
In Vivo Accelerator-Based Boron Neutron Capture Therapy for Spontaneous Tumors in Large Animals: Case Series


 ,
,  ,
, 
 and
and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
- –
- Tumors could not be surgically removed due to high risks of postoperative complications, tumor after recurrence, or with a high likelihood of recurrence;
- –
- A life and quality-of-life expectancy of 3 or more months for follow-up purposes;
- –
- A somatic status adequate to withstand prolonged (2 h) anesthesia during irradiation;
- –
- If the animal has previously received surgical treatment, there should be at least 3 weeks between the end of that treatment and BNCT.
3. Results
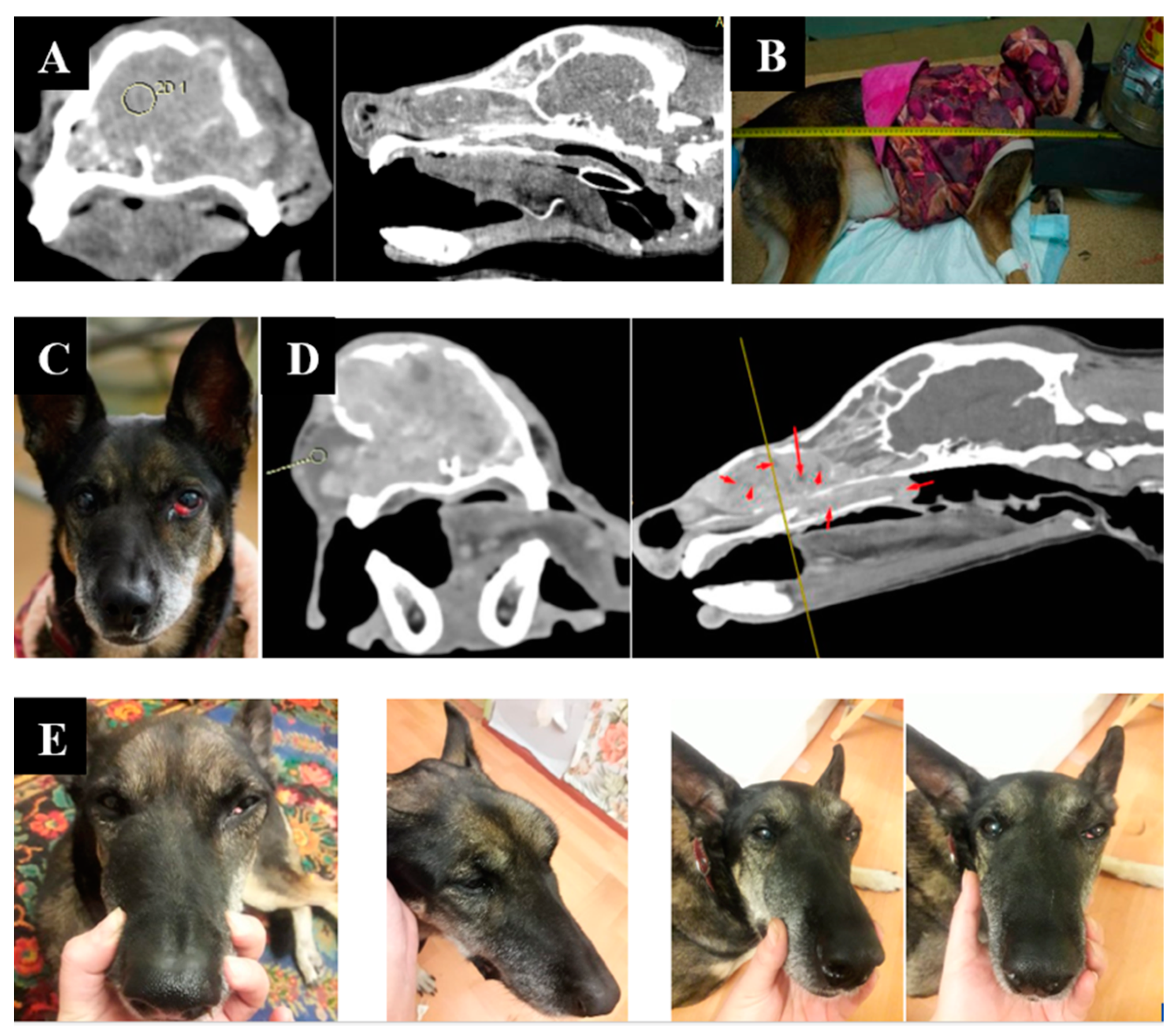
3.1. Case 1
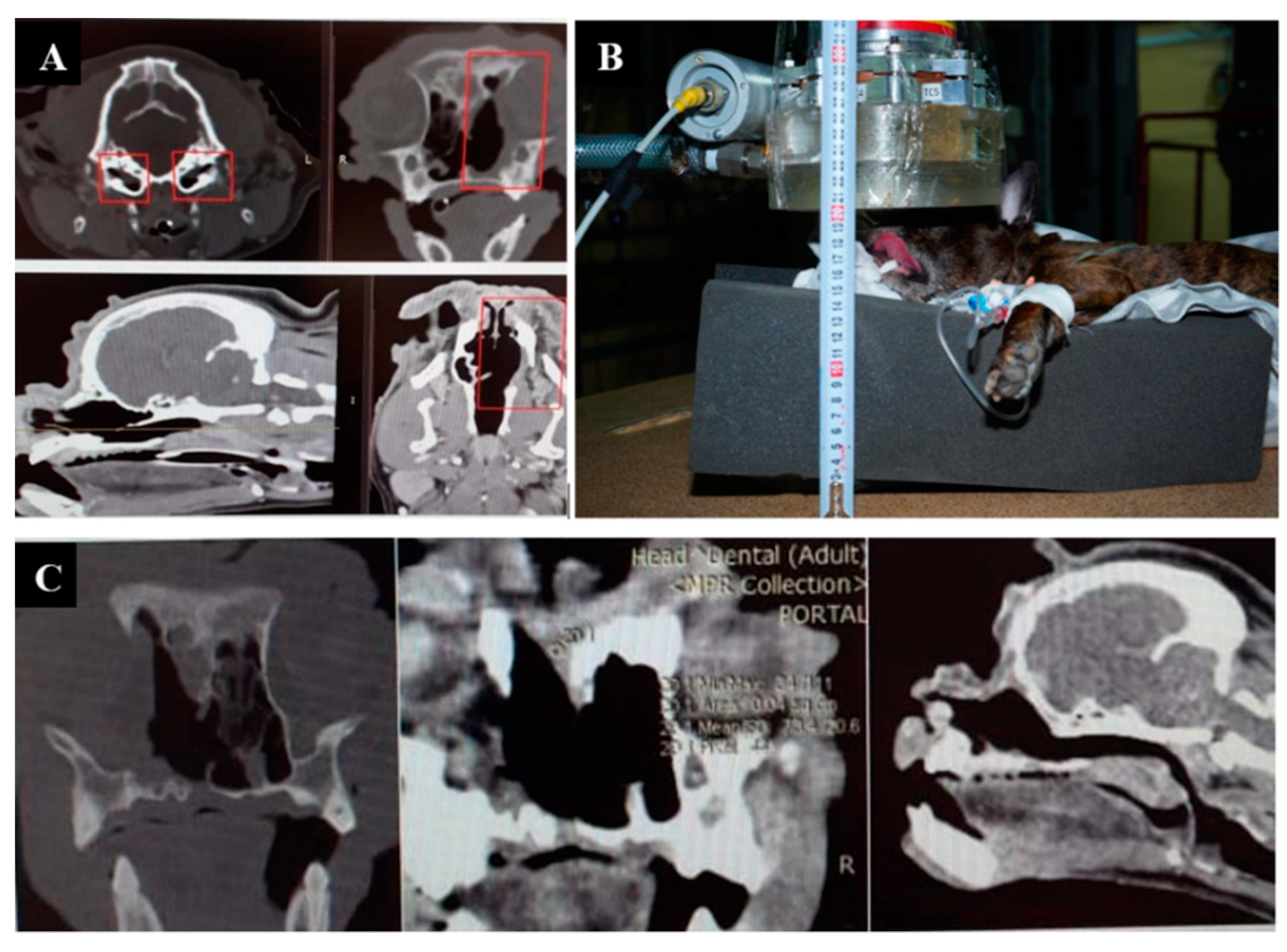
3.2. Case 2
3.3. Case 3
3.4. Case 4
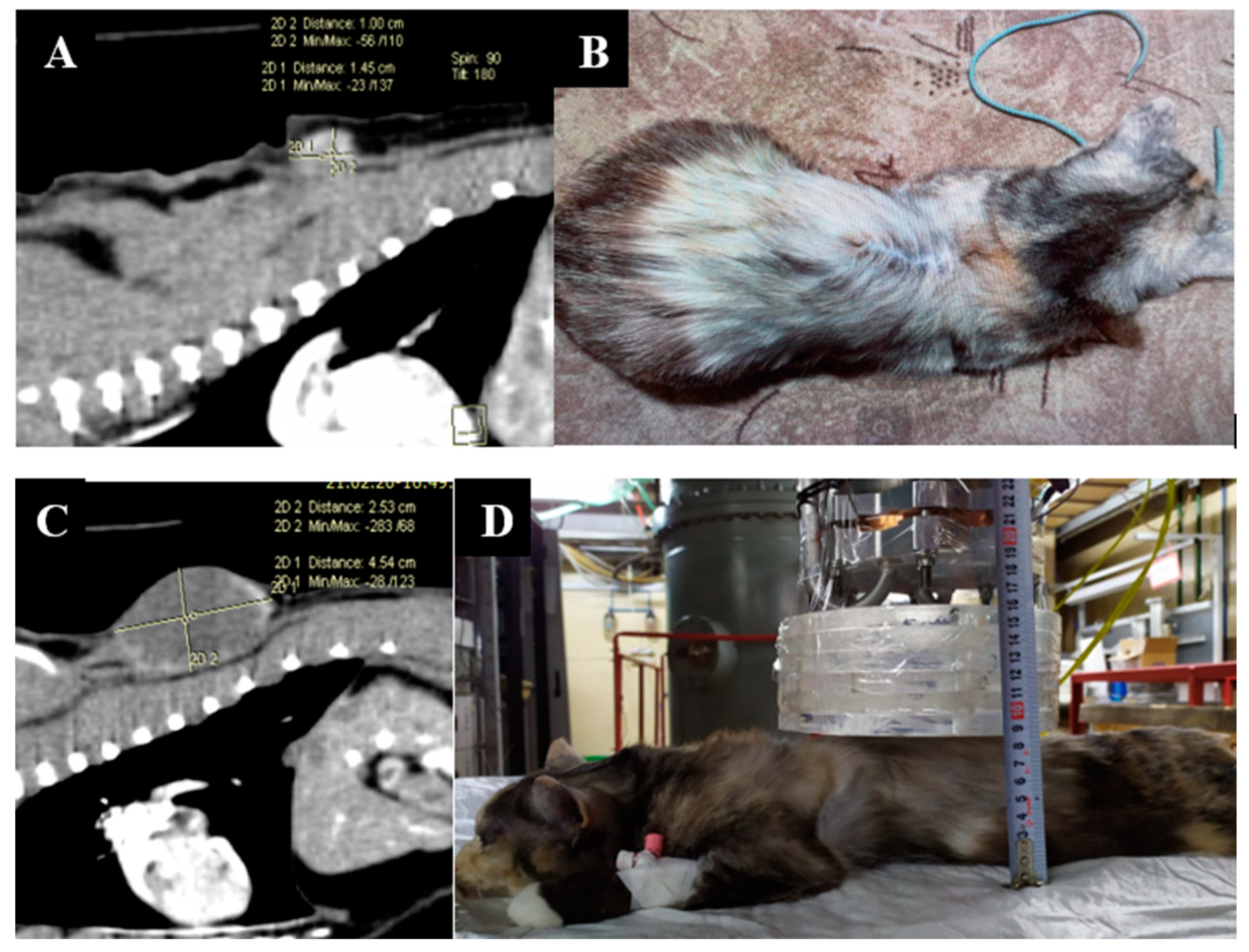
3.5. Case 5
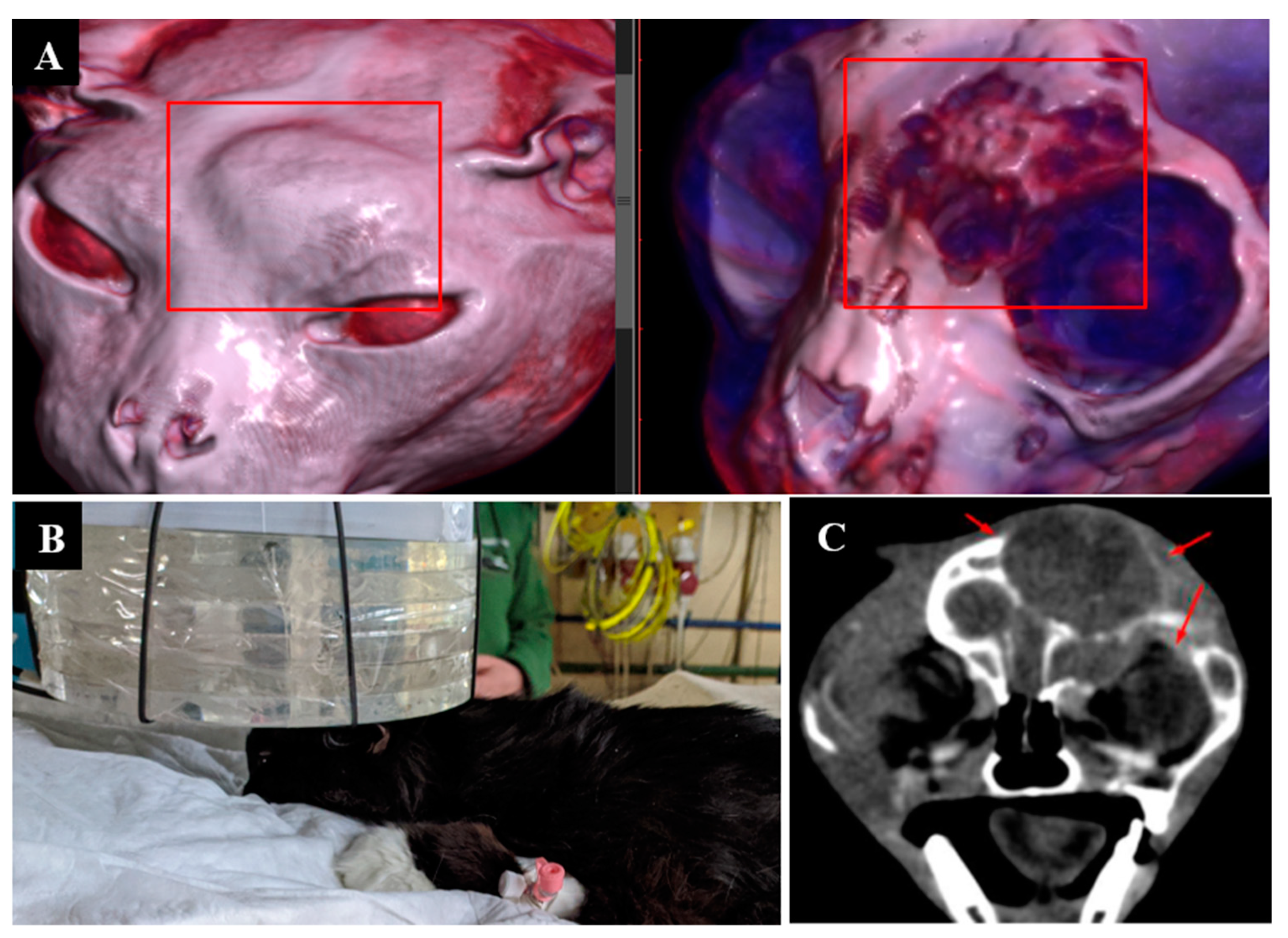
3.6. Case 6
3.7. Case 7
3.8. Case 8
3.9. Case 9
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Locher, G.L. Biological effects and therapeutic possibilities of neutrons. Am. J. Roentgenol. Radium. Ther. 1936, 36, 1–13. [Google Scholar] [CrossRef]
- Sauerwein, W.A.G.; Wittig, A.; Moss, R.; Nakagawa, Y. Neutron Capture Therapy. Principles and Applications; Springer: Berlin/Heidelberg, Germany, 2012; ISBN 978-3-642-31334-9. [Google Scholar]
- Barth, R.F.; Mi, P.; Yang, W. Boron delivery agents for neutron capture therapy of cancer. Cancer Commun. 2018, 38, 35. [Google Scholar] [CrossRef] [PubMed]
- Barth, R.F.; Zhang, Z.; Liu, T. A realistic appraisal of boron neutron capture therapy as a cancer treatment modality. Cancer Commun. 2018, 38, 36. [Google Scholar] [CrossRef]
- Dymova, M.A.; Taskaev, S.Y.; Richter, V.A.; Kuligina, E.V. Boron neutron capture therapy: Current status and future perspectives. Cancer Commun. 2020, 40, 406–421. [Google Scholar] [CrossRef] [PubMed]
- Malouff, T.D.; Seneviratne, D.S.; Ebner, D.K.; Stross, W.C.; Waddle, M.R.; Trifiletti, D.M.; Krishnan, S. Boron neutron capture therapy: A review of clinical applications. Front. Oncol. 2021, 11, 601820. [Google Scholar] [CrossRef]
- Mishima, Y.; Ichihashi, M.; Hatta, S.; Honda, C.; Sasase, A.; Yamamura, K.; Kanda, K.; Kobayashi, T.; Fukuda, H. Selective thermal neutron capture therapy and diagnosis of malignant melanoma: From basic studies to first clinical treatment. Basic Life Sci. 1989, 50, 251–260. [Google Scholar] [CrossRef]
- Nakagawa, Y.; Hatanaka, H. Boron neutron capture therapy. Clinical brain tumor studies. J. Neuro-Oncol. 1997, 33, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Chanana, A.D.; Capala, J.; Chadha, M.; Coderre, J.A.; Diaz, A.Z.; Elowitz, E.H.; Iwai, J.; Joel, D.D.; Liu, H.B.; Ma, R.; et al. Boron neutron capture therapy for glioblastoma multiforme: Interim results from the phase I/II dose-escalation studies. Neurosurgery 1999, 44, 1182–1193. [Google Scholar] [CrossRef] [PubMed]
- Palmer, M.R.; Goorley, J.T.; Kiger, W.S.; Busse, P.M.; Riley, K.J.; Harling, O.K.; Zamenhof, R.G. Treatment planning and dosimetry for the Harvard-MIT Phase I clinical trial of cranial neutron capture therapy. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 1361–1379. [Google Scholar] [CrossRef]
