SEM Analysis of Enamel Abrasion after Air Polishing Treatment with Erythritol, Glycine and Sodium Bicarbonate

 , ,
, , 
 ,
,  ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Sample
2.2. Interventions
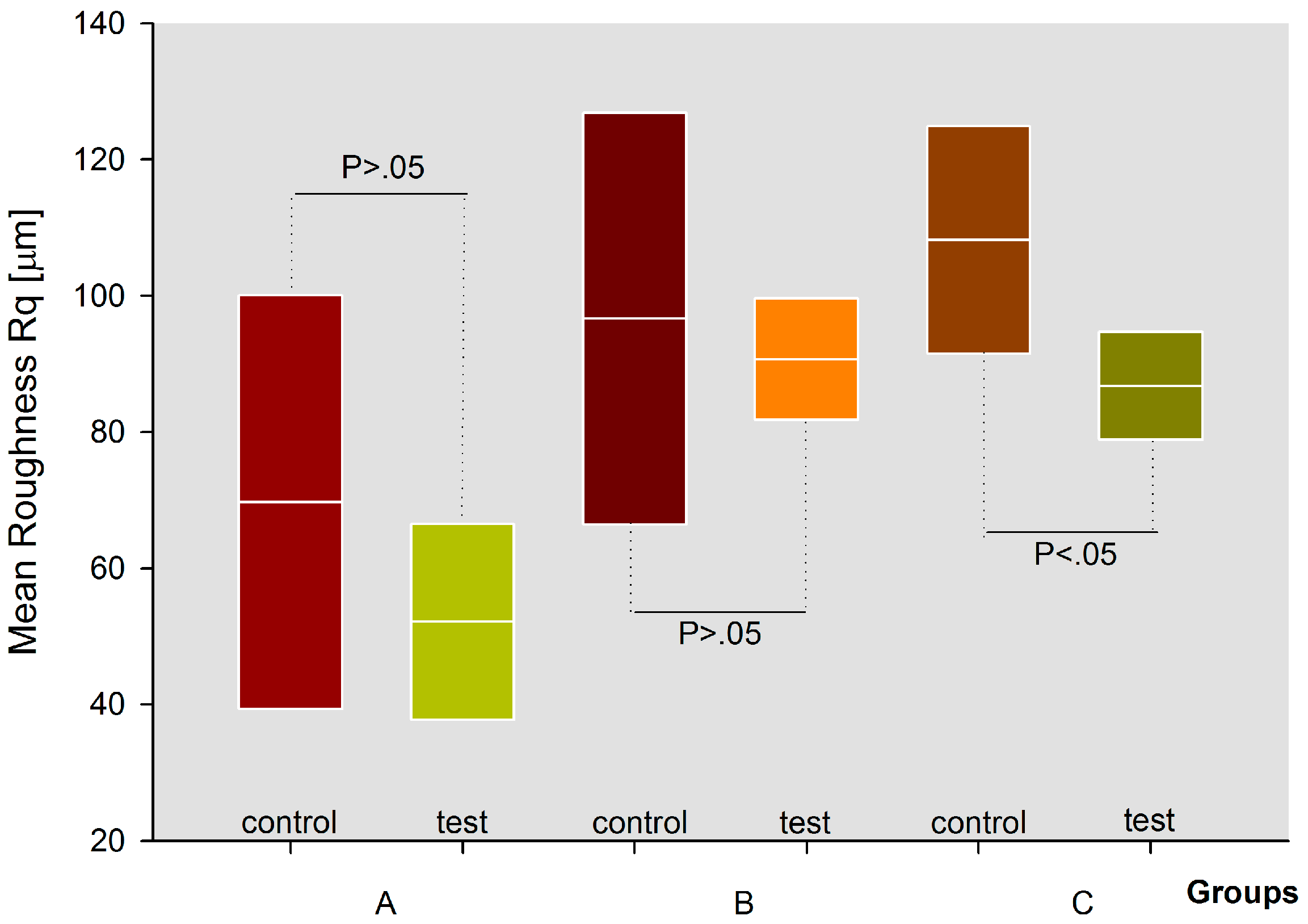
- Group A treated with glycine (Air Flow Soft powder, EMS Electro Medical System S.A., Nyon, Switzerland). The powder had a particle size of about 65 μm;
- Group B treated with erythritol (Air Flow Plus powder, EMS Electro Medical System S.A., Nyon, Switzerland). The powder had a particle size of about 14 μm;
- Group C treated with sodium bicarbonate (Air Flow Classic powder, EMS Electro Medical System S.A., Nyon, Switzerland). The powder had a particle size of about 65 μm.
