
IoMT with Deep CNN: AI-Based Intelligent Support System for Pandemic Diseases

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Related Work
3. Proposed System
- (1)
- Leverage the culmination of cutting-edge technologies to address the vital problems in the health care sector for the common public.
- (2)
- Design of intelligent data acquisition system.
- (3)
- Acquire heterogeneous raw data (CT images, RT-PCR results, pulse oxygen rate, X-ray imaging) from various sources, either directly and indirectly, and integrate them contextually to achieve a unified formatted data.
- (4)
- Design and develop a cloud platform for unified formatted data.
- (5)
- Design a system for multi-diseases classification (COVID-19/pneumonia/viral infections).
- (6)
- Develop a model to measure severity level of the lungs to provide suitable treatment to save their lives.
- (7)
- Present test summary report textually. It can be accessed by a user-friendly GUI.
- (a)
- Intelligent data acquisition system;
- (b)
- Cloud platform for storing the data;
- (c)
- Data pre-processing;
- (d)
- Synthetic data generation;
- (e)
- Proposed AI-based system for disease classification.
3.1. Intelligent Data Acquisition System
- (1)
- Case 1: RT-PCR test results are negative and pulse oxygen rate is not less than the threshold value (90%), then it generated the test report as “Non-COVID-Viral Infection”.
- (2)
- Case 2: If RT-PCR is negative and pulse oxygen rate is less than the threshold value (90%), it gives a suggestion to upload the CT images/X-ray images based on the available medical infrastructure.
- (3)
- Case 3: If RT-PCR is positive, it gives a suggestion to take CT scan or X-ray for analyzing intensity level of the diseases. The designed user interface is connected with Google Cloud for detailed medical analysis.
3.2. Cloud Platform
3.3. Data Preprocessing
3.4. Synthetic Data Generation
3.5. Proposed AI-Based System for Disease Classification
4. Experimentation for SARs Virus Classification
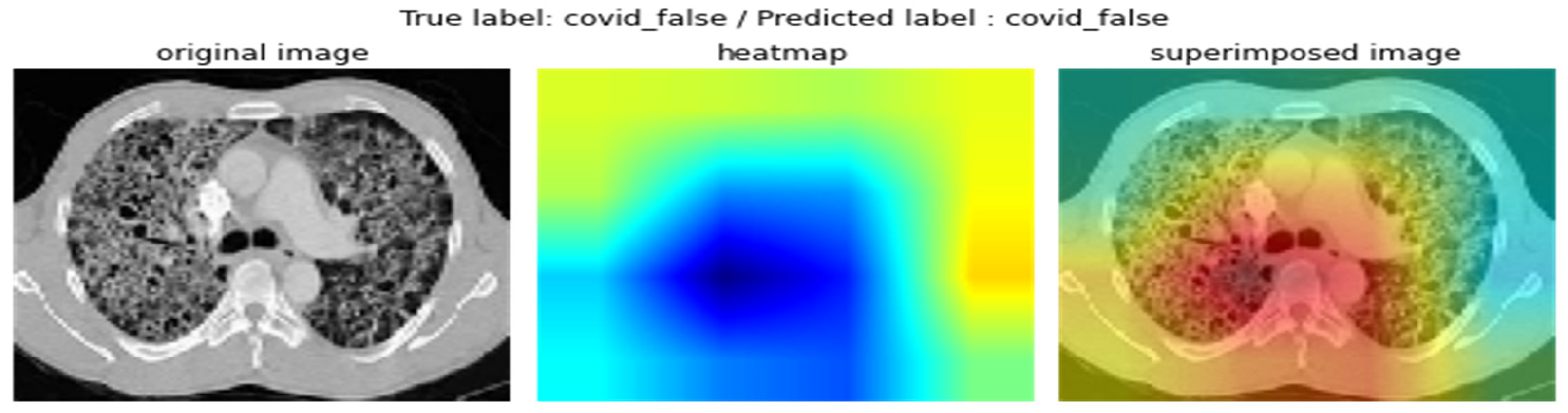
4.1. Experimental Results on CT Images
4.2. Experimental Results on X-ray Images
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Adhikari, S.P.; Meng, S.; Wu, Y.-J.; Mao, Y.-P.; Ye, R.-X.; Wang, Q.-Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, Causes, Clinical Manifestation and Diagnosis, Prevention and Control of Coronavirus Disease (COVID-19) during the Early Outbreak Period: A Scoping Review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef]
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.-W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.-Y.; Poon, R.W.-S.; et al. A Familial Cluster of Pneumonia Associated with the 2019 Novel Coronavirus Indicating Person-to-Person Transmission: A Study of a Family Cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Calimeri, F.; Cauteruccio, F.; Cinelli, L.; Marzullo, A.; Stamile, C.; Terracina, G.; Durand-Dubief, F.; Sappey-Marinier, D. A Logic-Based Framework Leveraging Neural Networks for Studying the Evolution of Neurological Disorders. Theory Pract. Log. Program. 2021, 21, 80–124. [Google Scholar] [CrossRef]
- Cong, I.; Choi, S.; Lukin, M.D. Quantum Convolutional Neural Networks. Nat. Phys. 2019, 15, 1273–1278. [Google Scholar] [CrossRef]
