_Kalra.png)

Development of AI-Based Prediction of Heart Attack Risk as an Element of Preventive Medicine

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Dataset
- Age—age of the patient;
- Sex—gender of the patient (male/female);
- Cholesterol—cholesterol levels of the patient;
- Blood Pressure—blood pressure of the patient (systolic/diastolic);
- Heart Rate—heart rate of the patient;
- Diabetes—whether the patient has diabetes (yes/no);
- Family History—family history of heart-related problems (1: yes, 0: no);
- Smoking—smoking status of the patient (1: smoker, 0: non-smoker);
- Obesity—obesity status of the patient (1: obese, 0: not-obese);
- Alcohol consumption—level of alcohol consumption by the patient (none/light/moderate/heavy);
- Exercise hours per week—number of exercise hours per week;
- Diet—dietary habits of the patient (healthy/average/nonhealthy);
- Previous heart problems—previous heart problems of the patient (1: yes, 0: no);
- Medication use—medication usage by the patient (1: yes, 0: no);
- Stress level—stress level reported by the patient (1–10);
- Sedentary hours per day—hours of sedentary activity per day;
- Income—income level of the patient;
- BMI—body mass index (BMI)of the patient;
- Triglycerides—triglyceride levels of the patient;
- Physical activity days per week—days of physical activity per week;
- Sleep hours per day—hours of sleep per day;
- Country—country of the patient;
- Continent—continent where the patient resides;
- Hemisphere—hemisphere where the patient resides;
- Heart attack risk—presence of heart attack risk (1: yes, 0: no).
2.2. Computational Analysis
3. Results
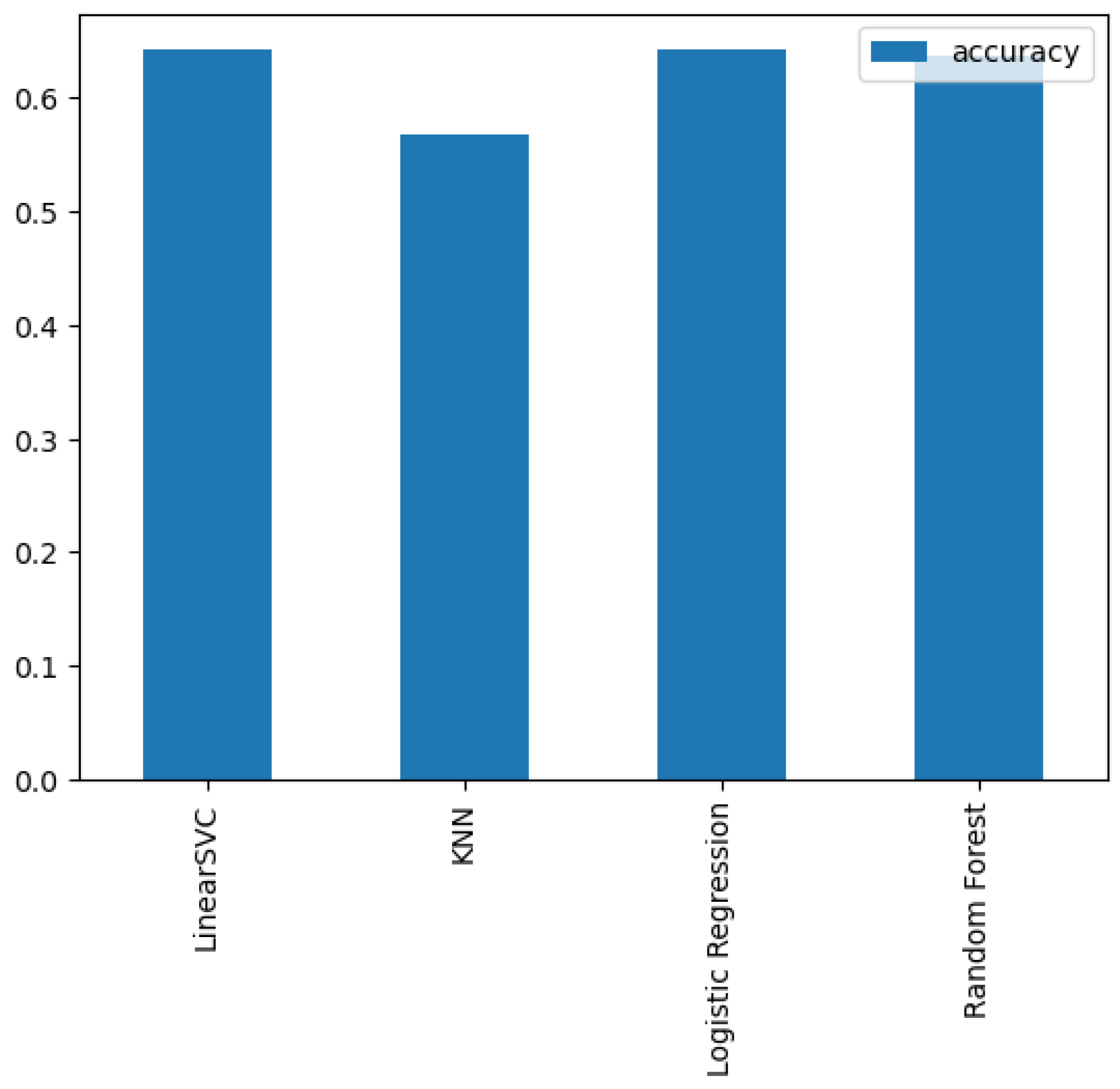
- LinearSVC—LinearSupport Vector Classifier;
- Logistic Regression—LogisticRegression;
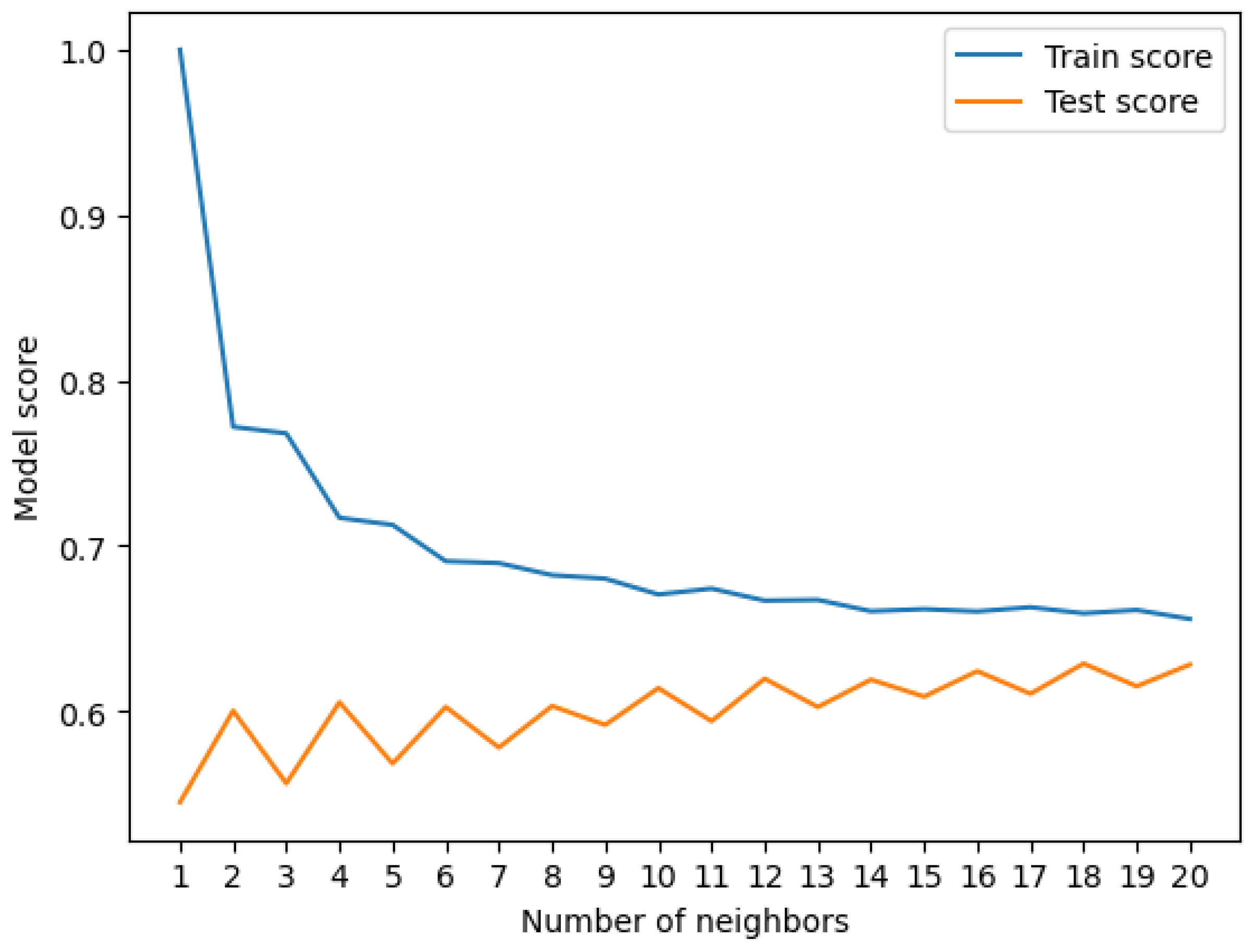
- K-Nearest Neighbors—KneighboursClassifier;
- RandomForest—RandomForestClassifier.
