
Artificial Intelligence in Plastic Surgery: Advancements, Applications, and Future




{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
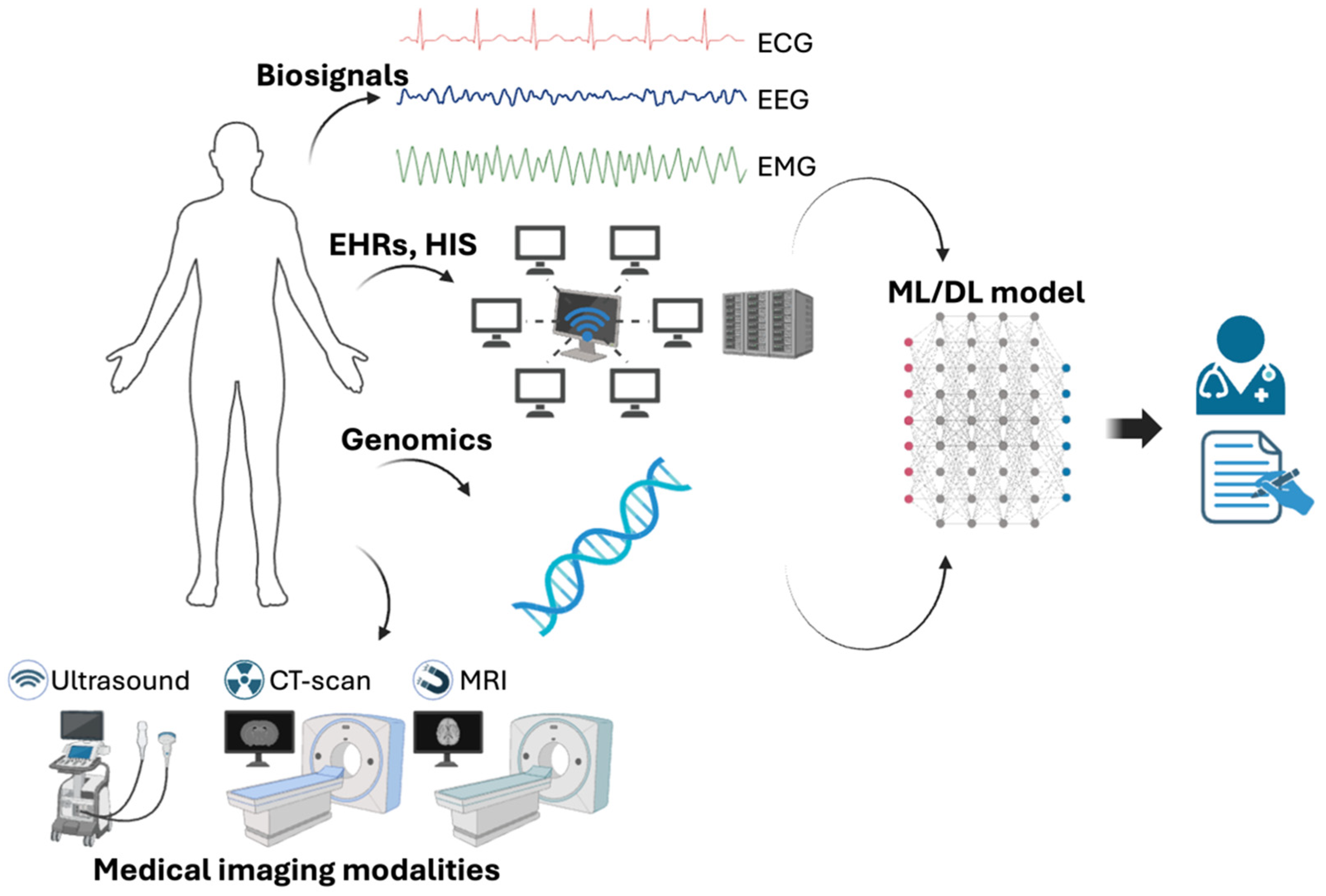
2. Concept of AI
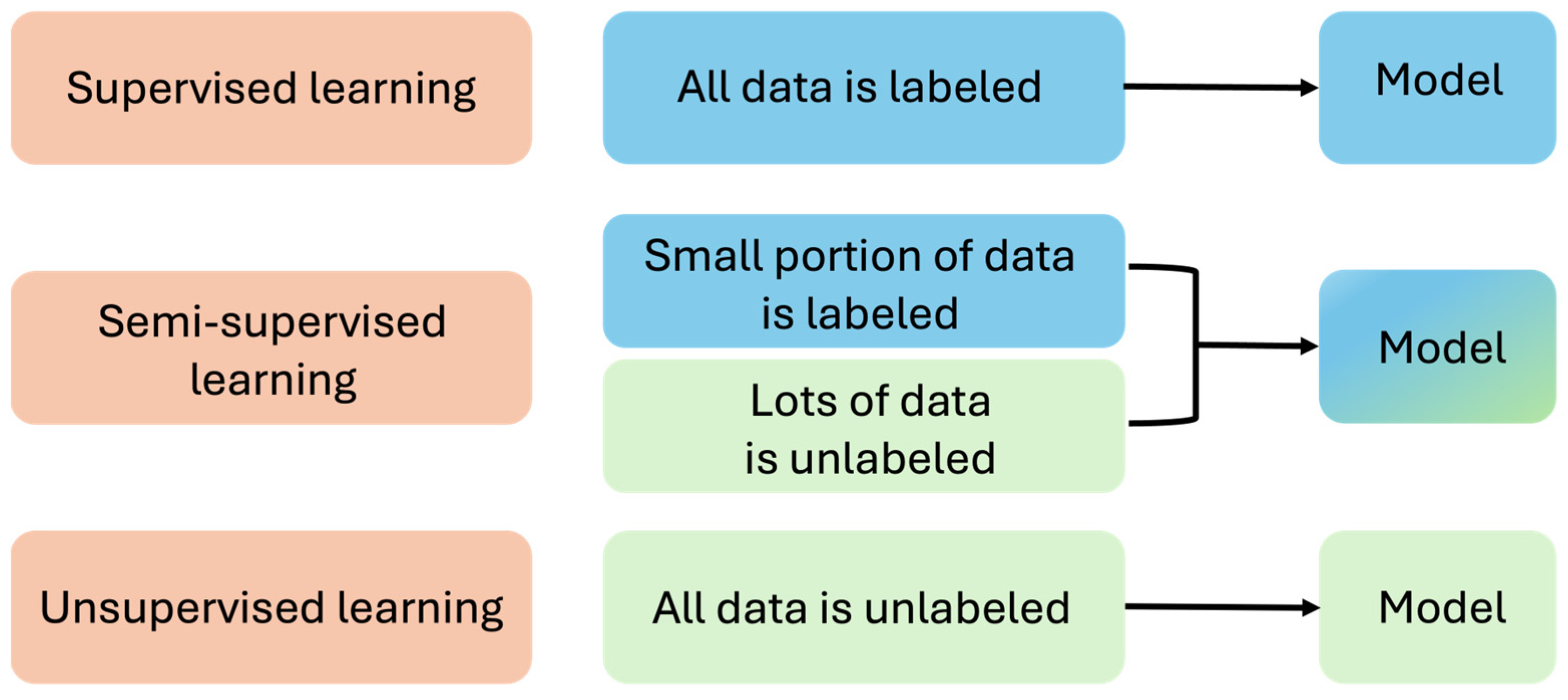
2.1. Machine Learning
2.2. Deep Learning
2.3. Natural Language Processing
3. Current Developments in AI for Plastic Surgery
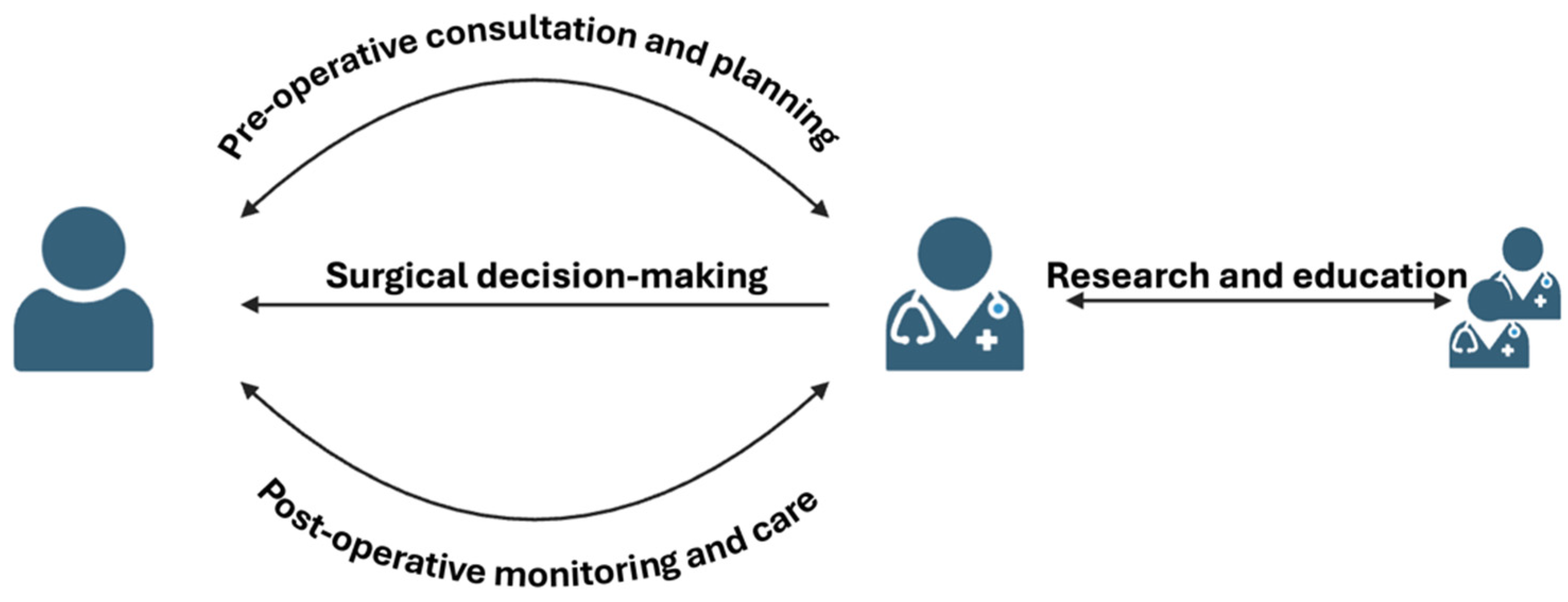
3.1. Using AI in Pre-Operative Consultation and Planning
3.2. Using AI in Surgical Decision-Making and Performance
3.3. Using AI in Simulating Surgical Outcomes
3.4. Using AI in Postoperative Monitoring and Care
3.5. Using AI in Research and Education
4. Future Perspectives and Challenges
4.1. Potential Applications of AI in Plastic Surgery beyond Current Capabilities
4.2. Challenges and Limitations in AI Implementation
4.3. Opportunities for Collaboration between AI Researchers, Plastic Surgeons, and Regulatory Bodies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rajpurkar, P.; Chen, E.; Banerjee, O.; Topol, E.J. AI in health and medicine. Nat. Med. 2022, 28, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Landi, I.; Glicksberg, B.S.; Lee, H.-C.; Cherng, S.; Landi, G.; Danieletto, M.; Dudley, J.T.; Furlanello, C.; Miotto, R. Deep representation learning of electronic health records to unlock patient stratification at scale. NPJ Digit. Med. 2020, 3, 96. [Google Scholar] [CrossRef] [PubMed]
- Hobensack, M.; Song, J.; Scharp, D.; Bowles, K.H.; Topaz, M. Machine learning applied to electronic health record data in home healthcare: A scoping review. Int. J. Med. Inf. 2023, 170, 104978. [Google Scholar] [CrossRef] [PubMed]
- Hung, T.N.K.; Vy, V.P.T.; Tri, N.M.; Hoang, L.N.; Tuan, L.V.; Ho, Q.T.; Le, N.Q.K.; Kang, J.H. Automatic Detection of Meniscus Tears Using Backbone Convolutional Neural Networks on Knee MRI. J. Magn. Reson. Imaging 2023, 57, 740–749. [Google Scholar] [CrossRef] [PubMed]
