
A Flexible Turning and Sensing System for Pressure Ulcers Prevention


 and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
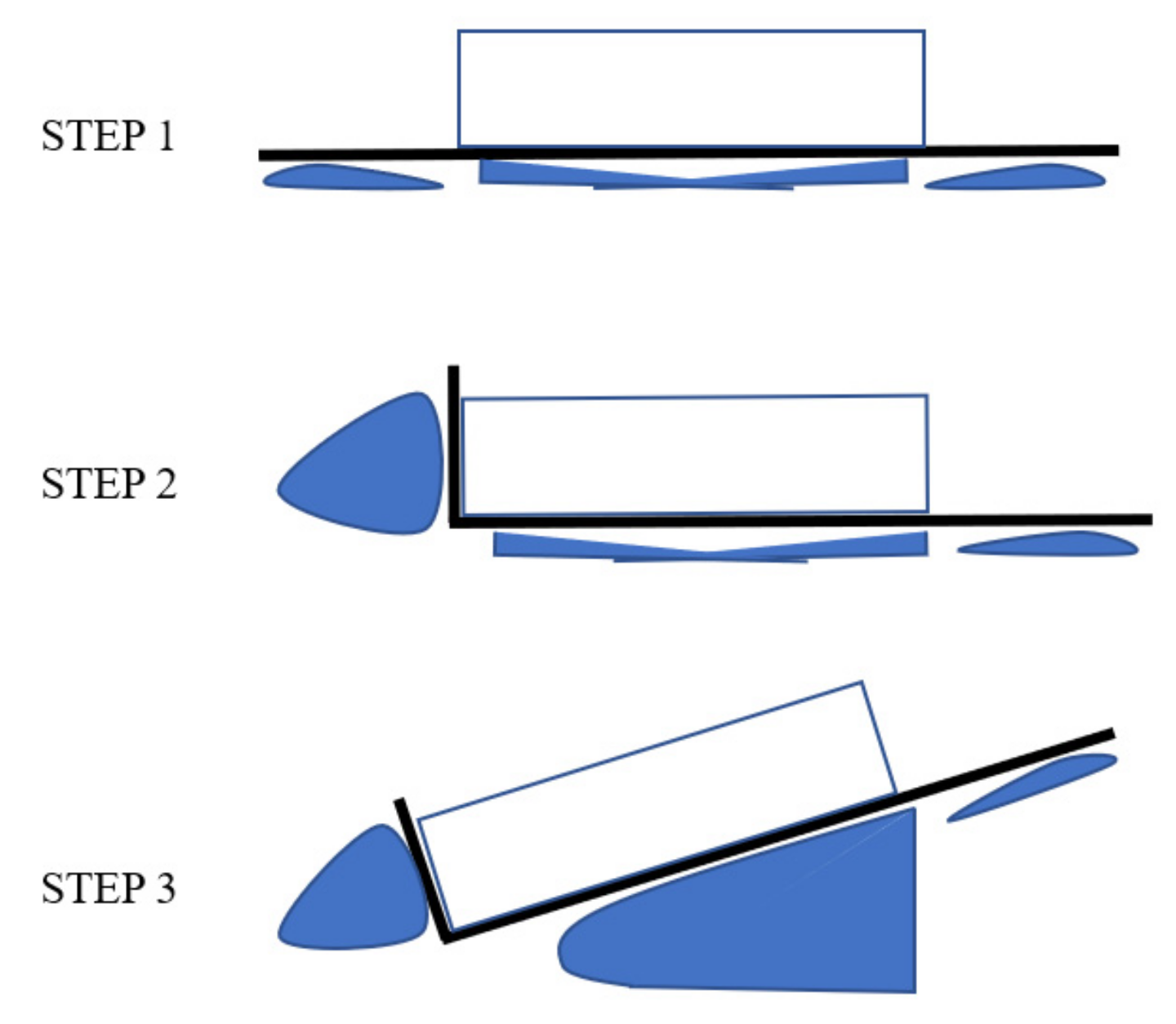
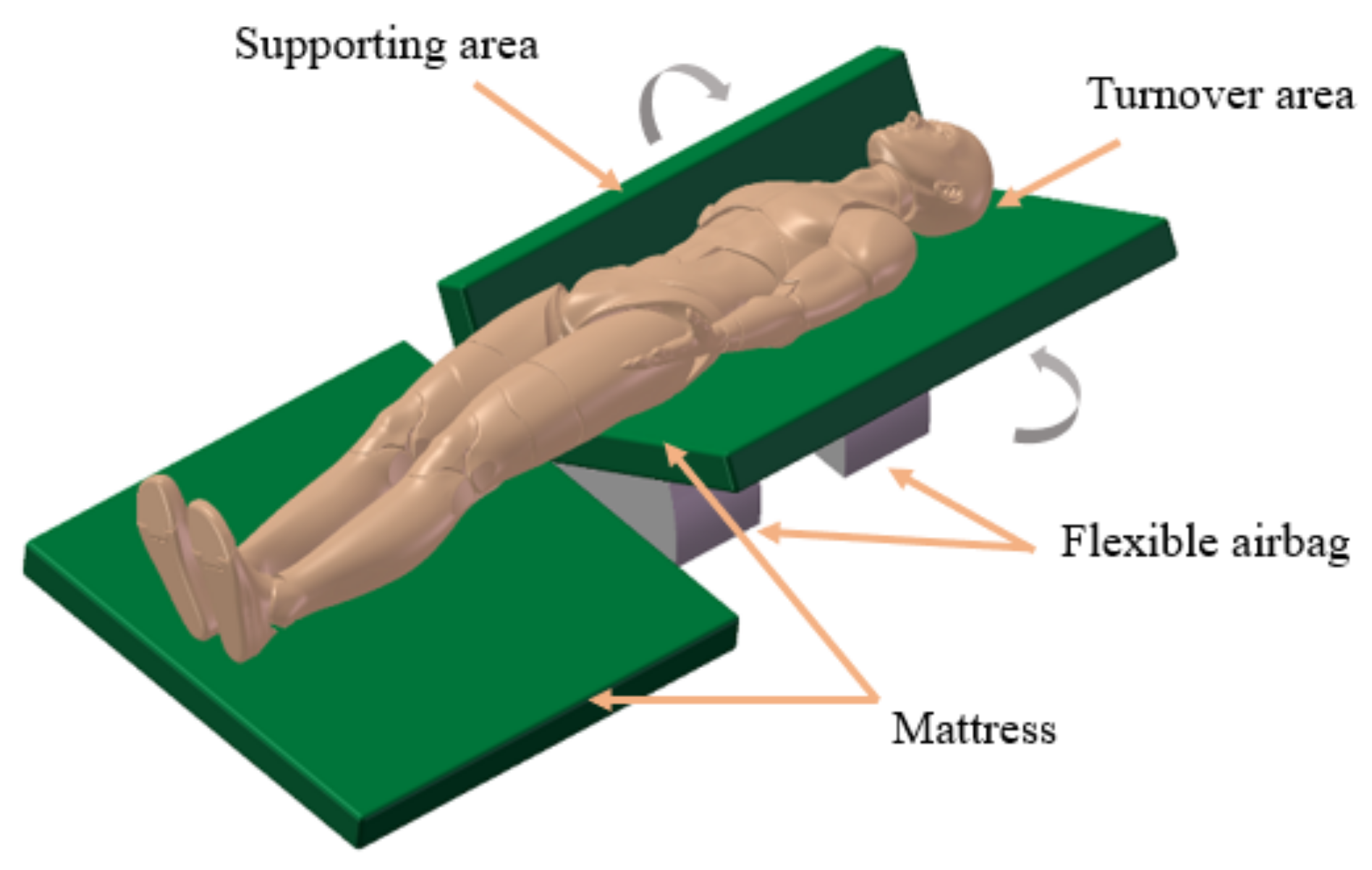
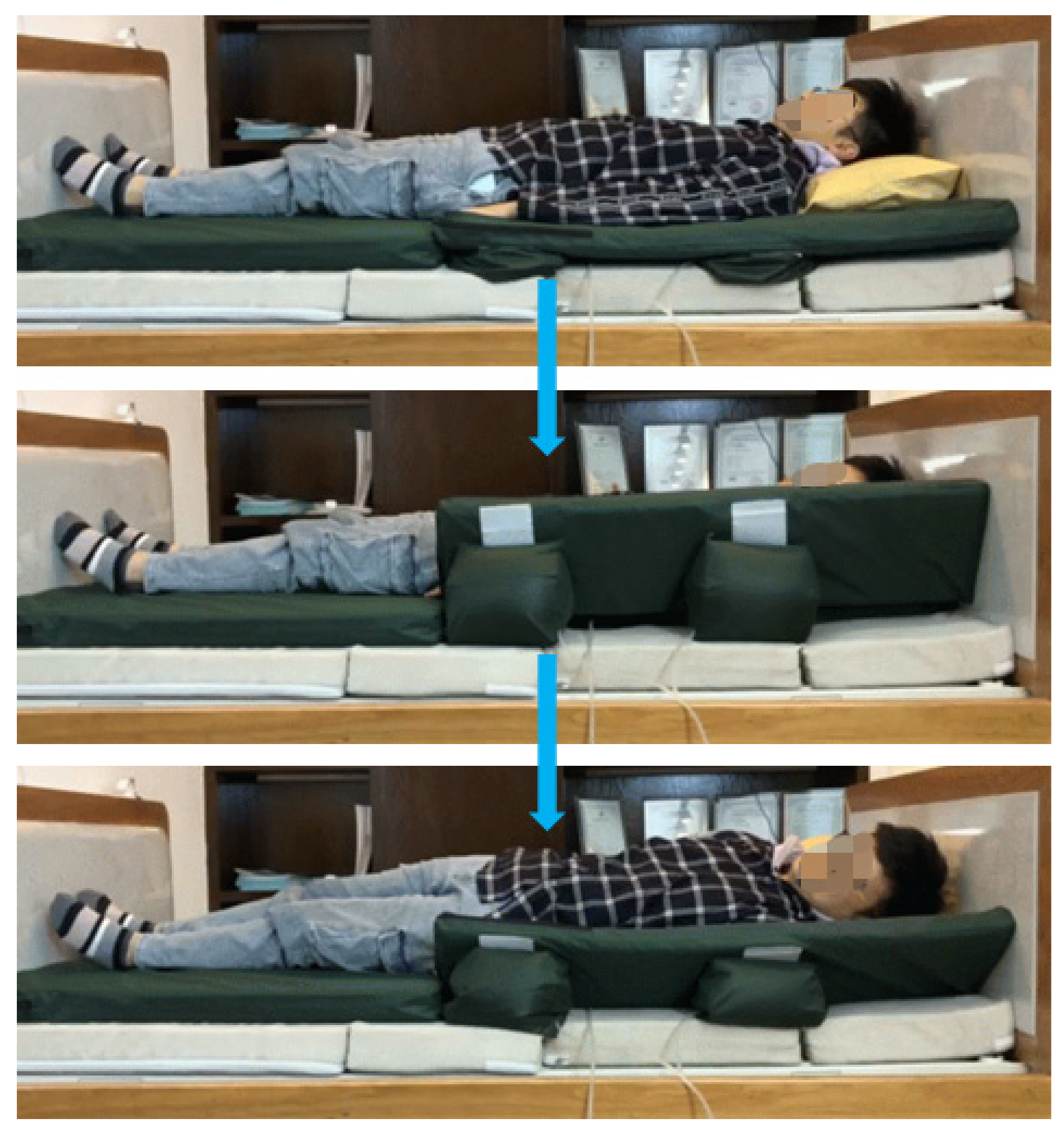
2.1. Turning-Body over Methods
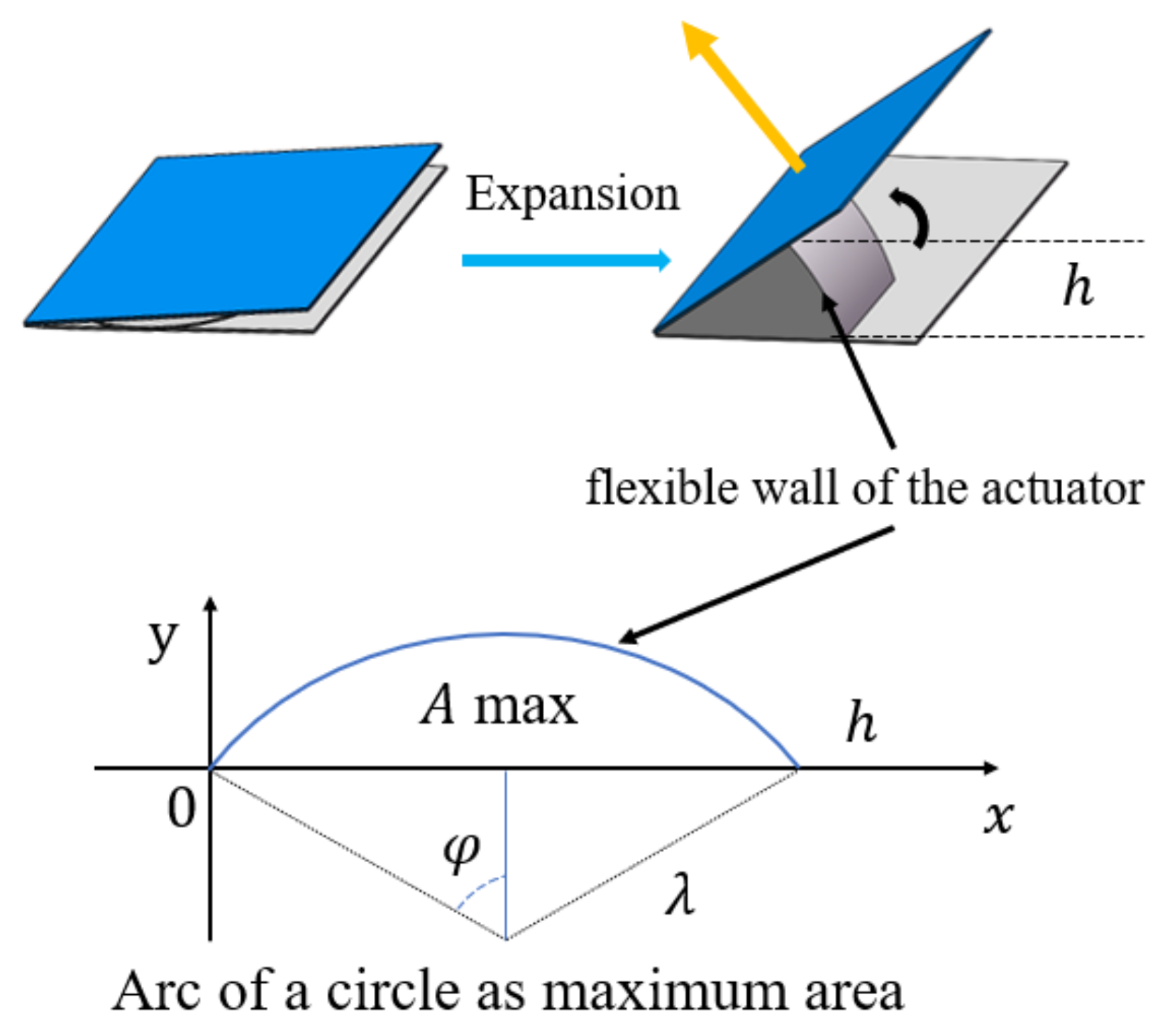
2.2. Mathematical Model of the Soft Actuator
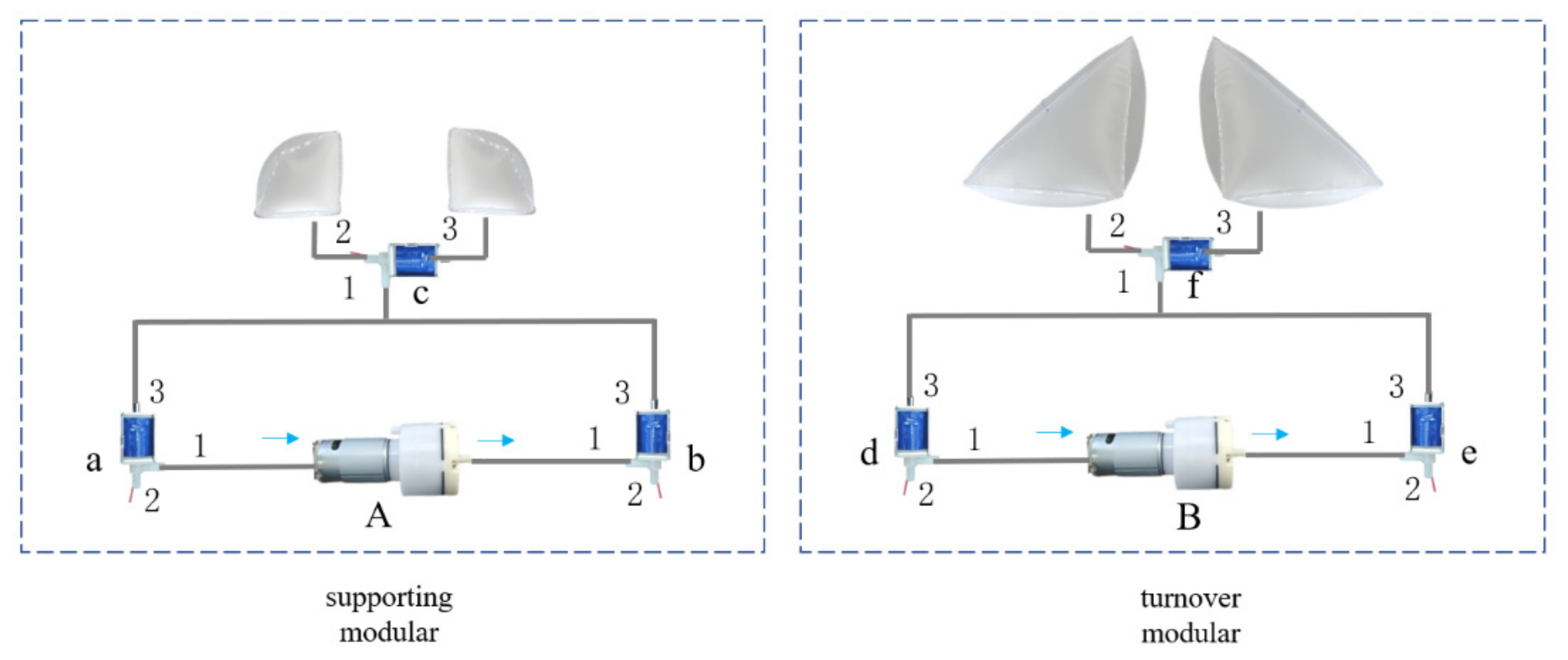
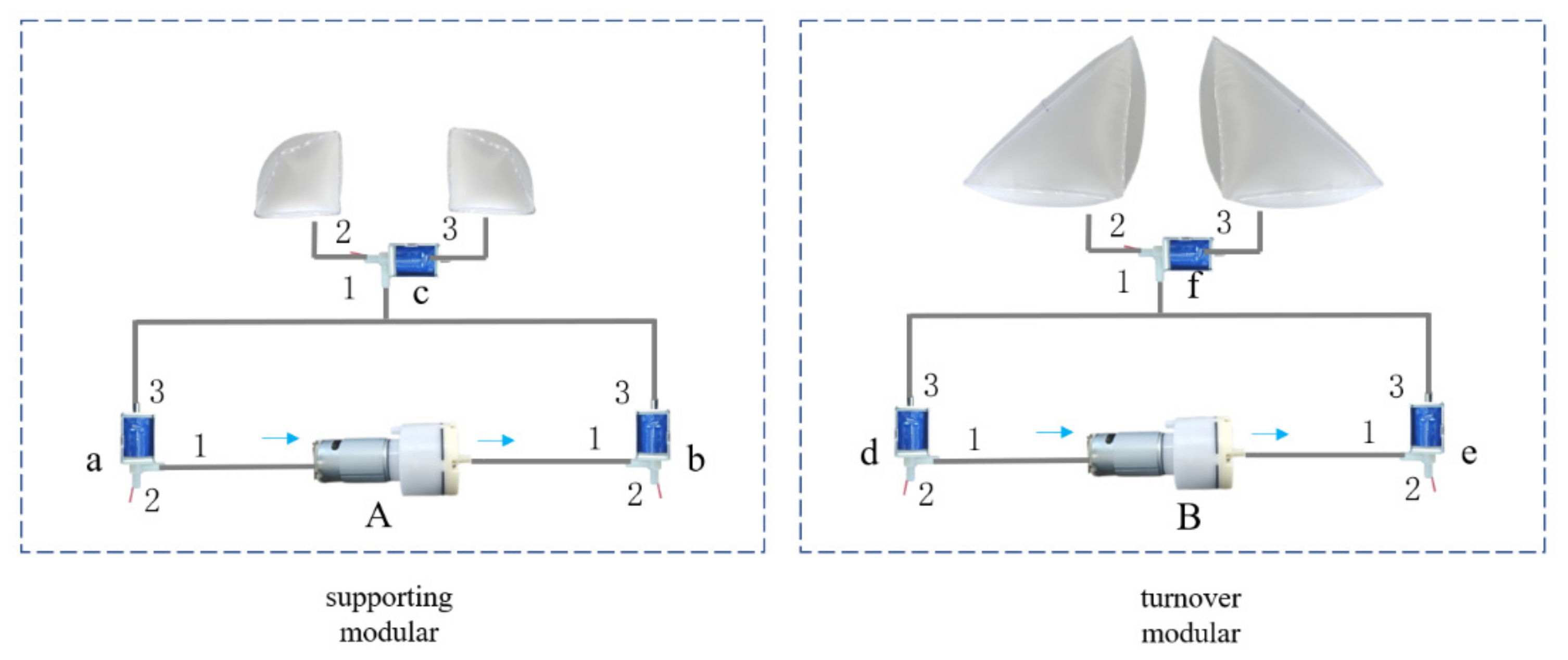
2.3. Pneumatic Turnover Mattress
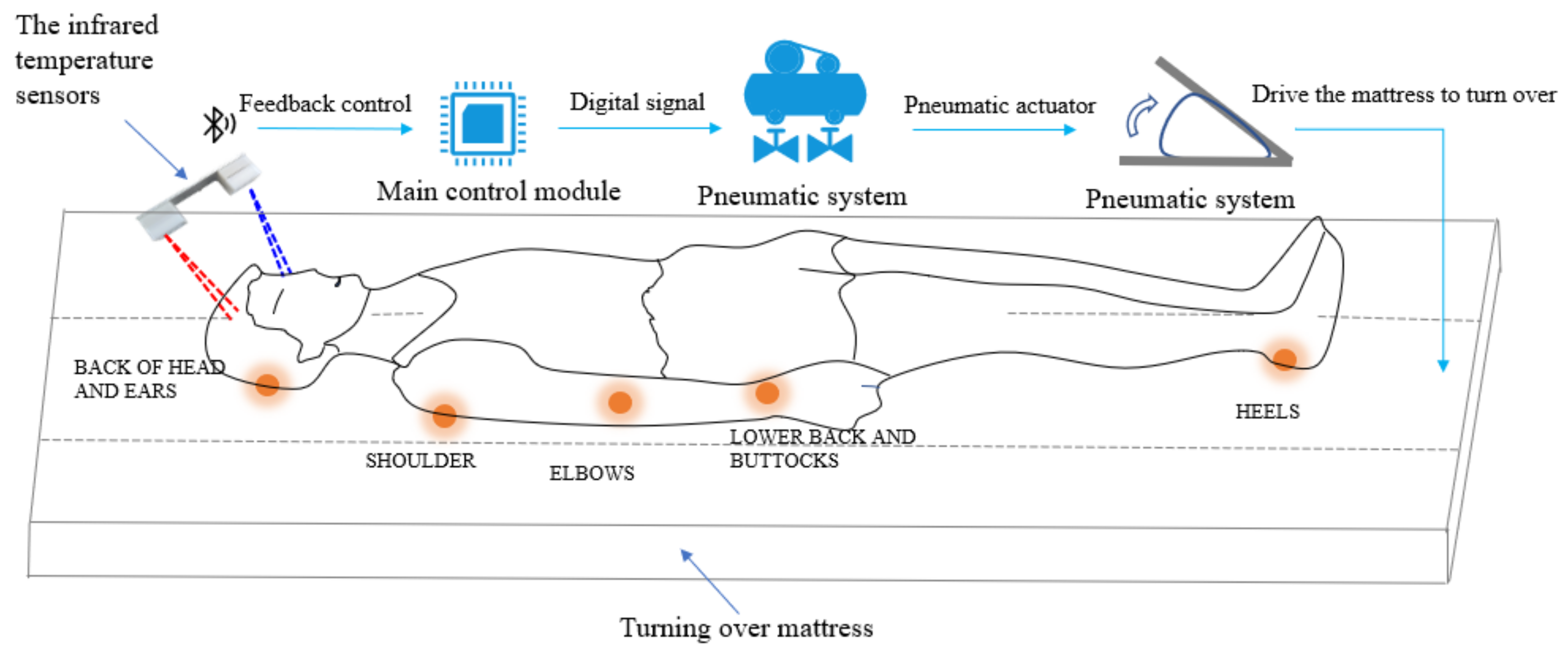
2.4. Design of Control System
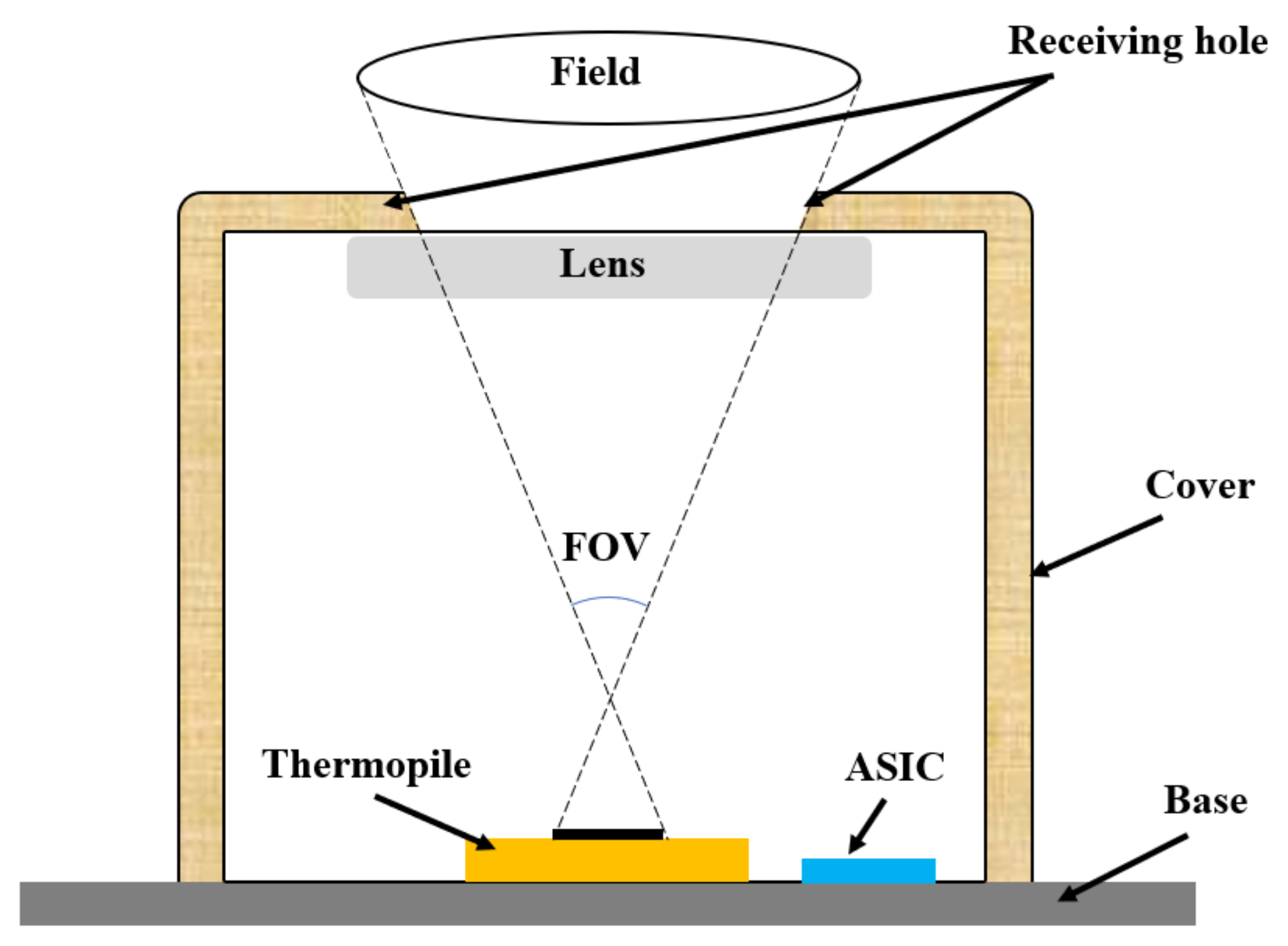
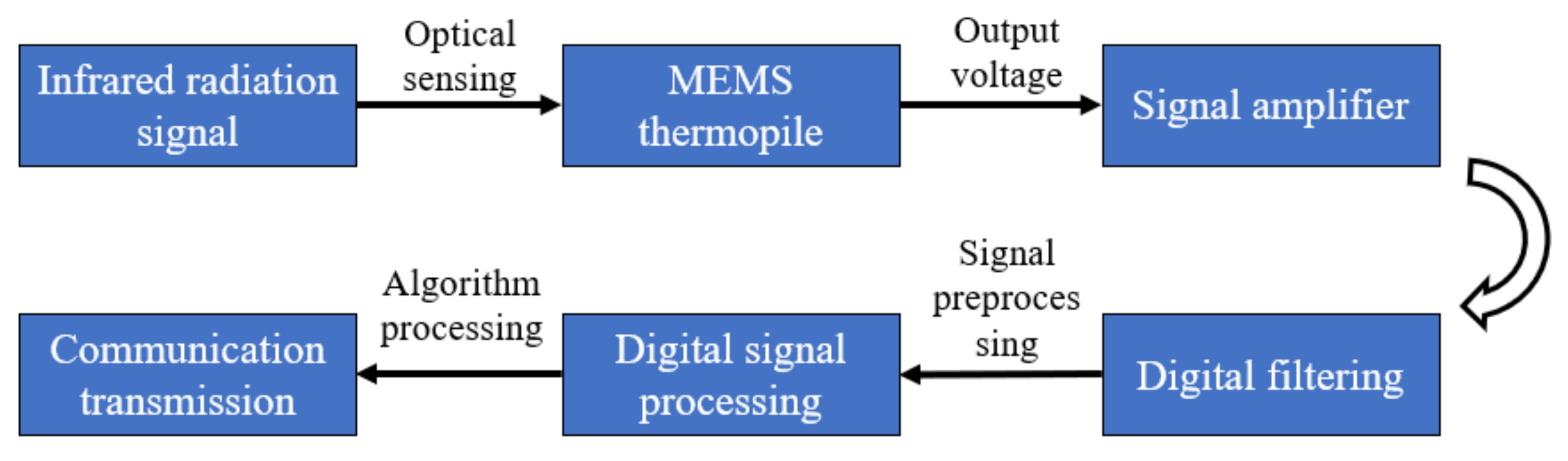
2.5. Design of Temperature Monitoring System
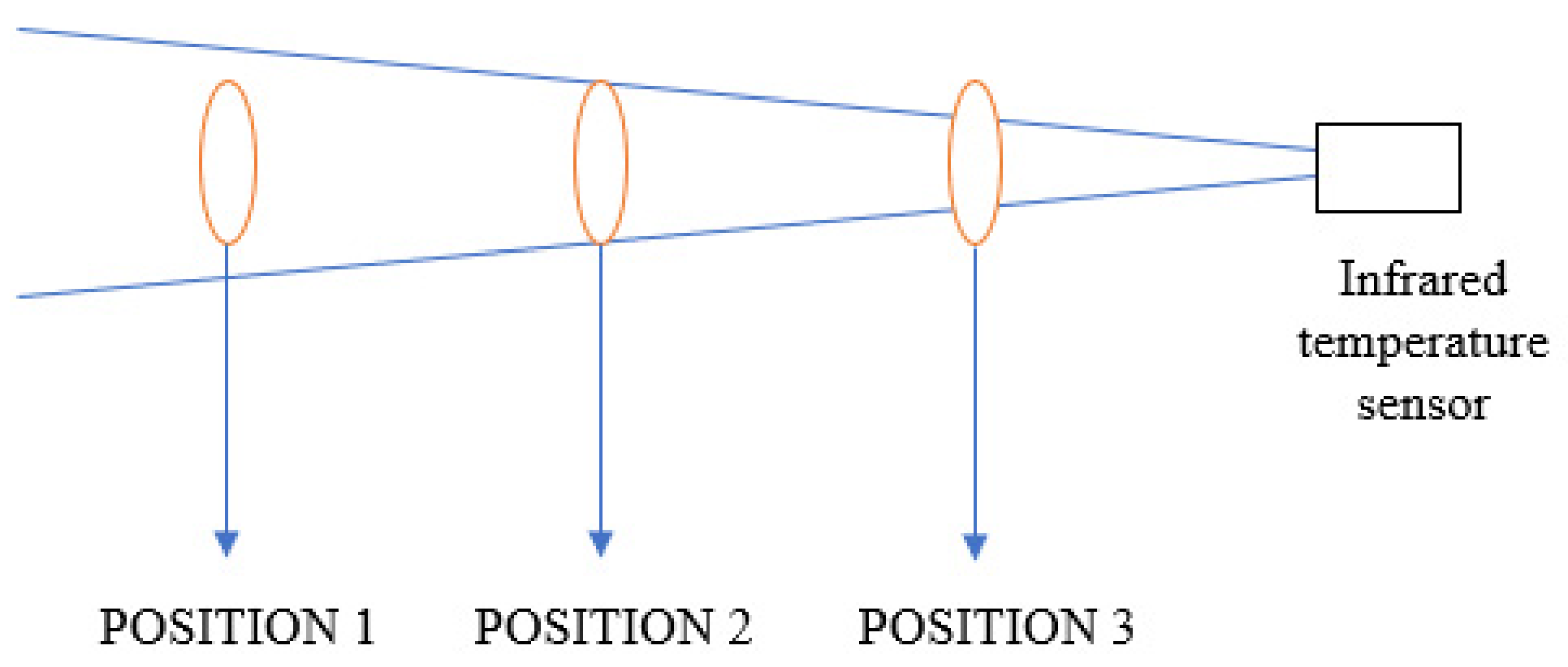
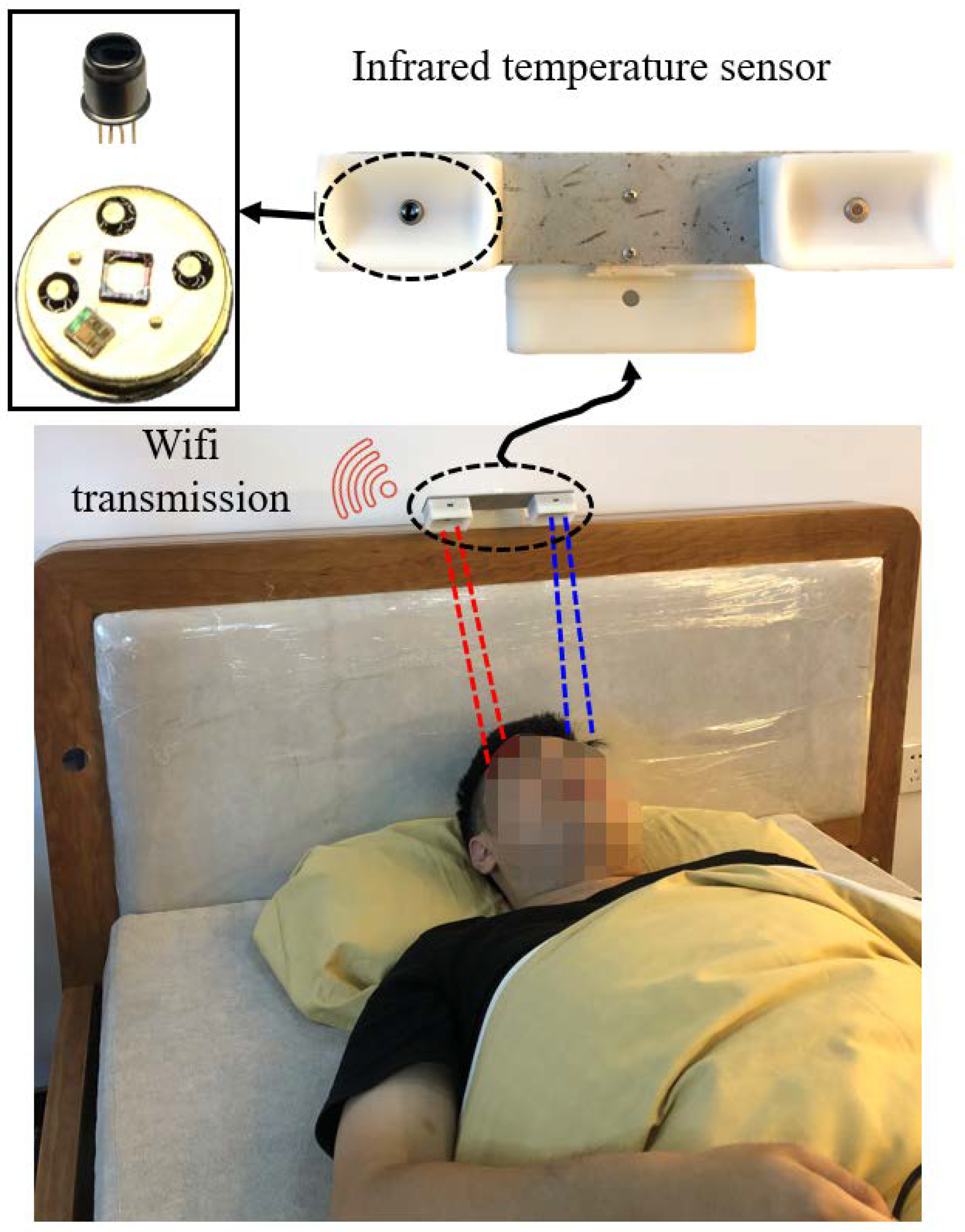
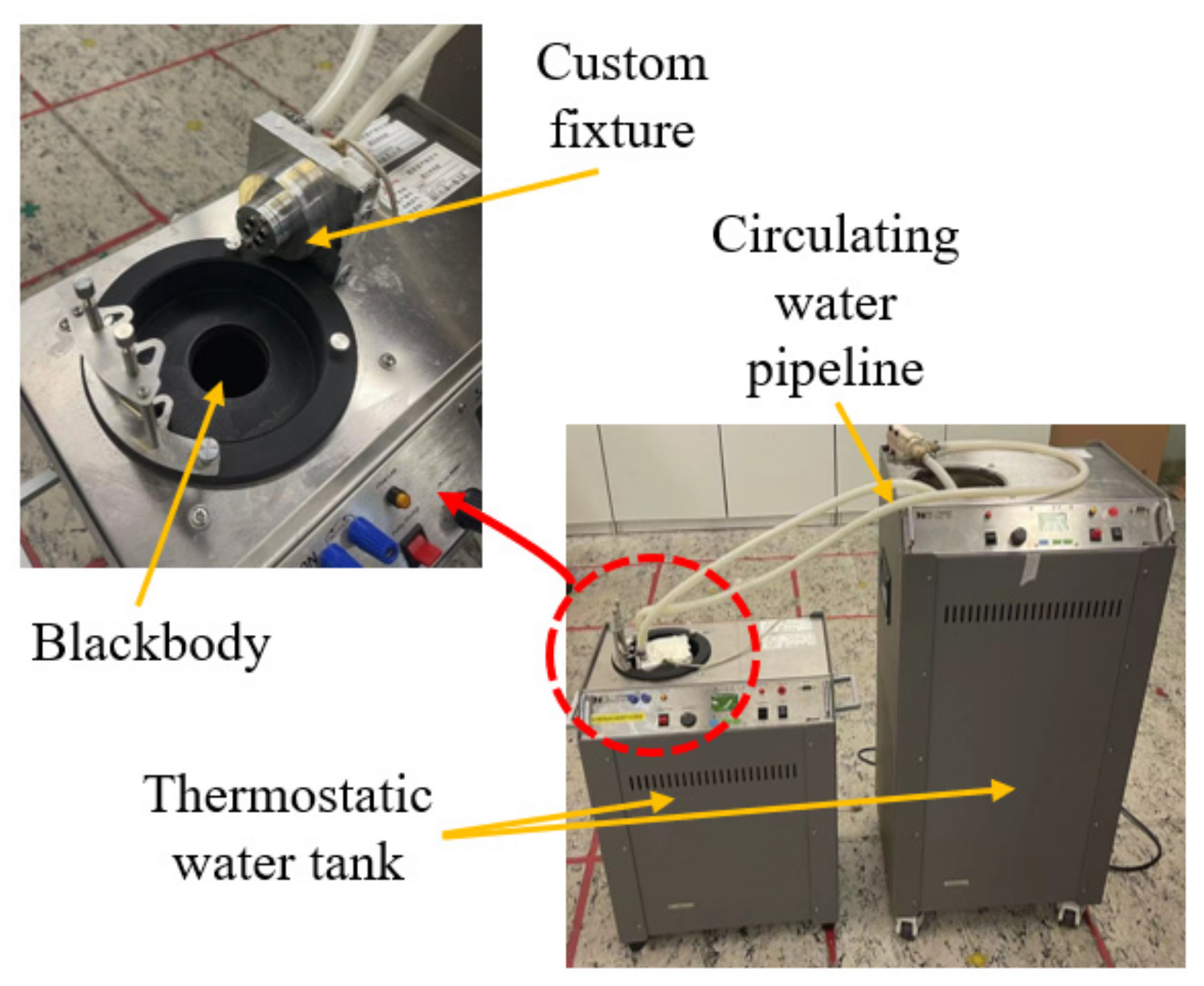
2.5.1. Design of Infrared Temperature Sensor
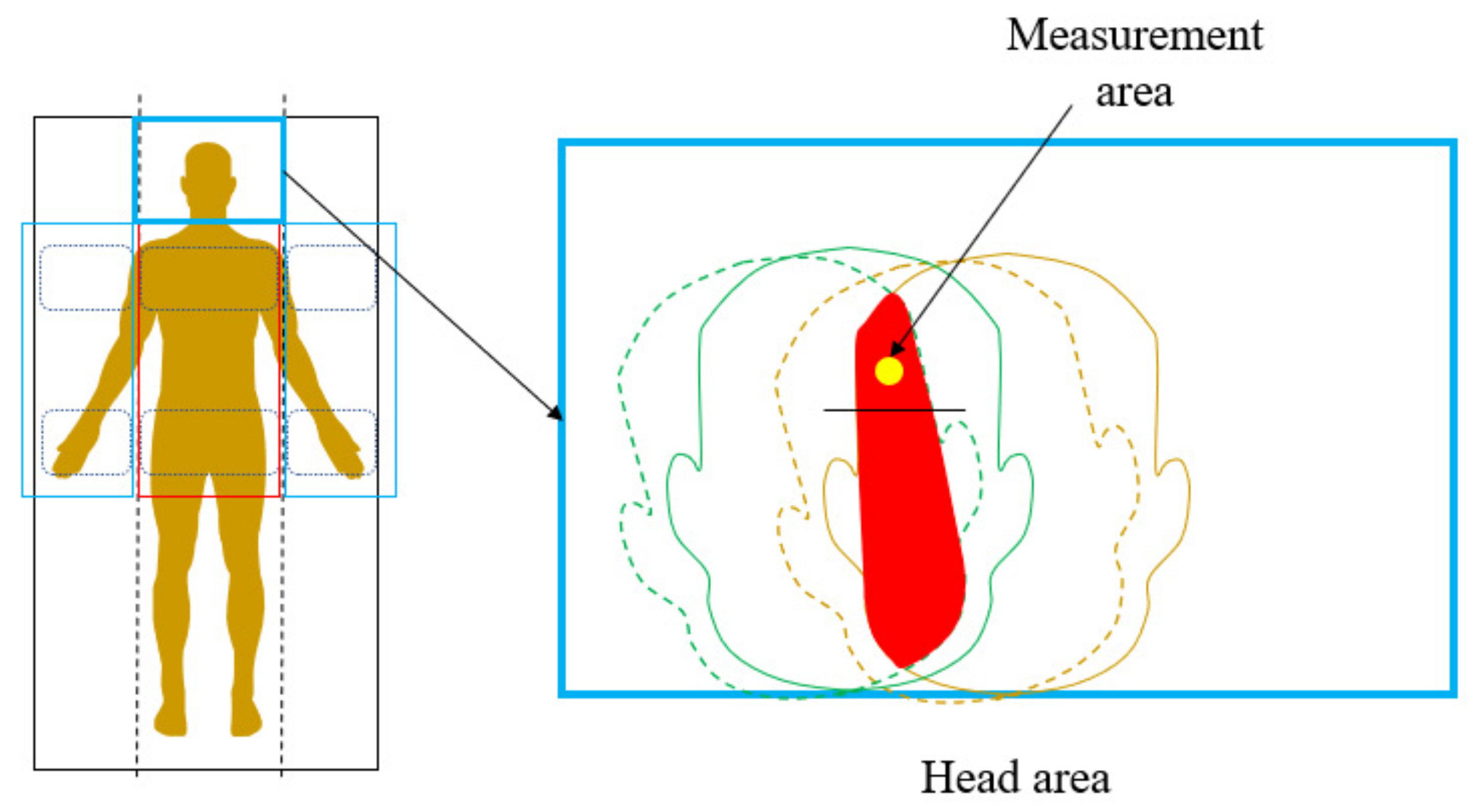
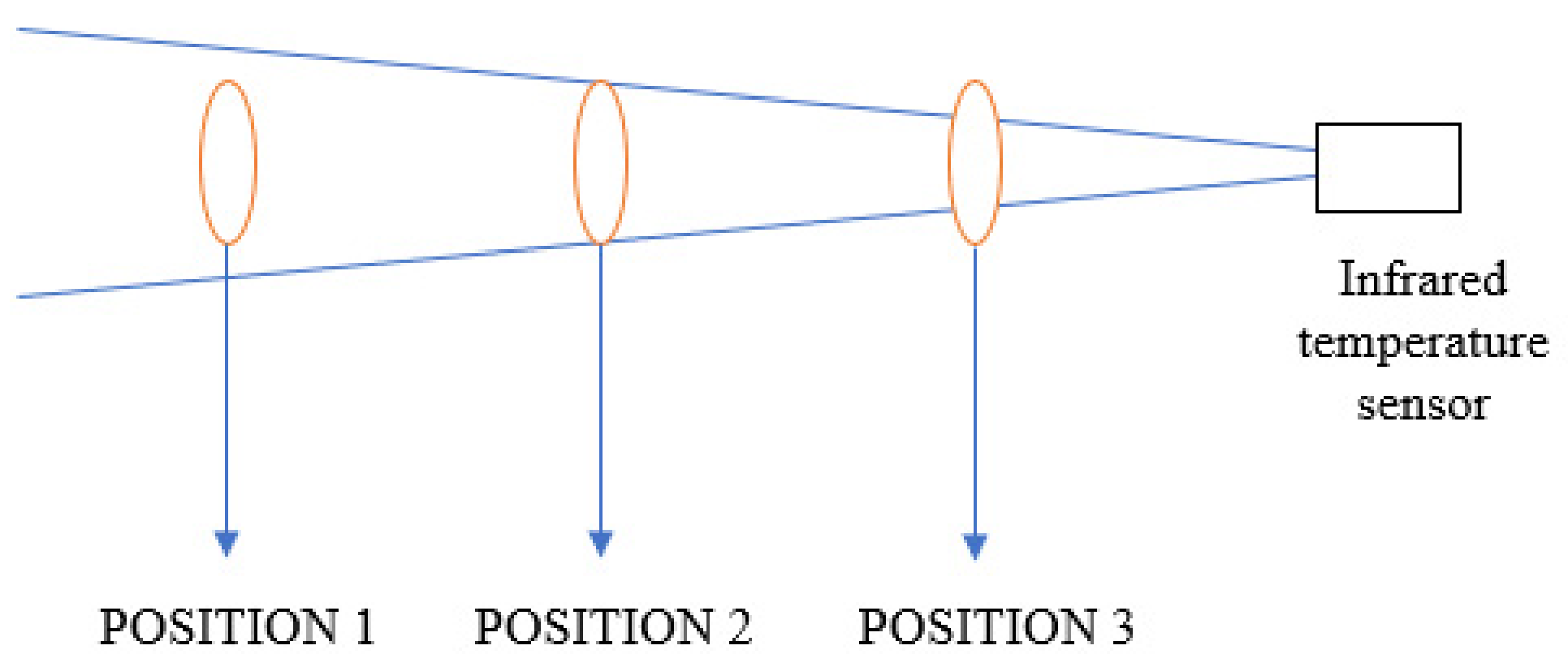
2.5.2. Design of Sensor Placement
3. Results
3.1. Mattress Turnover Test
3.2. Temperature Sensor Monitors the State of Bed Rest
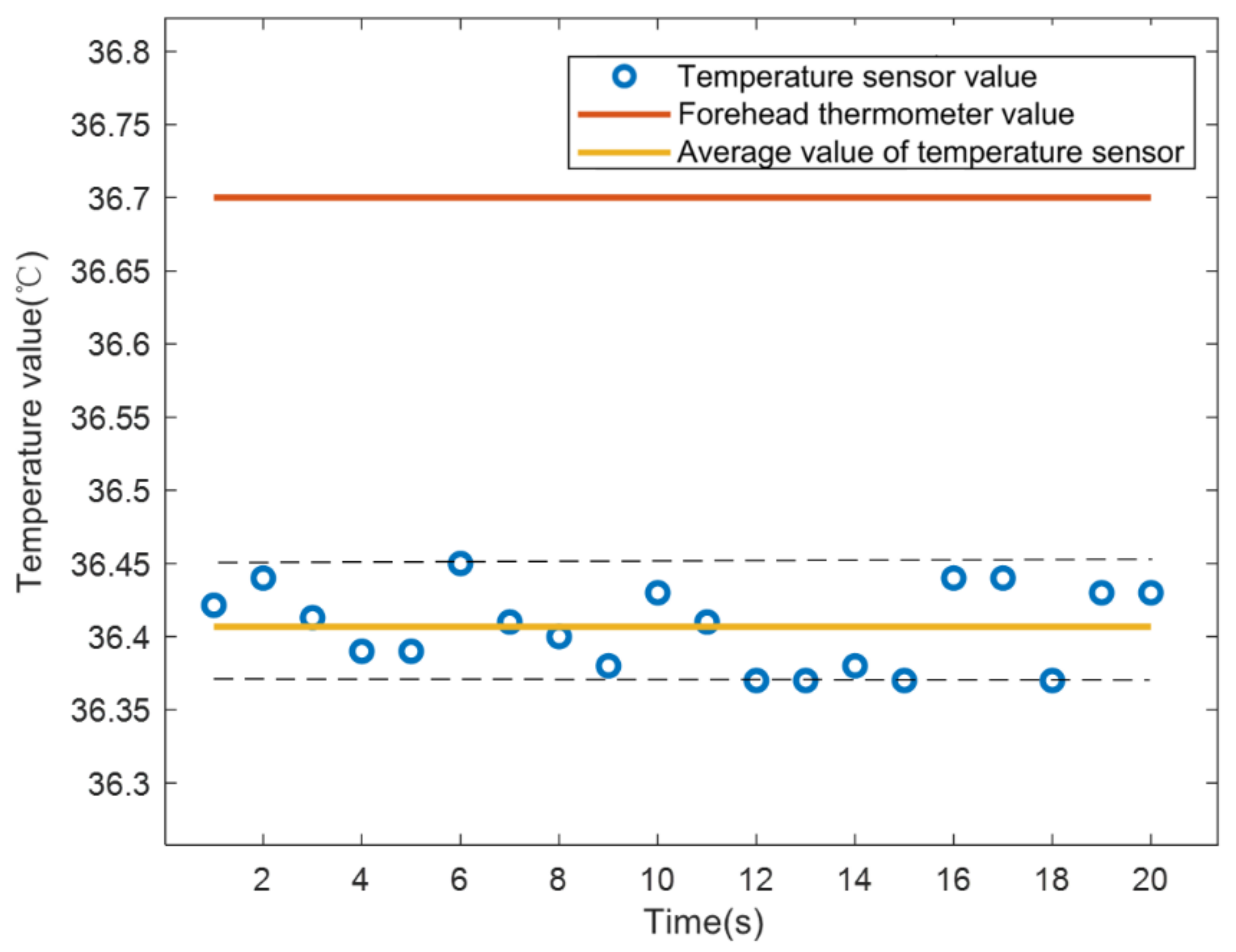