- Busse, P.M.; Harling, O.K.; Palmer, M.R.; Kiger, W.S.; Kaplan, J., 3rd; Kaplan, I.; Chuang, C.F.; Goorley, J.T.; Riley, K.J.; Newton, T.H.; et al. A critical examination of the results from the Harvard-MIT NCT program phase I clinical trial of neutron capture therapy for intracranial disease. J. Neuro-Oncol. 2003, 62, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Joensuu, H.; Kankaanranta, L.; Seppälä, T.; Auterinen, I.; Kallio, M.; Kulvik, M.; Laakso, J.; Vähätalo, J.; Kortesniemi, M.; Kotiluoto, P.; et al. Boron neutron capture therapy of brain tumors: Clinical trials at the finnish facility using boronophenylalanine. J. Neuro-Oncol. 2003, 62, 123–134. [Google Scholar] [CrossRef]
- Yamamoto, T.; Nakai, K.; Kageji, T.; Kumada, H.; Endo, K.; Matsuda, M.; Shibata, Y.; Matsumura, A. Boron neutron capture therapy for newly diagnosed glioblastoma. Radiother. Oncol. 2009, 91, 80–84. [Google Scholar] [CrossRef]
- Yamamoto, T.; Nakai, K.; Tsurubuchi, T.; Matsuda, M.; Shirakawa, M.; Zaboronok, A.; Endo, K.; Matsumura, A. Boron neutron capture therapy for newly diagnosed glioblastoma: A pilot study in Tsukuba. Appl. Radiat. Isot. 2009, 67 (Suppl. 7–8), S25–S26. [Google Scholar] [CrossRef] [PubMed]
- Kiger, W.S.; Lu, X.Q., 3rd; Harling, O.K.; Riley, K.J.; Binns, P.J.; Kaplan, J.; Patel, H.; Zamenhof, R.G.; Shibata, Y.; Kaplan, I.D.; et al. Preliminary treatment planning and dosimetry for a clinical trial of neutron capture therapy using a fission converter epithermal neutron beam. Appl. Radiat. Isot. 2004, 61, 1075–1081. [Google Scholar] [CrossRef] [PubMed]
- Capala, J.; Stenstam, B.H.; Sköld, K.; Rosenschöld, M.A.; Giusti, V.; Persson, C.; Wallin, E.; Brun, A.; Franzen, L.; Carlsson, J.; et al. Boron neutron capture therapy for glioblastoma multiforme: Clinical studies in Sweden. J. Neuro-Oncol. 2003, 62, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Henriksson, R.; Capala, J.; Michanek, A.; Lindahl, S.A.; Salford, L.G.; Franzén, L.; Blomquist, E.; Westlin, J.E.; Bergenheim, A.T.; Swedish Brain Tumour Study Group. Boron neutron capture therapy (BNCT) for glioblastoma multiforme: A phase II study evaluating a prolonged high-dose of boronophenylalanine (BPA). Radiother. Oncol. 2008, 88, 183–191. [Google Scholar] [CrossRef]
- Kawabata, S.; Miyatake, S.; Kuroiwa, T.; Yokoyama, K.; Doi, A.; Iida, K.; Miyata, S.; Nonoguchi, N.; Michiue, H.; Takahashi, M.; et al. Boron neutron capture therapy for newly diagnosed glioblastoma. J. Radiat. Res. 2009, 50, 51–60. [Google Scholar] [CrossRef]
- Miyatake, S.; Kawabata, S.; Hiramatsu, R.; Kuroiwa, T.; Suzuki, M.; Kondo, N.; Ono, K. Boron neutron capture therapy for malignant brain tumors. Neurol. Med.-Chir. 2016, 56, 361–371. [Google Scholar] [CrossRef]
- Miyatake, S.I.; Wanibuchi, M.; Hu, N.; Ono, K. Boron neutron capture therapy for malignant brain tumors. J. Neuro-Oncol. 2020, 149, 1–11. [Google Scholar] [CrossRef]
- Kawabata, S.; Hiramatsu, R.; Kuroiwa, T.; Ono, K.; Miyatake, S.I. Boron neutron capture therapy for recurrent high-grade meningiomas. J. Neurosurg. 2013, 119, 837–844. [Google Scholar] [CrossRef]
- Takeuchi, K.; Kawabata, S.; Hiramatsu, R.; Matsushita, Y.; Tanaka, H.; Sakurai, Y.; Suzuki, M.; Ono, K.; Miyatake, S.I.; Kuroiwa, T. Boron neutron capture therapy for high-grade skull-base meningioma. J. Neurol. Surg. B Skull Base 2018, 79 (Suppl. 4), S322–S327. [Google Scholar] [CrossRef]
