

Modelling Key Health Indicators from Sensor Data Using Knowledge Graphs and Fuzzy Logic

 ,
, 
 ,
,  and
and
Abstract

1. Introduction
Literature Review
2. Materials and Methods
- KG Model of KHI: We construct hierarchical knowledge graphs to represent critical health indicators, including sleep patterns, excretion control, physical mobility, and social interaction. In this work, we use the term ’excretion control’ as a general category; however, in clinical practice, it is more common to refer specifically to urinary and faecal control. It is important to note that in patients with incontinence who use absorbent products, data collection through environmental sensors may present limitations that should be considered. These graphs represent indicators as nodes, with edges that define relationships with control variables derived from sensor data. This structured approach allows us to integrate clinical knowledge with quantitative data, providing a comprehensive view of health status.
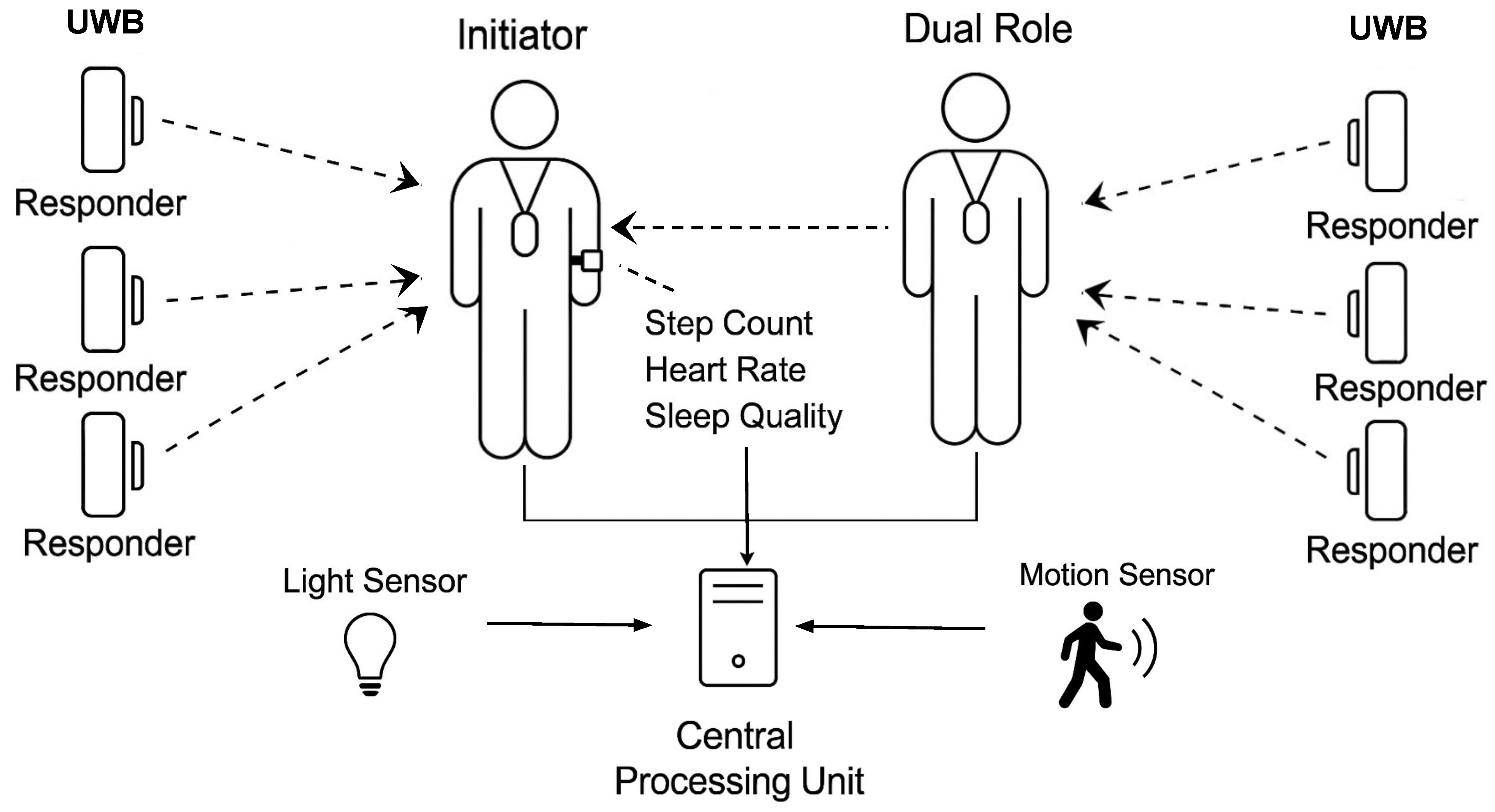
- Sensor Architecture for Data Acquisition: A minimally invasive sensing architecture is implemented, combining wearable devices and ambient sensors. Wearable devices track physical activity and sleep, while ambient sensors provide indoor localisation and activity data. This integration provides a general view of daily activity patterns while prioritising user comfort and long-term adherence.
- FL modelling of Linguistic Protoforms: FL bridges the gap between sensor data and clinical language. The temporal and linguistic terms used by healthcare professionals are modelled using membership functions, which allow the system to reason with imprecise and subjective information. This approach ensures that the system’s output is clinically relevant and interpretable.
2.1. Knowledge Graph Representation of Key Health Indicators
- V is a set of nodes (vertices) that represent entities or concepts related to health indicators. These entities are not merely static data points but are imbued with linguistic meaning, facilitating human-like reasoning.
- E is a set of edges that represent the relationships between these entities. Each edge is an ordered pair where .
- L is a set of labels associated with both the nodes and edges, providing semantic context.
- Each node/entity is associated with a protoform that captures its underlying semantic structure.
- These protoforms are instantiated with specific values derived from:
- –
- Terms: Linguistic variables representing ranges or categories of health indicators (e.g. “active mobility”, “adequate sleep time”).
- –
- Temporal Restrictions: Time-based constraints or patterns associated with health indicators (e.g., low physical activity “while daytime”).
- –
- Location Restrictions: Location-based constraints or patterns associated with user activity (e.g., sleep activity levels “in the living room”).