Hyperparameters Tuning
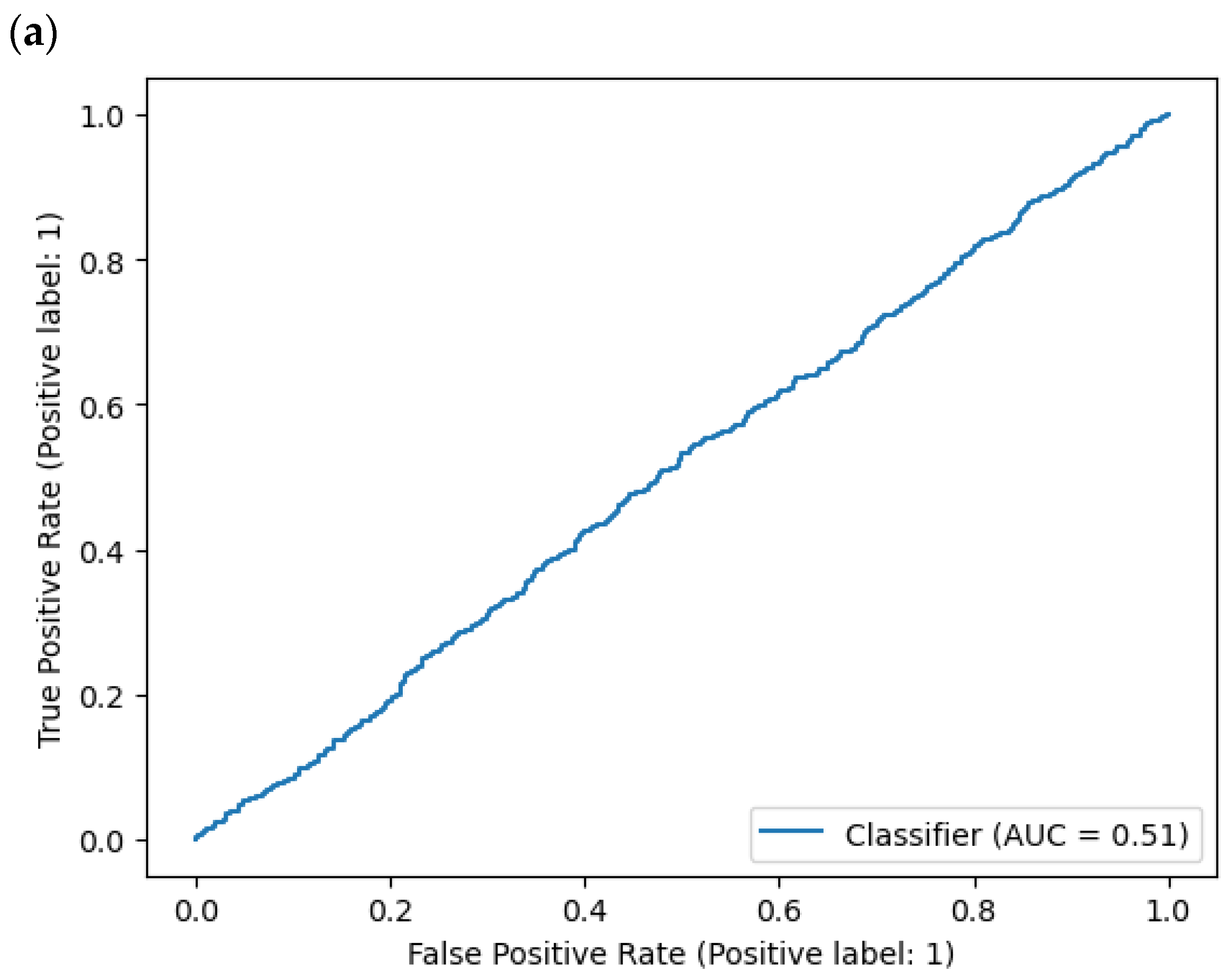
- True positive = model predicts 1 when truth is 1;
- False positive = model predicts 1 when truth is 0;
- True negative = model predicts 0 when truth is 0;
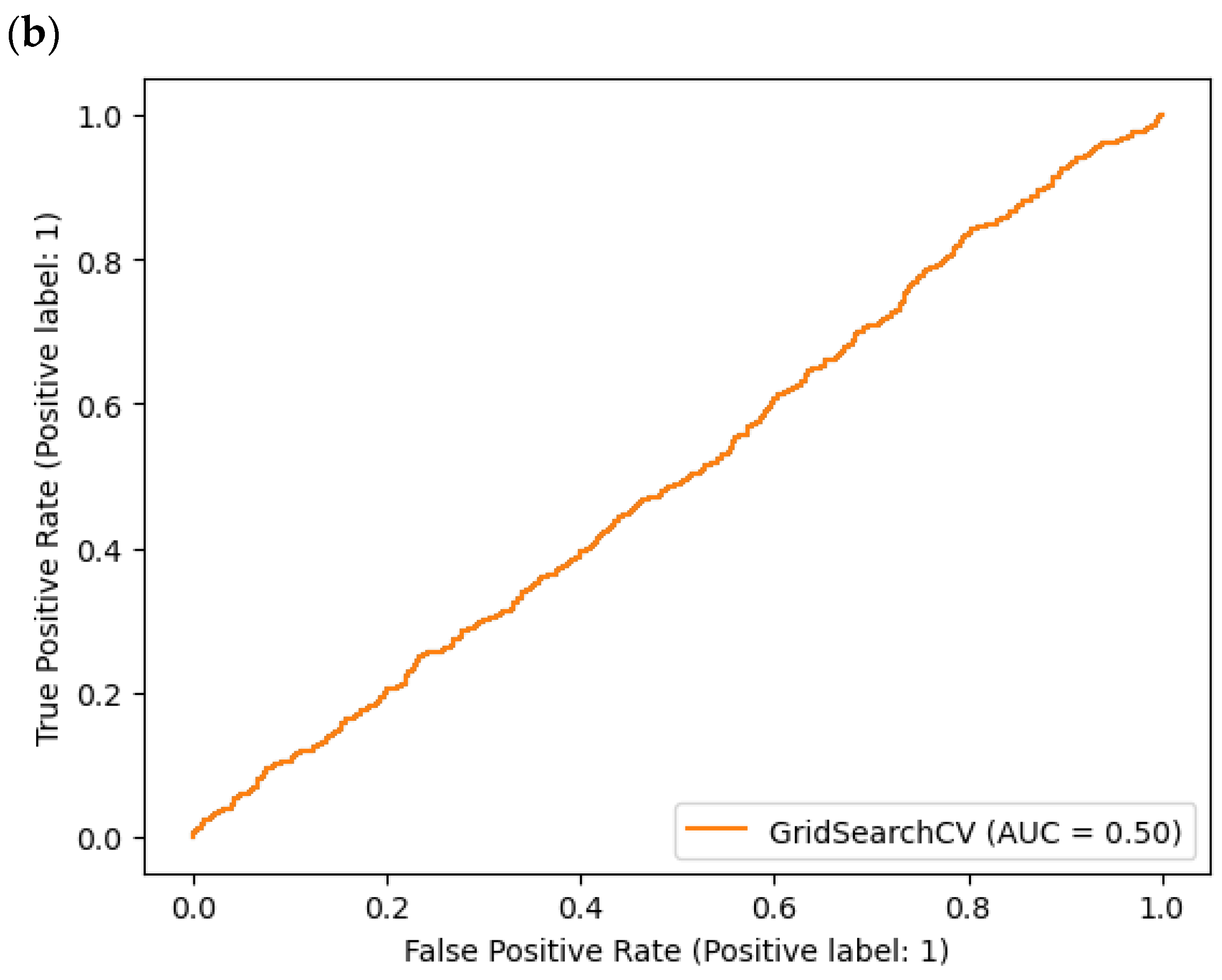
- False negative = model predicts 0 when truth is 1 (Figure 6).Figure 6. AUC (Area Under Curve): (a) DummyClassifier, (b) ExtraTreeClassifier.
![Electronics 13 00272 g006a]()
![Electronics 13 00272 g006b]()
4. Discussion
- Trust, information reliability, and security;
- Expected features, tailored feedback, and personalized advice;
- Adoption, usability, and general interest in artificial intelligence;
- Concerns and previous negative experiences with artificial intelligence;
- Perceived benefits and the usefulness of artificial intelligence in providing advice when regular contact with healthcare is not possible.
4.1. Limitations
4.2. Directions for Further Research
- legally and ethically (i.e.,the universal acceptance of preventive medicine);
- in terms of systematicity and the scope of periodic examinations of healthy and sick people;
- Automatic availability of data collected for analysis;
- The scope of notification and alerting about deviations from the norm.
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Verma, A.; Agarwal, G.; Gupta, A.K.; Sain, M. Novel Hybrid Intelligent Secure Cloud Internet of Things Based Disease Prediction and Diagnosis. Electronics 2021, 10, 3013. [Google Scholar] [CrossRef]
- Rojek, I.; Kozielski, M.; Dorożyński, J.; Mikołajewski, D. AI-Based Prediction of Myocardial Infarction Risk as an Element of Preventive Medicine. Appl. Sci. 2022, 12, 9596. [Google Scholar] [CrossRef]
- Shitara, S.; Tanaka-Mizuno, S.; Takashima, N.; Fujii, T.; Arima, H.; Kita, Y.; Tsuji, A.; Kitamura, A.; Urushitani, M.; Miura, K.; et al. Population-Based Incidence Rates of Subarachnoid Hemorrhage in Japan: The Shiga Stroke and Heart Attack Registry. J. Stroke 2022, 24, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Arima, H.; Takashima, N.; Kita, Y.; Miyamatsu, N.; Tanaka-Mizuno, S.; Shitara, S.; Urushitani, M.; Miura, K.; Nozaki, K. Seasonal Variation in Incidence of Stroke in a