Dynamic Response Systems of Healthcare Mask Production to COVID-19: A Case Study of Korea




Abstract
1. Introduction
2. Product and Demand
2.1. Types of Products
2.2. Demand Planning and Management
- HS 6307.90: Textiles, made up articles; sets; worn clothing and worn textile articles; rags (no. 63)/Textiles; made up articles (including dress patterns), n.e.s. in chapter 63, n.e.s. in heading (no. 6307)/non-woven disposal mask, hood mask, face mask, cotton mask, etc./Others (No. 630790)
- HS 3005.90: Wadding, gauze, bandages, and similar articles; (excluding adhesive dressings), impregnated or coated with pharmaceutical substances, packaged for retail sale
- HS 9018.90: Medical, surgical, or dental instruments and appliances; n.e.c. in heading no. 9018
- Use respirators as identified by CDC as performing adequately for healthcare delivery beyond the manufacturer-designated shelf life.
- Use respirators approved under standards used in other countries that are similar to NIOSH (CDC’s National Institute of Occupational Safety and Health)-approved respirators.
- Use additional respirators identified by CDC as NOT performing adequately for healthcare delivery beyond the manufacturer-designated shelf life [24].
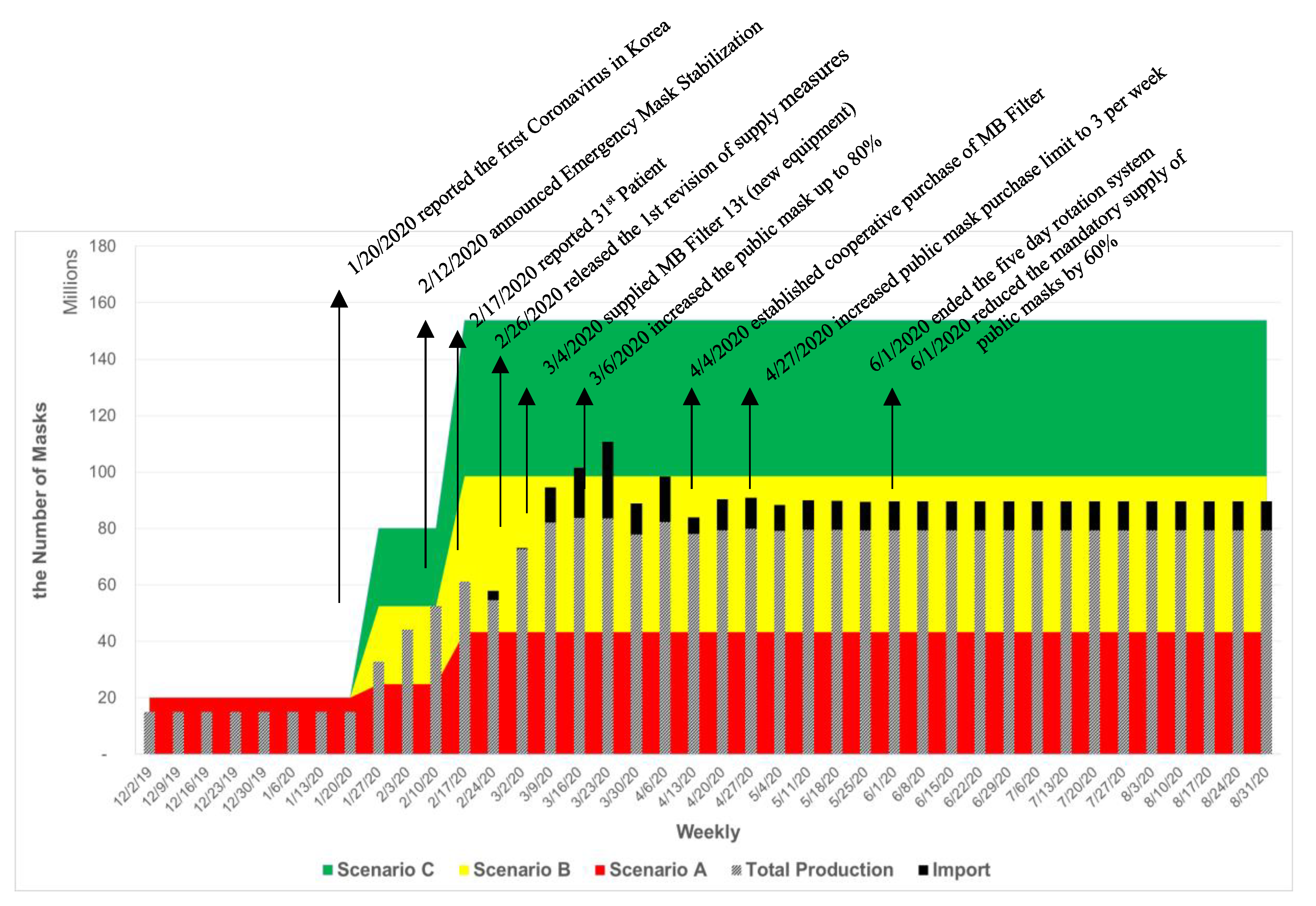
- Basic assumptions: This study assumes that around 36.8 million masks are estimated for college students, K-12 and kindergarten students, and business population in a day for five days a week. In addition, a medical population of 608,000 requires an average of 1.5 masks per day for seven days [25].