- –
- Quantifiers: Linguistic terms represent relative or absolute quantities, allowing the manipulation of linguistic concepts. They can be modelled under crisp or fuzzy approaches (e.g., “adequate number of excretions”, “most of sleeping time”).
- –
- Data Streams: Composed by the data from ambient and wearable devices collected and the inferred protoforms over time.
- This connection to protoforms allows the KG to reason with the semantic meaning of health data, not just its numerical values.
- In fuzzy rules, the relationships between nodes are assigned degrees of membership, reflecting the strength or certainty to the antecedents by means of fuzzy norms (T-norms and Co-norms) to represent conjunctive and disjunctive relationships, respectively.
- By applying these operators, the KG can perform fuzzy inference, combining evidence from multiple relationships to derive conclusions about health indicators. This allows for a more robust and flexible representation of complex health patterns.
2.2. Sensor Architecture for Data Acquisition
2.3. Fuzzy Logic Modelling of Linguistic Protoforms for Sensor Data
- V designates the fuzzy data stream derived from sensor or location sources.
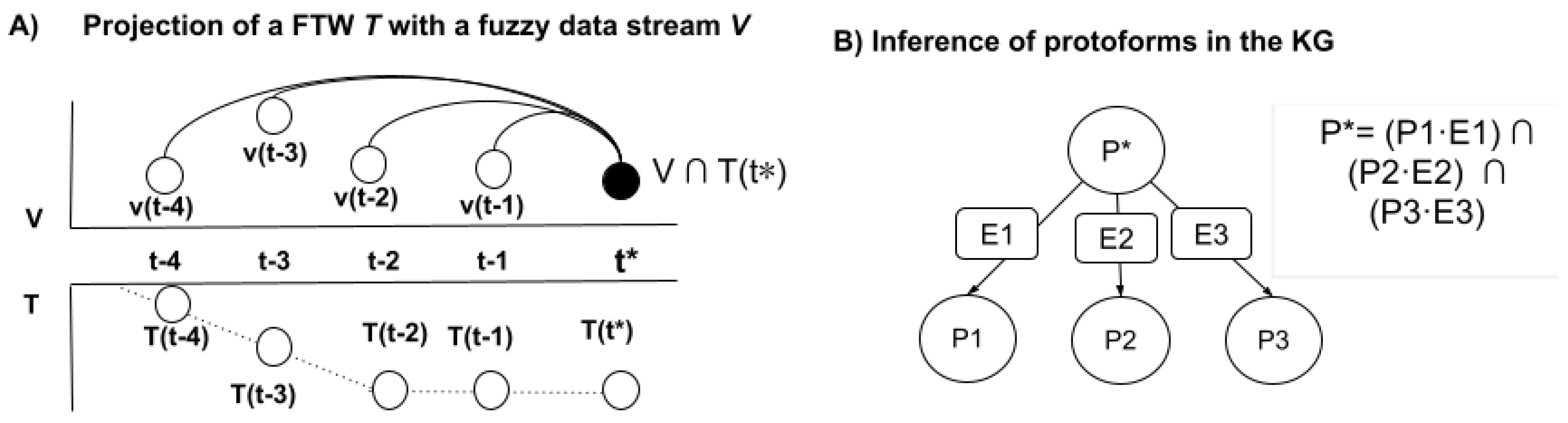
- T, an optional element, specifies a fuzzy temporal window (FTW) , within which the fuzzy data streams are aggregated, represented as . The projection of a fuzzy temporal window T with a fuzzy data stream is achieved through a membership function associated with the FTW, which is derived from the temporal displacement , where , measuring the interval from a present time to the preceding timestamps within the data stream. For every timestamp , we compute the combined membership degrees of the terms, considering the fuzzy temporal influence, utilising t-norm and co-norm operations:where define the aggregation of the temporal term T and the fuzzy stream V by means of t-norm ∩ for each timestamp and co-norm ∪ for aggregating them. In Figure 4, we describe the projection of an FTW with a fuzzy data stream. The choice of norms (max–min, weighted average = ) is determined by the specific semantic context [38].
- –
- In max–min, the norms are defined as and , which are related to existential aggregators where a single value indicates the presence of a single value of V within the fuzzy temporal window T.
- –
- In weighted average = , the norms are defined as and , which are related to the weighted impact of the term V within the fuzzy temporal window T.
- L, also optional, acts as a location filter to compute the spatial interaction in the environment [12] .
- Q, also optional, acts as a quantifier to filter and modulate the degree of aggregation of .
3. Case Study
3.1. Real-Home Deployment
- A motion sensor and a flush sensor (both Aqara) in the bathroom, providing cross-validation for presence and flush detection (see Figure 6B).
- A smart plug to monitor energy consumption (TP-Link) in the bedroom lamp (see Figure 6C). Another smart plug in the living room to monitor the use of the TV.
- The patient wore a smart watch (Amazfit Bip U Pro) (see Figure 6D) that collected physiological and activity-related data, including heart rate, step count, and sleep quality, including periods of deep, normal, and light sleep.