- Xie, Y.-M.; Lu, Y.-S.; Weng, C.-X.; Cao, X.-Y.; Jia, Z.-Y.; Bao, Y.; Wang, Y.; Fu, Y.; Yin, H.-L.; Chen, Z.-B. Breaking the Rate-Loss Bound of Quantum Key Distribution with Asynchronous Two-Photon Interference. PRX Quantum 2022, 3, 020315. [Google Scholar] [CrossRef]
- Zhou, M.-G.; Cao, X.-Y.; Lu, Y.-S.; Wang, Y.; Bao, Y.; Jia, Z.-Y.; Fu, Y.; Yin, H.-L.; Chen, Z.-B. Experimental Quantum Advantage with Quantum Coupon Collector. Research 2022, 2022, 1–11. [Google Scholar] [CrossRef]
- Sheng, Y.-B.; Zhou, L.; Long, G.-L. One-Step Quantum Secure Direct Communication. Sci. Bull. 2022, 67, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, B.; Bhattacharyya, S.; Pal, K. IoT-Based Applications in Healthcare Devices. J. Healthc. Eng. 2021, 2021, 1–18. [Google Scholar] [CrossRef]
- Ramesh, A.; Kambhampati, C.; Monson, J.; Drew, P. Artificial Intelligence in Medicine. Ann. R. Coll. Surg. Engl. 2004, 86, 334–338. [Google Scholar] [CrossRef]
- Digvijay, H.; Yadnyesh, P.; Parineeta, S. Hospital Management System. Int. J. Res. Eng. Appl. Manag. (IJREAM) 2016, 1, 1–4. [Google Scholar]
- Manne, R.; Kantheti, S.C. Application of Artificial Intelligence in Healthcare: Chances and Challenges. Curr. J. Appl. Sci. Technol. 2021, 40, 78–89. [Google Scholar] [CrossRef]
- National University of Sciences and Technology, Islamabad, Pakistan; Joyia, G.J.; Liaqat, R.M.; Farooq, A.; Rehman, S. Internet of Medical Things (IOMT): Applications, Benefits and Future Challenges in Healthcare Domain. J. Commun. 2017, 12, 240–247. [Google Scholar] [CrossRef]
- Hlatshwako, T.G.; Shah, S.J.; Kosana, P.; Adebayo, E.; Hendriks, J.; Larsson, E.C.; Hensel, D.J.; Erausquin, J.T.; Marks, M.; Michielsen, K.; et al. Online Health Survey Research during COVID-19. Lancet Digit. Health 2021, 3, 76–77. [Google Scholar] [CrossRef]
- Rismanbaf, A. Potential Treatments for COVID-19; a Literature Review. Arch. Acad. Emerg. Med. 2020, 8, 29. [Google Scholar] [CrossRef]
- Rahaman, M.M.; Li, C.; Yao, Y.; Kulwa, F.; Rahman, M.A.; Wang, Q.; Qi, S.; Kong, F.; Zhu, X.; Zhao, X. Identification of COVID-19 Samples from Chest X-Ray Images Using Deep Learning: A Comparison of Transfer Learning Approaches. J. X-Ray Sci. Technol. 2020, 28, 821–839. [Google Scholar] [CrossRef] [PubMed]
- Taresh, M.M.; Zhu, N.; Ali, T.A.A.; Hameed, A.S.; Mutar, M.L. Transfer Learning to Detect COVID-19 Automatically from X-Ray Images Using Convolutional Neural Networks. Int. J. Biomed. Imaging 2021, 2021, 1–9. [Google Scholar] [CrossRef]
- Perumal, V.; Narayanan, V.; Rajasekar, S.J.S. Prediction of COVID-19 with Computed Tomography Images Using Hybrid Learning Techniques. Dis. Mrk. 2021, 2021, 1–15. [Google Scholar] [CrossRef]
- Li, X.; Tan, W.; Liu, P.; Zhou, Q.; Yang, J. Classification of COVID-19 Chest CT Images Based on Ensemble Deep Learning. J. Healthc. Eng. 2021, 2021, 1–7. [Google Scholar] [CrossRef]
- Toor, A.A.; Usman, M.; Younas, F.; Fong, A.C.M.; Khan, S.A.; Fong, S. Mining Massive E-Health Data Streams for IoMT Enabled Healthcare Systems. Sensors 2020, 20, 2131. [Google Scholar] [CrossRef]
- AlShorman, O.; AlShorman, B.; Al-khassaweneh, M.; Alkahtani, F. A Review of Internet of Medical Things (IoMT)—Based Remote Health Monitoring through Wearable Sensors: A Case Study for Diabetic Patients. Indones. J. Electr. Eng. Comput. Sci. 2020, 20, 414. [Google Scholar] [CrossRef]
- Rodrigues, J.J.P.C.; De Rezende Segundo, D.B.; Junqueira, H.A.; Sabino, M.H.; Prince, R.M.; Al-Muhtadi, J.; De Albuquerque, V.H.C. Enabling Technologies for the Internet of Health Things. IEEE Access 2018, 6, 13129–13141. [Google Scholar] [CrossRef]