- Scenario A: With a lockdown approach, it is assumed that strong social distancing limits social activities, and that only 20% of the estimated population does basic economic activities five days a week.
- Scenario B: While maintaining strict social distancing and a high level of hygiene management, 50% of the estimated population actively engage in social and economic activities for five days a week.
- Scenario C: While practicing social distancing and a high level of hygiene management, 80% of the population is engaged in daily social and economic activities five days a week.
3. Production Capacity Planning and Expansion
3.1. Global Production Trends
3.2. Dynamic Response
3.3. Investing in Facility and Equipment
3.4. Mobilizing Industry
3.5. Staffing
“An employer shall, in addition to the ordinary wages, pay employees at least 50/100 thereof for extended work and pay employees who perform work on a holiday an amount the same as or more than the following amounts:
An employer shall, in addition to the ordinary wages, pay at least 50/100 thereof to employees who perform night work (referring to the work performed between 10:00 p.m. and 6:00 a.m. of the next day). (Labor Standards Act, Article 56)”
3.6. Regulations
3.7. Research and Development (R&D)
3.8. Cost and Profit
4. Strategic Production Plan for Emergency
5. Conclusions
- To develop a dynamic and timely response system to the changing market with flexible and agile operations.
- To increase visibility of inventory, distribution, and production systems.
- To collaborate with public and private sectors along with global organizations (such as WHO) for the global supply chain to overcome global challenges.
- To secure multiple separate channels for healthcare staff, public service providers, the underprivileged, and general consumers.
- To increase awareness of smart consumption with effective demand management.
- To develop management systems that respond to the dynamic, uncertain situations.
- To develop a strategic plan for long-term, and efficient operations for short-term.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Novel Coronavirus—Republic of Korea (ex-China). Available online: https://www.who.int/csr/don/21-january-2020-novel-coronavirus-republic-of-korea-ex-china/en/ (accessed on 21 January 2020).
- KTV. South Korean Government Joint-Briefing on COVID-19; Korea TV: Daejeon, Korea, 9 March 2020; Available online: http://www.ktv.go.kr/content/view?content_id=594852 (accessed on 18 April 2020).
- Nohria, N. What Organizations Need to Survive a Pandemic; Harvard Business Review: Boston, MA, USA, 2020; Volume 30. [Google Scholar]
- Mubareka, S.; Lowen, A.C.; Steel, J.; Coates, A.L.; García-Sastre, A.; Palese, P. Transmission of Influenza Virus via Aerosols and Fomites in the Guinea Pig Model. J. Infect. Dis. 2009, 199, 858–865. [Google Scholar] [CrossRef] [PubMed]
- Christian, M.D.; Loutfy, M.; McDonald, L.C.; Martinez, K.F.; Ofner, M.; Wong, T.; Wallington, T.; Gold, W.L.; Mederski, B.; Green, K.; et al. Possible SARS Coronavirus Transmission during Cardiopulmonary Resuscitation. Emerg. Infect. Dis. 2004, 10, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Harvard Medical School, Coronavirus Resource Center. 2020. Available online: https://www.health.harvard.edu/diseases-and-conditions/coronavirus-resource-center (accessed on 14 April 2020).
