.H. Recent Developments and Future Directions of Wearable Skin Biosignal Sensors. Adv. Sens. Res. 2024, 3, 2300118. [Google Scholar] [CrossRef]
- Yu, S.; Liu, S. A Novel Adaptive Recursive Least Squares Filter to Remove the Motion Artifact in Seismocardiography. Sensors 2020, 20, 1596. [Google Scholar] [CrossRef] [PubMed]
- Volak, J.; Bajzik, J.; Janisova, S.; Koniar, D.; Hargas, L. Real-Time Interference Artifacts Suppression in Array of ToF Sensors. Sensors 2020, 20, 3701. [Google Scholar] [CrossRef] [PubMed]
- Martis, R.J.; Acharya, U.R.; Min, L.C. ECG Beat Classification Using PCA, LDA, ICA and Discrete Wavelet Transform. Biomed. Signal Process. Control 2013, 8, 437–448. [Google Scholar] [CrossRef]
- Sabut, S.; Pandey, O.; Mishra, B.S.P.; Mohanty, M. Detection of Ventricular Arrhythmia Using Hybrid Time–Frequency-Based Features and Deep Neural Network. Phys. Eng. Sci. Med. 2021, 44, 135–145. [Google Scholar] [CrossRef]
- Saini, S.K.; Gupta, R. Artificial Intelligence Methods for Analysis of Electrocardiogram Signals for Cardiac Abnormalities: State-of-the-Art and Future Challenges. Artif. Intell. Rev. 2022, 55, 1519–1565. [Google Scholar] [CrossRef]
- Jha, C.K.; Kolekar, M.H. Cardiac Arrhythmia Classification Using Tunable Q-wavelet Transform Based Features and Support Vector Machine Classifier. Biomed. Signal Process. Control 2020, 59, 101875. [Google Scholar] [CrossRef]
- Acharya, U.R.; Oh, S.L.; Hagiwara, Y.; Tan, J.H.; Adam, M.; Gertych, A.; Tan, R.S. A Deep Convolutional Neural Network Model to Classify Heartbeats. Comput. Biol. Med. 2017, 89, 389–396. [Google Scholar] [CrossRef]
- Oh, S.L.; Ng, E.Y.; Tan, R.S.; Acharya, U.R. Automated Diagnosis of Arrhythmia Using Combination of CNN and LSTM Techniques with Variable Length Heart Beats. Comput. Biol. Med. 2018, 102, 278–287. [Google Scholar] [CrossRef]
- Liu, X.; Wang, H.; Li, Z.; Qin, L. Deep Learning in ECG Diagnosis: A Review. Knowl.-Based Syst. 2021, 227, 107187. [Google Scholar] [CrossRef]
- Rudin, C. Stop Explaining Black Box Machine Learning Models for High Stakes Decisions and Use Interpretable Models Instead. Nat. Mach. Intell. 2019, 1, 206–215. [Google Scholar] [CrossRef]
- Li, X.; Yang, D.; Liu, X.; Wu, X.M. Bridging Time Series Dynamics and Complex Network Theory with Application to Electrocardiogram Analysis. IEEE Circuits Syst. Mag. 2012, 12, 33–46. [Google Scholar] [CrossRef]
- Cai, Z.; Ma, C.; Li, J.; Liu, C. Hybrid Amplitude Ordinal Partition Networks for ECG Morphology Discrimination: An Application to PVC Recognition. IEEE Trans. Instrum. Meas. 2024, 73, 1–13. [Google Scholar] [CrossRef]
- Garcia, G.; Moreira, G.; Luz, E.; Menotti, D. Improving Automatic Cardiac Arrhythmia Classification: Joining Temporal-VCG, Complex Networks and SVM Classifier. In Proceedings of the 2016 International Joint Conference on Neural Networks (IJCNN), Vancouver, BC, Canada, 24–29 July 2016; pp. 3896–3900. [Google Scholar] [CrossRef]