- Lassau, N.; Ammari, S.; Chouzenoux, E.; Gortais, H.; Herent, P.; Devilder, M.; Soliman, S.; Meyrignac, O.; Talabard, M.-P.; Lamarque, J.-P.; et al. Integrating deep learning CT-scan model, biological and clinical variables to predict severity of COVID-19 patients. Nat. Commun. 2021, 12, 634. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.X.; Yordanov, B.; Gaunt, A.; Wang, M.X.; Dai, P.; Chen, Y.-J.; Zhang, K.; Fang, J.Z.; Dalchau, N.; Li, J.; et al. A deep learning model for predicting next-generation sequencing depth from DNA sequence. Nat. Commun. 2021, 12, 4387. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Ma, J. Machine Learning Methods for Exploring Sequence Determinants of 3D Genome Organization. J. Mol. Biol. 2022, 434, 167666. [Google Scholar] [CrossRef] [PubMed]
- Mincholé, A.; Camps, J.; Lyon, A.; Rodríguez, B. Machine learning in the electrocardiogram. J. Electrocardiol. 2019, 57, S61–S64. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.C.; Massey, S.L.; Kirschen, M.P.; Yuan, I.; Padiyath, A.; Simpao, A.F.; Tsui, F.R. Electroencephalogram-based machine learning models to predict neurologic outcome after cardiac arrest: A systematic review. Resuscitation 2024, 194, 110049. [Google Scholar] [CrossRef]
- Morbidoni, C.; Cucchiarelli, A.; Agostini, V.; Knaflitz, M.; Fioretti, S.; Di Nardo, F. Machine-Learning-Based Prediction of Gait Events from EMG in Cerebral Palsy Children. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 819–830. [Google Scholar] [CrossRef]
- Vy, V.P.T.; Yao, M.M.-S.; Khanh Le, N.Q.; Chan, W.P. Machine Learning Algorithm for Distinguishing Ductal Carcinoma In Situ from Invasive Breast Cancer. Cancers 2022, 14, 2437. [Google Scholar] [CrossRef]
- Abdollahi, J.; Mehrpour, O. Using Machine Learning Algorithms for Coronary Artery Disease (CAD) Prediction Prediction of Coronary Artery Disease (CAD) Using Machine Learning Algorithms. In Proceedings of the 2024 10th International Conference on Artificial Intelligence and Robotics (QICAR), Qazvin, Iran, 29 February 2024; pp. 164–172. [Google Scholar]
- Jeong, J.; Wang, L.; Ji, B.; Lei, Y.; Ali, A.; Liu, T.; Curran, W.J.; Mao, H.; Yang, X. Machine-learning based classification of glioblastoma using delta-radiomic features derived from dynamic susceptibility contrast enhanced magnetic resonance images. Quant. Imaging Med. Surg. 2019, 9, 1201–1213. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Xu, H.; Ming, Y.; Liu, Q.; Huang, C.; Xu, J.; Zhang, J.; Li, Y. Predicting myometrial invasion in endometrial cancer based on whole-uterine magnetic resonance radiomics. J. Cancer Res. Ther. 2020, 16, 1648–1655. [Google Scholar] [PubMed]