- Habibzadeh, H.; Dinesh, K.; RajabiShishvan, O.; Boggio-Dandry, A.; Sharma, G.; Soyata, T. A Survey of Healthcare Internet of Things (HIoT): A Clinical Perspective. IEEE Internet Things J. 2020, 7, 53–71. [Google Scholar] [CrossRef] [PubMed]
- Cao, S.; Lin, X.; Hu, K.; Wang, L.; Li, W.; Wang, M.; Le, Y. Cloud Computing-Based Medical Health Monitoring IoT System Design. Mob. Inf. Syst. 2021, 2021, 1–12. [Google Scholar] [CrossRef]
- Haoyu, L.; Jianxing, L.; Arunkumar, N.; Hussein, A.F.; Jaber, M.M. An IoMT Cloud-Based Real Time Sleep Apnea Detection Scheme by Using the SpO2 Estimation Supported by Heart Rate Variability. Future Gener. Comput. Syst. 2019, 98, 69–77. [Google Scholar] [CrossRef]
- Pratap Singh, R.; Javaid, M.; Haleem, A.; Vaishya, R.; Ali, S. Internet of Medical Things (IoMT) for Orthopaedic in COVID-19 Pandemic: Roles, Challenges, and Applications. J. Clin. Orthop. Trauma 2020, 11, 713–717. [Google Scholar] [CrossRef] [PubMed]
- Ou, T.; Cai, X.; Wang, M.; Guo, F.; Wu, B. A Novel Method of Clinical Nursing under the Medical Internet of Things Technology. J. Healthc. Eng. 2021, 2021, 1–10. [Google Scholar] [CrossRef]
- Ahsan, M.M.; Nazim, R.; Siddique, Z.; Huebner, P. Detection of COVID-19 Patients from CT Scan and Chest X-Ray Data Using Modified MobileNetV2 and LIME. Healthcare 2021, 9, 1099. [Google Scholar] [CrossRef]
- Avola, D.; Bacciu, A.; Cinque, L.; Fagioli, A.; Marini, M.R.; Taiello, R. Study on Transfer Learning Capabilities for Pneumonia Classification in Chest-X-rays Images. Comput. Methods Programs Biomed. 2022, 221, 106833. [Google Scholar] [CrossRef]
- Zhang, Y.; Su, L.; Liu, Z.; Tan, W.; Jiang, Y.; Cheng, C. A Semi-Supervised Learning Approach for COVID-19 Detection from Chest CT Scans. Neurocomputing 2022, 503, 314–324. [Google Scholar] [CrossRef]
- Sun, L.; Mo, Z.; Yan, F.; Xia, L.; Shan, F.; Ding, Z.; Song, B.; Gao, W.; Shao, W.; Shi, F.; et al. Adaptive Feature Selection Guided Deep Forest for COVID-19 Classification with Chest CT. IEEE J. Biomed. Health Inform. 2020, 24, 2798–2805. [Google Scholar] [CrossRef]
- Carvalho, E.D.; Carvalho, E.D.; de Carvalho Filho, A.O.; De Araújo, F.H.D.; Rabêlo, R.D.A.L. Diagnosis of COVID-19 in CT Image Using CNN and XGBoost. In Proceedings of the 2020 IEEE Symposium on Computers and Communications (ISCC), Rennes, France, 7–10 July 2020; IEEE: Rennes, France; pp. 1–6. [Google Scholar]
- Wang, G.; Liu, X.; Li, C.; Xu, Z.; Ruan, J.; Zhu, H.; Meng, T.; Li, K.; Huang, N.; Zhang, S. A Noise-Robust Framework for Automatic Segmentation of COVID-19 Pneumonia Lesions From CT Images. IEEE Trans. Med. Imaging 2020, 39, 2653–2663. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Deng, X.; Fu, Q.; Zhou, Q.; Feng, J.; Ma, H.; Liu, W.; Zheng, C. A Weakly-Supervised Framework for COVID-19 Classification and Lesion Localization from Chest CT. IEEE Trans. Med. Imaging 2020, 39, 2615–2625. [Google Scholar] [CrossRef] [PubMed]
- El-Kenawy, E.-S.M.; Ibrahim, A.; Mirjalili, S.; Eid, M.M.; Hussein, S.E. Novel Feature Selection and Voting Classifier Algorithms for COVID-19 Classification in CT Images. IEEE Access 2020, 8, 179317–179335. [Google Scholar] [CrossRef] [PubMed]
