
Relationship between Plasma Concentrations of Afatinib and the Onset of Diarrhea in Patients with Non-Small Cell Lung Cancer

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Protocols
2.2. Analytical Methods
2.3. Pharmacokinetic Analysis
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
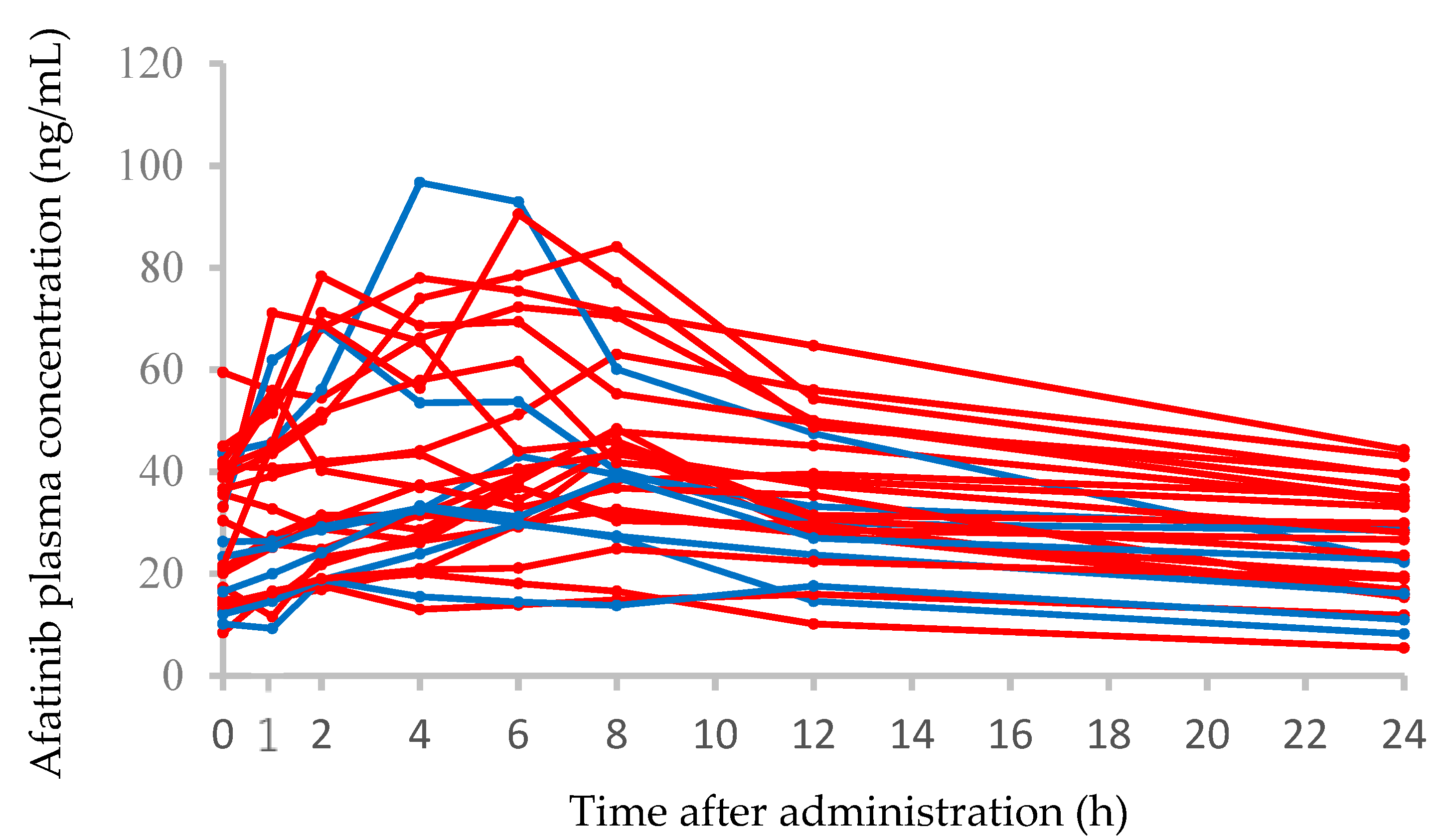
3.2. Afatinib Plasma Concentration–Time Profiles and Correlations between the AUC0–24 and Clinical Characteristics
3.3. Comparisons of Afatinib Pharmacokinetic Parameters or Clinical Characteristics between Patients with Grade 2 or Grade 0–1 Diarrhea
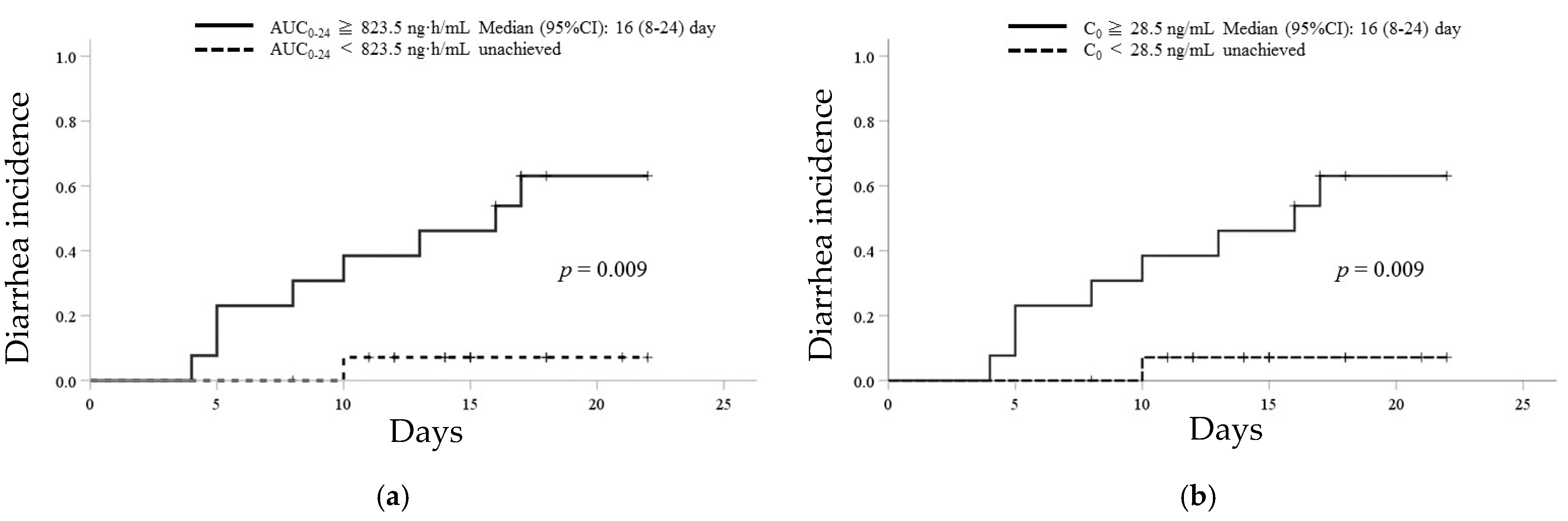
3.4. ROC Analysis and Kaplan–Meier Curves of Afatinib for the Incidence of Grade 2 Diarrhea
3.5. Prediction Formulae to Estimate the Afatinib AUC0–24
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Solca, F.; Dahl, G.; Zoephel, A.; Bader, G.; Sanderson, M.; Klein, C.; Kraemer, O.; Himmelsbach, F.; Haaksma, E.; Adolf, G.R. Target binding properties and cellular activity of afatinib (BIBW 2992), an irreversible ErbB family blocker. J. Pharmacol. Exp. Ther. 2012, 343, 342–350. [Google Scholar] [CrossRef]
- Machiels, J.-P.H.; Haddad, R.I.; Fayette, J.; Licitra, L.F.; Tahara, M.; Vermorken, J.B.; Clement, P.M.; Gauler, T.; Cupissol, D.; Grau, J.J.; et al. Afatinib versus methotrexate as second-line treatment in patients with recurrent or metastatic squamous cell carcinoma of the head and neck progressing on or after platinum-based therapy (LUX-Head & Neck 1): An open-label, randomised phase 3 trial. Lancet Oncol. 2015, 16, 583–594. [Google Scholar] [CrossRef]
- Yang, J.C.-H.; Shih, J.-Y.; Su, W.-C.; Hsia, T.-C.; Tsai, C.-M.; Ou, S.-H.I.; Yu, C.-J.; Chang, G.-C.; Ho, C.-L.; Sequist, L.V.; et al. Afatinib for patients with lung adenocarcinoma and epidermal growth factor receptor mutations (LUX-Lung 2): A phase 2 trial. Lancet Oncol. 2012, 13, 539–548. [Google Scholar] [CrossRef]
- Sequist, L.V.; Yang, J.C.-H.; Yamamoto, N.; O’Byrne, K.; Hirsh, V.; Mok, T.; Geater, S.L.; Orlov, S.; Tsai, C.-M.; Boyer, M.; et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. JCO 2013, 31, 3327–3334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katakami, N.; Atagi, S.; Goto, K.; Hida, T.; Horai, T.; Inoue, A.; Ichinose, Y.; Koboyashi, K.; Takeda, K.; Kiura, K.; et al. LUX-Lung 4: A phase II trial of afatinib in patients with advanced non–small-cell lung cancer who progressed during prior treatment with erlotinib, gefitinib, or both. JCO 2013, 31, 3335–3341. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-L.; Zhou, C.; Hu, C.-P.; Feng, J.; Lu, S.; Huang, Y.; Li, W.; Hou, M.; Shi, J.H.; Lee, K.Y.; et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): An open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 213–222. [Google Scholar] [CrossRef]
- Park, K.; Tan, E.-H.; O’Byrne, K.; Zhang, L.; Boyer, M.; Mok, T.; Hirsh, V.; Yang, J.C.-H.; Lee, K.H.; Lu, S.; et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): A phase 2B, open-label, randomised controlled trial. Lancet Oncol. 2016, 17, 577–589. [Google Scholar] [CrossRef]
- Tamura, K.; Nukiwa, T.; Gemma, A.; Yamamoto, N.; Mizushima, M.; Ochai, K.; Ikeda, R.; Azuma, H.; Nakanishi, Y. Real-world treatment of over 1600 Japanese patients with EGFR mutation-positive non-small cell lung cancer with daily afatinib. Int. J. Clin. Oncol. 2019, 24, 917–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.; Lee, S.-H.; Ahn, J.S.; Ahn, M.-J.; Park, K.; Sun, J.-M. Efficacy and safety of afatinib for EGFR-mutant non-small cell lung cancer, compared with gefitinib or erlotinib. Cancer Res. Treat. 2018, 51, 502–509. [Google Scholar] [CrossRef]
- Takeda, M.; Okamoto, I.; Nakagawa, K. Pooled safety analysis of EGFR-TKI treatment for EGFR mutation-positive non-small cell lung cancer. Lung Cancer 2015, 88, 74–79. [Google Scholar] [CrossRef]
- Ding, P.N.; Lord, S.J.; Gebski, V.; Links, M.; Bray, V.; Gralla, R.J.; Yang, J.C.-H.; Lee, C.K. Risk of treatment-related toxicities from EGFR tyrosine kinase inhibitors: A meta-analysis of clinical trials of gefitinib, erlotinib, and afatinib in advanced EGFR-mutated non–small cell lung cancer. J. Thoracic Oncol. 2017, 12, 633–643. [Google Scholar] [CrossRef] [Green Version]
- Kato, T.; Yoshioka, H.; Okamoto, I.; Yokoyama, A.; Hida, T.; Seto, T.; Kiura, K.; Massey, D.; Seki, Y.; Yamamoto, N. Afatinib versus cisplatin plus pemetrexed in Japanese patients with advanced non-small cell lung cancer harboring activating EGFR mutations: Subgroup analysis of LUX-Lung 3. Cancer Sci. 2015, 106, 1202–1211. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.C.-H.; Reguart, N.; Barinoff, J.; Köhler, J.; Uttenreuther-Fischer, M.; Stammberger, U.; O’Brien, D.; Wolf, J.; Cohen, E.E. Diarrhea associated with afatinib: An oral ErbB family blocker. Expert Rev. Anticancer Ther. 2013, 13, 729–736. [Google Scholar] [CrossRef]
