
Effects of Aquatic Training in Children with Autism Spectrum Disorder

 ,
, 
 , ,
, ,  , and
, and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
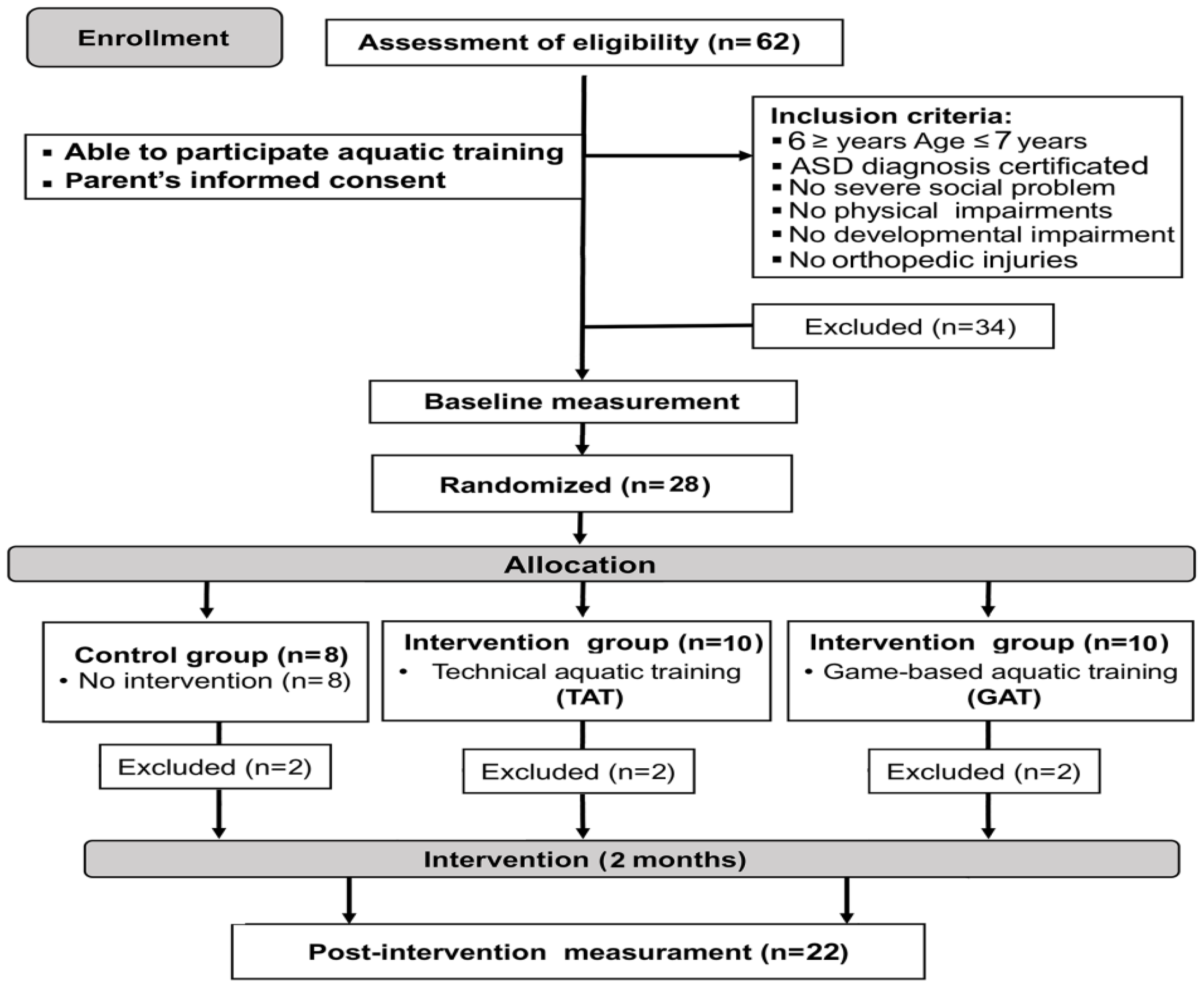
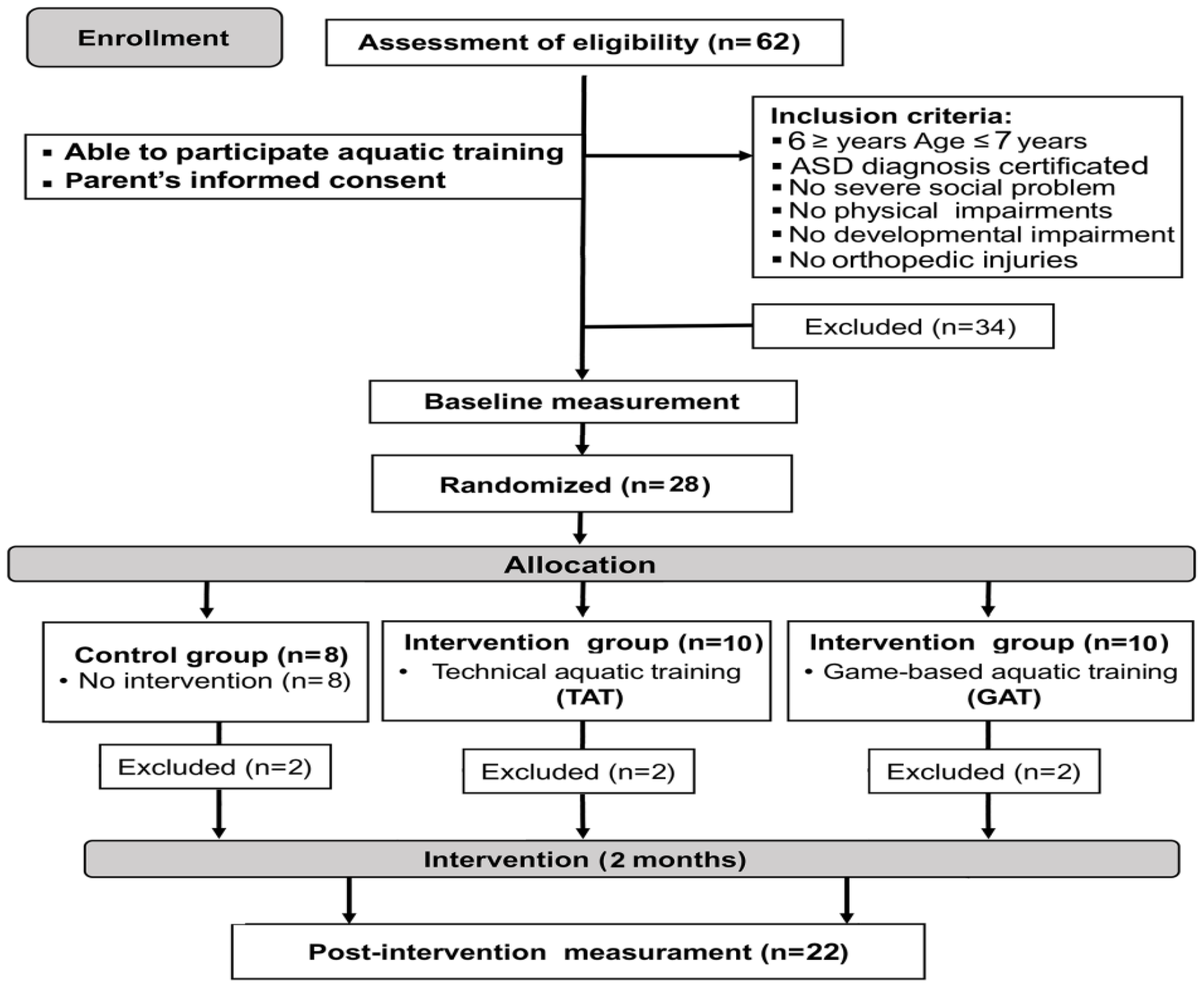
2.1. Study Design
2.2. Participants
2.3. Procedures
2.3.1. Anthropometric Measurements
2.3.2. Assessment of Gross Motor Skills
2.3.3. Assessment of Stereotyped Behavior
2.3.4. Assessment of Emotional Regulation
2.4. Training Programs
2.5. Statistical Analysis
3. Results
3.1. Gross Motor Skills
3.2. Emotion Regulation
3.3. Stereotypy Behavior
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, TX, USA, 2013. [Google Scholar] [CrossRef]
- Alesi, M.; Battaglia, G.; Roccella, M.; Testa, D.; Palma, A.; Pepi, A. Improvement of gross motor and cognitive abilities by an exercise training program: Three case reports. Neuropsychiatr. Dis. Treat. 2014, 10, 479–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fong, S.S.; Tsang, W.W.; Ng, G.Y. Taekwondo training improves sensory organization and balance control in children with developmental coordination disorder: A randomized controlled trial. Res. Dev. Disabil. 2012, 33, 85–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fragala-Pinkham, M.A.; Haley, S.M.; O’Neil, M.E. Group swimming and aquatic exercise programme for children with autism spectrum disorders: A pilot study. Dev. Neurorehabilit. 2011, 14, 230–241. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Vasques, A.T.; Lamonica, D.A. Motor, linguistic, personal, and social aspects of children with Down syndrome. J. Appl. Oral Sci. 2015, 23, 424–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Battaglia, G.; Agrò, G.; Cataldon, P.; Palma, A.; Alesi, M. Influence of a specific aquatic program on social and gross motor skills in adolescents with autism spectrum disorders: Three case reports. J. Funct. Morphol. Kinesiol. 2019, 4, 27. [Google Scholar] [CrossRef] [Green Version]
- Gabriels, R.L.; Agnew, J.A.; Beresford, C.; Morrow, M.A.; Mesibov, G.; Wamboldt, M. Improving psychiatric hospital care for pediatric patients with autism spectrum disorders and intellectual disabilities. Autism Res. Treat. 2012, 2012, 685053. [Google Scholar] [CrossRef]
- Pitetti, K.H.; Rendoff, A.D.; Grover, T.; Beets, M.W. The efficacy of a 9-month treadmill walking program on the exercise capacity and weight reduction for adolescents with severe autism. J. Autism Dev. Disord. 2007, 37, 997–1006. [Google Scholar] [CrossRef]