General Population of 1.4 Million Japanese: The Shiga Stroke Registry. Cerebrovasc. Dis. 2022, 51, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Naghavi, M. Preventive Cardiology: The SHAPE of the future. A Synopsis from the Screening for Heart Attack Prevention and Education (SHAPE) Task Force report. Herz 2007, 32, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Oeing, C.U.; Tschöpe, C.; Pieske, B. The new ESC Guidelines for acute and chronic heart failure 2016. Herz 2016, 41, 655–663. [Google Scholar] [CrossRef]
- Beleigoli, A.; Nicholls, S.J.; Brown, A.; Chew, D.P.; Beltrame, J.; Maeder, A.; Maher, C.; Versace, V.L.; Hendriks, J.M.; Tideman, P.; et al. Implementation and prospective evaluation of the Country Heart Attack Prevention model of care to improve attendance and completion of cardiac rehabilitation for patients with cardiovascular diseases living in rural Australia: A study protocol. BMJ Open 2022, 12, e054558. [Google Scholar] [CrossRef]
- Senanayake, S.; Halahakone, U.; Abell, B.; Kularatna, S.; McCreanor, V.; McPhail, S.M.; Redfern, J.; Tom, B.; Parsonage, W. Hybrid cardiac telerehabilitation for coronary artery disease in Australia: A cost-effectiveness analysis. BMC Health Serv. Res. 2023, 23, 512. [Google Scholar] [CrossRef]
- Chen, S.Q.; Xing, S.S.; Gao, H.Q. Clinical significance of automatic warning function of cardiac remote monitoring systems in preventing acute cardiac episodes. Pak. J. Med. Sci. 2014, 30, 1281–1285. [Google Scholar] [CrossRef]
- Pinero de Plaza, M.A.; Yadav, L.; Kitson, A. Co-designing, measuring, and optimizing innovations and solutions within complex adaptive health systems. Front. Health Serv. 2023, 3, 1154614. [Google Scholar] [CrossRef]
- Joshi, M.; Melo, D.P.; Ouyang, D.; Slomka, P.J.; Williams, M.C.; Dey, D. Current and Future Applications of Artificial Intelligence in Cardiac CT. Curr. Cardiol. Rep. 2023, 25, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Guo, N.; Ge, Y.; Zhang, L.; Oudkerk, M.; Xie, X. Development and application of artificial intelligence in cardiac imaging. Br. J. Radiol. 2020, 93, 20190812. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Liu, J.; Sun, Z.; Cui, Y.; He, Y.; Yang, Z. Deep learning analysis in coronary computed tomographic angiography imaging for the assessment of patients with coronary artery stenosis. Comput. Methods Programs Biomed. 2020, 196, 105651. [Google Scholar] [CrossRef] [PubMed]