- Wind, S.; Schmid, M.; Erhardt, J.; Goeldner, R.-G.; Stopfer, P. Pharmacokinetics of afatinib, a selective irreversible ErbB family blocker, in patients with advanced solid tumours. Clin. Pharmacokinet. 2013, 52, 1101–1109. [Google Scholar] [CrossRef]
- Wind, S.; Schnell, D.; Ebner, T.; Freiwald, M.; Stopfer, P. Clinical pharmacokinetics and pharmacodynamics of afatinib. Clin. Pharmacokinet. 2017, 56, 235–250. [Google Scholar] [CrossRef] [Green Version]
- Sato, J.; Morikawa, N.; Chiba, R.; Nihei, S.; Moriguchi, S.; Saito, H.; Yamauchi, K.; Kudo, K. Case series on the association between blood levels and side effects of afatinib maleate. Cancer Chemother. Pharmacol. 2017, 80, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, H.; Iihara, H.; Hirose, C.; Fukuda, Y.; Kitahora, M.; Kaito, D.; Yanase, K.; Endo, J.; Ohno, Y.; Suzuki, A.; et al. Effects of pharmacokinetics-related genetic polymorphisms on the side effect profile of afatinib in patients with non-small cell lung cancer. Lung Cancer 2019, 134, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Nakao, K.; Kobuchi, S.; Marutani, S.; Iwazaki, A.; Tamiya, A.; Isa, S.; Okishio, K.; Kanazu, M.; Tamiya, M.; Hirashima, T.; et al. Population pharmacokinetics of afatinib and exposure-safety relationships in Japanese patients with EGFR mutation-positive non-small cell lung cancer. Sci. Rep. 2019, 9, 18202. [Google Scholar] [CrossRef] [PubMed]
- Miura, M.; Sato, K.; Miura, H.; Niioka, T.; Kobayashi, H.; Narita, C.; Ito, H. A limited sampling strategy for estimation of the area under the plasma concentration–time curve of gefitinib. Ther. Drug Monitor. 2014, 36, 24–29. [Google Scholar] [CrossRef]
- Yokota, H.; Sato, K.; Okuda, Y.; Kobayashi, H.; Takeda, M.; Asano, M.; Ito, H.; Miura, M. Effects of histamine 2-receptor antagonists and proton pump inhibitors on the pharmacokinetics of gefitinib in patients with non-small-cell lung cancer. Clin. Lung Cancer 2017, 18, e433–e439. [Google Scholar] [CrossRef]