- Takai, S.; Wanibuchi, M.; Kawabata, S.; Takeuchi, K.; Sakurai, Y.; Suzuki, M.; Ono, K.; Miyatake, S. Reactor-based boron neutron capture therapy for 44 cases of recurrent and refractory high-grade meningiomas with long-term follow-up. Neuro-Oncology 2022, 24, 90–98. [Google Scholar] [CrossRef]
- Fukuda, H.; Hiratsuka, J.; Honda, C.; Kobayashi, T.; Yoshino, K.; Karashima, H.; Takahashi, J.; Abe, Y.; Kanda, K.; Ichihashi, M. Boron neutron capture therapy of malignant melanoma using 10B-paraboronophenylalanine with special reference to evaluation of radiation dose and damage to the normal skin. Radiat. Res. 1994, 138, 435–442. [Google Scholar] [CrossRef]
- Menéndez, P.R.; Roth, B.M.; Pereira, M.D.; Casal, M.R.; González, S.J.; Feld, D.B.; Santa Cruz, G.A.; Kessler, J.; Longhino, J.; Blaumann, H.; et al. BNCT for skin melanoma in extremities: Updated Argentine clinical results. Appl. Radiat. Isot. 2009, 67 (Suppl. 7–8), S50–S53. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, H.; Hiratsuka, J.; Kobayashi, T.; Sakurai, Y.; Yoshino, K.; Karashima, H.; Turu, K.; Araki, K.; Mishima, Y.; Ichihashi, M. Boron neutron capture therapy (BNCT) for malignant melanoma with special reference to absorbed doses to the normal skin and tumor. Australas Phys. Eng. Sci. Med. 2003, 26, 97–103. [Google Scholar] [CrossRef] [PubMed]
- González, S.J.; Bonomi, M.R.; Santa Cruz, G.A.; Blaumann, H.R.; Calzetta Larrieu, O.A.; Menéndez, P.; Jiménez Rebagliati, R.; Longhino, J.; Feld, D.B.; Dagrosa, M.A.; et al. First BNCT treatment of a skin melanoma in Argentina: Dosimetric analysis and clinical outcome. Appl. Radiat. Isot. 2004, 61, 1101–1105. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, H. Boron Neutron Capture Therapy (BNCT) for cutaneous malignant melanoma using 10B-p-boronophenylalanine (BPA) with special reference to the radiobiological basis and clinical results. Cells 2021, 10, 2881. [Google Scholar] [CrossRef] [PubMed]
- Wittig, A.; Collette, L.; Appelman, K.; Bührmann, S.; Jäckel, M.C.; Jöckel, K.H.; Schmid, K.W.; Ortmann, U.; Moss, R.; Sauerwein, W. EORTC trial 11001: Distribution of two 10B-compounds in patients with squamous cell carcinoma of head and neck, a translational research/phase 1 trial. J. Cell Mol. Med. 2009, 13, 1653–1665. [Google Scholar] [CrossRef]
- Kato, I.; Fujita, Y.; Maruhashi, A.; Kumada, H.; Ohmae, M.; Kirihata, M.; Imahori, Y.; Suzuki, M.; Sakrai, Y.; Sumi, T.; et al. Effectiveness of boron neutron capture therapy for recurrent head and neck malignancies. Appl. Radiat. Isot. 2009, 67 (Suppl. 7–8), S37–S42. [Google Scholar] [CrossRef]
- Kankaanranta, L.; Seppälä, T.; Koivunoro, H.; Saarilahti, K.; Atula, T.; Collan, J.; Salli, E.; Kortesniemi, M.; Uusi-Simola, J.; Välimäki, P.; et al. Boron neutron capture therapy in the treatment of locally recurred head-and-neck cancer: Final analysis of a phase I/II trial. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e67–e75. [Google Scholar] [CrossRef]
- Aihara, T.; Morita, N.; Kamitani, N.; Kumada, H.; Ono, K.; Hiratsuka, J.; Harada, T. Boron neutron capture therapy for advanced salivary gland carcinoma in head and neck. Int. J. Clin. Oncol. 2014, 19, 437–444. [Google Scholar] [CrossRef]