3.2.1. Real-Time Forehead Temperature Measurement
3.2.2. Out-of-Bed Monitoring and Position Monitoring
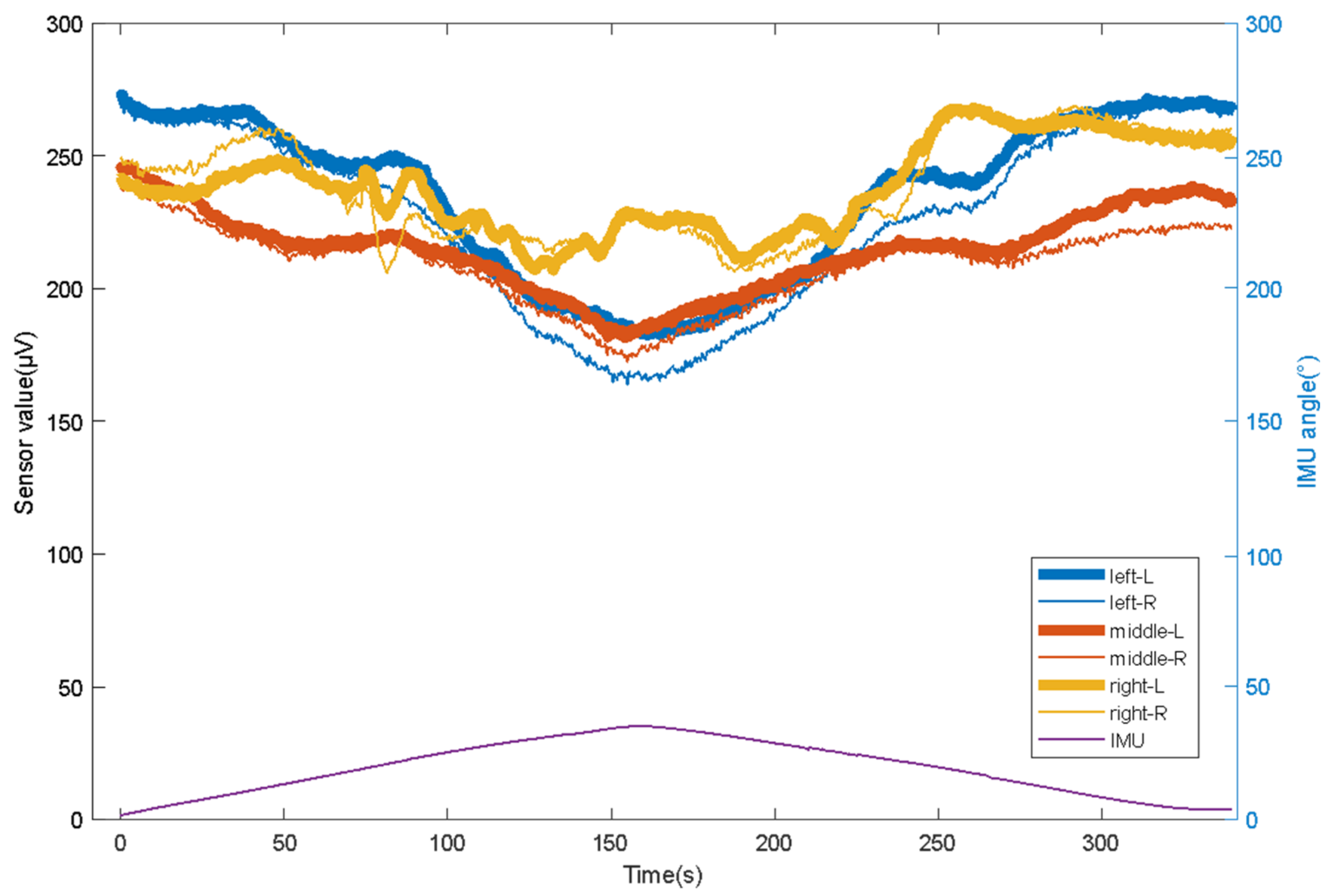
3.2.3. Real-Time Monitoring of the Turning Process
4. Conclusions and Discussion
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Gaspar, S.; Peralta, M.; Marques, A.; Budri, A.; De Matos, M.G. Effectiveness on hospital-acquired pressure ulcers prevention: A systematic review. Int. Wound J. 2019, 16, 1087–1102. [Google Scholar] [CrossRef]
- Serraes, B.; Van Leen, M.; Schols, J.; Van Hecke, A.; Verhaeghe, S.; Beeckman, D. Prevention of pressure ulcers with a static air support surface: A systematic review. Int. Wound J. 2018, 15, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Wang, L.; Yi, J.A.F.T.; Li, Q.; Liu, T. Reconstructing Walking Dynamics from Two Shank-Mounted Inertial Measurement Units (IMUs). IEEE/ASME Trans. Mechatron. 2021, 1. [Google Scholar] [CrossRef]
- Zhong, Z.; Chen, F.; Zhai, Q.; Fu, Z.; Ferreira, J.; Liu, Y.; Yi, J.; Liu, T. A real-time pre-impact fall detection and protection system. In Proceedings of the 2018 IEEE/ASME International Conference on Advanced Intelligent Mechatronics (AIM), Auckland, New Zealand, 9–12 June 2018; pp. 1039–1044. [Google Scholar]