- Guzman, J. WHO: No Evidence Wearing a Mask Can Protect Healthy People from Coronavirus. Available online: https://thehill.com/changing-america/well-being/prevention-cures/491725-who-no-evidence-wearing-a-mask-can-protect (accessed on 25 April 2020).
- World Health Organization. Advice on the Use of Masks the Community, during Home Care and in Health Care Settings in the Context of the Novel Coronavirus (2019-nCoV) Outbreak. Available online: https://www.who.int/docs/default-source/documents/advice-on-the-use-of-masks-2019-ncov.pdf (accessed on 29 January 2020).
- U.S. Center for Disease Control and Prevention. Recommendation Regarding the Use of Cloth Face Coverings, Especially in Areas of Significant Community-Based Transmission. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/cloth-face-cover.html (accessed on 3 April 2020).
- World Health Organization. Advice on the Use of Masks in the Context of COVID-19. Available online: https://apps.who.int/iris/bitstream/handle/10665/331693/WHO-2019-nCov-IPC_Masks-2020.3-eng.pdf?sequence=1&isAllowed=y (accessed on 6 April 2020).
- Korea Customs Service. Trade Statistics. Available online: https://unipass.customs.go.kr/ets/index_eng.do (accessed on 13 May 2020).
- Bank of Korea. Economic Statistics System. Available online: https://ecos.bok.or.kr/flex/EasySearch.jsp (accessed on 13 May 2020).
- World Health Organization. A Strategic Framework for Emergency Preparedness; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Madni, A.M.; Erwin, D.; Sievers, M. Constructing Models for Systems Resilience: Challenges, Concepts, and Formal Methods. Systems 2020, 8, 3. [Google Scholar] [CrossRef]
- Ratnapalan, S.; Uleryk, E. Organizational Learning in Health Care Organization. Systems 2014, 2, 24–33. [Google Scholar] [CrossRef]
- Ham, S.; Choi, W.-J.; Lee, W.; Kang, S.-K. Characteristics of Health Masks Certified by the Ministry of Food and Drug Safety. J. Environ. Health Sci. 2019, 45, 134–141. [Google Scholar] [CrossRef]
- Kyung, S.Y.; Jeong, S.H. Particulate-Matter Related Respiratory Diseases. Tuberc. Respir. Dis. 2020, 83, 116–121. [Google Scholar] [CrossRef]
- U.S. Center for Disease Control and Prevention. NIOSH-Approved Particulate Filtering Facepiece Respirators. 2020. Available online: https://www.cdc.gov/niosh/npptl/topics/respirators/disp_part/default.html (accessed on 16 April 2020).
- Dato, V.M.; Hostler, D.; Hahn, M.E. Simple Respiratory Mask. Emerg. Infect. Dis. 2006, 12, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.; Kim, J.; Lee, S.; Lee, J.; Kim, J.; Tsai, P.; Yoon, C. Comparison of Filtration Efficiency and Pressure Drop in Anti-Yellow Sand Masks, Quarantine Masks, Medical Masks, General Masks, and Handkerchiefs. Aerosol Air Q. Res. 2004, 14, 991–1002. [Google Scholar] [CrossRef]
- European Committee on Standardization, Making Standards for Europe, 6 May 2009. Available online: https://standards.cen.eu/dyn/www/f?p=204:110:0::::FSP_PROJECT:32928&cs=1B0AB06FEB70E43960D46D1198C37CC09 (accessed on 15 April 2020).
- U.S. Food and Drug Administration. N95 Respirators and Surgical Masks (Face Masks). Available online: https://www.fda.gov/medical-devices/personal-protective-equipment-infection-control/n95-respirators-and-surgical-masks-face-masks#s6 (accessed on 20 April 2020).
- UN Comtrade. “UN Comtrade,” United Nations Commodity Trade Statistics Database. 2019. Available online: https://comtrade.un.org/db/default.aspx (accessed on 14 May 2020).