- Aihara, T.; Morita, N.; Kamitani, N.; Kumada, H.; Ono, K.; Hiratsuka, J.; Harada, T. BNCT for advanced or recurrent head and neck cancer. Appl. Radiat. Isot. 2014, 88, 12–15. [Google Scholar] [CrossRef]
- Suzuki, M.; Kato, I.; Aihara, T.; Hiratsuka, J.; Yoshimura, K.; Niimi, M.; Kimura, Y.; Ariyoshi, Y.; Haginomori, S.; Sakurai, Y.; et al. Boron neutron capture therapy outcomes for advanced or recurrent head and neck cancer. J. Radiat. Res. 2014, 55, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.W.; Chen, Y.W.; Ho, C.Y.; Hsueh Liu, Y.W.; Chou, F.I.; Liu, Y.H.; Liu, H.M.; Peir, J.J.; Jiang, S.H.; Chang, C.W.; et al. Fractionated BNCT for locally recurrent head and neck cancer: Experience from a phase I/II clinical trial at Tsing Hua Open-Pool Reactor. Appl. Radiat. Isot. 2014, 88, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.W.; Liu, Y.H.; Chou, F.I.; Jiang, S.H. Clinical trials for treating recurrent head and neck cancer with boron neutron capture therapy using the Tsing-Hua Open Pool Reactor. Cancer Commun. 2018, 38, 37. [Google Scholar] [CrossRef]
- Suzuki, M.; Sakurai, Y.; Hagiwara, S.; Masunaga, S.; Kinashi, Y.; Nagata, K.; Maruhashi, A.; Kudo, M.; Ono, K. First attempt of boron neutron capture therapy (BNCT) for hepatocellular carcinoma. Jpn. J. Clin. Oncol. 2007, 37, 376–381. [Google Scholar] [CrossRef]
- Yanagie, H.; Higashi, S.; Seguchi, K.; Ikushima, I.; Fujihara, M.; Nonaka, Y.; Oyama, K.; Maruyama, S.; Hatae, R.; Suzuki, M.; et al. Pilot clinical study of boron neutron capture therapy for recurrent hepatic cancer involving the intra-arterial injection of a (10)BSH-containing WOW emulsion. Appl. Radiat. Isot. 2014, 88, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Zonta, A.; Pinelli, T.; Prati, U.; Roveda, L.; Ferrari, C.; Clerici, A.M.; Zonta, C.; Mazzini, G.; Dionigi, P.; Altieri, S.; et al. Extra-corporeal liver BNCT for the treatment of diffuse metastases: What was learned and what is still to be learned. Appl. Radiat. Isot. 2009, 67 (Suppl. 7–8), S67–S75. [Google Scholar] [CrossRef]
- Suzuki, M.; Sakurai, Y.; Masunaga, S.; Kinashi, Y.; Nagata, K.; Maruhashi, A.; Ono, K. A preliminary experimental study of boron neutron capture therapy for malignant tumors spreading in thoracic cavity. Jpn. J. Clin. Oncol. 2007, 37, 245–249. [Google Scholar] [CrossRef]
- Masunaga, S.I.; Sakurai, Y.; Tano, K.; Tanaka, H.; Suzuki, M.; Kondo, N.; Narabayashi, M.; Watanabe, T.; Nakagawa, Y.; Maruhashi, A.; et al. Effect of bevacizumab combined with boron neutron capture therapy on local tumor response and lung metastasis. Exp. Ther. Med. 2014, 8, 291–301. [Google Scholar] [CrossRef]
- Kouri, M.; Kankaanranta, L.; Seppälä, T.; Tervo, L.; Rasilainen, M.; Minn, H.; Eskola, O.; Vähätalo, J.; Paetau, A.; Savolainen, S.; et al. Undifferentiated sinonasal carcinoma may respond to single-fraction boron neutron capture therapy. Radiother. Oncol. 2004, 72, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Kimura, Y.; Ariyoshi, Y.; Shimahara, M.; Miyatake, S.; Kawabata, S.; Ono, K.; Suzuki, M.; Maruhashi, A. Boron neutron capture therapy for recurrent oral cancer and metastasis of cervical lymph node. Appl. Radiat. Isot. 2009, 67 (Suppl. 7–8), S47–S49. [Google Scholar] [CrossRef]