2.3. Variables Measured
2.4. Statistical Analysis
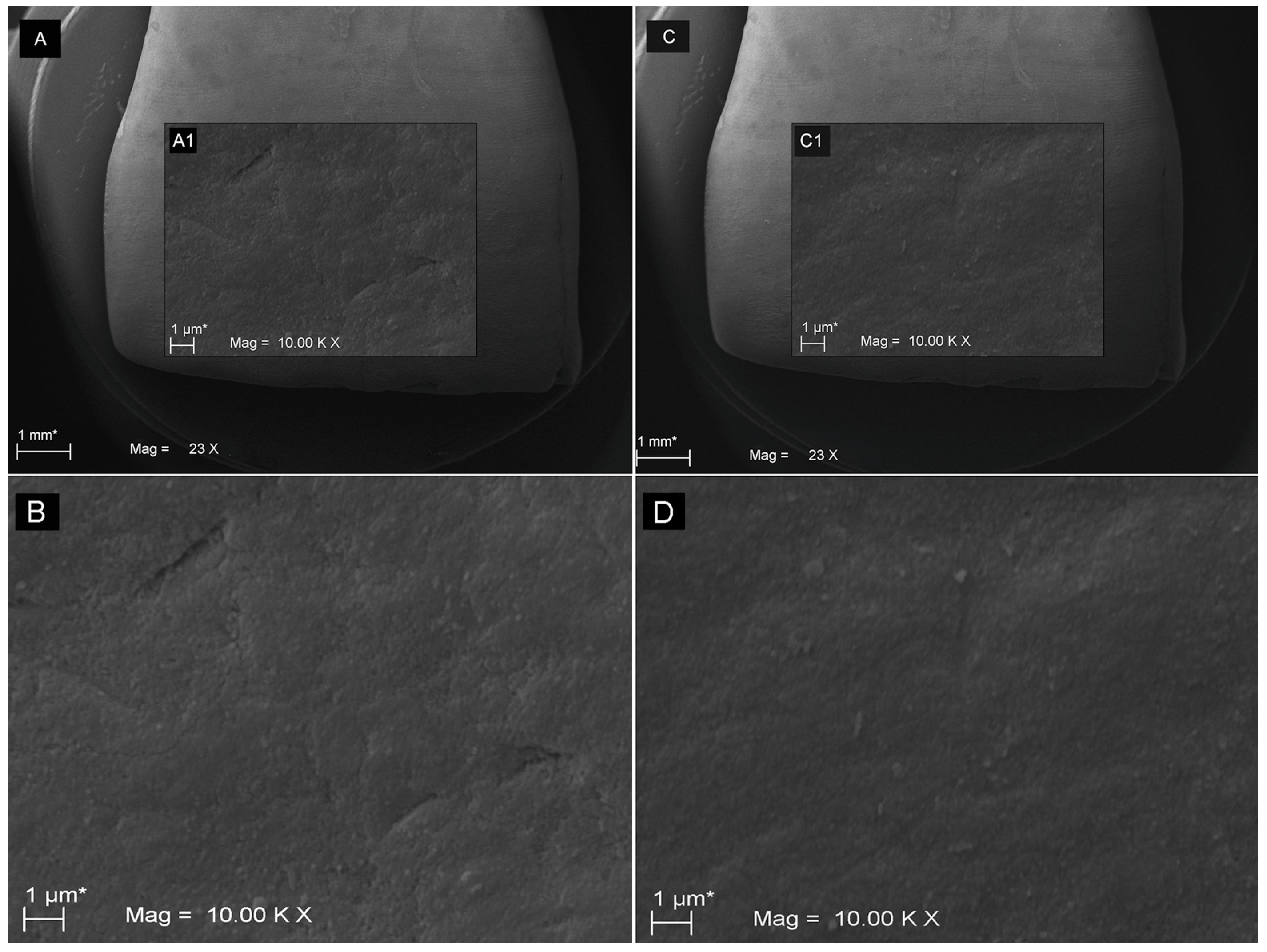
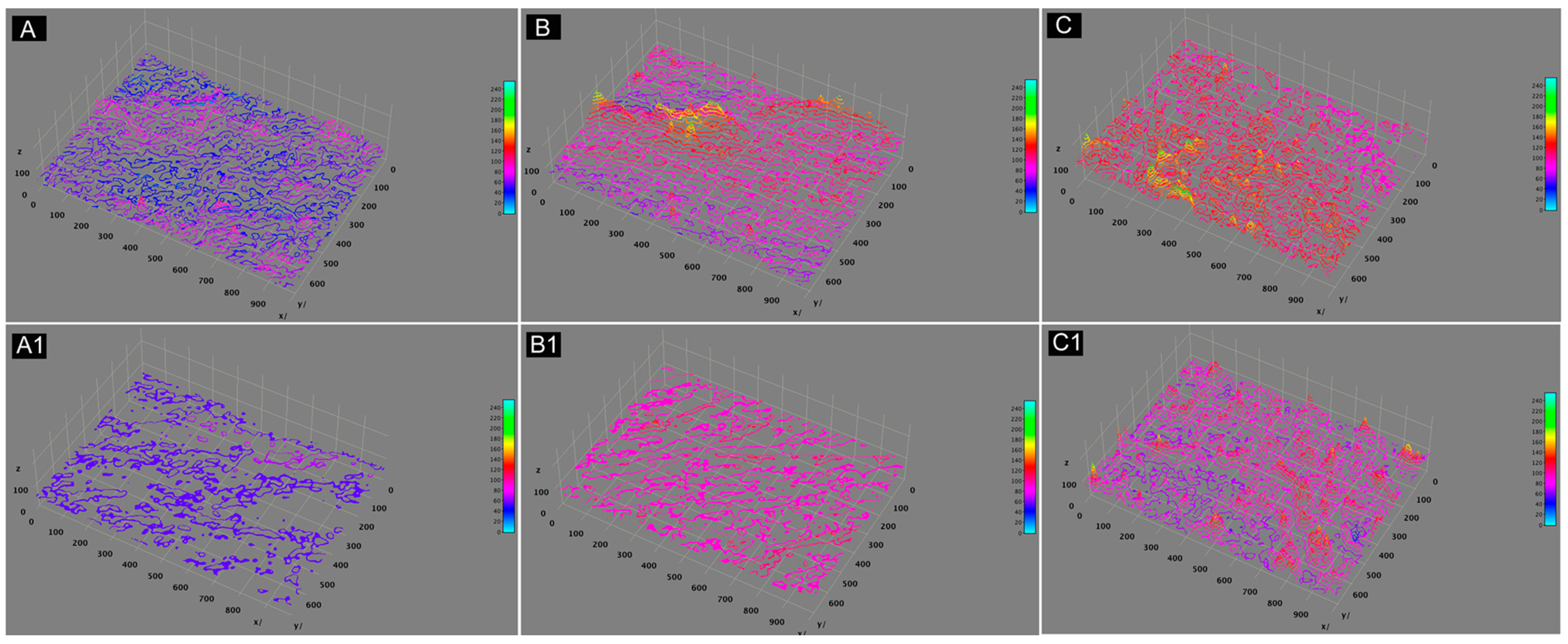
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- WHO Expert Committee. Prevention Methods and Programs for Oral Diseases; Technical Report, Series 713; World Health Organization: Geneva, Switzerland, 1984. [Google Scholar]
- Axelsson, P.; Nyström, B.; Lindhe, J. The long-term effect of a plaque control program on tooth mortality, caries and periodontal disease in adults: Results after 30 years of maintenance. J. Clin. Periodontol. 2004, 31, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Tonetti, M.S. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev. Dent. 2003, 1, 7–16. [Google Scholar] [PubMed]
- Graumann, S.J.; Sensat, M.L.; Stoltenberg, J.L. Air polishing: A review of current literature. J. Dent. Hyg. 2013, 87, 173–180. [Google Scholar] [PubMed]
- Fux, C.A.; Stoodley, P.; Hall-Stoodley, L.; Costerton, J.W. Bacterial bio-films: A diagnostic and therapeutic challenge. Expert Rev. Anti Infect. Ther. 2003, 1, 667–683. [Google Scholar] [CrossRef] [PubMed]
- Socransky, S.S.; Haffajee, A.D. Dental biofilms: Difficult therapeutic targets. Periodontol. 2000 2002, 28, 12–55. [Google Scholar] [CrossRef] [PubMed]
- Eslamian, L.; Borzabadi-Farahani, A.; Tavakol, P.; Tavakol, A.; Amini, N.; Lynch, E. Effect of multiple debonding sequences on shear bond strength of new stainless steel brackets. J. Orthod. Sci. 2015, 4, 37–41. [Google Scholar] [PubMed]
- Sculean, A.; Bastendorf, K.D.; Becker, C.; Bush, B.; Einwag, J.; Lanoway, C.; Platzer, U.; Schmage, P.; Schoeneich, B.; Walter, C.; et al. A paradigm shift in mechanical biofilm management? Subgingival air polishing: A new way to improve mechanical biofilm management in the dental practice. Quintessence Int. 2013, 44, 475–477. [Google Scholar] [PubMed]
- Petersilka, G.J. Subgingival air-polishing in the treatment of periodontal biofilm infections. Periodontol. 2000 2011, 55, 124–142. [Google Scholar] [CrossRef]