3.2. Fuzzy Inference in KG for Sleep Pattern Evaluation
3.2.1. Input Data Sources
3.2.2. Knowledge Graph
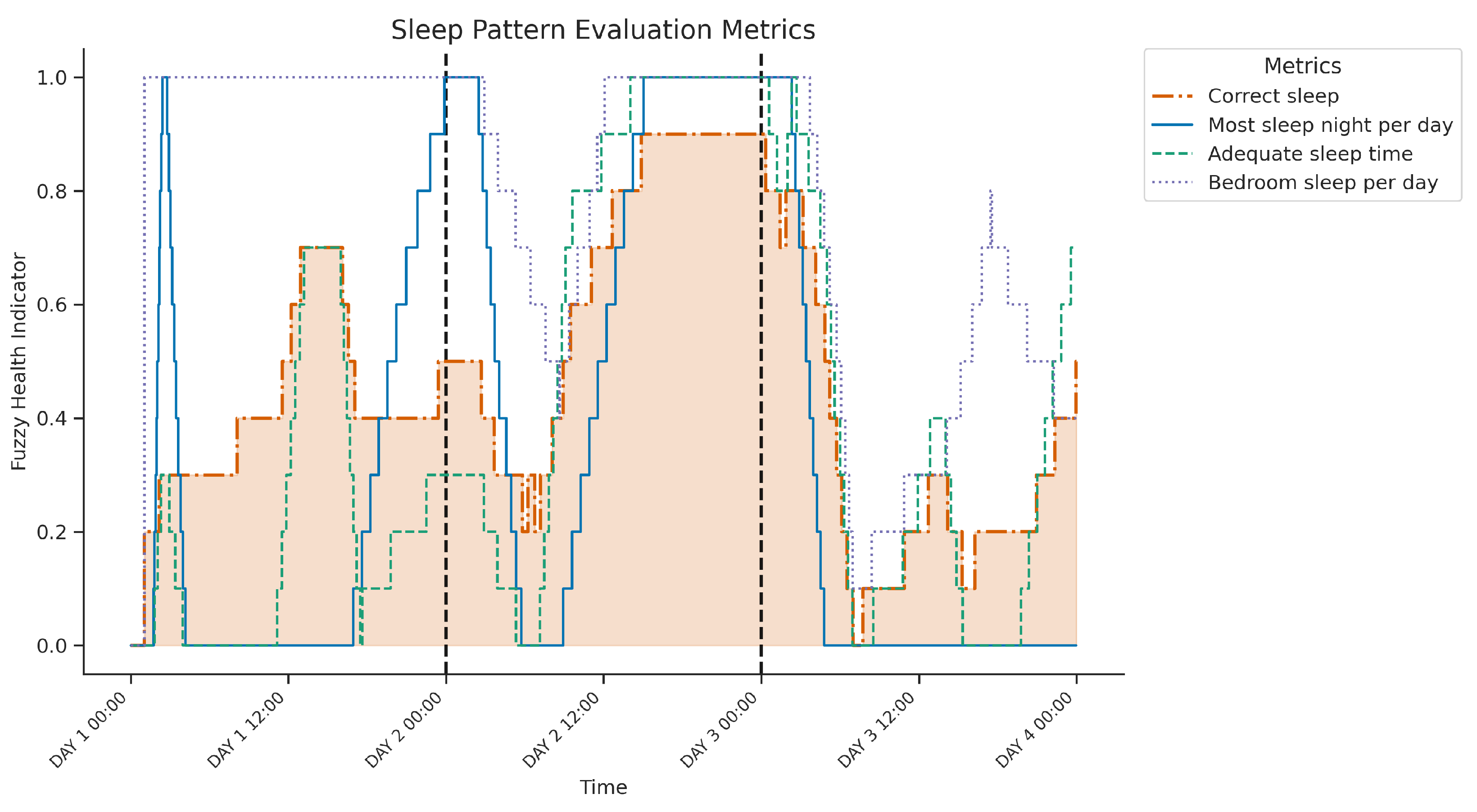
- +) SA: Adequate sleep time
- SA1: Most of the sleeping at night. Evaluates whether most of the sleeping time occurs during the night window and combines quantity (Q), temporality (T), and value streams (V).
- SA2: Sleeping quantity. Assesses if the total sleep time falls between 6 and 8 h per day. Fuzzy weighted by value (V) and time window (T).
- +) SB: Quality of sleep
- SB1: Sleeping is normal or deep. Measures if the majority of sleep is spent in normal or deep stages and uses value (V), quantity (Q), and temporal alignment (T)
- SB2: Sleep in the bedroom Assesses whether sleep occurs predominantly in the bedroom and relies on value (V), localisation (L), and quantity (Q).
3.2.3. Discussion and Explainability
3.3. Fuzzy Inference in KG for Excretion Control
3.3.1. Input Data Sources
3.3.2. Knowledge Graph
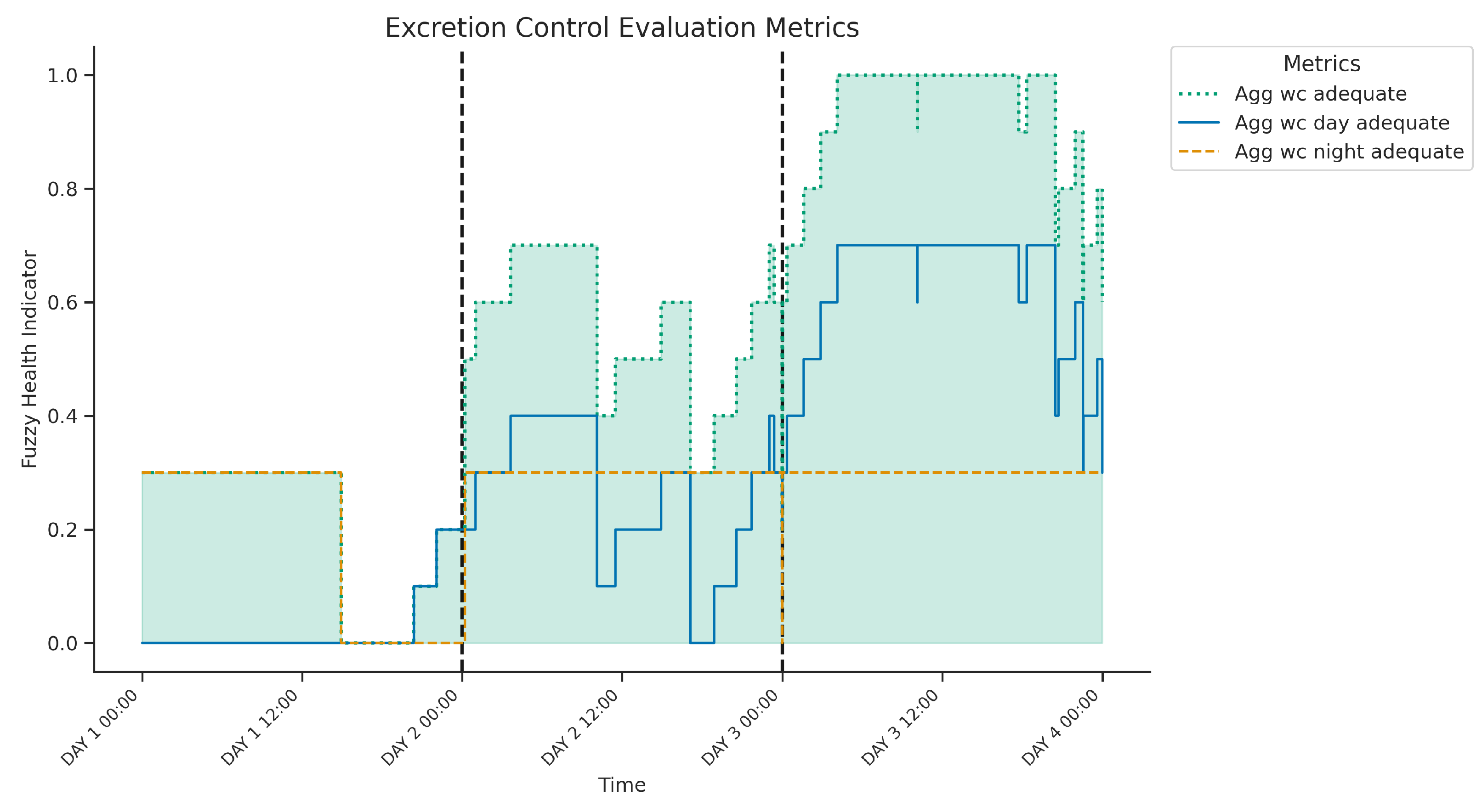
- +) SA: Daily excretions
- Captures regularity and frequency of bathroom visits throughout the day aggregating value (V) and time-based frequency (T) over the full day.