- Green, D.; Charman, T.; Pickles, A.; Chandler, S.; Loucas, T.; Simono, E.; Baird, G. Impairment in movement skills of children with autistic spectrum disorders. Dev. Med. Child Neurol. 2009, 51, 311–316. [Google Scholar] [CrossRef]
- Pusponegoro, H.D.; Efar, P.; Soedjatmiko; Soebadi, A.; Firmansyah, A.; Chen, H.J.; Hung, K.L. Gross Motor Profile, and Its Association with Socialization Skills in Children with Autism Spectrum Disorders. Pediatr. Neonatol. 2016, 57, 501–507. [Google Scholar] [CrossRef] [Green Version]
- Bandini, L.G.; Gleason, J.; Curtin, C.; Lividini, K.; Anderson, S.E.; Cermak, S.A.; Maslin, M.; Must, A. Comparison of physical activity between children with autism spectrum disorders and typically developing children. Autism 2013, 17, 44–54. [Google Scholar] [CrossRef] [Green Version]
- Siaperas, P.; Ring, H.A.; McAllister, C.J.; Henderson, S.; Barnett, A.; Watson, P.; Holland, A.J. Atypical movement performance and sensory integration in Asperger’s syndrome. J. Autism Dev. Disord. 2012, 42, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Gregor, S.; Bruni, N.; Grkinic, P.; Schwarz, L.; McDonald, A.; Thille, P.; Gabison, S.; Gibson, B.; Jachyra, P. Parents’ perspectives of physical activity participation among Canadian adolescents with autism spectrum disorder. Res. Autism Spectr. Disord. 2018, 48, 53–62. [Google Scholar] [CrossRef]
- Zachor, D.A.; Vardi, S.; Baron-Eitan, S.; Brodai-Meir, I.; Ginossar, N.; Ben-Itzchak, E. The effectiveness of an outdoor adventure programmed for young children with autism spectrum disorder: A controlled study. Dev. Med. Child Neurol. 2017, 59, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Yarimkaya, E.; Ilhan, E.L.; Karasu, N. An investigation of the changes in the communication skills of an individual with autism spectrum disorder participating in peer mediated adapted physical activities. Ank. Üniv. Eğit. Bilimleri Fak. Özel Eğit. Dergisi. 2017, 18, 225–252. [Google Scholar]
- Gabriels, R.; Pan, Z.; Dechant, B.; Agnew, J.A.; Brim, N.; Mesibov, G. Randomized controlled trial of therapeutic horseback riding in children and adolescents with autism spectrum disorder. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 541–549. [Google Scholar] [CrossRef] [Green Version]