- Nagahama, M.; Ozeki, T.; Suzuki, A.; Sugino, K.; Niioka, T.; Ito, K.; Miura, M. Association of lenvatinib trough plasma concentrations with lenvatinib-induced toxicities in Japanese patients with thyroid cancer. Med. Oncol. 2019, 36, 39. [Google Scholar] [CrossRef]
- Efron, B.; Tibshirani, R.J. An introduction to the bootstrap. Monographs on Statistics and Applied Probability, No. 57. Chapman and Hall, London, 436 p. Monogr. Stat. Appl. Probab. 1993, 57, 436. [Google Scholar]
- Freiwald, M.; Schmid, U.; Fleury, A.; Wind, S.; Stopfer, P.; Staab, A. Population pharmacokinetics of afatinib, an irreversible ErbB family blocker, in patients with various solid tumors. Cancer Chemother. Pharmacol. 2014, 73, 759–770. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, A.M.; Nguyen, A.-M.; Karapetis, C.S.; Rowland, A.; Sorich, M.J. Risk factors for severe diarrhea with an afatinib treatment of non-small cell lung cancer: A pooled analysis of clinical trials. Cancers 2018, 10, 384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duan, T.; Cil, O.; Thiagarajah, J.R.; Verkman, A.S. Intestinal epithelial potassium channels and CFTR chloride channels activated in ErbB tyrosine kinase inhibitor diarrhea. JCI Insight 2019, 4, e126444. [Google Scholar] [CrossRef]
- Kim, Y.; Quach, A.; Das, S.; Barrett, K.E. Potentiation of calcium-activated chloride secretion and barrier dysfunction may underlie EGF receptor tyrosine kinase inhibitor-induced diarrhea. Physiol. Rep. 2020, 8, e14490. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.-H.; Sequist, L.V.; Zhou, C.; Schuler, M.; Geater, S.L.; Mok, T.; Hu, C.-P.; Yamamoto, N.; Feng, J.; O’Byrne, K.; et al. Effect of dose adjustment on the safety and efficacy of afatinib for EGFR mutation-positive lung adenocarcinoma: Post hoc analyses of the randomized LUX-Lung 3 and 6 trials. Ann. Oncol. 2016, 27, 2103–2110. [Google Scholar] [CrossRef] [PubMed]
- Halmos, B.; Tan, E.-H.; Soo, R.A.; Cadranel, J.; Lee, M.K.; Foucher, P.; Hsia, T.-C.; Hochmair, M.; Griesinger, F.; Hida, T.; et al. Impact of afatinib dose modification on safety and effectiveness in patients with EGFR mutation-positive advanced NSCLC: Results from a global real-world study (RealGiDo). Lung Cancer 2019, 127, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.