- Defined as healthy when the total number of inferred excretion episodes is between 3 and 5 per day.
- +) SB: Night excretions
- Evaluates bathroom visits during the night calculated using a fuzzy combination of value (V) and temporal indicator (T) restricted to night-time hours.
- Considered healthy if the number of visits ranges between 0 and 2.
- +) S1: Excretion detection
- Core detection mechanism combining: flush events, presence in the toilet, and localisation in the toilet room.
- Fuzzy temporal aggregation is applied over short intervals (2 to 4 min) to infer likely excretion episodes.
- Outputs a time-aligned indicator that feeds into both the SA and SB branches.
3.3.3. Discussion and Explainability
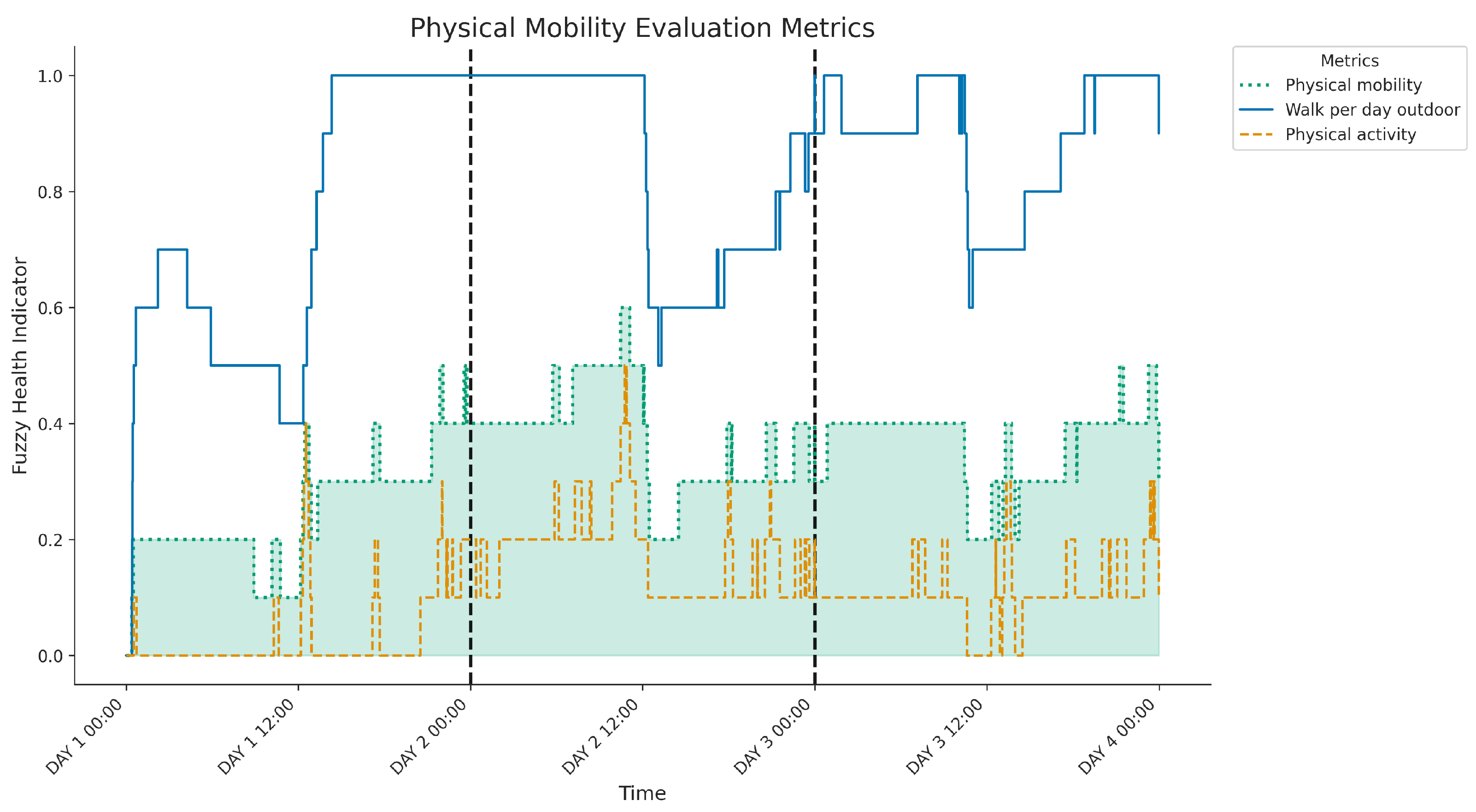
3.4. Fuzzy Inference in KG for Physical Mobility
3.4.1. Input Data Sources
3.4.2. Knowledge Graph
- +) SA: Physical activity
- SA1: Active mobility. Assesses whether an adequate number of steps is taken each day and combines quantity (Q), temporality (T), and step count values (V).