- Nageswaran, S.; Vijayakumar, R.; Sivarasu, S. Design of mechanical interface to re-distribute excess pressure to prevent the formation of decubitus ulcers in bed ridden patients. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 1021–1024. [Google Scholar]
- Demarré, L.; Van Lancker, A.; Van Hecke, A.; Verhaeghe, S.; Grypdonck, M.; Lemey, J.; Annemans, L.; Beeckman, D. The cost of prevention and treatment of pressure ulcers: A systematic review. Int. J. Nurs. Stud. 2015, 52, 1754–1774. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.; Mathur, S.; Bhandare, R.; Narayanan, G. Bed sore Prevention using Pneumatic controls. In Proceedings of the 2020 IEEE International Conference on Electronics, Computing and Communication Technologies (CONECCT), Bangalore, India, 2–4 July 2020; pp. 1–5. [Google Scholar]
- Guo, S.; Kato, Y.; Ito, H.; Mukai, T. Development of rubber-based flexible sensor sheet for care-related apparatus. SEI Tech. Rev. 2012, 75, 125–131. [Google Scholar]
- Meaume, S.; Marty, M. Pressure ulcer prevention using an alternating-pressure mattress overlay: The MATCARP project. J. Wound Care 2020, 29 (Suppl. 9a), S32–S38. [Google Scholar] [CrossRef]
- Misaki, A.; Imanishi, K.; Takasugi, S.I.; Wada, M.; Fukagawa, S.; Furue, M. Body pressure sensing mattress for bedsore prevention. SEI Tech. Rev. 2014, 79, 95–99. [Google Scholar]
- Aleksandrowicz, H.; Owczarczyk-Saczonek, A.; Placek, W. Venous Leg Ulcers: Advanced Therapies and New Technologies. Biomedicines 2021, 9, 1569. [Google Scholar] [CrossRef] [PubMed]
- Tayyib, N.; Coyer, F. Effectiveness of pressure ulcer prevention strategies for adult patients in intensive care units: A systematic review. Worldviews Evid.-Based Nurs. 2016, 13, 432–444. [Google Scholar] [CrossRef] [Green Version]
- Bergstrom, N. Treatment of Pressure Ulcers: Clinical Practice Guideline; DIANE Publishing: Collingdale, PA, USA, 2004. [Google Scholar]
- Carter, M.J. Economic Evaluations of Guideline-Based or Strategic Interventions for the Prevention or Treatment of Chronic Wounds. Appl. Health Econ. Health Policy 2014, 12, 373–389. [Google Scholar] [CrossRef] [Green Version]