- U.S. Center for Disease Control and Prevention. Summary for Healthcare Facilities: Strategies for Optimizing the Supply of N95 Respirators during the COVID-19 Response. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/checklist-n95-strategy.html (accessed on 6 April 2020).
- KOSIS. Summary of Industry and City & Province. Available online: http://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1KB9001&vw_cd=MT_ZTITLE&list_id=J_20_6&seqNo=&lang_mode=ko&language=kor&obj_var_id=&itm_id=&conn_path=MT_ZTITLE (accessed on 27 March 2020).
- Korea Ministry of Economy and Finance. Mask Supply and Demand Stabilization Measures. Available online: http://www.moef.go.kr/com/synap/synapView.do;jsessionid=7kkTyiOn4kjlqZZHDh1ckLY4.node10?atchFileId=ATCH_000000000013363&fileSn=3 (accessed on 5 March 2020).
- Chuan, K.; Kao, E. Taiwan Approves New Rationing System for Surgical Masks. Available online: https://focustaiwan.tw/society/202002030019 (accessed on 3 February 2020).
- Health Insurance and Review Assessment Service. “HIRA System,” May 2020. Available online: https://www.hira.or.kr/eng/about/08/02/index.html (accessed on 14 May 2020).
- Bradsher, K.; Alderman, L. The World Needs Masks. China Makes Them, but has been Hoarding Them, The New York Times. Available online: https://www.nytimes.com/2020/03/13/business/masks-china-coronavirus.html (accessed on 13 March 2020).
- Zhang, L. Coronavirus: Demand for Face Masks Creates Shortfall for Those in Real Need, 7 February 2020. Available online: https://news.un.org/en/story/2020/02/1056942 (accessed on 12 April 2020).
- World Health Organization. Shortage of Personal Protective Equipment Endangering Health Workers Worldwide, 3 March 2020. Available online: https://www.who.int/news-room/detail/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide (accessed on 12 April 2020).
- Song, J.-Y.; Yun, J.-G.; Noh, J.-Y.; Cheong, H.-J.; Kim, W.-J. Covid-19 in South Korea—Challenges of Subclinical Manifestations. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Villasanta, A. China Hoards PPEs, Blocks Export of Coronavirus Masks: This Is ‘Considered First-Degree Murder’. Available online: https://www.ibtimes.com/china-hoards-ppes-blocks-export-coronavirus-masks-considered-first-degree-murder-2953130 (accessed on 15 April 2020).
- Kwai, I. How a Pharmacy Handles Mask Hoarders and Coronavirus Fears. Available online: https://www.nytimes.com/2020/02/18/world/asia/mask-hoarders-coronavirus-pharmacy.html (accessed on 18 February 2020).
- Kang, S.-Y. China Expands Mask Production and Exports, but...It’s Hard to Meet the Demand in Korea. Available online: http://www.newspim.com/news/view/20200303000784 (accessed on 3 March 2020).
- Jin, Y.Z. Responding to the Global “Mask Shortage”: China, the United States and Japan have Made a Big Hit on Their Capacity. Available online: https://finance.sina.com.cn/chanjing/cyxw/2020-03-03/doc-iimxxstf5939393.shtml (accessed on 3 March 2020).
- Korea Foods and Drug Administration. Announcement of the Current Status of Health Mask Production. Available online: https://www.mfds.go.kr/brd/m_99/view.do?seq=43965&srchFr=&srchTo=&srchWord=&srchTp=&itm_seq_1=0&itm_seq_2=0&multi_itm_seq=0&company_cd=&company_nm=&page=1 (accessed on 18 February 2020).
- Korea Law Information Center. Emergency Demand and Supply Stabilization Measures of Mask and Hand Sanitizer. Available online: http://www.law.go.kr/admRulSc.do?tabMenuId=tab133&eventGubun=060103&query=%EB%A7%88%EC%8A%A4%ED%81%AC+%EB%B0%8F+%EC%86%90%EC%86%8C%EB%8F%85%EC%A0%9C+%EA%B8%B4%EA%B8%89%EC%88%98%EA%B8%89%EC%A1%B0%EC%A0%95%EC%A1%B0%EC%B9%98#J595633 (accessed on 6 March 2020).