- Nakagawa, Y.; Kageji, T.; Mizobuchi, Y.; Kumada, H.; Nakagawa, Y. Clinical results of BNCT for malignant brain tumors in children. Appl. Radiat. Isot. 2009, 67 (Suppl. 7–8), S27–S30. [Google Scholar] [CrossRef]
- Inoue, M.; Lee, C.M.; Ono, K.; Suzuki, M.; Tokunaga, T.; Sawa, Y.; Okumura, M. Clinical effectiveness of boron neutron capture therapy for a recurrent malignant peripheral nerve sheath tumor in the mediastinum. Clinical effectiveness of boron neutron capture therapy for a recurrent malignant peripheral nerve sheath tumor in the mediastinum. J. Thorac. Oncol. 2010, 5, 2037–2038. [Google Scholar] [CrossRef] [PubMed]
- Haapaniemi, A.; Kankaanranta, L.; Saat, R.; Koivunoro, H.; Saarilahti, K.; Mäkitie, A.; Atula, T.; Joensuu, H. Boron neutron capture therapy in the treatment of recurrent laryngeal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Hiratsuka, J.; Kamitani, N.; Tanaka, R.; Yoden, E.; Tokiya, R.; Suzuki, M.; Barth, R.F.; Ono, K. Boron neutron capture therapy for vulvar melanoma and genital extramammary Paget’s disease with curative responses. Cancer Commun. 2018, 38, 38. [Google Scholar] [CrossRef]
- Omori, M.; Fujiwara, S.; Shimizu, H.; Ikeda, T.; Bito, T.; Suzuki, M.; Masunaga, S.I.; Ono, K.; Nishigori, C. Boron neutron capture therapy using reactor epithermal neutron beams could effectively control in-transit and lymph node metastases originating from a cutaneous malignant melanoma. J. Dermatol. 2018, 45, e90–e91. [Google Scholar] [CrossRef]
- Tsurubuchi, T.; Shirakawa, M.; Kurosawa, W.; Matsumoto, K.; Ubagai, R.; Umishio, H.; Suga, Y.; Yamazaki, J.; Arakawa, A.; Maruyama, Y.; et al. Evaluation of a novel boron-containing α-d-mannopyranoside for BNCT. Cells 2020, 9, 1277. [Google Scholar] [CrossRef]
- Lan, T.L.; Chou, F.I.; Lin, K.H.; Pan, P.S.; Lee, J.C.; Huang, W.S.; Liu, Y.M.; Chao, Y.; Chen, Y.W. Using salvage boron neutron capture therapy (BNCT) for recurrent malignant brain tumors in Taiwan. Appl. Radiat. Isot. 2020, 160, 109105. [Google Scholar] [CrossRef]
- Gadan, M.A.; González, S.J.; Batalla, M.; Olivera, M.S.; Policastro, L.; Sztejnberg, M.L. Application of BNCT to the treatment of HER2+ breast cancer recurrences: Research and developments in Argentina. Appl. Radiat. Isot. 2015, 104, 155–159. [Google Scholar] [CrossRef]
- Schwint, A.E.; Monti Hughes, A.; Garabalino, M.A.; Santa Cruz, G.A.; González, S.J.; Longhino, J.; Provenzano, L.; Oña, P.; Rao, M.; Cantarelli, M.d.l.Á.; et al. Clinical veterinary boron neutron capture therapy (BNCT) studies in dogs with head and neck cancer: Bridging the gap between translational and clinical studies. Biology 2020, 9, 327. [Google Scholar] [CrossRef]
- Zhang, Z.; Liu, T. A review of the development of In-Hospital Neutron Irradiator-1 and boron neutron capture therapy clinical research on malignant melanoma. Ther. Radiol. Oncol. 2018, 2, 49. [Google Scholar] [CrossRef]
- Kawabata, S.; Suzuki, M.; Hirose, K.; Tanaka, H.; Kato, T.; Goto, H.; Narita, Y.; Miyatake, S.I. Accelerator-based BNCT for patients with recurrent glioblastoma: A multicenter phase II study. Neurooncol. Adv. 2021, 3, vdab067. [Google Scholar] [CrossRef] [PubMed]