- Molenaar, M.A.; Selder, J.L.; Nicolas, J.; Claessen, B.E.; Mehran, R.; Bescós, J.O.; Schuuring, M.J.; Bouma, B.J.; Verouden, N.J.; Chamuleau, S.A.J. Current State and Future Perspectives of Artificial Intelligence for Automated Coronary Angiography Imaging Analysis in Patients with Ischemic Heart Disease. Curr. Cardiol. Rep. 2022, 24, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Truslow, J.G.; Goto, S.; Homilius, M.; Mow, C.; Higgins, J.M.; MacRae, C.A.; Deo, R.C. Cardiovascular Risk Assessment Using Artificial Intelligence-Enabled Event Adjudication and Hematologic Predictors. Circ. Cardiovasc. Qual. Outcomes 2022, 15, e008007. [Google Scholar] [CrossRef] [PubMed]
- Serhal, H.; Abdallah, N.; Marion, J.M.; Chauvet, P.; Oueidat, M.; Humeau-Heurtier, A. Overview on prediction, detection, and classification of atrial fibrillation using wavelets and AI on ECG. Comput. Biol. Med. 2022, 142, 105168. [Google Scholar] [CrossRef] [PubMed]
- Dogan, M.V.; Knight, S.; Dogan, T.K.; Knowlton, K.U.; Philibert, R. External validation of integrated genetic-epigenetic biomarkers for predicting incident coronary heart disease. Epigenomics 2021, 13, 1095–1112. [Google Scholar] [CrossRef]
- Kakadiaris, I.A.; Vrigkas, M.; Yen, A.A.; Kuznetsova, T.; Budoff, M.; Naghavi, M. Machine Learning Outperforms ACC/AHA CVD Risk Calculator in MESA. J. Am. Hear. Assoc. 2018, 7, e009476. [Google Scholar] [CrossRef]
- Verma, L.; Srivastava, S.; Negi, P.C. A Hybrid Data Mining Model to Predict Coronary Artery Disease Cases Using Non-Invasive Clinical Data. J. Med. Syst. 2016, 40, 178. [Google Scholar] [CrossRef]
- Zarrin-Khameh, N.; Barzi, A.; Sadeghi, S. Intelligent system and risk of different diseases in the general population. Stud. Health Technol. Inform. 2001, 81, 601–603. [Google Scholar]
- Kaggle Data Set. Available online: https://www.kaggle.com/datasets/iamsouravbanerjee/heart-attack-prediction-dataset (accessed on 10 October 2023).