- Bahrami, F.A.; Movahedi, A.; Marandi, S.M.; Abedi, A. Kata techniques training consistently decreases stereotypy in children with autism spectrum disorder. Res. Dev. Disabil. 2012, 33, 1183–1193. [Google Scholar] [CrossRef]
- Sowa, M.; Meulenbroek, R. Effects of physical exercise on autism spectrum disorders: A meta-analysis. Res. Autism Spectr. Disord. 2012, 6, 46–57. [Google Scholar] [CrossRef]
- Groff, D.; Lundberg, N.; Zabriskie, R. Influence of adapted sport on quality of life: Perceptions of athletes with cerebral palsy. Disabil. Rehabil. 2009, 31, 318–326. [Google Scholar] [CrossRef]
- Bremer, E.; Crozier, M.; Lloyd, M. A systematic review of the behavioral outcomes following exercise interventions for children and youth with autism spectrum disorder. Autism 2016, 20, 899–915. [Google Scholar] [CrossRef]
- Mortimer, R.; Privopoulos, M.; Kumar, S. The effectiveness of hydrotherapy in the treatment of social and behavioral aspects of children with autism spectrum disorders: A systematic review. J. Multidiscip. Healthc. 2014, 7, 93–104. [Google Scholar]
- Ansari, S.; Hosseinkhanzadeh, A.A.; AdibSaber, F.; Shojaei, M.; Daneshfar, A. The Effects of Aquatic Versus Kata Techniques Training on Static and Dynamic Balance in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2021, 51, 3180–3186. [Google Scholar] [CrossRef] [PubMed]
- Caputo, G.; Ippolito, G.; Sentenza, L.; Muzio, M.R.; Salzano, S.; Conson, M. Effectiveness of a multisystem aquatic therapy for children with autism spectrum disorders. J. Autism Dev. Disord. 2018, 48, 1945–1956. [Google Scholar] [CrossRef]
- Pan, C.Y. Effects of water exercise swimming program on aquatic skills and social behaviors in children with autism spectrum disorders. Autism 2010, 14, 9–28. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.Y. The efficacy of an aquatic program on physical fitness and aquatic skills in children with and without autism spectrum disorders. Res. Autism Spectr. Disord. 2011, 5, 657–665. [Google Scholar] [CrossRef]
- Rogers, L.; Hemmeter, M.L.; Wolery, M. Using a constant time delay procedure to teach foundational swimming skills to children with autism. Top. Early Child. Spec. Educ. 2010, 30, 102–111. [Google Scholar] [CrossRef]
- Yilmaz, I.; Yanarda, M.; Birkan, B.; Bumin, G. Effects of swimming training on physical fitness and water orientation in autism. Pediatr. Int. 2004, 46, 624–626. [Google Scholar] [CrossRef]