- Sakib, S.; Tazrin, T.; Fouda, M.M.; Fadlullah, Z.M.; Guizani, M. DL-CRC: Deep Learning-Based Chest Radiograph Classification for COVID-19 Detection: A Novel Approach. IEEE Access 2020, 8, 171575–171589. [Google Scholar] [CrossRef]
- Rajaraman, S.; Siegelman, J.; Alderson, P.O.; Folio, L.S.; Folio, L.R.; Antani, S.K. Iteratively Pruned Deep Learning Ensembles for COVID-19 Detection in Chest X-rays. IEEE Access 2020, 8, 115041–115050. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.K.; Das, S.K.; Roy, P.; Bandyopadhyay, S. Identifying COVID-19 from Chest CT Images: A Deep Convolutional Neural Networks Based Approach. J. Healthc. Eng. 2020, 2020, 1–7. [Google Scholar] [CrossRef]
- Singh, D.; Kumar, V.; Vaishali; Kaur, M. Classification of COVID-19 Patients from Chest CT Images Using Multi-Objective Differential Evolution–Based Convolutional Neural Networks. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1379–1389. [Google Scholar] [CrossRef]
- Goel, C.; Kumar, A.; Dubey, S.K.; Srivastava, V. Efficient Deep Network Architecture for COVID-19 Detection Using Computed Tomography Images. medRxiv 2020. [Google Scholar] [CrossRef]
- Jain, R.; Gupta, M.; Taneja, S.; Hemanth, D.J. Deep Learning Based Detection and Analysis of COVID-19 on Chest X-ray Images. Appl. Intell. 2021, 51, 1690–1700. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Summary of the Work in the View of IoMT | ||
|---|---|---|
| Title | Techniques Used | Strength |
| IoMT cloud-based real time sleep apnea detection scheme using SpO2 estimation supported by heart rate variability | The sensing unit involved SpO2 for measuring oxygen blood level, and heart rate. The rules are used for analysis. Mobile app is used as actuation unit. | The designed system continuously monitors the oxygen level and heart rate of the person who is having breathing disorder during sleeping time with the help of sensors attached to the human body (wearables) and to alert the people during sleeping time. |
| IoMT for orthopedic in COVID-19 pandemic: roles, challenges, and applications | Cloud-based consultation. | The designed system addresses the problem of orthopedic patients during lockdown period and offers telemedicine services using cloud and internet services. |
| A novel method of clinical nursing under the medical internet of things technology | Sensing unit involves temperature and pulse rate sensors for measuring human vitals. Analysis is performed by medical experts. | The designed system continuously monitors the human body which is communicated to the medical community via internet and cloud technologies. If they find any abnormality, it is notified to the concerned via phone or mobile app. It reduces the treatment cost and burden of the health care takers. |
| Scope for improvements (from the study, it is observed that we can automate anything if we have a device for real time data collection, techniques for analysis, and a medium (user interface, mobile app, etc.) for controlling the event. | ||
| Proposed System | Sensing unit involves UI for data collection, pulse oximeter for oxygen, pulse rate measurement, RT-PCR kit for knowing COVID positivity Analysis involves deep convolution network architectures, such as ResNet-50, ResNet-100, ResNet-101, VGG 16, and VGG 19. After analysis, test summary report and assistance are communicated via designed UI. | Proposed system collects the information via the designed UI. Then, the collected information is analyzed using deep convolution network architectures. We used major voting classifier for getting precise results. It also avoids the classifier bias. After analysis, automatic test summary report is communicated via the same UI. It reduces the summary generation time. It helps to reduce the spreading rate. It also gives better assistance to the needy. |