- Hirose, K.; Konno, A.; Hiratsuka, J.; Yoshimoto, S.; Kato, T.; Ono, K.; Otsuki, N.; Hatazawa, J.; Tanaka, H.; Takayama, K.; et al. Boron neutron capture therapy using cyclotron-based epithermal neutron source and borofalan (10B) for recurrent or locally advanced head and neck cancer (JHN002): An open-label phase II trial. Radiother. Oncol. 2021, 155, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Sumitomo Heavy Industries. Available online: https://www.shi.co.jp/english/info/2019/6kgpsq0000002cez.html (accessed on 21 December 2021).
- Stella Pharma. Available online: https://stella-pharma.co.jp/en/spm-011/ (accessed on 21 December 2021).
- Kumada, H.; Naito, F.; Hasegawa, K.; Kobayashi, H.; Kurihara, T.; Takada, K.; Onishi, T.; Sakurai, H.; Matsumura, A.; Sakae, T. Development of LINAC-based neutron source for boron neutron capture therapy in University of Tsukuba. Plasma Fusion Res. 2018, 13, 2406006. [Google Scholar] [CrossRef]
- Kumada, H.; Tanaka, S.; Naito, F.; Kurihara, T.; Sugimura, T.; Sakurai, H.; Matsumura, A.; Sakae, T. Neutron beam performance of iBNCT as linac-based neutron source for boron neutron capture therapy. E3S Web Conf. 2020, 231, 01003. [Google Scholar] [CrossRef][Green Version]
- National Cancer Center Japan. Available online: https://www.ncc.go.jp/en/publication_report/2019/epoc/epoc18.html (accessed on 21 December 2021).
- Fujimura, A.; Yasui, S.; Igawa, K.; Ueda, A.; Watanabe, K.; Hanafusa, T.; Ichikawa, Y.; Yoshihashi, S.; Tsuchida, K.; Kamiya, A.; et al. In vitro studies to define the cell-surface and intracellular targets of polyarginine-conjugated sodium borocaptate as a potential delivery agent for boron neutron capture therapy. Cells 2020, 9, 2149. [Google Scholar] [CrossRef]
- Neutron Therapeutics. Available online: https://www.neutrontherapeutics.com/news/pr-041819/ (accessed on 21 December 2021).
- Porra, L.; Seppälä, T.; Wendland, L.; Revitzer, H.; Joensuu, H.; Eide, P.; Koivunoro, H.; Smick, N.; Smick, T.; Tenhunen, M. Accelerator-based boron neutron capture therapy facility at the Helsinki University Hospital. Acta Oncol. 2021, 1–5. [Google Scholar] [CrossRef]
- TAE Life Sciences. Available online: https://taelifesciences.com/alphabeam-neutron-system/ (accessed on 21 December 2021).
- Business Wire. Available online: https://www.businesswire.com/news/home/20210926005023/en/TAE-Life-Sciences-Announces-Installation-of-First-Accelerator-based-Neutron-Beam-System-for-Biologically-Targeted-Radiation-Therapy-at-Xiamen-Humanity-Hospital-in-China (accessed on 21 December 2021).
- Chinese Academy of Sciences. China Builds First Accelerator-Based Facility for Boron Neutron Capture Therapy Experiments. Available online: https://english.cas.cn/newsroom/research_news/phys/202008/t20200813_241689.shtml (accessed on 21 December 2021).
- Chinese Academy of Sciences. China’s Radiation Cancer Therapy Facility Starts Cell, Animal Tests. Available online: https://english.cas.cn/newsroom/cas_media/202008/t20200814_241702.shtml (accessed on 21 December 2021).
- Russian Science Foundation. Project No. 19-72-30005. Available online: https://rscf.ru/upload/iblock/fb2/fb203c7d99c321ddbd17257ac7edf5b1.pdf (accessed on 21 December 2021). (In Russian).