- Vonder Hulls, D.S.; Walker, L.K.; Powell, J.M. Clinicians’ perceptions of the benefits of aquatic therapy for young children with autism: A preliminary study. Phys. Occup. Ther. Pediatr. 2006, 26, 13–22. [Google Scholar] [CrossRef]
- World Medical Association. Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Schopler, E.; Reichler, R.I.; Renner, B.R. The Childhood Autism Rating Scale (CARS) for Diagnostic Screening and Classification in Autism; Irvington: New York, NY, USA, 1993. [Google Scholar]
- Wechsler, D. Wechsler Intelligence Scale for Children, 4th ed.; Psychological Corporation: San Antonio, TX, USA, 2003. [Google Scholar]
- Ulrich, D.A. Test of Gross Motor Development 2: Examiner’s Manual, 2nd ed.; Pro-Ed: Austin, TX, USA, 2000. [Google Scholar]
- Gilliam, J.E. Gilliam Autism Rating Scale 2, 2nd ed.; Pro-Ed: Austin, TX, USA, 2006. [Google Scholar]
- Worley, J.; Matson, J. Diagnostic instruments for the core features of ASD. In International Handbook of Autism and Pervasive Developmental Disorders; Matson, J.L., Sturmey, P., Eds.; Springer: New York, NY, USA, 2011; Volume 1, pp. 215–231. [Google Scholar]
- Shields, A.; Cicchetti, D. Emotion regulation among school-age children: The development and validation of a new criterion Q-sort scale. Dev. Psychol. 1997, 33, 906–916. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Casey, A.F.; Quenneville-Himbeault, G.; Normore, A.; Davis, H.; Martell, S.G. A therapeutic skating intervention for children with autism spectrum disorder. Pediatr. Phys. Ther. 2015, 27, 170–177. [Google Scholar] [CrossRef]
- Ward, S.C.; Whalon, K.; Rusnak, K.; Wendell, K.; Paschall, N. The association between therapeutic horseback riding and the social communication and sensory reactions of children with autism. J. Autism Dev. Disord. 2013, 43, 2190–2198. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.; Koegel, L.K.; Ashbaugh, K.; Regester, A.; Ence, W.; Smith, W. Physical exercise and individuals with autism spectrum disorders: A systematic review. Res. Autism Spectr. Disord. 2010, 4, 565–576. [Google Scholar] [CrossRef]