- Fujihara, K.; Sone, H. Machine Learning Approach to Drug Treatment Strategy for Diabetes Care. Diabetes Metab. J. 2023, 47, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Shen, X.; Pan, W. Deep reinforcement learning for personalized treatment recommendation. Stat. Med. 2022, 41, 4034–4056. [Google Scholar] [CrossRef] [PubMed]
- Jin, C.; Yu, H.; Ke, J.; Ding, P.; Yi, Y.; Jiang, X.; Duan, X.; Tang, J.; Chang, D.T.; Wu, X.; et al. Predicting treatment response from longitudinal images using multi-task deep learning. Nat. Commun. 2021, 12, 1851. [Google Scholar] [CrossRef]
- Rafique, R.; Islam, S.M.R.; Kazi, J.U. Machine learning in the prediction of cancer therapy. Comput. Struct. Biotechnol. J. 2021, 19, 4003–4017. [Google Scholar] [CrossRef] [PubMed]
- Squarcina, L.; Villa, F.M.; Nobile, M.; Grisan, E.; Brambilla, P. Deep learning for the prediction of treatment response in depression. J. Affect. Disord. 2021, 281, 618–622. [Google Scholar] [CrossRef]
- Sharma, S.; Rawal, R.; Shah, D. Addressing the challenges of AI-based telemedicine: Best practices and lessons learned. J. Educ. Health Promot. 2023, 12, 338. [Google Scholar] [CrossRef]
- Bhaskar, S.; Bradley, S.; Sakhamuri, S.; Moguilner, S.; Chattu, V.K.; Pandya, S.; Schroeder, S.; Ray, D.; Banach, M. Designing futuristic telemedicine using artificial intelligence and robotics in the COVID-19 era. Front. Public. Health 2020, 8, 556789. [Google Scholar] [CrossRef]
- Beldhuis, I.E.; Marapin, R.S.; Jiang, Y.Y.; Simões de Souza, N.F.; Georgiou, A.; Kaufmann, T.; Castela Forte, J.; van der Horst, I.C.C. Cognitive biases, environmental, patient and personal factors associated with critical care decision making: A scoping review. J. Crit. Care 2021, 64, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Hastie, T.; Tibshirani, R.; Friedman, J.H.; Friedman, J.H. The Elements of Statistical Learning: Data Mining, Inference, and Prediction; Springer: Berlin/Heidelberg, Germany, 2009; Volume 2. [Google Scholar]