- Wennstrom, J.L.; Dahlen, G.; Ramberg, P. Subgingival debridement of periodontal pockets by air polishing in comparison with ultrasonic instrumentation during maintenance therapy. J. Clin. Periodontol. 2011, 38, 820–827. [Google Scholar] [CrossRef]
- Black, R.B. Air polishing: Some fundamentals. J. Am. Dent. Assoc. 1950, 41, 701–710. [Google Scholar] [CrossRef]
- Johnson, W.W.; Barnes, C.M.; Covey, D.A.; Walker, M.P.; Ross, J.A. An in vitro investigation of the effects of an aluminum air polishing powder delivered via the Prophy Jet™ on dental restorative materials. J. Prosthodont. 2004, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Schmage, P.; Kahili, F.; Nergiz, I.; Scorziello, T.M.; Platzer, U.; Pfeiffer, P. Cleaning effectiveness of implant prophylaxis instruments. Int. J. Oral Maxillofac. Implants 2014, 29, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Louropoulou, A.; Slot, D.E.; Van der Weijden, F. Influence of mechanical instruments on the biocompatibility of titanium dental implants surfaces: A systematic review. Clin. Oral Implant Res. 2015, 26, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Barnes, C.M.; Covey, D.; Watanabe, H.; Simetich, B.; Schulte, J.R.; Chen, H. An in vitro comparison of the effects of various air polishing powders on enamel and selected aesthetic restorative materials. J. Clin. Dent. 2014, 25, 76–87. [Google Scholar] [PubMed]
- Bühler, J.; Amato, M.; Weiger, R.; Walter, C. A systematic review on the effects of air polishing devices on oral tissues. Int. J. Dent. Hyg. 2016, 14, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Jost-Brinkmann, P.G. The influence of air polishers on tooth enamel. An in-vitro study. J. Orofac. Orthop. 1998, 59, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Tada, K.; Kakuta, K.; Ogura, H.; Sato, S. Effect of particle diameter on air polishing of dentin surfaces. Odontology 2010, 98, 31–36. [Google Scholar] [CrossRef]
- Bühler, J.; Schmidli, F.; Weiger, R.; Walter, C. Analysis of the effects of air polishing powders containing sodium bicarbonate and glycine on human teeth. Clin. Oral Investig. 2015, 19, 877–885. [Google Scholar] [CrossRef]