- Bass, M.M.; Duchowny, C.A.; Llabre, M.M. The effect of therapeutic horseback riding on social functioning in children with autism. J. Autism Dev. Disord. 2009, 39, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.H.; Pan, C.Y. The effect of peer- and sibling-assisted aquatic program on interaction behaviors and aquatic skills of children with autism spectrum disorders and their peers/siblings. Res. Autism Spectr. Disord. 2012, 6, 1211–1223. [Google Scholar] [CrossRef]
- Ennis, E. The effects of a physical therapy-directed aquatic program on children with autism spectrum disorders. J. Aquat. Phys. Ther. 2011, 19, 4–10. [Google Scholar]
- Bonifacci, P. Children with low motor ability have lower visual-motor integration ability but unaffected perceptual skills. Hum. Mov. Sci. 2004, 23, 157–168. [Google Scholar] [CrossRef]
- Wilson, P.H.; McKenzie, B.E. Information processing deficits associated with developmental coordination disorder: A meta-analysis of research findings. J. Child Psychol. Psychiatry 1998, 39, 829–840. [Google Scholar]
- Sigmundsson, R.; Hopkins, B. Baby swimming: Exploring the effects of early intervention on subsequent motor abilities. Child Care Health Dev. 2009, 36, 428–430. [Google Scholar]
- Ferreira, J.P.; Ghiarone, T.; Júnior, C.R.C.; Furtado, G.E.; Carvalho, H.M.; Machado-Rodrigues, A.M.; Toscano, C.V.A. Effects of physical exercise on the stereotyped behavior of children with autism spectrum disorders. Medicina 2019, 55, 685. [Google Scholar] [CrossRef] [Green Version]
- Watters, R.G.; Watters, W.E. Decreasing self-stimulatory behavior with physical exercise in a group of autistic boys. J. Autism Dev. Disord. 1980, 10, 379–387. [Google Scholar] [CrossRef]

{kind=link}
| TAT (7 B + 1 G) | GAT (8 B) | CONT (5 B + 1 G) | |
|---|---|---|---|
| Age (year) | 6.3 ± 0.5 | 6.4 ± 0.5 | 6.3 ± 0.5 |
| Height (cm) | 113.1 ± 11.3 | 113.2 ± 3.3 | 112.8 ± 2.4 |
| Weight (kg) | 18.7 ± 3.5 | 18.5 ± 2.2 | 18.3 ± 3.2 |
| BMI (kg·m−2) | 14.7 ± 2.8 | 14.4 ± 1.7 | 14.4 ± 2.4 |
| IQ | 83.9 ± 2.1 | 83.4 ± 2.6 | 84.3 ± 1.4 |
| CARS | 35.1 ± 2.0 | 35.9 ± 2.7 | 34.8 ± 2.6 |
| Week | Session | Sets/Repetitions | Aim | Activities/Games |
|---|---|---|---|---|
| 1st | 1 | 6 × 2 |
| Cooperative games/activities (e.g., noodle kick/jump/float, Aqua hot potato, Dinosaur eggs) |
| 2 | 6 × 2 | |||
| 2nd | 3 | 6 × 2 | ||
| 4 | 6 × 2 | |||
| 3rd | 5 | 7 × 2 | Cooperative games/activities (e.g., hula-hoop swimming, throwing, and catching the ball, a star fish is born) | |
| 6 | 7 × 2 | |||
| 4th | 7 | 7 × 2 | ||
| 8 | 7 × 2 | |||