| Summary of the Work in the View of Image Analysis | ||
|---|---|---|
| Title | Techniques Used | Strength |
| Detection of COVID-19 Patients from CT Scan and Chest X-ray Data Using Modified MobileNetV2 and LIME | Experimented VGG-16, MobileNet V2, Inception ResNet V2, ResNet 50, ResNet101, VGG 19. | The proposed approach used CT and X-ray images for detecting COVID-19. VGG16 obtains 95% accuracy for X-ray images, MobileNetV2 obtains 98.5 for CT images. |
| Study on Transfer Learning Capabilities for Pneumonia Classification in Chest X-ray Images | 12 different pre trained models are tested. Two different chest X-ray image datasets are used. 6330 images are taken for experimentation. | The study was performed for pneumonia classification. DenseNet yields better result. |
| A Semi-Supervised Learning Approach for COVID-19 Detection from Chest CT Scans | MixMatch Rules. | It is focused on reducing the impact of overfitting and enhancement. |
| A Logic-Based Framework Leveraging Neural Networks for Studying the Evolution of Neurological Disorders | Answer Set Programming. | It is designed for learning the evolution of neurological diseases. It makes the use of ANN and ASP for better analysis. |
| Quantum Convolutional Neural Networks. Experimental Quantum Advantage with Quantum Coupon Collector, Breaking the Rate-Loss Bound of Quantum Key Distribution with Asynchronous Two-Photon Interference | CNN and Quantum Computing. | Proposed System combined the features of CNN and quantum computing for better image classification. |
| Diagnosis of COVID-19 in CT Image Using CNN and XGBoost | CNN and XGBoost. 708 CT images considered for experimentation. | The system is designed for diagnosis of COVID-19. CNN is used for feature selection and XGBoost is used for grouping. It achieves 95.07% accuracy. |
| A Noise-Robust Framework for Automatic Segmentation of COVID-19 Pneumonia Lesions from CT Images | 558 CT images are taken for experimentation. Combination of Max pooling and average pooling is used for down sampling. | Advanced COVID-19 pneumonia lesion segmentation network (COPLE-Net) is proposed for extracting pneumonia lesions. |
| Classification of COVID-19 Patients from Chest CT Images Using Multi-Objective Differential Evolution-Based Convolutional Neural Networks | CT images are taken as dataset. Focused on binary classification. CNN, ANN, and ANFIS are experimented for classification. | It is designed for COVID-19 classification. |
| Scope for improvements—from the study, it was observed that numerous AI techniques and convolution neural network architectures are available for better image classification. Some of the researchers took X-ray images, some of them took CT images, and some of them took both for better classification. However, all are support system for medical practitioners. | ||