- Kooi, T.; Litjens, G.; van Ginneken, B.; Gubern-Mérida, A.; Sánchez, C.I.; Mann, R.; den Heeten, A.; Karssemeijer, N. Large scale deep learning for computer aided detection of mammographic lesions. Med. Image Anal. 2017, 35, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Cicero, M.; Bilbily, A.; Colak, E.; Dowdell, T.; Gray, B.; Perampaladas, K.; Barfett, J. Training and Validating a Deep Convolutional Neural Network for Computer-Aided Detection and Classification of Abnormalities on Frontal Chest Radiographs. Investig. Radiol. 2017, 52, 281–287. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Lysaght, T.; Lim, H.Y.; Xafis, V.; Ngiam, K.Y. AI-Assisted Decision-making in Healthcare: The Application of an Ethics Framework for Big Data in Health and Research. Asian Bioeth. Rev. 2019, 11, 299–314. [Google Scholar] [CrossRef] [PubMed]
- Lorenzini, G.; Arbelaez Ossa, L.; Shaw, D.M.; Elger, B.S. Artificial intelligence and the doctor–patient relationship expanding the paradigm of shared decision making. Bioethics 2023, 37, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.W.; Tsai, T.Y.; Hsieh, Y.H.; Hsu, C.C.; Chen, S.H.; Lee, C.H.; Lin, Y.T.; Kao, H.K.; Lin, C.H. Reliability of Postoperative Free Flap Monitoring with a Novel Prediction Model Based on Supervised Machine Learning. Plast. Reconstr. Surg. 2023, 152, 943e–952e. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.; Farnebo, S.; Horwitz, M.D. Insights and trends review: Artificial intelligence in hand surgery. J. Hand Surg. Eur. Vol. 2023, 48, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, D.R. Art, Artificial Intelligence, and Aesthetics in Plastic Surgery. Plast. Reconstr. Surg. 2021, 148, 529e–530e. [Google Scholar] [CrossRef]
- Hassan, A.M.; Biaggi-Ondina, A.; Asaad, M.; Morris, N.; Liu, J.; Selber, J.C.; Butler, C.E. Artificial Intelligence Modeling to Predict Periprosthetic Infection and Explantation following Implant-Based Reconstruction. Plast. Reconstr. Surg. 2023, 152, 929–938. [Google Scholar] [CrossRef]
- Turner, A.E.; Abu-Ghname, A.; Davis, M.J.; Ali, K.; Winocour, S. Role of simulation and artificial intelligence in plastic surgery training. Plast. Reconstr. Surg. 2020, 146, 390e–391e. [Google Scholar] [CrossRef]
- Qin, F.; Gu, J. Artificial intelligence in plastic surgery: Current developments and future perspectives. Plast. Aesthetic Res. 2023, 10, 3. [Google Scholar] [CrossRef]