- SA2: Walking consecutive. Evaluates whether walking sessions include at least one sustained period of approximately 30 min. Derived from continuous step activity patterns, weighted by time (T) and value (V).
- +) SB: Most activity outdoor
- Checks whether most activity occurs outside the home environment. Using location data (L), step values (V), and quantity (Q) to infer whether physical activity occurs predominantly in outdoor settings.
- Considered relevant to prevent the sedentary routines commonly associated with indoor confinement.
- +) SB: Physical mobility
- Aggregates quantity and location using fuzzy temporal indicators. The model balances beneficial closeness with potential overdependence, providing a complete interpretation of daily caregiver engagement.
3.4.3. Discussion and Explainability
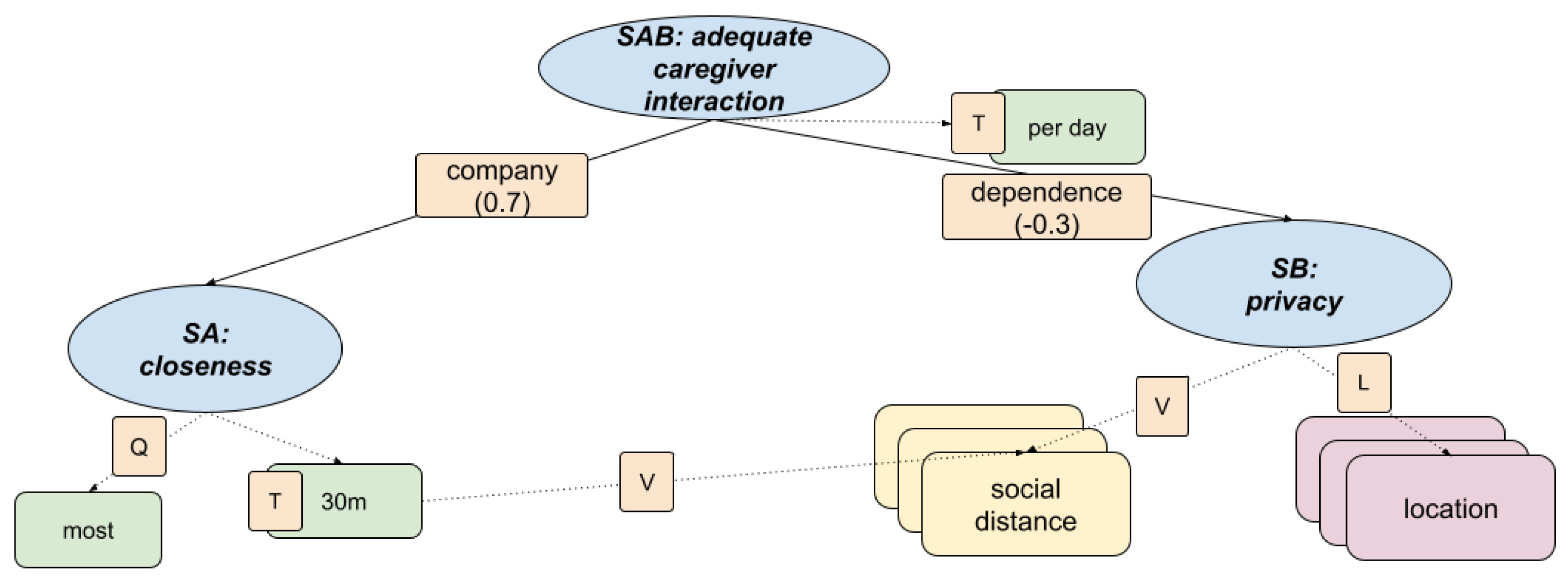
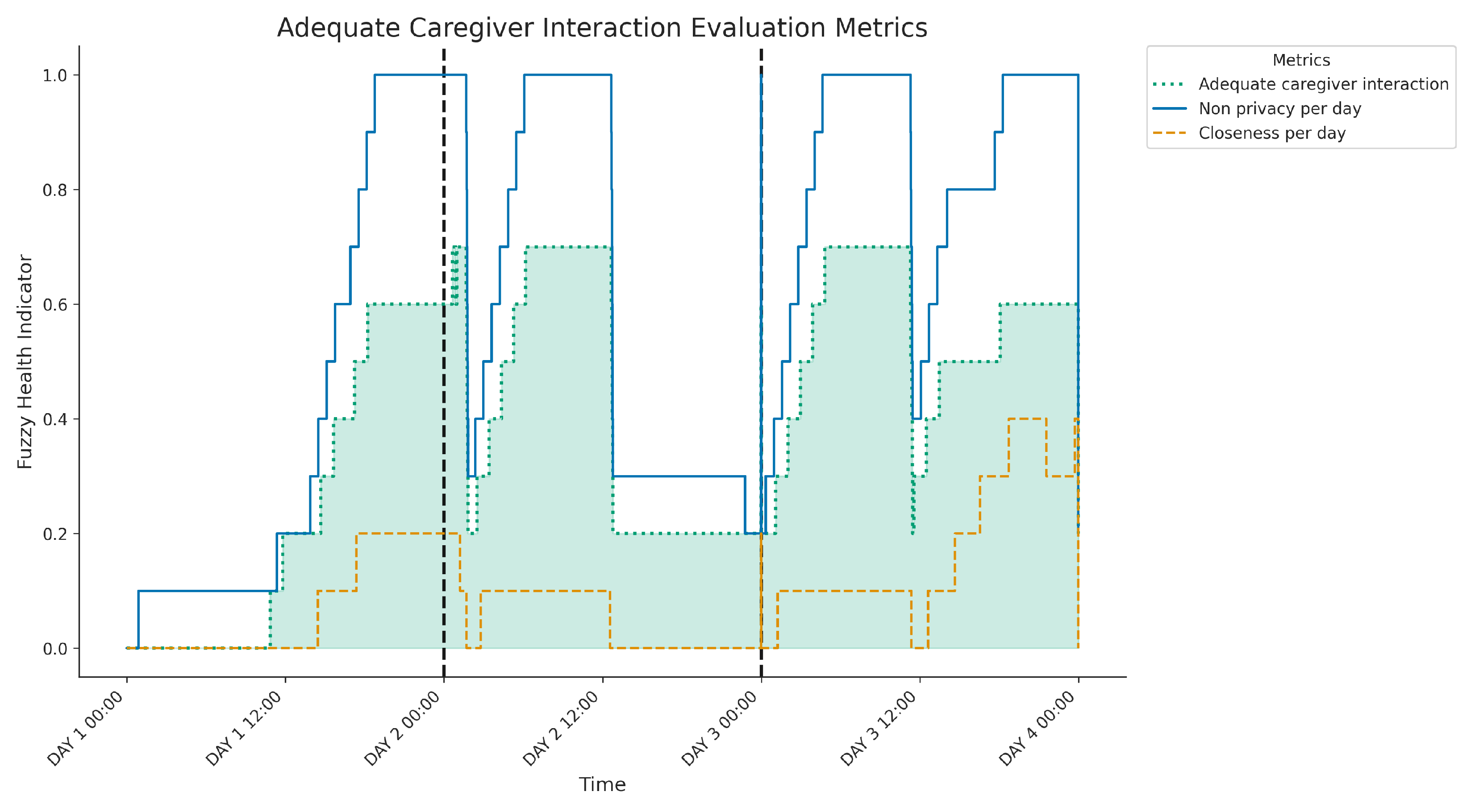
3.5. Fuzzy Inference in KG for Adequate Caregiver Interaction
3.5.1. Input Data Sources
3.5.2. Knowledge Graph
- +) SA: Closeness
- The social distance is tracked and compared against a fuzzy threshold (for example, within 1 to 2 metres for at least 30 min/day).