- Kronish, I.M.; Lynch, A.I.; Oparil, S.; Whittle, J.; Davis, B.R.; Simpson, L.M.; Krousel-Wood, M.; Cushman, W.C.; Chang, T.I.; Muntner, P. The Association Between Antihypertensive Medication Nonadherence and Visit-to-Visit Variability of Blood Pressure: Findings from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Hypertension 2016, 68, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Wald, N.; Morris, J. Lowering blood pressure to prevent myocardial infarction and stroke: A new preventive strategy. Health Technol Assess. 2003, 7, 1–94. [Google Scholar] [CrossRef] [PubMed]
- Moser, M.; Cushman, W.; Weber, M. Roundtable discussion: The ALLHAT trial. J. Clin. Hypertens. 2003, 5, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Jasiulewicz-Kaczmarek, M.; Antosz, K.; Zhang, C.; Waszkowski, R. Assessing the barriers to Industry 4.0 implementation from a maintenance management perspective–pilot study results. IFAC-PapersOnLine 2022, 55, 223–228. [Google Scholar] [CrossRef]
- Antosz, K.; Jasiulewicz-Kaczmarek, M.; Machado, J.; Relich, M. Application of principle component analysis and logistic regression to support Six Sigma implementation in maintenance. Eksploat. I Niezawodn. Maint. Reliab. 2023, 25, 174603. [Google Scholar] [CrossRef]
- Rojek, I.; Studziński, J. Comparison of different types of neuronal nets for failures location within water-supply networks. Eksploat. I Niezawodn.-Maint. Reliab. 2014, 16, 42–47. [Google Scholar]
- Rojek, I. Hybrid neural networks as prediction models. In Artifical Intelligence and Soft Computing. ICAISC 2010; Lecture Notes in Artificial Intelligence; Rutkowski, L., Scherer, R., Tadeusiewicz, R., Zadeh, L.A., Zurada, J.M., Eds.; Springer: Berlin/Heidelberg, Germany, 2010; Volume 6114, pp. 88–95. [Google Scholar]
- Mikołajewska, E.; Prokopowicz, P.; Mikolajewski, D. Computational gait analysis using fuzzy logic for everyday clinical purposes–preliminary findings. Bio-Algorithms Med-Syst. 2017, 13, 37–42. [Google Scholar] [CrossRef]
- Rojek, I.; Mikołajewski, D.; Kotlarz, P.; Macko, M.; Kopowski, J. Intelligent system supporting technological process planning for machining and 3D printing. Bull. Pol. Acad. Sci. Tech. Sci. 2021, 69, e136722. [Google Scholar]
- Mikołajewska, E.; Mikołajewski, D. Integrated IT environment for people with disabilities: A new concept. Cent. Eur. J. Med. 2014, 9, 177–182. [Google Scholar] [CrossRef]
- Pelly, M.; Fatehi, F.; Liew, D.; Verdejo-Garcia, A. Artificial intelligence for secondary prevention of myocardial infarction: A qualitative study of patient and health professional perspectives. Int. J. Med. Inform. 2023, 173, 105041. [Google Scholar] [CrossRef]
- Choi, A.; Kim, M.J.; Sung, J.M.; Kim, S.; Lee, J.; Hyun, H.; Kim, H.C.; Kim, J.H.; Chang, H.J.; Connected Network for EMS Comprehensive Technical Support Using Artificial Intelligence Investigators. Development of Prediction Models for Acute Myocardial Infarction at Prehospital Stage with Machine Learning Based on a Nationwide Database. J. Cardiovasc. Dev. Dis. 2022, 9, 430. [Google Scholar] [CrossRef] [PubMed]
- Schulte, C.; Singh, B.; Theofilatos, K.; Sörensen, N.A.; Lehmacher, J.; Hartikainen, T.; Haller, P.M.; Westermann, D.; Zeller, T.; Blankenberg, S.; et al. Serial measurements of protein and microRNA biomarkers to specify myocardial infarction subtypes. J.Mol. Cell Cardiol. Plus 2022, 1, 100014. [Google Scholar] [CrossRef] [PubMed]
- Tern, P.J.W.; Vaswani, A.; Yeo, K.K. Identifying and Solving Gaps in Pre- and In-Hospital Acute Myocardial Infarction Care in Asia-Pacific Countries. Korean Circ. J. 2023, 53, 594–605. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H. Data integration using information and communication technology for emergency medical services and systems. Clin. Exp. Emerg. Med. 2023, 10, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Wingrove, G.; McGinnis, K. Integration of Tehnology Data is nice but must be turned into useful information. EMS World 2016, (Suppl. 14), 2158–7833. [Google Scholar]
- Ważny, M.; Wójcik, G.M. Shifting spatial attention–numerical model of Posner experiment. Neurocomputing 2014, 135, 139–144. [Google Scholar] [CrossRef]
- Kawala-Janik, A.; Bauer, W.; Żołubak, M.; Baranowski, J. Early-stage pilot study on using fractional-order calculus-based filtering for the purpose of analysis of electroencephalography signals. Stud. Log. Gramm. Rhetor. 2016, 47, 103–111. [Google Scholar] [CrossRef]