- TerKonda, S.P.; TerKonda, A.A.; Sacks, J.M.; Kinney, B.M.; Gurtner, G.C.; Nachbar, J.M.; Reddy, S.K.; Jeffers, L.L. Artificial Intelligence: Singularity Approaches. Plast. Reconstr. Surg. 2024, 153, 10–1097. [Google Scholar] [CrossRef]
- Nasteski, V. An overview of the supervised machine learning methods. HORIZONSB 2017, 4, 51–62. [Google Scholar] [CrossRef]
- Alloghani, M.; Al-Jumeily, D.; Mustafina, J.; Hussain, A.J.; Aljaaf, A.J. A Systematic Review on Supervised and Unsupervised Machine Learning Algorithms for Data Science. In Supervised and Unsupervised Learning for Data Science; Unsupervised Semi-Supervised Learn; Springer: Berlin/Heidelberg, Germany, 2019; pp. 3–21. [Google Scholar]
- Zhu, X.; Goldberg, A.B. Overview of Semi-Supervised Learning. In Introduction to Semi-Supervised Learning; Springer International Publishing: Cham, Switzerland, 2009; pp. 9–19. [Google Scholar]
- Wang, J.; Chen, Y. Overview of Transfer Learning Algorithms. In Introduction to Transfer Learning: Algorithms and Practice; Wang, J., Chen, Y., Eds.; Springer Nature: Singapore, 2023; pp. 53–66. [Google Scholar]
- Sarker, I.H. Deep Learning: A Comprehensive Overview on Techniques, Taxonomy, Applications and Research Directions. SN Comput. Sci. 2021, 2, 420. [Google Scholar] [CrossRef]
- Kotu, V.; Deshpande, B. Chapter 10—Deep Learning. In Data Science, 2nd ed.; Kotu, V., Deshpande, B., Eds.; Morgan Kaufmann: Burlington, MA, USA, 2019; pp. 307–342. [Google Scholar]
- Chen, Y.; Li, L.; Li, W.; Guo, Q.; Du, Z.; Xu, Z. Chapter 3—Deep learning. In AI Computing Systems; Chen, Y., Li, L., Li, W., Guo, Q., Du, Z., Xu, Z., Eds.; Morgan Kaufmann: Burlington, MA, USA, 2024; pp. 53–121. [Google Scholar]
- Boczar, D.; Sisti, A.; Oliver, J.D.; Helmi, H.; Restrepo, D.J.; Huayllani, M.T.; Spaulding, A.C.; Carter, R.; Rinker, B.D.; Forte, A.J. Artificial Intelligent Virtual Assistant for Plastic Surgery Patient’s Frequently Asked Questions: A Pilot Study. Ann. Plast. Surg. 2020, 84, e16–e21. [Google Scholar] [CrossRef]
- Hammond, D.C.; Kim, K.; Bageris, M.H.; Chaudhry, A. Use of three-dimensional imaging to assess the effectiveness of volume as a critical variable in breast implant selection. Plast. Reconstr. Surg. 2022, 149, 70–79. [Google Scholar] [CrossRef]