-Y.; Wang, C.-L.; Li, S.-H.; Hsu, P.-C.; Chen, C.-H.; Lin, T.-Y.; Kuo, C.-H.; Fang, Y.-F.; Ko, H.-W.; Yu, C.-T.; et al. The efficacy of 40 mg versus dose de-escalation to less than 40 mg of afatinib (Giotrif) as the first-line therapy for patients with primary lung adenocarcinoma harboring favorable epidermal growth factor mutations. Oncotarget 2017, 8, 97602–97612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, R.; Shukuya, T.; Imamura, C.K.; Tokito, T.; Shimada, N.; Koyama, R.; Yamada, K.; Ishii, H.; Azuma, K.; Takahashi, K. Phase I study of afatinib plus bevacizumab in patients with advanced non-squamous non-small cell lung cancer harboring EGFR mutations. Transl. Lung Cancer Res. 2021, 10, 183–192. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number or Values | |
|---|---|---|
| Total number | 28 | |
| Female:Male | 13:15 | |
| Age, years | 67.4 ± 7.7 | (51–86) |
| Body weight, kg | 57.3 ± 9.4 | (35.3–78.3) |
| Body surface area, m2 | 1.59 ± 0.16 | (1.23–1.93) |
| Body mass index, kg/m2 | 22.7 ± 1.5 | (19.8–25.8) |
| Laboratory test values | ||
| White blood cell, ×103/mm3 | 5.7 ± 1.4 | (3.7–10.4) |
| Red blood cell, ×104/mm3 | 422 ± 43 | (342–498) |
| Hemoglobin, g/dL | 12.6 ± 1.7 | (8–15) |
| Platelets, ×104/mm3 | 238 ± 59 | (122–366) |
| Aspartate aminotransferase, IU/L | 22.4 ± 5.4 | (12–39) |
| Alanine aminotransferase, IU/L | 16.9 ± 5.6 | (8–30) |
| Alkaline phosphatase, IU/L | 314 ± 218 | (115–1336) |
| Lactate dehydrogenase, IU/L | 219 ± 92 | (135–601) |
| Serum albumin, g/dL | 3.8 ± 0.4 | (2.8–4.6) |
| Total bilirubin, mg/dL | 0.5 ± 0.2 | (0.3–1.1) |
| Serum creatinine, mg/dL | 0.69 ± 0.21 | (0.43–1.30) |
| eGFR, mL/min/1.73 m2 | 82.4 ± 21.4 | (43.6–125.5) |
| Stage IV:IIIb:IIb | 26:1:1 | |
| Tumor history, adenocarcinoma:other | 28:0 | |
| EGFR mutation, exon 19 deletions:exon 21 L858R:other | 16:7:5 | |
| Initial dose, 30 mg:40 mg | 7:21 | |
| Diarrhea (grade 1:2): no diarrhea | 23 (14:9):5 | |
| Characteristics | Median AUC0–24 (Range), ng·h/mL | p-Value |
|---|---|---|
| Female | 848 (574–1480) | 0.205 |
| Male | 753 (289–1366) | |
| Correlation Coefficient (r) | p-Value | |
| Age | 0.037 | 0.850 |
| Body weight | −3.480 | 0.070 |
| Body surface area | −2.540 | 0.192 |
| BMI | −0.050 | 0.799 |