- Korea Legislation Research Institute. Labor Standards Act. Available online: https://elaw.klri.re.kr/eng_service/lawView.do?hseq=50313&lang=ENG (accessed on 4 September 2019).
- Yonhap, Scientists Develop Reusable Face Mask Filter. Available online: https://www.koreatimes.co.kr/www/nation/2020/03/119_286296.html (accessed on 17 March 2020).
- Kwon, Y.-T.; Ryu, S.H.; Shin, J.W.; Yeo, W.-H.; Chao, Y.-H. Electrospun CuS/PVP Nanowires and Superior Near-Infrared Filtration Efficiency for Thermal Shielding Applications. ACS Appl. Mater. Interfaces 2019, 11, 6575–6580. [Google Scholar] [CrossRef] [PubMed]
- Oh, M.H. Mask Prices are Up To 27.2% Higher Per Unit than They Were Two Weeks Ago. Available online: https://www.khanews.com/news/articleView.html?idxno=200901 (accessed on 18 February 2020).
- Korea Law Translation Center, Korea Price Stabilization Act. Available online: https://elaw.klri.re.kr/kor_service/lawView.do?hseq=22059&lang=ENG (accessed on 27 January 2012).
- Korea Ministry of Finance and Economy. Price Structure of Public Mask; Korea Ministry of Finance and Economy: Seoul, Korea, 2020.
- Korea Ministry of Food and Drug Safety. New and Notice; Korea Ministry of Food and Drug Safety: Seoul, Korea, 2020.
- The Ministry of Economy and Finance, Price Structure of Public Mask Supply Rights. Available online: https://www.mfds.go.kr/brd/m_99/view.do?seq=44004&srchFr=&srchTo=&srchWord=&srchTp=&itm_seq_1=0&itm_seq_2=0&multi_itm_seq=0&company_cd=&company_nm=&page=1# (accessed on 9 March 2020).
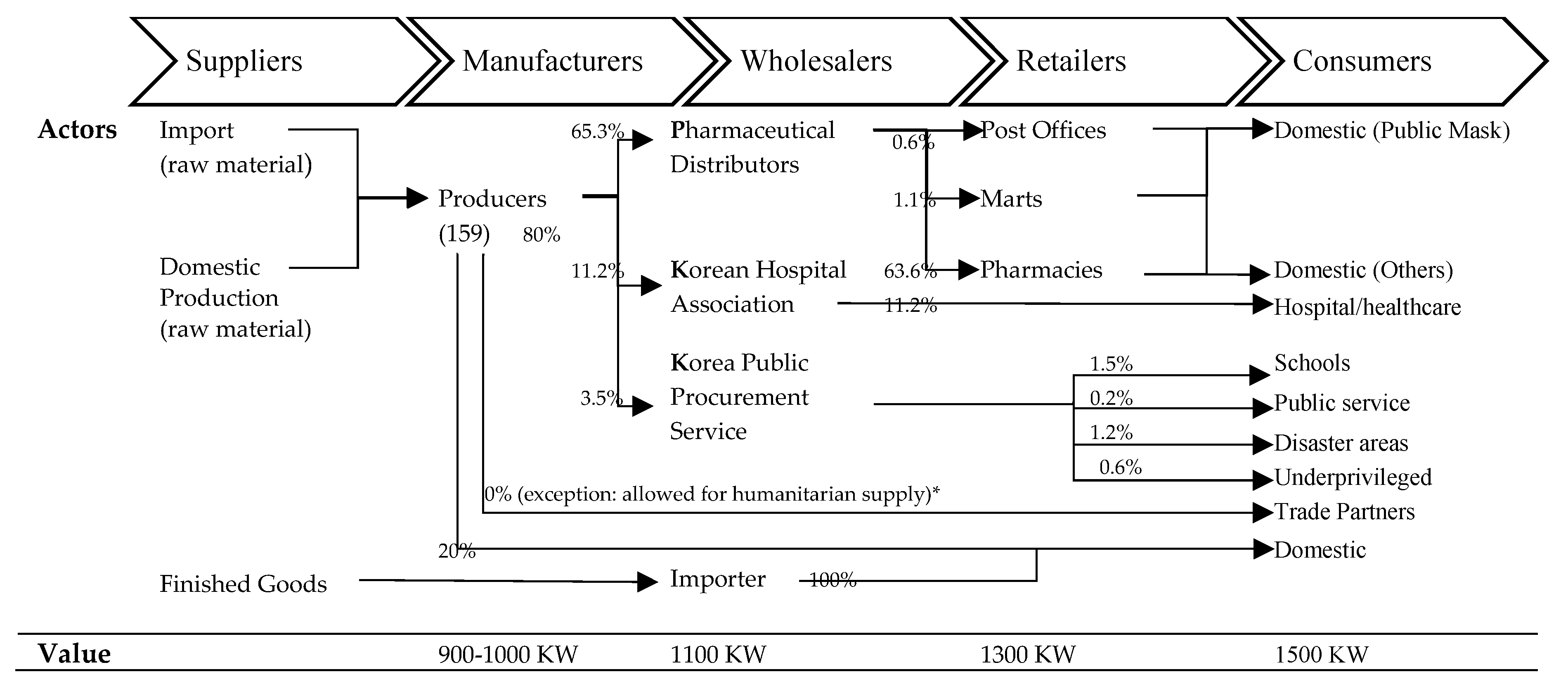