- Kooi, K.; Martinez, E.T.; Freundt, L.; Oflazoglu, K.; Ritt, M.J.P.F.; Eberlin, K.R.; Selles, R.W.; Clemens, M.W.; Rakhorst, H.A. From Data to Decisions: How AI Is Revolutionizing Clinical Prediction Models in Plastic Surgery. Plast. Reconstr. Surg. 2021, 10–1097. [Google Scholar] [CrossRef]
- Hoogendam, L.; Bakx, J.A.C.; Souer, J.S.; Slijper, H.P.; Andrinopoulou, E.-R.; Selles RWobotHWSG. Predicting Clinically Relevant Patient-Reported Symptom Improvement After Carpal Tunnel Release: A Machine Learning Approach. Neurosurgery 2022, 90, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Loos, N.L.; Hoogendam, L.; Souer, J.S.; Slijper, H.P.; Andrinopoulou, E.-R.; Coppieters, M.W.; Selles, R.W.; Group tH-WS. Machine Learning Can be Used to Predict Function but Not Pain after Surgery for Thumb Carpometacarpal Osteoarthritis. Clin. Orthop. Relat. Res. 2022, 480, 1271–1284. [Google Scholar] [CrossRef] [PubMed]
- Shademan, A.; Decker, R.S.; Opfermann, J.D.; Leonard, S.; Krieger, A.; Kim, P.C. Supervised autonomous robotic soft tissue surgery. Sci. Transl. Med. 2016, 8, 337ra364. [Google Scholar] [CrossRef]
- Li, Y.; Cheng, J.; Mei, H.; Ma, H.; Chen, Z.; Li, Y. CLPNet: Cleft Lip and Palate Surgery Support with Deep Learning. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2019, 2019, 3666–3672. [Google Scholar] [PubMed]
- Phillips, M.; Marsden, H.; Jaffe, W.; Matin, R.N.; Wali, G.N.; Greenhalgh, J.; McGrath, E.; James, R.; Ladoyanni, E.; Bewley, A.; et al. Assessment of Accuracy of an Artificial Intelligence Algorithm to Detect Melanoma in Images of Skin Lesions. JAMA Netw. Open 2019, 2, e1913436. [Google Scholar] [CrossRef]
- Bodenstedt, S.; Wagner, M.; Müller-Stich, B.P.; Weitz, J.; Speidel, S. Artificial Intelligence-Assisted Surgery: Potential and Challenges. Visc. Med. 2020, 36, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, B.; Nadri, H.; Lotfnezhad Afshar, H.; Timpka, T. A Systematic Review of the Technology Acceptance Model in Health Informatics. Appl. Clin. Inf. 2018, 9, 604–634. [Google Scholar] [CrossRef]