- Müller, N.; Moëne, R.; Cancela, J.A.; Mombelli, A. Subgingival air-polishing with erythritol during periodontal maintenance: Randomized clinical trial of twelve months. J. Clin. Periodontol. 2014, 41, 883–889. [Google Scholar] [CrossRef]
- Munro, I.C.; Berndt, W.O.; Borzelleca, J.F.; Flamm, G.; Lynch, B.S.; Kennepohl, E.; Bar, E.A.; Modderman, J. Erythritol: An interpretive summary of biochemical, metabolic, toxicological and clinical data. Food Chem. Toxicol. 1998, 36, 1139–1174. [Google Scholar] [CrossRef]
- Park, E.J.; Kwon, E.Y.; Kim, H.J.; Lee, J.Y.; Choi, J.; Joo, J.Y. Clinical and microbiological effects of the supplementary use of an erythritol powder air-polishing device in non-surgical periodontal therapy: A randomized clinical trial. J. Periodontal Implant Sci. 2018, 48, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Sinjari, B.; D’Addazio, G.; Bozzi, M.; Celletti, R.; Traini, T.; Mavriqi, L.; Caputi, S. Comparison of a novel ultrasonic scaler tip vs. conventional design on a titanium surface. Material 2018, 11, 2345. [Google Scholar] [CrossRef] [PubMed]
- Weaks, L.M.; Lescher, N.B.; Barnes, C.M.; Holroyd, S.V. Clinical evaluation of the Prophy-Jet as an instrument for routine removal of tooth stain and plaque. J. Periodontol. 1984, 55, 486–488. [Google Scholar] [CrossRef] [PubMed]
- Kontturi-Närki, V.; Markkanen, S.; Markkanen, H. Effects of air polishing on dental plaque removal and hard tissue as evaluated by scanning electron microscopy. J. Periodontol. 1990, 61, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Karacaoglu, F.; Tuzcel, N.Y.; Akkaya, M. A comperative evaluation of 3 different polishing methods on tooth surface roughness. J. Biomed. Sci. 2016, 6, 1–6. [Google Scholar] [CrossRef]
- Camboni, S.; Donnet, M. Tooth surface comparison after air polishing and rubber cup: A scanning electron microscopy study. J. Clin. Dent. 2016, 27, 13–18. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Paired Samples Statistics (T test) | |||||||||
| Groups | Mean | N | Std. Deviation | Std. Error Mean | |||||