- Hayakawa, T.; Misaki, A.; Takasugi, S.I.; Furue, M. Smart Rubber Active Mattress” Taiatsu Bunsan. SEI Tech. Rev. 2017, 85, 65–67. [Google Scholar]
- Yousefi, R.; Ostadabbas, S.; Faezipour, M.; Nourani, M.; Ng, V.; Tamil, L.S.; Bowling, A.; Behan, D.; Pompeo, M. A smart bed platform for monitoring & ulcer prevention. In Proceedings of the 2011 4th International Conference on Biomedical Engineering and Informatics (BMEI), Shanghai, China, 15–17 October 2011; pp. 1362–1366. [Google Scholar]
- Ricci, E.; Roberto, C.; Ippolito, A.; Bianco, A.; Scalise, M.T. A new pressure-relieving mattress overlay. EWMA J. 2013, 13, 1. [Google Scholar]
- Defloor, T.; De Bacquer, D.; Grypdonck, M.H. The effect of various combinations of turning and pressure reducing devices on the incidence of pressure ulcers. Int. J. Nurs. Stud. 2005, 42, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Sikka, M.P.; Garg, S. Functional textiles for prevention of pressure ulcers—A review. Res. J. Text. Appar. 2020, 24, 185–198. [Google Scholar] [CrossRef]