- Liu, H.; Meng, Q.; Zhang, Q.; Wei, Y.; Liu, M.; Zhang, H. A Novel Detection of Ventricular Tachycardia and Fibrillation Based on Degree Centrality of Complex Network. In Intelligent Computing Theories and Application; Huang, D.S., Bevilacqua, V., Premaratne, P., Gupta, P., Eds.; Springer International Publishing: Cham, Switzerland, 2017; Volume 10361, pp. 329–337. [Google Scholar] [CrossRef]
- Shen, Y.; Cai, Z.; Zhang, L.; Lin, B.S.; Li, J.; Liu, C. Efficient Premature Ventricular Contraction Detection Based on Network Dynamics Features. IEEE Trans. Instrum. Meas. 2024, 73, 1–15. [Google Scholar] [CrossRef]
- Chasman, D.; Fotuhi Siahpirani, A.; Roy, S. Network-Based Approaches for Analysis of Complex Biological Systems. Curr. Opin. Biotechnol. 2016, 39, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.P.; Warule, P.; Deb, S. Fixed Frequency Range Empirical Wavelet Transform Based Acoustic and Entropy Features for Speech Emotion Recognition. Speech Commun. 2025, 166, 103148. [Google Scholar] [CrossRef]
- Lacasa, L.; Luque, B.; Ballesteros, F.; Luque, J.; Nuño, J.C. From Time Series to Complex Networks: The Visibility Graph. Proc. Natl. Acad. Sci. USA 2008, 105, 4972–4975. [Google Scholar] [CrossRef]
- Han, X.; Cai, Z.; Gao, H.; Li, J.; Liu, C. Detection of Shockable Ventricular Arrhythmias Using Multiscale Visual Graph Network. IEEE Trans. Instrum. Meas. 2025, 74, 1–9. [Google Scholar] [CrossRef]
- Marwan, N.; Kurths, J. Nonlinear Analysis of Bivariate Data with Cross Recurrence Plots. Phys. Lett. A 2002, 302, 299–307. [Google Scholar] [CrossRef]
- León, C.; Carrault, G.; Pladys, P.; Beuchée, A. Early Detection of Late Onset Sepsis in Premature Infants Using Visibility Graph Analysis of Heart Rate Variability. IEEE J. Biomed. Health Inform. 2021, 25, 1006–1017. [Google Scholar] [CrossRef] [PubMed]
- Hou, F.Z.; Li, F.W.; Wang, J.; Yan, F.R. Visibility Graph Analysis of Very Short-Term Heart Rate Variability during Sleep. Phys. A Stat. Mech. Its Appl. 2016, 458, 140–145. [Google Scholar] [CrossRef]
- Li, L.; Alderson, D.; Doyle, J.C.; Willinger, W. Towards a Theory of Scale-Free Graphs: Definition, Properties, and Implications. Internet Math. 2005, 2, 431–523. [Google Scholar] [CrossRef]
- Balakrishnan, R. The Energy of a Graph. Linear Algebra Its Appl. 2004, 387, 287–295. [Google Scholar] [CrossRef]
- Lorenzini, L.; Ingala, S.; Collij, L.E.; Wottschel, V.; Haller, S.; Blennow, K.; Frisoni, G.; Chételat, G.; Payoux, P.; Lage-Martinez, P.; et al. Eigenvector Centrality Dynamics Are Related to Alzheimer’s Disease Pathological Changes in Non-Demented Individuals. Brain Commun. 2023, 5, fcad088. [Google Scholar] [CrossRef]
- Cheng, P.; Dong, X. Life-Threatening Ventricular Arrhythmia Detection With Personalized Features. IEEE Access 2017, 5, 14195–14203. [Google Scholar] [CrossRef]
- Nguyen, M.T.; Shahzad, A.; Nguyen, B.V.; Kim, K. Diagnosis of Shockable Rhythms for Automated External Defibrillators Using a Reliable Support Vector Machine Classifier. Biomed. Signal Process. Control 2018, 44, 258–269. [Google Scholar] [CrossRef]
- Sharma, M.; Tan, R.S.; Acharya, U.R. Detection of Shockable Ventricular Arrhythmia Using Optimal Orthogonal Wavelet Filters. Neural Comput. Appl. 2020, 32, 15869–15884. [Google Scholar] [CrossRef]