| 5th | 9 | 8 × 2 | Cooperative and fun games (e.g., circle tag, ball hoop and block, boogie-woogie) | |
| 10 | 8 × 2 | |||
| 6th | 11 | 8 × 2 | ||
| 12 | 8 × 2 | |||
| 7th | 13 | 6 × 2 | Cooperative and fun games (e.g., Octopus tag, water polo) | |
| 14 | 6 × 2 | |||
| 8th | 15 | 6 × 2 | ||
| 16 | 6 × 2 |
| Variables | Group | T1 | T2 | ES | CI 95% |
|---|---|---|---|---|---|
| LoS scores | TAT | 6.75 ± 1.75 | 11.0 ± 2.0 †,‡ | 2.260 | 3.35–5.15 |
| GAT | 4.0 ± 2.73 | 8.5 ± 2.56 †,‡ | 2.928 | 3.60–5.40 | |
| CONT | 3.8 ± 2.64 | 4.0 ± 1.55 | - | - | |
| CoS scores | TAT | 7.0 ± 3.66 | 13.0 ± 2.33 †,‡ | 1.952 | 4.94–7.06 |
| GAT | 4.38 ± 3.42 | 12.75 ± 3.15 †,‡ | 2.547 | 7.32–9.43 | |
| CONT | 5.5 ± 3.0 | 6.7 ± 3.1 | - | - | |
| EmR scores | TAT | 27.5 ± 3.07 | 28.13 ± 3.0 † | 0.206 | 0.05–1.20 |
| GAT | 27.5 ± 3.07 | 28.63 ± 2.92 † | 0.385 | 0.55–1.70 | |
| CONT | 26.33 ± 2.42 | 27.17 ± 2.4 † | 0.346 | 0.17–1.50 | |
| L/N scores | TAT | 25.5 ± 3.17 | 24.0 ± 3.51 † | 0.455 | 0.45–2.55 |
| GAT | 24.63 ± 3.29 | 23.38 ± 3.29 † | 0.380 | 0.20–2.30 | |
| CONT | 24.5 ± 3.45 | 24.33 ± 3.01 | - | - | |
| Ster scores | TAT | 31.63 ± 5.32 | 28.25 ± 5.37 † | 0.632 | 2.60–4.15 |
| GAT | 34.63 ± 4.53 | 30.63 ± 4.47 † | 0.889 | 3.23–4.77 | |
| CONT | 32.17 ± 3.87 | 30.0 ± 3.69 † | 0.573 | 1.27–3.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marzouki, H.; Soussi, B.; Selmi, O.; Hajji, Y.; Marsigliante, S.; Bouhlel, E.; Muscella, A.; Weiss, K.; Knechtle, B. Effects of Aquatic Training in Children with Autism Spectrum Disorder. Biology 2022, 11, 657. https://doi.org/10.3390/biology11050657
Marzouki H, Soussi B, Selmi O, Hajji Y, Marsigliante S, Bouhlel E, Muscella A, Weiss K, Knechtle B. Effects of Aquatic Training in Children with Autism Spectrum Disorder. Biology. 2022; 11(5):657. https://doi.org/10.3390/biology11050657
Chicago/Turabian StyleMarzouki, Hamza, Badis Soussi, Okba Selmi, Yamina Hajji, Santo Marsigliante, Ezdine Bouhlel, Antonella Muscella, Katja Weiss, and Beat Knechtle. 2022. "Effects of Aquatic Training in Children with Autism Spectrum Disorder" Biology 11, no. 5: 657. https://doi.org/10.3390/biology11050657
APA StyleMarzouki, H., Soussi, B., Selmi, O., Hajji, Y., Marsigliante, S., Bouhlel, E., Muscella, A., Weiss, K., & Knechtle, B. (2022). Effects of Aquatic Training in Children with Autism Spectrum Disorder. Biology, 11(5), 657. https://doi.org/10.3390/biology11050657