- Yul, L. Mask Distributors Receive 900 to 1000 Won and Supply 1100 Won to Pharmacies. Available online: https://www.yna.co.kr/view/AKR20200309001500002 (accessed on 9 March 2020).
- Public Procurement Service, Policy Briefing. Available online: Pps.go.kr/bbs/selectBoard.do?boardSeqNo=3060&pageIndex=1&boardId=PPS093 (accessed on 6 March 2020).
- Swamidass, P. (Ed.) Chase Strategy for Capacity Planning. In Encyclopedia of Production and Manufacturing Management; Springer: Boston, MA, USA, 2000. [Google Scholar]
- Martell, A.; Warburton, M. Millions of Masks Stockpiled in Canada’s Ontario Expired before Coronavirus Hit; Reuters: London, UK, 2020. [Google Scholar]
- Esbitt, D. The Strategic National Stockpile: Roles and Responsibilities of Health Care Professionals for Receiving the Stockpile Assets. Dis. Manag. Response 2003, 1, 68–70. [Google Scholar] [CrossRef]
- Malatino, E.M. Strategic National Stockpile: Overview and Ventilator Assets. Respir. Care 2008, 53, 91–95. [Google Scholar] [PubMed]
- Dimitrov, N.; Goll, S.; Hupert, N.; Pourbohloul, B.; Meyers, L. Optimizing Tactics for Use of the U.S. Antiviral Strategic National Stockpile for Pandemic Influenza. PLoS ONE 2011, 6, 1–10. [Google Scholar] [CrossRef]
- Dasaklis, T.; Pappis, C.; Rachaniotis, N. Epidemics Control and Logistics Operations: A Review. Int. J. Prod. Econ. 2012, 393–410. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. About the Strategic National Stockpile. Available online: https://www.phe.gov/about/sns/Pages/about.aspx (accessed on 12 September 2019).