- Mansfield, S.; Obraczka, K.; Roy, S. Pressure Injury Prevention: A Survey. IEEE Rev. Biomed. Eng. 2019, 13, 352–368. [Google Scholar] [CrossRef] [PubMed]
- Tannen, A.; Dassen, T.; Halfens, R. Differences in prevalence of pressure ulcers between the Netherlands and Germany—Associations between risk, prevention and occurrence of pressure ulcers in hospitals and nursing homes. J. Clin. Nurs. 2008, 17, 9. [Google Scholar] [CrossRef] [PubMed]
- McInnes, E.; National Institite for Clinical Excellence. The use of pressure-relieving devices (beds, mattresses and overlays) for the prevention of pressure ulcers in primary and secondary care. J. Tissue Viability 2004, 14, 4–6. [Google Scholar] [PubMed]
- Pan, P.; Haesler, E. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline; Cambridge Media: Hong Kong, China, 2014. [Google Scholar]
- Padula, W.V.; Mishra, M.K.; Makic, M.B.F.; Sullivan, P.W. Improving the Quality of Pressure Ulcer Care with Prevention: A Cost-Effectiveness Analysis. Med. Care 2011, 49, 385. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.P.; Patricia, W.S. A systematic review of economic evaluations assessing interventions aimed at preventing or treating pressure ulcers. Int. J. Nurs. Stud. 2015, 52, 769–788. [Google Scholar] [CrossRef] [PubMed]
- Schulz, S.; Pylatiuk, C.; Bretthauer, G. A new ultralight anthropomorphic hand. In Proceedings of the 2001 ICRA. IEEE International Conference on Robotics and Automation (Cat. No. 01CH37164), Seoul, Korea, 21–26 May 2001; pp. 2437–2441. [Google Scholar]
- Spetz, J.; Brown, D.S.; Aydin, C.; Donaldson, N. The value of reducing hospital-acquired pressure ulcer prevalence: An illustrative analysis. J. Nurs. Adm. 2013, 43, 235. [Google Scholar] [CrossRef] [PubMed]
- Vanderwee, K.; Defloor, T.; Beeckman, D.; Demarré, L.; Verhaeghe, S.; Van Durme, T.; Gobert, M. Assessing the adequacy of pressure ulcer prevention in hospitals: A nationwide prevalence survey. BMJ Qual. Saf. 2011, 20, 260–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgarten, M.; Margolis, D.; Orwig, D.; Hawkes, W.; Rich, S.; Langenberg, P.; Shardell, M.; Palmer, M.H.; McArdle, P.; Sterling, R.; et al. Use of Pressure-Redistributing Support Surfaces Among Elderly