| A | gly_control | 69.7100 | 5 | 30.38000 | 13.58635 | ||||
| gly_treatment | 52.1200 | 5 | 14.39000 | 6.43540 | |||||
| B | eryt_control | 96.6600 | 5 | 30.20000 | 13.50585 | ||||
| eryt_treatment | 90.6800 | 5 | 8.93000 | 3.99362 | |||||
| C | sodbi_control | 108.1700 | 5 | 16.70000 | 7.46847 | ||||
| sodbi_treatment | 86.7800 | 5 | 7.92000 | 3.54193 | |||||
| Groups | Paired Differences | t | df | Sig. (2-tailed) | |||||
| Mean | Std. Deviation | Std. Error Mean | 95% Confidence Interval of the Difference | ||||||
| Lower | Upper | ||||||||
| A | gly_control | 17.59000 | 15.99000 | 7.15095 | −2.26421 | 37.44421 | 2.460 | 4 | 0.070 |
| gly_treatment | |||||||||
| B | gly_control | 5.98000 | 21.27000 | 9.51223 | −20.43019 | 32.39019 | 0.629 | 4 | 0.564 |
| gly_treatment | |||||||||
| C | sodbi_control | 21.39000 | 8.78000 | 3.92654 | 10.48819 | 32.29181 | 5.448 | 4 | 0.006 |
| sodbi_treatment | |||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sinjari, B.; D’Addazio, G.; Bozzi, M.; Santilli, M.; Traini, T.; Murmura, G.; Caputi, S. SEM Analysis of Enamel Abrasion after Air Polishing Treatment with Erythritol, Glycine and Sodium Bicarbonate. Coatings 2019, 9, 549. https://doi.org/10.3390/coatings9090549
Sinjari B, D’Addazio G, Bozzi M, Santilli M, Traini T, Murmura G, Caputi S. SEM Analysis of Enamel Abrasion after Air Polishing Treatment with Erythritol, Glycine and Sodium Bicarbonate. Coatings. 2019; 9(9):549. https://doi.org/10.3390/coatings9090549
Chicago/Turabian StyleSinjari, Bruna, Gianmaria D’Addazio, Martina Bozzi, Manlio Santilli, Tonino Traini, Giovanna Murmura, and Sergio Caputi. 2019. "SEM Analysis of Enamel Abrasion after Air Polishing Treatment with Erythritol, Glycine and Sodium Bicarbonate" Coatings 9, no. 9: 549. https://doi.org/10.3390/coatings9090549
APA StyleSinjari, B., D’Addazio, G., Bozzi, M., Santilli, M., Traini, T., Murmura, G., & Caputi, S. (2019). SEM Analysis of Enamel Abrasion after Air Polishing Treatment with Erythritol, Glycine and Sodium Bicarbonate. Coatings, 9(9), 549. https://doi.org/10.3390/coatings9090549