- Chartier, C.; Watt, A.; Lin, O.; Chandawarkar, A.; Lee, J.; Hall-Findlay, E. BreastGAN: Artificial Intelligence-Enabled Breast Augmentation Simulation. Aesthet. Surg. J. Open Forum 2022, 4, ojab052. [Google Scholar] [CrossRef]
- Chinski, H.; Lerch, R.; Tournour, D.; Chinski, L.; Caruso, D. An Artificial Intelligence Tool for Image Simulation in Rhinoplasty. Facial Plast. Surg. 2022, 38, 201–206. [Google Scholar] [CrossRef]
- Conforth, M.; Meng, Y.; Valmikinathan, C.; Yu, X. Nerve graft selection for peripheral nerve regeneration using neural networks trained by a hybrid ACO/PSO method. In Proceedings of the 2009 IEEE Symposium on Computational Intelligence in Bioinformatics and Computational Biology, Nashville, TN, USA, 30 March–2 April 2009; pp. 208–214. [Google Scholar]
- Crystal, D.T.; Cuccolo, N.G.; Ibrahim, A.M.S.; Furnas, H.; Lin, S.J. Photographic and Video Deepfakes Have Arrived: How Machine Learning May Influence Plastic Surgery. Plast. Reconstr. Surg. 2020, 145, 1079–1086. [Google Scholar] [CrossRef]
- Chartier, C.; Gfrerer, L.; Knoedler, L.; Austen, W.G., Jr. Artificial Intelligence–Enabled Evaluation of Pain Sketches to Predict Outcomes in Headache Surgery. Plast. Reconstr. Surg. 2023, 151, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Aasvang, E.K.; Meyhoff, C.S. The future of postoperative vital sign monitoring in general wards: Improving patient safety through continuous artificial intelligence-enabled alert formation and reduction. Curr. Opin. Anesthesiol. 2023, 36, 683–690. [Google Scholar] [CrossRef]
- Chairat, S.; Chaichulee, S.; Dissaneewate, T.; Wangkulangkul, P.; Kongpanichakul, L. AI-Assisted Assessment of Wound Tissue with Automatic Color and Measurement Calibration on Images Taken with a Smartphone. Healthcare 2023, 11, 273. [Google Scholar] [CrossRef] [PubMed]
- Soguero-Ruiz, C.; Fei, W.M.; Jenssen, R.; Augestad, K.M.; Álvarez, J.L.; Jiménez, I.M.; Lindsetmo, R.O.; Skrøvseth, S.O. Data-driven Temporal Prediction of Surgical Site Infection. AMIA Annu. Symp. Proc. 2015, 2015, 1164–1173. [Google Scholar] [PubMed]
- Sadideen, H.; Goutos, I.; Kneebone, R. Burns education: The emerging role of simulation for training healthcare professionals. Burns 2017, 43, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, M.J.; Luck, J.; Billingsley, M.L.; Heyes, R.; Smith, O.J.; Mosahebi, A.; Khoussa, A.; Abu-Sittah, G.; Hachach-Haram, N. Demonstration of the Effectiveness of Augmented Reality Telesurgery in Complex Hand Reconstruction in Gaza. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1708. [Google Scholar] [CrossRef] [PubMed]