- Volkova, O.Y.; Mechetina, L.V.; Taranin, A.V.; Zaboronok, A.A.; Nakai, K.; Lezhnin, S.I.; Frolov, S.A.; Kasatov, D.A.; Lezhnin, S.I.; Frolov, S.A.; et al. Impact of neutron radiation on the viability of tumor cells cultured in the presence of boron-10 isotope. Vestn. Rentgenol. Radiol. 2016, 97, 283–288. (In Russian) [Google Scholar] [CrossRef]
- Zaboronok, A.; Byvaltsev, V.; Kanygin, V.; Iarullina, A.; Kichigin, A.; Volkova, O.; Mechetina, L.; Taskaev, S.; Muhamadiyarov, R.; Nakai, K.; et al. Boron-neutron capture therapy in Russia: Preclinical evaluation of efficacy and perspectives of its application in neurooncology. New Armen. Med. J. 2017, 11, 6–15. [Google Scholar]
- Sato, E.; Zaboronok, A.; Yamamoto, T.; Nakai, K.; Taskaev, S.; Volkova, O.; Mechetina, L.; Taranin, A.; Kanygin, V.; Isobe, T.; et al. Radiobiological response of U251MG, CHO-K1 and V79 cell lines to accelerator-based boron neutron capture therapy. J. Radiat. Res. 2018, 59, 101–107. [Google Scholar] [CrossRef]
- Byvaltsev, V.A.; Zavyalov, E.L.; Kanygin, V.V.; Kasatova, A.I.; Kichigin, A.I.; Razumov, I.A.; Sycheva, T.V.; Taskaev, S.Y. Cytopathic effects of boron neutron capture therapy at an accelerating source of epithermal neutrons for the culture of human glioblastoma cells. Sib. J. Oncol. 2019, 4, 34–42. (In Russian) [Google Scholar] [CrossRef]
- Zaboronok, A.; Taskaev, S.; Volkova, O.; Mechetina, L.; Kasatova, A.; Sycheva, T.; Nakai, K.; Kasatov, D.; Makarov, A.; Kolesnikov, I.; et al. Gold nanoparticles permit in situ absorbed dose evaluation in boron neutron capture therapy for malignant tumors. Pharmaceutics 2021, 13, 1490. [Google Scholar] [CrossRef] [PubMed]
- Zavjalov, E.; Zaboronok, A.; Kanygin, V.; Kasatova, A.; Kichigin, A.; Mukhamadiyarov, R.; Razumov, I.; Sycheva, T.; Mathis, B.J.; Maezono, S.E.B.; et al. Accelerator-based boron neutron capture therapy for malignant glioma: A pilot neutron irradiation study using boron phenylalanine, sodium borocaptate and liposomal borocaptate with a heterotopic U87 glioblastoma model in SCID mice. Int. J. Radiat. Biol. 2020, 96, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Kanygin, V.; Razumov, I.; Zaboronok, A.; Zavjalov, E.; Kichigin, A.; Solovieva, O.; Tsygankova, A.; Guselnikova, T.; Kasatov, D.; Sycheva, T.; et al. Dose-dependent suppression of human glioblastoma xenograft growth by accelerator-based boron neutron capture therapy with simultaneous use of two boron-containing compounds. Biology 2021, 10, 1124. [Google Scholar] [CrossRef] [PubMed]
- Rowell, J.L.; McCarthy, D.O.; Alvarez, C.E. Dog models of naturally occurring cancer. Trends Mol. Med. 2011, 17, 380–388. [Google Scholar] [CrossRef]
- Mizuno, T. Spontaneously occurring canine cancer as a relevant animal model for developing novel treatments for human cancers. Transl. Regul. Sci. 2021, 3, 51–59. [Google Scholar] [CrossRef]
- Riccardo, F.; Aurisicchio, L.; Impellizeri, J.A.; Cavallo, F. The importance of comparative oncology in translational medicine. Cancer Immunol. Immunother. 2015, 64, 137–148. [Google Scholar] [CrossRef]
- Taskaev, S.; Berendeev, E.; Bikchurina, M.; Bykov, T.; Kasatov, D.; Kolesnikov, I.; Koshkarev, A.; Makarov, A.; Ostreinov, G.; Porosev, V.; et al. Neutron source based on vacuum insulated tandem accelerator and lithium target. Biology 2021, 10, 350. [Google Scholar] [CrossRef]
- Bayanov, B.; Belov, V.; Kindyuk, V.; Oparin, E.; Taskaev, S. Lithium neutron producing target for BINP accelerator-based neutron source. Appl. Radiat. Isot. 2004, 61, 817–821. [Google Scholar] [CrossRef]
- Bayanov, B.; Kashaeva, E.; Makarov, A.; Malyshkin, G.; Samarin, S.; Taskaev, S. A neutron producing target for BINP accelerator-based neutron source. Appl. Radiat. Isot. 2009, 67 (Suppl. 7–8), S282–S284. [Google Scholar] [CrossRef] [PubMed]
- Bikchurina, M.; Bykov, T.; Kasatov, D.; Kolesnikov, I.; Makarov, A.; Shchudlo, I.; Sokolova, E.; Taskaev, S. The measurement of the neutron yield of the 7Li(p,n)7Be reaction in lithium targets. Biology 2021, 10, 824. [Google Scholar] [CrossRef]
- Taskaev, S. Accelerator based epithermal neutron source. Phys. Part. Nucl. 2015, 46, 956–990. [Google Scholar] [CrossRef]
- Zaidi, L.; Kashaeva, E.; Lezhnin, S.; Malyshkin, G.; Samarin, S.; Sycheva, T.; Taskaev, S.; Frolov, S. Neutron-beam-shaping assembly for Boron Neutron-Capture Therapy. Phys. At. Nucl. 2017, 80, 60–66. [Google Scholar] [CrossRef]
- Zaidi, L.; Belgaid, M.; Taskaev, S.; Khelifi, R. Beam shaping assembly design of 7Li(p,n)7Be neutron source for boron neutron capture therapy of deep-seated tumor. Appl. Radiat. Isot. 2018, 139, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Taskaev, S. Development of an accelerator-based epithermal neutron source for boron neutron capture therapy. Phys. Part. Nucl. 2019, 50, 569–575. [Google Scholar] [CrossRef]
- Taskaev, S.; Bykov, T.; Kasatov, D.; Kolesnikov, I.; Koshkarev, A.; Makarov, A.; Savinov, S.; Shchudlo, I.; Sokolova, E. Measurement of the 7Li(p,p′γ)7Li reaction cross-section and 478 keV photon yield from a thick lithium target at proton energies from 0.65 MeV to 2.225 MeV. Nucl. Instrum. Methods Phys. Res. B 2021, 502, 85–94. [Google Scholar] [CrossRef]
- Bykov, T.A.; Kasatov, D.A.; Koshkarev, A.M.; Makarov, A.N.; Leonov, V.V.; Porosev, V.V.; Savinov, G.A.; Savinov, S.S.; Shchudlo, I.M.; Taskaev, S.Y.; et al. Evaluation of depth-dose profiles in a water phantom at the BNCT facility at BINP. J. Instrum. 2021, 16, P10016. [Google Scholar] [CrossRef]