- Gajos-Balińska, A.; Wójcik, G.M.; Stpiczyński, P. Hybrid implementation of the fastICA algorithm for high-density EEG using the capabilities of the Intel architecture and CUDA programming. Comput. Sci. 2024, 24. [Google Scholar] [CrossRef]
- Wojcik, G.M.; Masiak, J.; Kawiak, A.; Kwasniewicz, L.; Schneider, P.; Polak, N.; Gajos-Balinska, A. Mapping the Human Brain in Frequency Band Analysis ofBrain Cortex Electroencephalographic Activity for Selected Psychiatric Disorders. Front. Neuroinformatics 2018, 12, 73. [Google Scholar] [CrossRef]
- Wojcik, G.M.; Masiak, J.; Kawiak, A.; Kwasniewicz, L.; Schneider, P.; Postepski, F.; Gajos-Balinska, A. Analysis of Decision-Making Process Using Methods ofQuantitative Electroencephalography and Machine Learning Tools. Front. Neuroinformatics 2019, 13, 73. [Google Scholar] [CrossRef]
- Wojcik, G.M.; Masiak, J.; Kawiak, A.; Schneider, P.; Kwasniewicz, L.; Polak, N.; Gajos-Balinska, A. New Protocol for Quantitative Analysis of Brain Cortex Electroencephalographic Activity in Patients with Psychiatric Disorders. Front. Neuroinformatics 2018, 12, 27. [Google Scholar] [CrossRef] [PubMed]
- AHA23 Conference. Available online: https://professional.heart.org/en/meetings/scientific-sessions (accessed on 25 December 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Row No. | Patient ID | Age | Sex | Cholesterol | Blood Pressure | Heart Rate | Diabetes | Family History | --- | Country |
|---|---|---|---|---|---|---|---|---|---|---|
| 0 | BMW7812 | 67 | Male | 208 | 158/88 | 72 | 0 | 0 | … | Argentina |
| 1 | CZE1114 | 21 | Male | 389 | 165/93 | 98 | 1 | 1 | … | Canada |
| 2 | BNI9906 | 21 | Female | 324 | 174/99 | 72 | 1 | 0 | … | France |
| 3 | JUN3497 | 84 | Male | 383 | 163/100 | 73 | 1 | 1 | … | Canada |
| 4 | GFO8847 | 66 | Male | 318 | 91/88 | 93 | 1 | 1 | … | Thailand |
| … | … | … | … | … | … | … | … | … | … | … |
| 8759 | QSV6764 | 28 | Female | 120 | 157/102 | 73 | 1 | 0 | … | Canada |
| 8760 | XKA5925 | 47 | Male | 250 | 161.75 | 105 | 0 | 1 | … | Brazil |
| 8761 | EPE6801 | 36 | Male | 178 | 119/67 | 60 | 1 | 0 | … | Brazil |
| 8762 | ZWN9666 | 25 | Female | 356 | 138/67 | 75 | 1 | 1 | … | United Kingdom |
| Score No. | Score Value |
|---|---|
| 1. | 1.0 |
| 2. | 0.7718972895863053 |
| 3. | 0.7679029957203994 |
| 4. | 0.7168330955777461 |
| 5. | 0.7125534950071327 |
| 6. | 0.6905848787446505 |
| 7. | 0.6894436519258202 |
| 8. | 0.6894436519258202 |
| 9. | 0.6821683309557774 |
| 10. | 0.6800285306704708 |
| 11. | 0.6704707560627675 |
| 12. | 0.6740370898716119 |
| 13. | 0.6667617689015692 |
| 14. | 0.6671897289586305 |
| 15. | 0.660342368045649 |
| 16. | 0.6616262482168331 |
| 17. | 0.6601997146932953 |
| 18. | 0.6627674750356634 |
| 19. | 0.6590584878744651 |
| 20. | 0.661055634807418 |
| 21. | 0.6556348074179743 |
| Score No. | Score Value |
|---|---|
| 1. | 0.5447803764974329 |
| 2. | 0.6001140901312036 |
| 3. | 0.5561893896177981 |
| 4. | 0.6052481460353679 |
| 5. | 0.5681688533941814 |
| 6. | 0.6023958927552767 |
| 7. | 0.5778665145464917 |
| 8. | 0.602966343411295 |
| 9. | 0.5915573302909298 |
| 10. | 0.6138049058756417 |
| 11. | 0.5938391329150029 |
| 12. | 0.6195094124358242 |
| 13. | 0.6023958927552767 |
| 14. | 0.618938961779806 |
| 15. | 0.6086708499714775 |
| 16. | 0.6240730176839704 |
| 17. | 0.6103822019395322 |
| 18. | 0.6286366229321164 |
| 19. | 0.6149458071876782 |
| 20. | 0.6280661722760981 |
| Model | Accuracy | Balanced Accuracy | ROC AUC | F1 Score | Time Taken |
|---|---|---|---|---|---|
| ExtraTreeClassifier | 0.55 | 0.51 | 0.51 | 0.55 | 0.04 |
| LabelSpreading | 0.56 | 0.51 | 0.51 | 0.55 | 6.00 |
| LabelProppagation | 0.55 | 0.51 | 0.51 | 0.55 | 5.07 |
| XGBClassifier | 0.59 | 0.51 | 0.51 | 0.56 | 0.50 |
| BaggingClassifier | 0.61 | 0.51 | 0.51 | 0.55 | 1.43 |
| NuSVC | 0.57 | 0.50 | 0.50 | 0.55 | 9.16 |
| SGDClassifier | 0.64 | 0.50 | 0.50 | 0.51 | 0.21 |
| RandomForestClassifier | 0.64 | 0.50 | 0.50 | 0.51 | 3.67 |
| DecisionTreeClassifier | 0.54 | 0.50 | 0.50 | 0.54 | 0.28 |
| RidgeClassifier | 0.64 | 0.50 | 0.50 | 0.50 | 0.19 |
| Ridge ClassifierCV | 0.64 | 0.50 | 0.50 | 0.50 | 0.11 |
| LogisticRegression | 0.64 | 0.50 | 0.50 | 0.50 | 0.06 |
| LinearSVC | 0.64 | 0.50 | 0.50 | 0.50 | 1.22 |
| LinearDiscriminantAnalysis | 0.64 | 0.50 | 0.50 | 0.50 | 0.42 |
| GaussianNB | 0.64 | 0.50 | 0.50 | 0.50 | 0.05 |
| DummyClassifier | 0.64 | 0.50 | 0.50 | 0.50 | 0.04 |
| CalibratedClassifierCV | 0.64 | 0.50 | 0.50 | 0.50 | 4.39 |