- Schork, N.J. Artificial intelligence and personalized medicine. In Precision Medicine in Cancer Therapy; Springer: Berlin/Heidelberg, Germany, 2019; pp. 265–283. [Google Scholar]
- Mir, M.A. Artificial Intelligence Revolutionizing Plastic Surgery Scientific Publications. Cureus 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Farid, Y.; Fernando Botero Gutierrez, L.; Ortiz, S.; Gallego, S.; Zambrano, J.C.; Morrelli, H.U.; Patron, A. Artificial Intelligence in Plastic Surgery: Insights from Plastic Surgeons, Education Integration, ChatGPT’s Survey Predictions, and the Path Forward. Plast. Reconstr. Surg. Glob. Open 2024, 12, e5515. [Google Scholar] [CrossRef] [PubMed]
- Liu, J. Artificial Intelligence Is Still Far from Truly Revolutionizing Plastic Surgery. Plast. Reconstr. Surg. 2020, 146, 390e. [Google Scholar] [CrossRef]
- Parliament, E. Artificial Intelligence Act; European Parliament: Strasbourg, France, 2024. [Google Scholar]
- Farid, Y. A call for guidelines and regulatory body in adopting artificial intelligence for plastic surgeons. Plast. Reconstr. Surg. Glob. Open 2023, 11, e5340. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duong, T.V.; Vy, V.P.T.; Hung, T.N.K. Artificial Intelligence in Plastic Surgery: Advancements, Applications, and Future. Cosmetics 2024, 11, 109. https://doi.org/10.3390/cosmetics11040109
Duong TV, Vy VPT, Hung TNK. Artificial Intelligence in Plastic Surgery: Advancements, Applications, and Future. Cosmetics. 2024; 11(4):109. https://doi.org/10.3390/cosmetics11040109
Chicago/Turabian StyleDuong, Tran Van, Vu Pham Thao Vy, and Truong Nguyen Khanh Hung. 2024. "Artificial Intelligence in Plastic Surgery: Advancements, Applications, and Future" Cosmetics 11, no. 4: 109. https://doi.org/10.3390/cosmetics11040109
APA StyleDuong, T. V., Vy, V. P. T., & Hung, T. N. K. (2024). Artificial Intelligence in Plastic Surgery: Advancements, Applications, and Future. Cosmetics, 11(4), 109. https://doi.org/10.3390/cosmetics11040109