- Includes temporal coverage (T), quantity of interactions (Q), and value assessment (V) of proximity episodes.
- Based on the detection of caregiver presence in specific rooms (e.g., bedroom, bathroom) where autonomy is expected.
- Uses spatial location (L) and value (V) indicators to assess appropriateness of room-sharing patterns.
- Aggregates both positive (company) and negative (dependence) contributions using fuzzy temporal indicators. The model balances beneficial closeness with potential over-dependence, providing a complete interpretation of daily caregiver engagement.
3.5.3. Discussion and Explainability
3.6. Data-Driven Approaches for Modelling KHI
- Temporal windowing: We employed a sliding window approach to aggregate sensor data [39]. This method enabled the capture of both current and preceding sensor values within defined window size (WS), providing a comprehensive context for each point of time. The window size for each protoform is elaborated in further detail in Table 1.
- Protoform Defuzzification: To enable the training of supervised learning models, the expert-defined protoforms of KHI were defuzzified using alpha-cuts. This transformation converted the fuzzy linguistic descriptions into a quantifiable, typically binary, classification problem for each indicator. The precise alpha-cut values used in this stage are presented in Table 1.
- Cross-Validation Strategy: For the validation of our models, we implemented a cross-validation strategy of 2-hour-leave-out. This method ensured that the models’ performance was assessed on entirely unseen temporal blocks of data, thus providing a more reliable estimation of their generalisation capabilities.
- Model Evaluation: The performance of the selected machine learning models, specifically K-Nearest Neighbours (KNN), Support Vector Machines (SVM) and Random Forest (RF), was thoroughly evaluated. Their effectiveness was quantified using established metrics, namely accuracy (ACC) and F1 score. The detailed evaluation results for each model are summarised in Table 1.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AAL | Ambient Assisted Living |
| FL | Fuzzy Logic |
| FTW | Fuzzy Temporal Window |
| KHI | Fuzzy Health Indicators |
| KG | Knowledge Graph |
| TLA | Three letter acronym |
| UWB | Ultra-Wideband |
References
- Caballero, P.; Ortiz, G.; Medina-Bulo, I. Systematic literature review of ambient assisted living systems supported by the Internet of Things. Univers. Access Inf. Soc. 2024, 23, 1631–1656. [Google Scholar] [CrossRef]
- Wang, K.; Ghafurian, M.; Chumachenko, D.; Cao, S.; Butt, Z.A.; Salim, S.; Abhari, S.; Morita, P.P. Application of artificial intelligence in active assisted living for aging population in real-world setting with commercial devices—A scoping review. Comput. Biol. Med. 2024, 173, 108340. [Google Scholar] [CrossRef] [PubMed]
- Perandrés-Gómez, A.; Merdeces Párraga-Vico, M.; Díaz-Jiménez, D.; Medina-Quero, J.; Polo-Rodríguez, A. Impact of Training Programmes in Digital Skills to Reduce Unwanted Loneliness in Older Andalusian Women. In Proceedings of the Italian Forum of Ambient Assisted Living, Florence, Italy, 25–28 June 2024; pp. 431–440. [Google Scholar]
- Rehan, H. Enhancing Early Detection and Management of Chronic Diseases With AI-Driven Predictive Analytics on Healthcare Cloud Platforms. J. AI-Assist. Sci. Discov. 2024, 4, 1–38. [Google Scholar]
- Rehman, A.; Naz, S.; Razzak, I. Leveraging big data analytics in healthcare enhancement: Trends, challenges and opportunities. Multimed. Syst. 2022, 28, 1339–1371. [Google Scholar] [CrossRef]
- Peláez-Aguilera, M.D.; Espinilla, M.; Fernandez Olmo, M.R.; Medina, J. Fuzzy linguistic protoforms to summarize heart rate streams of patients with ischemic heart disease. Complexity 2019, 2019, 694126. [Google Scholar] [CrossRef]
- Polo-Rodríguez, A.; Romero-Sanchez, J.; Fernández-García, E.; Paloma-Castro, O.; Porcel-Gálvez, A.M.; Medina-Quero, J. Review on internet of things for innovation in nursing process-a pubmed-based search. In Proceedings of the International Conference on Ubiquitous Computing and Ambient Intelligence, Riviera Maya, Mexico, 28–29 November 2023; pp. 57–70. [Google Scholar]
- Wang, J.; Zhang, Q.; Shi, F.; Li, D.; Cai, Y.; Wang, J.; Li, B.; Wang, X.; Zhang, Z.; Zheng, C. Knowledge graph embedding model with attention-based high-low level features interaction convolutional network. Inf. Process. Manag. 2023, 60, 103350. [Google Scholar] [CrossRef]
- Arrotta, L.; Civitarese, G.; Bettini, C. Dexar: Deep explainable sensor-based activity recognition in smart-home environments. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2022, 6, 1–30. [Google Scholar] [CrossRef]