| Laboratory test values | ||
| White blood cell | 0.115 | 0.561 |
| Red blood cell | −0.293 | 0.130 |
| Hemoglobin | −0.289 | 0.136 |
| Platelets | −0.151 | 0.444 |
| Aspartate aminotransferase | 0.287 | 0.138 |
| Alanine aminotransferase | −0.171 | 0.386 |
| Alkaline phosphatase | −0.365 | 0.056 |
| Lactate dehydrogenase | 0.241 | 0.217 |
| Serum albumin | −0.002 | 0.991 |
| Total bilirubin | 0.119 | 0.546 |
| Serum creatinine | −0.070 | 0.724 |
| eGFR | −0.107 | 0.587 |
| Parameters/Characteristics | Grade 2 Diarrhea | Grade 0–1 Diarrhea | p-Value |
|---|---|---|---|
| Median (Quartile 1–Quartile 3) | Median (Quartile 1–Quartile 3) | ||
| Cmax (ng/mL) | 78.0 (47.9–84.1) | 38.9 (32.8–55.0) | 0.017 |
| C0 (ng/mL) | 38.9 (33.1–42.0) | 21.0 (15.0–29.8) | 0.032 |
| Cmin (ng/mL) | 28.1 (24.8–34.4) | 16.5(14.5–25.0) | 0.046 |
| Cmax/Cmin ratio | 2.20 (1.90–2.70) | 2.20 (1.75–2.45) | 0.657 |
| AUC0–24 (ng·h/mL) | 1225 (891–1344) | 666 (580–863) | 0.013 |
| AUC6–24 (ng·h/mL) | 787 (672–950) | 500 (424–592) | 0.007 |
| AUC6–24/AUC0–24 × 100 (%) | 71.7 (67.8–73.3) | 73.6 (69.7–75.8) | 0.389 |
| Daily dose, 30 mg:40 mg | 1:8 | 6:13 | 0.249 |
| Female:male | 6:3 | 7:12 | 0.142 |
| Age, years | 65.0 (62.0–71.0) | 67.0 (63.5–73.5) | 0.693 |
| Body weight, kg | 50.5 (46.7–56.0) | 56.2 (53.2–64.3) | 0.085 |
| Body surface area, m2 | 1.54 (1.41–1.57) | 1.60 (1.54–1.73) | 0.109 |
| BMI, kg/m2 | 22.9 (22.8–23.3) | 23.0 (21.3–23.4) | 0.694 |
| Laboratory test values | |||
| White blood cell, ×103/mm3 | 5.3 (4.0–6.9) | 5.4 (4.1–6.0) | 0.825 |
| Red blood cell, ×104/mm3 | 405 (384–430) | 413 (372–455) | 0.640 |
| Hemoglobin, g/dL | 12.1 (11.5–12.4) | 12.5 (11.5–13.6) | 0.403 |
| Platelets, ×104/mm3 | 21.4 (16.6–23.1) | 23.7 (20.6–27.2) | 0.210 |
| Aspartate aminotransferase, IU/L | 21 (18–22) | 19 (18–28) | 0.730 |
| Alanine aminotransferase, IU/L | 15 (11–28) | 18 (14–25) | 0.362 |
| Alkaline phosphatase, IU/L | 241 (211–419) | 261 (226–290) | 0.825 |
| Lactate dehydrogenase, IU/L | 174 (156–191) | 176 (160–217) | 0.980 |
| Serum albumin, g/dL | 3.4 (3.3–3.6) | 3.7 (3.4–3.9) | 0.311 |
| Total bilirubin, mg/dL | 0.5 (0.4–0.7) | 0.5 (0.4–0.6) | 0.439 |
| Serum creatinine, mg/dL | 0.67 (0.56–0.70) | 0.74 (0.66–0.85) | 0.110 |
| eGFR, mL/min/1.73 m2 | 78.5 (62.3–97.3) | 74.1 (65.9–82.6) | 0.539 |