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N. Engl. J. Med. 2020, 1–9. [Google Scholar] [CrossRef]
- National Research Council of the National Academies. Chapter 3: Emergency Management Framework; The National Academies Press: Washington, DC, USA, 2007. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Applications | Non-Woven | Woven |
|---|---|---|
| Industrial products | Respirators Single-use, disposable respiratory | |
| Medical products | Surgical masks/Dental masks Veterinary masks/Procedure masks Medical respirator | Cloth surgical face masks |
| Personal products | Healthcare masks | Cloth masks |
| Type | Korea | China | U.S.A. | Europe | Filter Performance | |||
|---|---|---|---|---|---|---|---|---|
| Certification Body | MFDS | KOSHA | SAC | NIOSH | NIOSH and FDA | CEN | Airborne particles (efficiency) | |
| Standards | KFDA No. 2009-6 | KMOEL—2017-64 | GB2626-2006 | NIOSH-42CFR84 | FDA-21 CFR 878.4040 and CDC-NIOSH-42 CFR84 | EN 149:2001 | ||
| Oily particle filtration | Yes | Yes | No | No | Yes | Yes | No | |
| Type 1 | KF80 (0.6 μm) | 2nd Class (0.4 μm) | FFP1 (0.3 μm) | ≥80% | ||||
| Type 2 | KN90 (0.3 μm) | ≥90% | ||||||
| Type 3 | KF94 (0.4 μm) | 1st Class (0.4 μm) | KN95 (0.3 μm) | N95 (0.3 μm) | R95 (0.3 μm) | Surgical N95 | FFP2 (0.3 μm) | ≥94–95% |
| Type 4 | KF99 (0.4 μm) | Special Class (0.4 μm) | KN99 (0.3 μm) | N99 (0.3 μm) | R99 (0.3 μm) | FFP3 (0.3 μm) | ≥99% | |
| Type 5 | N100 (0.3 μm) | R100 (0.3 μm) | ≥99.95% | |||||
| Countries | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | Rank | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| U.S.A. | 2688 | 2976 | 3164 | 3230 | 3422 | 3735 | 3879 | 4019 | 4311 | 34.3% | 1 |
| Japan | 991 | 1109 | 1171 | 1176 | 1155 | 1140 | 1140 | 1191 | 1261 | 10.0% | 2 |
| Germany | 726 | 852 | 734 | 771 | 873 | 822 | 875 | 949 | 1,057 | 8.4% | 3 |
| France | 320 | 378 | 369 | 367 | 407 | 437 | 444 | 462 | 529 | 4.2% | 4 |
| U.K. | 279 | 266 | 259 | 283 | 352 | 357 | 351 | 352 | 384 | 3.1% | 5 |
| Mexico | 218 | 256 | 275 | 318 | 353 | 281 | 299 | 357 | 370 | 2.9% | 6 |
| China | 228 | 233 | 222 | 268 | 279 | 267 | 262 | 300 | 343 | 2.7% | 7 |
| The Netherlands | 174 | 212 | 193 | 195 | 237 | 222 | 239 | 289 | 328 | 2.6% | 8 |
| Australia | 153 | 159 | 183 | 197 | 218 | 232 | 240 | 269 | 292 | 2.3% | 9 |
| Canada | 211 | 225 | 246 | 260 | 275 | 254 | 247 | 256 | 263 | 2.1% | 10 |
| Poland | 183 | 172 | 198 | 244 | 282 | 286 | 340 | 277 | 260 | 2.1% | 11 |
| Italy | 210 | 239 | 205 | 224 | 240 | 214 | 212 | 223 | 247 | 2.0% | 12 |
| Korea | 73 | 113 | 112 | 125 | 140 | 162 | 156 | 183 | 234 | 1.9% | 13 |
| Spain | 208 | 200 | 123 | 115 | 142 | 161 | 154 | 178 | 201 | 1.6% | 14 |
| Belgium | 133 | 151 | 134 | 142 | 148 | 136 | 154 | 159 | 174 | 1.4% | 15 |
| Switzerland | 116 | 128 | 122 | 129 | 155 | 142 | 151 | 155 | 166 | 1.3% | 16 |
| Russian Federation | 84 | 119 | 149 | 155 | 147 | 90 | 133 | 112 | 132 | 1.0% | 17 |
| Austria | 75 | 92 | 88 | 101 | 112 | 101 | 108 | 114 | 129 | 1.0% | 18 |
| Sweden | 88 | 104 | 101 | 105 | 113 | 108 | 96 | 107 | 122 | 1.0% | 19 |