- Salguero, A.G.; Espinilla, M.; Delatorre, P.; Medina, J. Using ontologies for the online recognition of activities of daily living. Sensors 2018, 18, 1202. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Razik, M.S.M.; Rizk, H.I.; Zein, M.M.; Abdel-Megeid, S.M.E.S.; Abd El Fatah, S.A. Promoting the culture of key performance indicators (KPIs) among primary health care staff at health district level: An intervention study. Eval. Program Plan. 2023, 96, 102188. [Google Scholar] [CrossRef]
- Polo-Rodriguez, A.; Cavallo, F.; Nugent, C.; Medina-Quero, J. Human activity mining in multi-occupancy contexts based on nearby interaction under a fuzzy approach. Internet Things 2024, 25, 101018. [Google Scholar] [CrossRef]
- Gürsel, G. Healthcare, uncertainty, and fuzzy logic. Digit. Med. 2016, 2, 101–112. [Google Scholar] [CrossRef]
- Chen, X.; Hu, Z.; Sun, Y. Fuzzy logic based logical query answering on knowledge graphs. In Proceedings of the AAAI Conference on Artificial Intelligence, Online, 22 February–1 March 2022; Volume 36, pp. 3939–3948. [Google Scholar]
- Johnson, K.B.; Wei, W.Q.; Weeraratne, D.; Frisse, M.E.; Misulis, K.; Rhee, K.; Zhao, J.; Snowdon, J.L. Precision medicine, AI, and the future of personalized health care. Clin. Transl. Sci. 2021, 14, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Lin, K.J.; Wang, H. Toward Lightweight End-to-End Semantic Learning of Real-Time Human Activity Recognition for Enabling Ambient Intelligence. IEEE Trans. Knowl. Data Eng. 2024, 36, 7157–7170. [Google Scholar] [CrossRef]
- Chen, T.C.T. Explainable Ambient Intelligence (XAmI): Explainable Artificial Intelligence Applications in Smart Life; Springer Nature: Berlin/Heidelberg, Germany, 2024. [Google Scholar]
- Chen, L.; Nugent, C.D.; Wang, H. A knowledge-driven approach to activity recognition in smart homes. IEEE Trans. Knowl. Data Eng. 2011, 24, 961–974. [Google Scholar] [CrossRef]
- Medina, J.; Espinilla, M.; Zafra, D.; Martínez, L.; Nugent, C. Fuzzy fog computing: A linguistic approach for knowledge inference in wearable devices. In Proceedings of the Ubiquitous Computing and Ambient Intelligence: 11th International Conference, UCAmI 2017, Philadelphia, PA, USA, 7–10 November 2017; Springer: Berlin/Heidelberg, Germany, 2017; pp. 473–485. [Google Scholar]
- Zadeh, L.A. Fuzzy sets. Inf. Control 1965, 8, 338–353. [Google Scholar] [CrossRef]
- Sajedi, S.N.; Maadani, M.; Nesari Moghadam, M. F-LEACH: A fuzzy-based data aggregation scheme for healthcare IoT systems. J. Supercomput. 2022, 78, 1030–1047. [Google Scholar] [CrossRef]
- Zadeh, L.A. A prototype-centered approach to adding deduction capability to search engines-the concept of protoform. In Proceedings of the 2002 Annual Meeting of the North American Fuzzy Information Processing Society Proceedings, NAFIPS-FLINT 2002 (Cat. No. 02TH8622), New Orleans, LA, USA, 27–29 June 2002; pp. 523–525. [Google Scholar]
- Fontenla-Seco, Y.; Bugarin, A.; Lama, M. Fuzzy temporal protoforms for the quantitative description of processes in natural language. In Proceedings of the 2021 IEEE International Conference on Fuzzy Systems (FUZZ-IEEE), Luxembourg, 11–14 July 2021; pp. 1–6. [Google Scholar]
- Ramos-Soto, A.; Bugarin, A.J.; Barro, S.; Taboada, J. Linguistic descriptions for automatic generation of textual short-term weather forecasts on real prediction data. IEEE Trans. Fuzzy Syst. 2014, 23, 44–57. [Google Scholar] [CrossRef]
- Kaczmarek-Majer, K.; Casalino, G.; Castellano, G.; Hryniewicz, O.; Dominiak, M. Explaining smartphone-based acoustic data in bipolar disorder: Semi-supervised fuzzy clustering and relative linguistic summaries. Inf. Sci. 2022, 588, 174–195. [Google Scholar] [CrossRef]
- Chen, K.; Zhang, D.; Yao, L.; Guo, B.; Yu, Z.; Liu, Y. Deep learning for sensor-based human activity recognition: Overview, challenges, and opportunities. ACM Comput. Surv. (CSUR) 2021, 54, 1–40. [Google Scholar] [CrossRef]
- Liu, P.; Wang, L.; Ranjan, R.; He, G.; Zhao, L. A survey on active deep learning: From model driven to data driven. ACM Comput. Surv. (CSUR) 2022, 54, 1–34. [Google Scholar] [CrossRef]
- Abidi, S.S.R.; Abidi, S.R. Intelligent health data analytics: A convergence of artificial intelligence and big data. In Healthcare Management Forum; SAGE Publications: Los Angeles, CA, USA, 2019; Volume 32, pp. 178–182. [Google Scholar]
- Liaw, W.; Kakadiaris, I.A. Primary care artificial intelligence: A branch hiding in plain sight. Ann. Fam. Med. 2020, 18, 194. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, R.C. Quality Health Care: A Guide to Developing and Using Indicators; Jones & Bartlett Learning: Burlington, MA, USA, 2019. [Google Scholar]
- Loh, H.W.; Ooi, C.P.; Seoni, S.; Barua, P.D.; Molinari, F.; Acharya, U.R. Application of explainable artificial intelligence for healthcare: A systematic review of the last decade (2011–2022). Comput. Methods Programs Biomed. 2022, 226, 107161. [Google Scholar] [CrossRef] [PubMed]