- Xu, Y.; Wang, D.; Zhang, W.; Ping, P.; Feng, L. Detection of Ventricular Tachycardia and Fibrillation Using Adaptive Variational Mode Decomposition and Boosted-CART Classifier. Biomed. Signal Process. Control 2018, 39, 219–229. [Google Scholar] [CrossRef]
- Lai, D.; Fan, X.; Zhang, Y.; Chen, W. Intelligent and Efficient Detection of Life-Threatening Ventricular Arrhythmias in Short Segments of Surface ECG Signals. IEEE Sens. J. 2021, 21, 14110–14120. [Google Scholar] [CrossRef]
- Panda, R.; Jain, S.; Tripathy, R.K.; Acharya, U.R. Detection of Shockable Ventricular Cardiac Arrhythmias from ECG Signals Using FFREWT Filter-Bank and Deep Convolutional Neural Network. Comput. Biol. Med. 2020, 124, 103939. [Google Scholar] [CrossRef]
- Acharya, U.R.; Fujita, H.; Oh, S.L.; Raghavendra, U.; Tan, J.H.; Adam, M.; Gertych, A.; Hagiwara, Y. Automated Identification of Shockable and Non-Shockable Life-Threatening Ventricular Arrhythmias Using Convolutional Neural Network. Future Gener. Comput. Syst. 2018, 79, 952–959. [Google Scholar] [CrossRef]
- Verma, A.; Dong, X. Detection of Ventricular Fibrillation Using Random Forest Classifier. J. Biomed. Sci. Eng. 2016, 9, 259. [Google Scholar] [CrossRef]
- Tripathy, R.K.; Zamora-Mendez, A.; de la O Serna, J.A.; Paternina, M.R.A.; Arrieta, J.G.; Naik, G.R. Detection of Life Threatening Ventricular Arrhythmia Using Digital Taylor Fourier Transform. Front. Physiol. 2018, 9, 722. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Type | # 10 s Segment | # 8 s Segment | # 5 s Segment | # 2 s Segment |
|---|---|---|---|---|---|
| VFDB | NSR | 3089 | 3882 | 6262 | 15,809 |
| SVA | 748 | 951 | 1556 | 4022 | |
| CUDB | NSR | 1284 | 1621 | 2642 | 6731 |
| SVA | 303 | 391 | 660 | 1747 | |
| Train set | NSR | 3935 | 4952 | 7932 | 20,286 |
| SVA | 945 | 1207 | 1994 | 5192 | |
| Test set | NSR | 438 | 551 | 882 | 2254 |
| SVA | 106 | 135 | 222 | 577 | |
| Total | NSR | 4373 | 5503 | 8814 | 22,540 |
| SVA | 1051 | 1342 | 2216 | 5769 |
| Features | Se (%) | Sp (%) | Acc (%) |
|---|---|---|---|
| VGN1 | 88.64 ± 1.44 | 88.75 ± 1.33 | 88.65 ± 0.03 |
| VGN2 | 94.87 ± 0.99 | 94.91 ± 1.40 | 94.86 ± 0.02 |
| RN1 | 97.13 ± 0.62 | 97.59 ± 0.77 | 97.38 ± 0.03 |
| RN2 | 96.29 ± 1.46 | 96.26 ± 1.65 | 96.24 ± 0.01 |
| CRN1 | 98.24 ± 1.04 | 97.30 ± 1.10 | 97.79 ± 0.01 |
| CRN2 | 92.96 ± 0.80 | 94.78 ± 0.31 | 93.92 ± 0.04 |
| Features | Se (%) | Sp (%) | Acc (%) |
|---|---|---|---|
| VGN | 97.22 ± 1.39 | 96.69 ± 1.41 | 97.00 ± 0.02 |
| RN | 98.35 ± 0.58 | 98.08 ± 0.72 | 98.26 ± 0.02 |
| CRN | 98.10 ± 0.79 | 97.62 ± 0.56 | 97.82 ± 0.02 |
| JRN | 96.65 ± 1.26 | 94.76 ± 1.42 | 95.65 ± 0.01 |
| VGN + RN | 97.95 ± 1.18 | 97.75 ± 1.10 | 97.80 ± 0.01 |
| VGN + CRN | 98.73 ± 0.71 | 97.97 ± 0.76 | 98.31 ± 0.01 |
| VGN + JRN | 97.39 ± 1.01 | 97.59 ± 0.87 | 97.55 ± 0.03 |
| RN + CRN | 98.97 ± 0.49 | 98.11 ± 0.54 | 98.59 ± 0.01 |
| RN + JRN | 98.31 ± 1.11 | 98.05 ± 1.17 | 98.11 ± 0.01 |
| CRN + JRN | 98.48 ± 0.70 | 98.18 ± 0.80 | 98.36 ± 0.02 |
| VGN + RN + CRN | 98.28 ± 0.92 | 98.56 ± 1.07 | 98.49 ± 0.01 |