| Czechia | 66 | 94 | 94 | 85 | 103 | 95 | 99 | 114 | 122 | 1.0% | 20 |
| Others | 1004 | 1129 | 1204 | 1305 | 1441 | 1411 | 1465 | 1558 | 1658 | 13.2% | |
| World Total | 8229 | 9208 | 9344 | 9795 | 10,594 | 10,653 | 11,043 | 11,621 | 12,586 | 100% | |
| Exporter | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | Rank | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| China | 2940 | 3318 | 3675 | 4173 | 4605 | 4820 | 4569 | 4789 | 5304 | 45.3% | 1 |
| Germany | 474 | 572 | 557 | 607 | 748 | 704 | 720 | 767 | 862 | 7.4% | 2 |
| U.S.A. | 516 | 544 | 576 | 677 | 689 | 660 | 661 | 676 | 678 | 5.8% | 3 |
| Vietnam | 106 | 162 | 259 | 339 | 475 | 554 | 526 | 484 | 546 | 4.7% | 4 |
| Mexico | 345 | 383 | 377 | 470 | 510 | 500 | 499 | 529 | 514 | 4.4% | 5 |
| India | 216 | 251 | 265 | 365 | 338 | 402 | 519 | 603 | 473 | 4.0% | 6 |
| The Netherlands | 150 | 208 | 146 | 191 | 202 | 185 | 217 | 269 | 311 | 2.7% | 7 |
| Morocco | 86 | 137 | 91 | 136 | 201 | 218 | 289 | 255 | 229 | 2.0% | 8 |
| France | 185 | 191 | 179 | 190 | 201 | 168 | 177 | 183 | 229 | 2.0% | 9 |
| Poland | 115 | 116 | 106 | 115 | 126 | 122 | 141 | 157 | 227 | 1.9% | 10 |
| U.K. | 181 | 156 | 158 | 184 | 208 | 187 | 155 | 156 | 179 | 1.5% | 11 |
| Romania | 79 | 87 | 115 | 134 | 136 | 123 | 122 | 142 | 162 | 1.4% | 12 |
| Canada | 79 | 87 | 115 | 134 | 136 | 123 | 122 | 142 | 162 | 1.4% | 13 |
| Belgium | 77 | 86 | 84 | 86 | 95 | 91 | 141 | 144 | 143 | 1.2% | 14 |
| Japan | 103 | 114 | 99 | 105 | 99 | 98 | 113 | 130 | 138 | 1.2% | 15 |
| Italy | 88 | 84 | 76 | 82 | 78 | 78 | 106 | 112 | 115 | 1.0% | 16 |
| Turkey | 88 | 84 | 76 | 82 | 78 | 78 | 106 | 112 | 115 | 1.0% | 17 |
| Korea | 78 | 82 | 75 | 93 | 113 | 95 | 90 | 94 | 108 | 0.9% | 18 |
| Czechia | 29 | 31 | 38 | 50 | 65 | 61 | 74 | 90 | 106 | 0.9% | 19 |
| Sweden | 86 | 95 | 90 | 104 | 100 | 92 | 89 | 103 | 105 | 0.9% | 20 |
| Others | 816 | 931 | 993 | 1064 | 1195 | 1076 | 1137 | 1213 | 1112 | 9.5% | |
| World Total | 6750 | 7625 | 8062 | 9277 | 10,298 | 10,345 | 10,485 | 11,049 | 11,713 | 100% | |
| Prepare | Respond and Recover | |
|---|---|---|
| Capacity |
|
|
| Governance |
|
|
| Resources |
|
|
| Inventory Management |
|
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, E.; Chen, Y.-Y.; McDonald, M.; O’Neill, E. Dynamic Response Systems of Healthcare Mask Production to COVID-19: A Case Study of Korea. Systems 2020, 8, 18. https://doi.org/10.3390/systems8020018
Lee E, Chen Y-Y, McDonald M, O’Neill E. Dynamic Response Systems of Healthcare Mask Production to COVID-19: A Case Study of Korea. Systems. 2020; 8(2):18. https://doi.org/10.3390/systems8020018
Chicago/Turabian StyleLee, EunSu, Yi-Yu Chen, Melanie McDonald, and Erin O’Neill. 2020. "Dynamic Response Systems of Healthcare Mask Production to COVID-19: A Case Study of Korea" Systems 8, no. 2: 18. https://doi.org/10.3390/systems8020018
APA StyleLee, E., Chen, Y.-Y., McDonald, M., & O’Neill, E. (2020). Dynamic Response Systems of Healthcare Mask Production to COVID-19: A Case Study of Korea. Systems, 8(2), 18. https://doi.org/10.3390/systems8020018