| BernoulliNB | 0.64 | 0.50 | 0.50 | 0.50 | 0.12 |
| SVC | 0.64 | 0.50 | 0.50 | 0.50 | 6.47 |
| QuadraticDiscriminantAnalysis | 0.62 | 0.50 | 0.50 | 0.53 | 0.09 |
| LGBMClassifier | 0.62 | 0.50 | 0.50 | 0.53 | 0.56 |
| AdaBoostClassifier | 0.64 | 0.50 | 0.50 | 0.51 | 1.31 |
| ExtraTreesClassifier | 0.63 | 0.49 | 0.49 | 0.51 | 1.52 |
| KNeighborsClassifier | 0.56 | 0.49 | 0.49 | 0.54 | 0.39 |
| Perceptron | 0.52 | 0.49 | 0.49 | 0.52 | 0.05 |
| PassiveAggressiveClassifier | 0.47 | 0.48 | 0.48 | 0.47 | 0.07 |
| NearestCentroid | 0,48 | 0.47 | 0.47 | 0.49 | 0.05 |
| Precision | Recall | F1-Score | Support | |
|---|---|---|---|---|
| 0 | 0.64 | 1.00 | 0.78 | 1126 |
| 1 | 0.00 | 0.00 | 0.00 | 628 |
| Accuracy | - | - | 0.64 | 1753 |
| Macro average | 0.32 | 0.50 | 0.39 | 1753 |
| Weighted average | 0.41 | 0.64 | 0.50 | 1753 |
| Limitation | Results |
|---|---|
| Accuracy, data quality, and bias | Biased or incomplete training data may make the model’s predictions inaccurate or may perpetuate existing biases in healthcare. |
| AI models trained on specific datasets may have difficulty generalizing different populations, as genetics, lifestyles, and socio-economic conditions can vary widely. | |
| The dynamic nature of health data means that health conditions and risk factors change over time, which requires the capturing of their dynamic changes (including, for example, changes in the norm). | |
| Limited predictive horizon | AI models trained on historical data may have limited predictive capabilities—accurately predicting future events can be challenging. |
| Societal changes | Predictive models may not take into account changes in patient behavior (medication adherence, lifestyle modifications, etc.), which can significantly affect the actual risk of myocardial infarction, but may be difficult to predict accurately. |
| Direction | Detailed Tasks |
|---|---|
| Data standardization and integration | Combining different datasets (combining electronic medical records, genetic data, lifestyle information, etc.) to improve the accuracy and reliability of AI models. |
| AI models should be easy to implement, integrate with already existing healthcare data flows, and support strategies to facilitate the practical implementation of AI-based heart disease risk prediction tools in healthcare settings. | |
| The widespread use of wearable technology and remote monitoring can enable real-time risk assessment and early intervention. | |
| Validation of AI models on diverse and external datasets to ensure generalizability to other populations. | |
| Explainability/interpretability | Models that make accurate predictions and provide clear explanations of their decisions will help to gain the trust of medical professionals and the acceptance of public. |
| Refining models to provide more personalized predictions, taking into account factors such as genetics, environmental influences and socio-economic factors. | |
| Possible long-term impact | In the long term, the outcomes of people identified by AI models as being at high risk of cardiovascular disease adhering to recommendations and undergoing improvements in health may change the face of preventive medicine and healthcare in general. |
| Ethical and legal considerations | Data privacy, cybersecurity, and the responsible and safe use of patient data in AI models. |
| Liability for an erroneous prediction made based on AI inference. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojek, I.; Kotlarz, P.; Kozielski, M.; Jagodziński, M.; Królikowski, Z. Development of AI-Based Prediction of Heart Attack Risk as an Element of Preventive Medicine. Electronics 2024, 13, 272. https://doi.org/10.3390/electronics13020272
Rojek I, Kotlarz P, Kozielski M, Jagodziński M, Królikowski Z. Development of AI-Based Prediction of Heart Attack Risk as an Element of Preventive Medicine. Electronics. 2024; 13(2):272. https://doi.org/10.3390/electronics13020272
Chicago/Turabian StyleRojek, Izabela, Piotr Kotlarz, Mirosław Kozielski, Mieczysław Jagodziński, and Zbyszko Królikowski. 2024. "Development of AI-Based Prediction of Heart Attack Risk as an Element of Preventive Medicine" Electronics 13, no. 2: 272. https://doi.org/10.3390/electronics13020272
APA StyleRojek, I., Kotlarz, P., Kozielski, M., Jagodziński, M., & Królikowski, Z. (2024). Development of AI-Based Prediction of Heart Attack Risk as an Element of Preventive Medicine. Electronics, 13(2), 272. https://doi.org/10.3390/electronics13020272