| Sampling Numbers | Sampling Time (h) | Prediction Formula for AUC0–24 | Predicted versus Observed AUC0–24 | Slope | Intercept 95% CI * | p * | ||
|---|---|---|---|---|---|---|---|---|
| r2 | p | 95% CI * | p * | |||||
| One-point | 0 | 22.3× C0 + 215.9 | 0.761 | <0.001 | 17.7 to 28.6 | 0.001 | 85.5 to 331.2 | 0.005 |
| 1 | 16.4 × C1 + 286.1 | 0.712 | <0.001 | 12.2 to 21.8 | 0.001 | 143.7 to 411.0 | 0.001 | |
| 2 | 14.5 × C2 + 276.9 | 0.691 | <0.001 | 10.6 to 19.7 | 0.001 | 110.3 to 433.1 | 0.012 | |
| 4 | 13.7 × C4 + 263.4 | 0.762 | <0.001 | 10.5 to 18.0 | 0.001 | 112.1 to 410.0 | 0.007 | |
| 6 | 14.0 × C6 + 214.6 | 0.840 | <0.001 | 11.4 to 17.3 | 0.001 | 81.7 to 334.6 | 0.004 | |
| 8 | 17.5 × C8 + 75.9 | 0.899 | <0.001 | 15.6 to 20.1 | 0.001 | −25.0 to 159.6 | 0.108 | |
| 12 | 23.8 × C12 + 11.9 | 0.916 | <0.001 | 21.6 to 26.7 | 0.001 | −75.2 to 84.7 | 0.770 | |
| Two-points † | 0 | 10.6 × C0 + 9.1 × C6 + 135.4 | 0.911 | <0.001 | 6.1 to 16.5 | 0.003 | 38.8 to 228.5 | 0.022 |
| 6 | 5.6 to 12.3 | 0.001 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yokota, H.; Sato, K.; Sakamoto, S.; Okuda, Y.; Asano, M.; Takeda, M.; Nakayama, K.; Miura, M. Relationship between Plasma Concentrations of Afatinib and the Onset of Diarrhea in Patients with Non-Small Cell Lung Cancer. Biology 2021, 10, 1054. https://doi.org/10.3390/biology10101054
Yokota H, Sato K, Sakamoto S, Okuda Y, Asano M, Takeda M, Nakayama K, Miura M. Relationship between Plasma Concentrations of Afatinib and the Onset of Diarrhea in Patients with Non-Small Cell Lung Cancer. Biology. 2021; 10(10):1054. https://doi.org/10.3390/biology10101054
Chicago/Turabian StyleYokota, Hayato, Kazuhiro Sato, Sho Sakamoto, Yuji Okuda, Mariko Asano, Masahide Takeda, Katsutoshi Nakayama, and Masatomo Miura. 2021. "Relationship between Plasma Concentrations of Afatinib and the Onset of Diarrhea in Patients with Non-Small Cell Lung Cancer" Biology 10, no. 10: 1054. https://doi.org/10.3390/biology10101054
APA StyleYokota, H., Sato, K., Sakamoto, S., Okuda, Y., Asano, M., Takeda, M., Nakayama, K., & Miura, M. (2021). Relationship between Plasma Concentrations of Afatinib and the Onset of Diarrhea in Patients with Non-Small Cell Lung Cancer. Biology, 10(10), 1054. https://doi.org/10.3390/biology10101054