| Proposed System | Major voting classifier is used for reducing the classifier bias. Outcomes of ResNet 50, ResNet100, ResNet101, VGG 16, and VGG 19 are given as input to the major voting classifier. It selects the majority voted one. Image data generator used for synthetic data generation. | Data analysis is one of the modules used in making the system automated. Pre-trained models are used for image analyses. Totally, 7455 CT images and 8900 X-ray images are considered for experimentation. |
| Dataset Size | Type of the Image | Algorithm Used | Classification Report | |
|---|---|---|---|---|
| 1700 (images collected from public resource) + 7455 (synthetic data) | CT | ResNet 50 | Precision | 78% |
| Recall | 79% | |||
| F1-Score | 82% | |||
| Accuracy | 78% | |||
| 1700 (images collected from public resource) + 7455 (synthetic data) | CT | ResNet 100 | Precision | 92% |
| Recall | 89% | |||
| F1-Score | 93% | |||
| Accuracy | 93% | |||
| 1700 (images collected from public resource) + 7455 (synthetic data) | CT | ResNet 101 | Precision | 97% |
| Recall | 92% | |||
| F1-Score | 96% | |||
| Accuracy | 97% | |||
| 1700 (images collected from public resource) + 7455 (synthetic data) | CT | VGG 16 | Precision | 89% |
| Recall | 86% | |||
| F1-Score | 89% | |||
| Accuracy | 81% | |||
| 1700 (images collected from public resource) + 7455 (synthetic data) public resource) + 7455 (synthetic data) | CT | VGG 19 | Precision | 97% |
| Recall | 90% | |||
| F1-Score | 95% | |||
| Accuracy | 97% | |||
| Dataset Size | Type of the Image | Algorithm Used | Classification Report | |
|---|---|---|---|---|
| 2200 (images collected from public resource) + 8900 (synthetic data) | X-ray | ResNet 50 | Precision | 82% |
| Recall | 81% | |||
| F1-Score | 83% | |||
| Accuracy | 80% | |||
| 2200 (images collected from public resource) + 8900 (synthetic data) | X-ray | ResNet 100 | Precision | 95% |
| Recall | 89% | |||
| F1-Score | 94% | |||
| Accuracy | 95% | |||
| 2200 (images collected from public resource) + 8900 (synthetic data) | X-ray | ResNet 101 | Precision | 98% |
| Recall | 92% | |||
| F1-Score | 96% | |||
| Accuracy | 98% | |||
| 2200 (images collected from public resource) + 8900 (synthetic data) | X-ray | VGG 19 | Precision | 96% |
| Recall | 95% | |||
| F1-Score | 96% | |||
| Accuracy | 95% | |||
| 2200 (images collected from public resource) + 8900 (synthetic data) | X-ray | VGG 16 | Precision | 85% |
| Recall | 81% | |||
| F1-Score | 82% | |||
| Accuracy | 81% | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thandapani, S.; Mahaboob, M.I.; Iwendi, C.; Selvaraj, D.; Dumka, A.; Rashid, M.; Mohan, S. IoMT with Deep CNN: AI-Based Intelligent Support System for Pandemic Diseases. Electronics 2023, 12, 424. https://doi.org/10.3390/electronics12020424
Thandapani S, Mahaboob MI, Iwendi C, Selvaraj D, Dumka A, Rashid M, Mohan S. IoMT with Deep CNN: AI-Based Intelligent Support System for Pandemic Diseases. Electronics. 2023; 12(2):424. https://doi.org/10.3390/electronics12020424
Chicago/Turabian StyleThandapani, Sujithra, Mohamed Iqbal Mahaboob, Celestine Iwendi, Durai Selvaraj, Ankur Dumka, Mamoon Rashid, and Senthilkumar Mohan. 2023. "IoMT with Deep CNN: AI-Based Intelligent Support System for Pandemic Diseases" Electronics 12, no. 2: 424. https://doi.org/10.3390/electronics12020424
APA StyleThandapani, S., Mahaboob, M. I., Iwendi, C., Selvaraj, D., Dumka, A., Rashid, M., & Mohan, S. (2023). IoMT with Deep CNN: AI-Based Intelligent Support System for Pandemic Diseases. Electronics, 12(2), 424. https://doi.org/10.3390/electronics12020424