Hip Fracture Patients Across the Continuum of Care: Adherence to Pressure Ulcer Prevention Guidelines. Gerontologist 2010, 50, 253–262. [Google Scholar] [CrossRef] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Zou, X.; Zhang, B.; Han, Y.; Wang, S.; Liu, T.; Zhang, X. A Flexible Turning and Sensing System for Pressure Ulcers Prevention. Electronics 2021, 10, 2971. https://doi.org/10.3390/electronics10232971
Zhang Y, Zou X, Zhang B, Han Y, Wang S, Liu T, Zhang X. A Flexible Turning and Sensing System for Pressure Ulcers Prevention. Electronics. 2021; 10(23):2971. https://doi.org/10.3390/electronics10232971
Chicago/Turabian StyleZhang, Ying, Xiaofeng Zou, Bin Zhang, Yi Han, Shuoyu Wang, Tao Liu, and Xiufeng Zhang. 2021. "A Flexible Turning and Sensing System for Pressure Ulcers Prevention" Electronics 10, no. 23: 2971. https://doi.org/10.3390/electronics10232971
APA StyleZhang, Y., Zou, X., Zhang, B., Han, Y., Wang, S., Liu, T., & Zhang, X. (2021). A Flexible Turning and Sensing System for Pressure Ulcers Prevention. Electronics, 10(23), 2971. https://doi.org/10.3390/electronics10232971