| VGN + RN + JRN | 98.21 ± 0.72 | 97.01 ± 0.52 | 97.53 ± 0.02 |
| VGN + CRN + JRN | 98.17 ± 0.51 | 98.27 ± 0.38 | 98.23 ± 0.01 |
| RN + CRN + JRN | 99.03 ± 0.08 | 98.00 ± 0.09 | 98.41 ± 0.01 |
| All | 99.02 ± 0.53 | 99.17 ± 0.43 | 98.73 ± 0.02 |
| Segment Length (s) | Features | Se (%) | Sp (%) | Acc (%) | Mean Running Time (ms) | Mean Energy Consumption (mWh) |
|---|---|---|---|---|---|---|
| 10 | VGN-related | 97.22 ± 1.39 | 96.69 ± 1.41 | 97.00 ± 0.02 | 228 | 0.035 |
| RN-related | 99.03 ± 0.08 | 98.00 ± 0.09 | 98.41 ± 0.01 | 356 | 0.048 | |
| All | 99.02 ± 0.53 | 98.44 ± 0.43 | 98.73 ± 0.02 | 667 | 0.095 | |
| 8 | VGN-related | 96.74 ± 0.09 | 96.66 ± 0.09 | 96.68 ± 0.03 | 185 | 0.028 |
| RN-related | 97.49 ± 0.74 | 98.95 ± 0.63 | 98.21 ± 0.01 | 297 | 0.043 | |
| All | 98.06 ± 1.29 | 98.67 ± 1.16 | 98.29 ± 0.01 | 502 | 0.078 | |
| 5 | VGN-related | 95.57 ± 0.35 | 95.54 ± 0.34 | 95.60 ± 0.04 | 121 | 0.018 |
| RN-related | 97.56 ± 1.04 | 98.36 ± 0.87 | 97.91 ± 0.01 | 184 | 0.023 | |
| All | 98.48 ± 0.66 | 98.00 ± 0.44 | 98.21 ± 0.01 | 346 | 0.054 | |
| 2 | VGN-related | 90.75 ± 1.37 | 92.30 ± 0.97 | 91.67 ± 0.01 | 34 | 0.008 |
| RN-related | 97.43 ± 1.10 | 95.54 ± 1.07 | 96.54 ± 0.01 | 58 | 0.011 | |
| All | 97.23 ± 0.76 | 95.85 ± 0.95 | 96.62 ± 0.02 | 97 | 0.021 |
| Author | Method | Segment Length (s) | Se (%) | Sp (%) | Acc (%) |
|---|---|---|---|---|---|
| Panda [45] | FFREWT + CNN | 8 | 99.95 | 95.95 | 99.04 |
| Verma [47] | Features + RF | 8 | 95.17 | 97.32 | 97.17 |
| Cheng [40] | Features + SVM | 8 | 93.87 | 95.56 | 95.46 |
| Nguyen [41] | Features + SVM | 5 | 90.8 | 96.90 | 95.70 |
| Tripathy [48] | Taylor–Fourier Transform + Phase Difference + SVM | 5 | 82.61 | 79.57 | 80.99 |
| Xu [43] | VMD + Boosting-CART | 5 | 97.32 | 98.95 | 98.29 |
| Lai [44] | 2D-CNN | 3 | 95.05 | 99.43 | 98.82 |
| Acharya [46] | CNN | 2 | 95.32 | 91.04 | 93.18 |
| Our | FFREWT + Multiple Complex Networks + XGBoost | 10 | 99.02 ± 0.53 | 98.44 ± 0.43 | 98.73 ± 0.02 |
| 8 | 98.06 ± 1.29 | 98.67 ± 1.16 | 98.29 ± 0.01 | ||
| 5 | 98.48 ± 0.66 | 98.00 ± 0.44 | 98.21 ± 0.01 | ||
| 2 | 97.23 ± 0.76 | 95.85 ± 0.95 | 96.62 ± 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, Z.; Yu, M.; Yu, J.; Han, X.; Li, J.; Qu, Y. Life-Threatening Ventricular Arrhythmia Identification Based on Multiple Complex Networks. Electronics 2025, 14, 2921. https://doi.org/10.3390/electronics14152921
Cai Z, Yu M, Yu J, Han X, Li J, Qu Y. Life-Threatening Ventricular Arrhythmia Identification Based on Multiple Complex Networks. Electronics. 2025; 14(15):2921. https://doi.org/10.3390/electronics14152921
Chicago/Turabian StyleCai, Zhipeng, Menglin Yu, Jiawen Yu, Xintao Han, Jianqing Li, and Yangyang Qu. 2025. "Life-Threatening Ventricular Arrhythmia Identification Based on Multiple Complex Networks" Electronics 14, no. 15: 2921. https://doi.org/10.3390/electronics14152921
APA StyleCai, Z., Yu, M., Yu, J., Han, X., Li, J., & Qu, Y. (2025). Life-Threatening Ventricular Arrhythmia Identification Based on Multiple Complex Networks. Electronics, 14(15), 2921. https://doi.org/10.3390/electronics14152921