- Brednikhin, S.A.; Lezhnin, S.I.; Frolov, S.A.; Yurov, D.M. NMC code for statistical modeling of neutron transport in fissionable media. Valid. Appl. 2012, 4, 24. (In Russian) [Google Scholar]
- Lee, C.L.; Zhou, X. Thick target neutron yields for the 7Li(p,n)7Be reaction near threshold. Nucl. Instr. Methods Phys. Res. B 1999, 152, 1–11. [Google Scholar] [CrossRef]
- Takeuchi, A.; Nagata, T.; Ohashi, F.; Sasaki, N.; Ushio, Y.; Hatanaka, H. Tolerance of canine brain to boron neutron capture therapy. Nihon Juigaku Zasshi 1985, 47, 859–868. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, A. Possible application of boron neutron capture therapy to canine osteosarcoma. Nihon Juigaku Zasshi 1985, 47, 869–878. [Google Scholar] [CrossRef]
- Kraft, S.L.; Gavin, P.R.; de Haan, C.E.; Leathers, C.W.; Bauer, W.F.; Miller, D.L.; Dorn, R.V., 3rd. Borocaptate sodium: A potential boron delivery compound for boron neutron capture therapy evaluated in dogs with spontaneous intracranial tumors. Proc. Natl. Acad. Sci. USA 1992, 89, 11973–11977. [Google Scholar] [CrossRef] [PubMed]
- Kraft, S.L.; Gavin, P.R.; Leathers, C.W.; de Haan, C.E.; Bauer, W.F.; Miller, D.L.; Dorn, R.V., 3rd; Griebenow, M.L. Biodistribution of boron in dogs with spontaneous intracranial tumors following borocaptate sodium administration. Cancer Res. 1994, 54, 1259–1263. [Google Scholar]
- Gavin, P.R.; Kraft, S.L.; de Haan, C.E.; Swartz, C.D.; Griebenow, M.L. Large animal normal tissue tolerance with boron neutron capture. Int. J. Radiat. Oncol. Biol. Phys. 1994, 28, 1099–1106. [Google Scholar] [CrossRef]
- Mitin, V.N.; Kulakov, V.N.; Khokhlov, V.F.; Sheino, I.N.; Arnopolskaya, A.M.; Kozlovskaya, N.G.; Zaitsev, K.N.; Portnov, A.A. Comparison of BNCT and GdNCT efficacy in treatment of canine cancer. Appl. Radiat. Isot. 2009, 67, 299–301. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Nickname | Species | Age | Tumor Localization | Histological Diagnosis |
|---|---|---|---|---|---|
| 1 | Daya | dog | 12 | soft tissue of the facial skull | osteosarcoma |
| 2 | Perchik | cat | 4 | mammary gland, frontal bone | carcinoma |
| 3 | Kira | cat | 6 | soft tissue of the back | fibrosarcoma |
| 4 | Kapa | dog | 10 | nasal cavity | - |
| 5 | Sabrina | cat | unknown | nasal meatus (passage) | lymphoma |
| 6 | Pushok | cat | 8 | nose and upper lip area soft tissues | squamous cell carcinoma |
| 7 | Seledka | cat | 4 | soft tissue of the thigh | mesenchymal tumor |
| 8 | Fenya | cat | 13 | trapezius and rhomboid muscles (after tumor removal) | fibrosarcoma |
| 9 | Lucky | cat | 5 | hyoid area | - |
| 10 | Shon | dog | 11 | upper jaw, hard palate | fibrosarcoma |
| Proton Beam Energy, MeV | Dose Rates, Gy/mC | |||
|---|---|---|---|---|
| Thermal Neutrons | Fast Neutrons | Boron-Related for 1 ppm | Photons | |
| Tumor | ||||
| 2.05 | 3.94 × 10−5 | 1.41 × 10−5 | 1.91 × 10−5 | 3.98 × 10−4 |
| 2.10 | 5.07 × 10−5 | 2.58 × 10−5 | 2.45 × 10−5 | 5.08 × 10−4 |
| Surrounding healthy tissues (brain) | ||||
| 2.05 | 5.22 × 10−6 | 9.42 × 10−7 | 2.52 × 10−6 | 1.20 × 10−4 |
| 2.10 | 6.75 × 10−6 | 1.86 × 10−6 | 3.26 × 10−6 | 1.52 × 10−4 |
| Skin | ||||
| 2.05 | 4.46 × 10−5 | 3.96 × 10−5 | 2.17 × 10−5 | 3.74 × 10−4 |
| 2.10 | 5.61 × 10−5 | 6.84 × 10−5 | 2.73 × 10−5 | 4.67 × 10−4 |
| N | Nickname | Species | Boron Concentration in Blood, µg/g | Irradiation Parameters | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Before Irradiation | After Irradiation | Energy (MeV) | Current (mA) | Current Integral (mAh) | Neutron Fluence (×1014 n/cm2) | Tumor Dose (Gy-eq) | Skin Dose (Gy-eq) | |||
| 1 | Daya | dog | 149 128 | 119 104 | 2.1 2.05 | 2 2.6 | 3.3 4 | 1.95 1.79 | 42.1 39.5 | 14.5 13.3 |
| 2 | Perchik | cat | 138 | 98 | 2.05 | 2.6 | 4 | 1.79 | 39.5 | 13.3 |
| 3 | Kira | cat | 99 124 | 74 70 | 2.05 2.05 | 2.6 2.6 | 4 2.7 | 1.79 1.21 | 39.5 26.7 | 13.3 9 |
| 4 | Kapa | dog | 99 | 65 | 2.1 | 2.1 | 4.4 | 2.60 | 56.2 | 19.3 |
| 5 | Sabrina | cat | 60 | 32 | 2.05 | 1.8 | 4.4 | 1.97 | 39.5 | 13.3 |
| 6 | Pushok | cat | 80 | 50 | 2.05 | 1.8 | 4.4 | 1.97 | 39.5 | 13.3 |
| 7 | Seledka | cat | 120 | 59 | 2.1 | 2.1 | 3.9 | 2.31 | 49.8 | 17.1 |
| 8 | Fenya | cat | 167 | 92 | 2.05 | 1.8 | 4 | 1.79 | 39.5 | 13.3 |
| 9 | Lucky | cat | 75 | 44 | 2.05 | 1.8 | 4 | 1.79 | 39.5 | 13.3 |
| 10 | Shon | dog | 109 | 44 | 2.1 | 2 | 4 | 2.37 | 51 | 17.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanygin, V.; Kichigin, A.; Zaboronok, A.; Kasatova, A.; Petrova, E.; Tsygankova, A.; Zavjalov, E.; Mathis, B.J.; Taskaev, S. In Vivo Accelerator-Based Boron Neutron Capture Therapy for Spontaneous Tumors in Large Animals: Case Series. Biology 2022, 11, 138. https://doi.org/10.3390/biology11010138
Kanygin V, Kichigin A, Zaboronok A, Kasatova A, Petrova E, Tsygankova A, Zavjalov E, Mathis BJ, Taskaev S. In Vivo Accelerator-Based Boron Neutron Capture Therapy for Spontaneous Tumors in Large Animals: Case Series. Biology. 2022; 11(1):138. https://doi.org/10.3390/biology11010138
Chicago/Turabian StyleKanygin, Vladimir, Aleksandr Kichigin, Alexander Zaboronok, Anna Kasatova, Elena Petrova, Alphiya Tsygankova, Evgenii Zavjalov, Bryan J. Mathis, and Sergey Taskaev. 2022. "In Vivo Accelerator-Based Boron Neutron Capture Therapy for Spontaneous Tumors in Large Animals: Case Series" Biology 11, no. 1: 138. https://doi.org/10.3390/biology11010138
APA StyleKanygin, V., Kichigin, A., Zaboronok, A., Kasatova, A., Petrova, E., Tsygankova, A., Zavjalov, E., Mathis, B. J., & Taskaev, S. (2022). In Vivo Accelerator-Based Boron Neutron Capture Therapy for Spontaneous Tumors in Large Animals: Case Series. Biology, 11(1), 138. https://doi.org/10.3390/biology11010138