- Wan, S.; Guan, S.; Tang, Y. Advancing bridge structural health monitoring: Insights into knowledge-driven and data-driven approaches. J. Data Sci. Intell. Syst. 2024, 2, 129–140. [Google Scholar] [CrossRef]
- Singh, B.; Chastin, S.; Miatke, A.; Curtis, R.; Dumuid, D.; Brinsley, J.; Ferguson, T.; Szeto, K.; Simpson, C.; Eglitis, E.; et al. Real-world accuracy of wearable activity trackers for detecting medical conditions: Systematic review and meta-analysis. JMIR mHealth uHealth 2024, 12, e56972. [Google Scholar] [CrossRef]
- Adewoyin, O.; Wesson, J.; Vogts, D. User modelling to support behavioural modelling in smart environments. In Proceedings of the 2022 3rd International Conference on Next Generation Computing Applications (NextComp), Flic-en-Flac, Mauritius, 6–8 October 2022; pp. 1–6. [Google Scholar]
- Martínez-Cruz, C.; Quero, J.M.; Serrano, J.M.; Gramajo, S. Monwatch: A fuzzy application to monitor the user behavior using wearable trackers. In Proceedings of the 2020 IEEE International Conference on Fuzzy Systems (FUZZ-IEEE), Glasgow, UK, 19–24 July 2020; pp. 1–8. [Google Scholar]
- Bugarin, A.; Marín, N.; Sánchez, D.; Trivino, G. Fuzzy knowledge representation for linguistic description of time series. In Proceedings of the 2015 Conference of the International Fuzzy Systems Association and the European Society for Fuzzy Logic and Technology (IFSA-EUSFLAT-15), Gijón, Spain, 30 June–3 July 2015; Atlantis Press: Amsterdam, The Netherlands, 2015; pp. 1346–1353. [Google Scholar]
- Silva, M.A.S.; Dimuro, G.P.; Borges, E.N.; Lucca, G.; Marco-Detchart, C. Analysis of Fuzzy Techniques in Edge Detection. In Proceedings of the International Conference on Enterprise Information Systems, Prague, Czech Republic, 24–26 April 2023; Springer: Berlin/Heidelberg, Germany, 2024; pp. 161–180. [Google Scholar]
- Medina, J.; Martinez, L.; Espinilla, M. Subscribing to fuzzy temporal aggregation of heterogeneous sensor streams in real-time distributed environments. Int. J. Commun. Syst. 2017, 30, e3238. [Google Scholar] [CrossRef]
- Sun, L.; Yang, X.; Hu, C. Dswhar: A dynamic sliding window based human activity recognition method. In Proceedings of the 2022 IEEE Smartworld, Ubiquitous Intelligence & Computing, Scalable Computing & Communications, Digital Twin, Privacy Computing, Metaverse, Autonomous & Trusted Vehicles (SmartWorld/UIC/ScalCom/DigitalTwin/PriComp/Meta), Haikou, China, 15–18 December 2022; pp. 1421–1426. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Alpha-Cut | WS | Protoform | ACC | F1 Score | ||||
|---|---|---|---|---|---|---|---|---|
| SVM | RF | KNN | SVM | RF | KNN | |||
| 0.75 | 360 | C#most_sleep_night_per_day | 0.89 | 0.83 | 0.87 | 0.88 | 0.79 | 0.88 |
| 0.75 | 360 | C#sleep_per_day | 0.56 | 0.76 | 0.88 | 0.52 | 0.73 | 0.89 |
| 0.98 | 360 | C#deep_per_day | 0.98 | 0.99 | 0.97 | 0.99 | 0.99 | 0.98 |
| 0.71 | 360 | C#bedroom_sleep_per_day | 0.71 | 0.67 | 0.86 | 0.66 | 0.62 | 0.86 |
| 0.5 | 15 | C#excretion_detection | 0.99 | 0.99 | 0.99 | 0.99 | 0.99 | 0.99 |
| 0.5 | 360 | C#agg_wc_day_adequate | 0.77 | 0.83 | 0.92 | 0.75 | 0.81 | 0.92 |
| 0.25 | 360 | C#agg_wc_night_adequate | 0.82 | 0.90 | 0.96 | 0.83 | 0.88 | 0.96 |
| 0.25 | 360 | C#active_mobility | 0.74 | 0.80 | 0.95 | 0.71 | 0.78 | 0.95 |
| 0.25 | 60 | C#walking30m | 0.98 | 0.96 | 0.98 | 0.97 | 0.96 | 0.98 |
| 0.75 | 360 | C#walk_per_day_outdoor | 0.81 | 0.81 | 0.92 | 0.79 | 0.79 | 0.92 |
| 0.25 | 360 | C#social_distance2_per_day | 0.65 | 0.72 | 0.90 | 0.61 | 0.70 | 0.90 |
| 0.25 | 360 | C#non_privacy__per_day | 0.76 | 0.84 | 0.90 | 0.74 | 0.83 | 0.86 |
| AVG | 0.80 | 0.84 | 0.93 | 0.79 | 0.82 | 0.92 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polo-Rodríguez, A.; López, I.V.; Diaz, R.; Rivadeneyra, A.; Gil, D.; Medina-Quero, J. Modelling Key Health Indicators from Sensor Data Using Knowledge Graphs and Fuzzy Logic. Electronics 2025, 14, 2459. https://doi.org/10.3390/electronics14122459
Polo-Rodríguez A, López IV, Diaz R, Rivadeneyra A, Gil D, Medina-Quero J. Modelling Key Health Indicators from Sensor Data Using Knowledge Graphs and Fuzzy Logic. Electronics. 2025; 14(12):2459. https://doi.org/10.3390/electronics14122459
Chicago/Turabian StylePolo-Rodríguez, Aurora, Isabel Valenzuela López, Raquel Diaz, Almudena Rivadeneyra, David Gil, and Javier Medina-Quero. 2025. "Modelling Key Health Indicators from Sensor Data Using Knowledge Graphs and Fuzzy Logic" Electronics 14, no. 12: 2459. https://doi.org/10.3390/electronics14122459
APA StylePolo-Rodríguez, A., López, I. V., Diaz, R., Rivadeneyra, A., Gil, D., & Medina-Quero, J. (2025). Modelling Key Health Indicators from Sensor Data Using Knowledge Graphs and Fuzzy Logic. Electronics, 14(12), 2459. https://doi.org/10.3390/electronics14122459