
Optimal Design and Processing Technology of 3D Printed Tibial Implants


Abstract
:1. Introduction
2. Materials and Methods
2.1. Modeling Methods
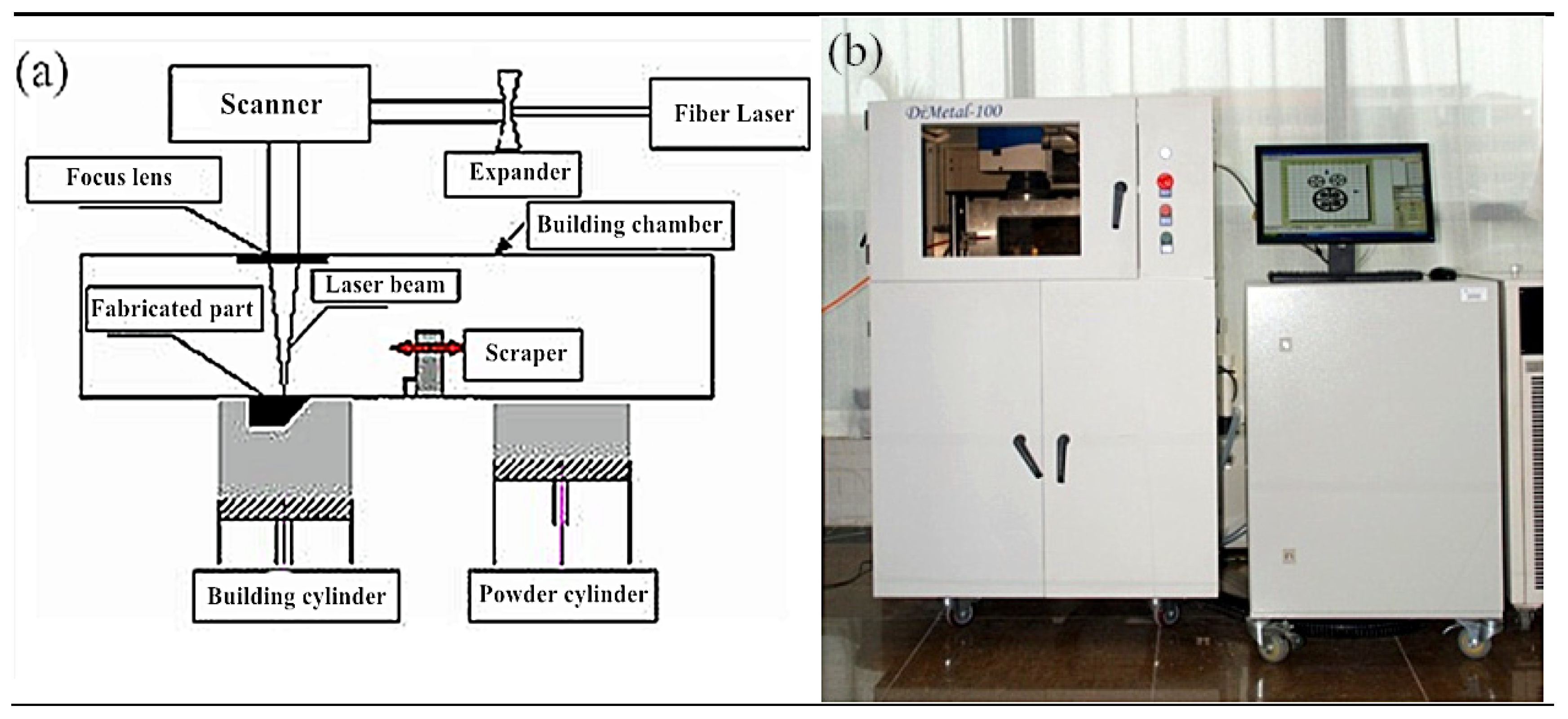
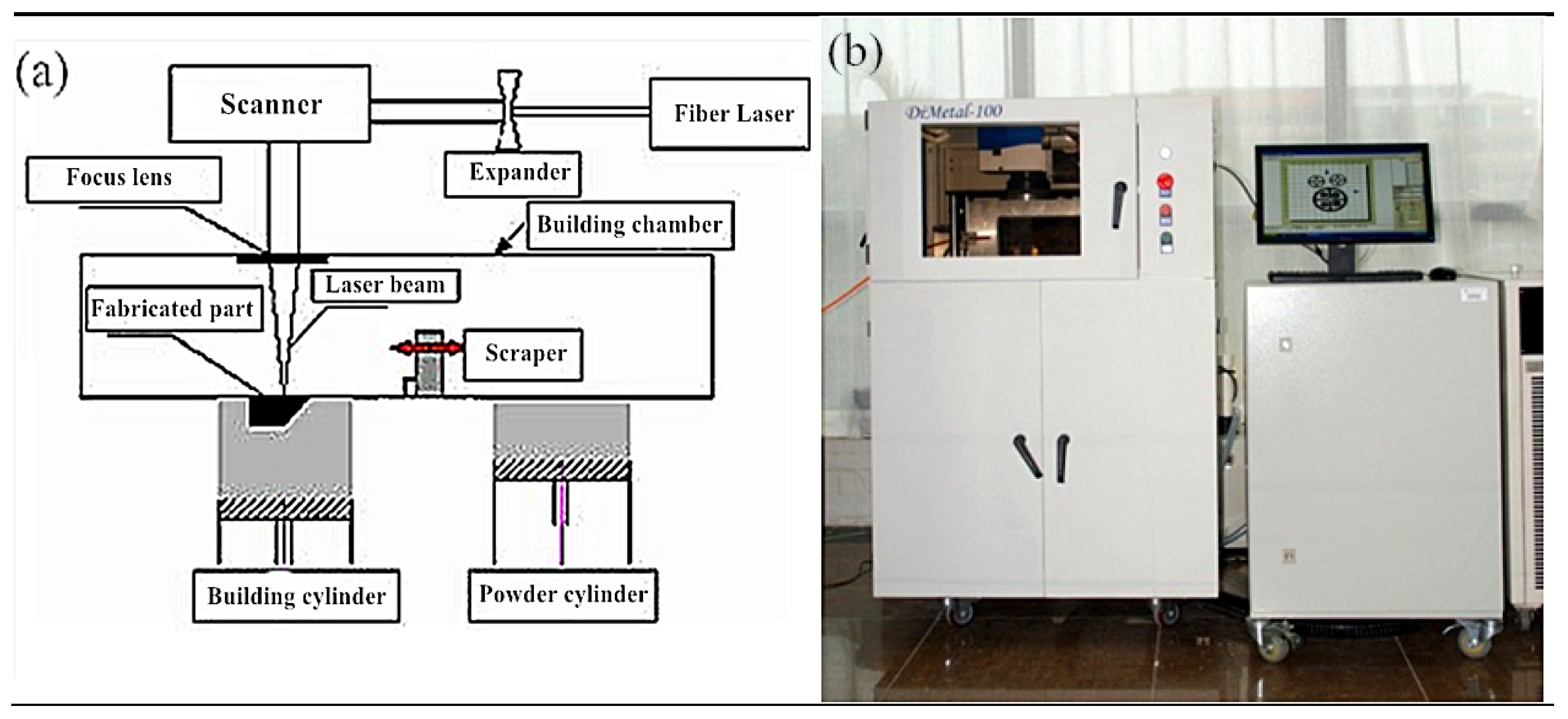
2.2. Manufacturing Method
2.3. Analytical Methods
3. Results and Discussion
3.1. Reverse Reconstruction of Tibial Implant
- ①
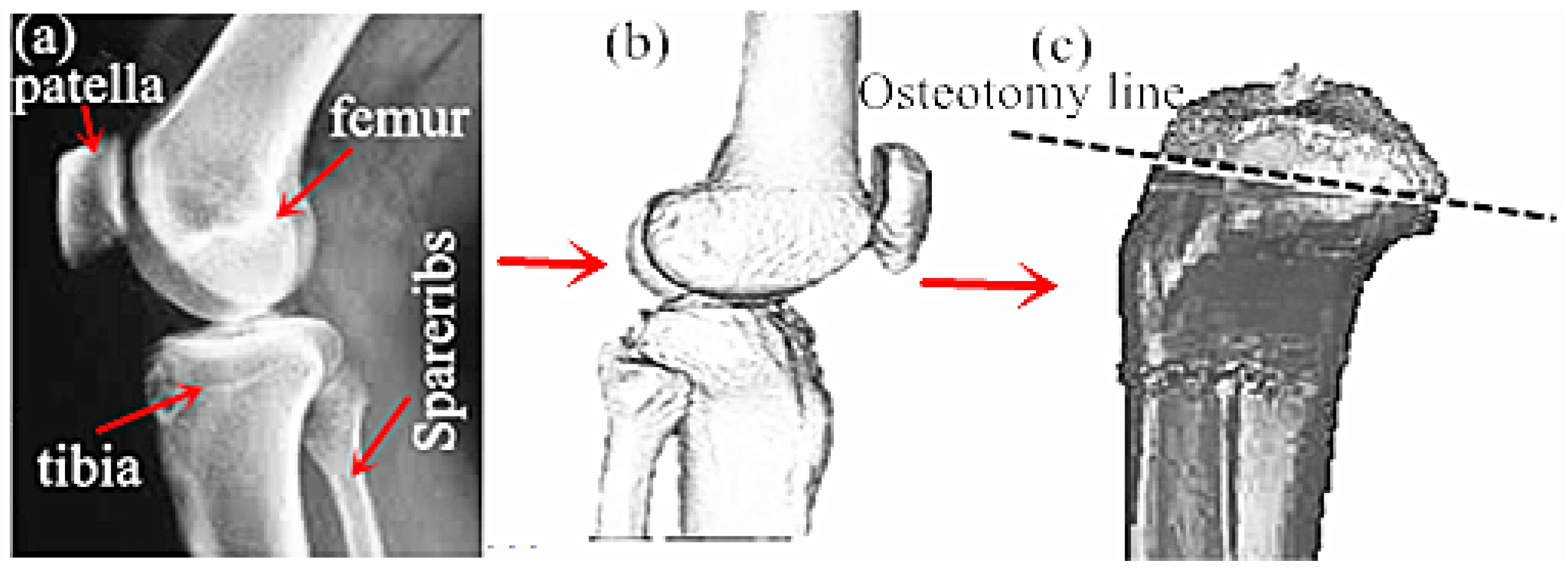
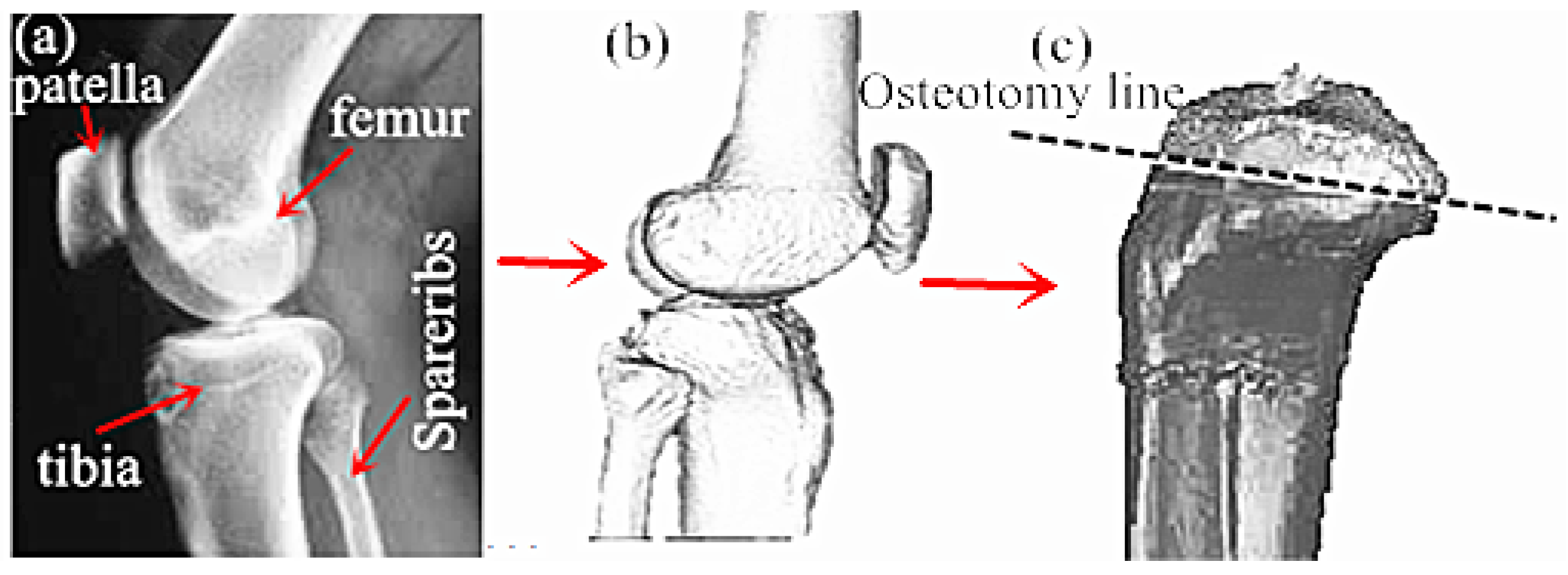
- First, CT or NMR was applied to scan the disease site in patients, so as to obtain the disease site images of patients. Subsequently, the CT scanned knee disease sites were imported into the Mimics. During the importing process, the correct orientation could be selected through the right-hand button in the Change orientation window, as shown in Figure 3a.
- ②
- The CT scanned images in Mimics were carried out with threshold segmentation. Then, the segmentation regions that were not connected to each other on the preliminary threshold segmentation mask were further divided into subgroups to generate the new mask. The soft tissue site was labeled as the starting point, and the ending point was labeled after the line had penetrated the bone. At this time, an intensity interface was produced, in which the prominent part represented the threshold.
- ③
- The images processed after threshold segmentation were carried out with a morphological operation, and some tiny burrs on the segmentation mask border were eliminated through the opening operation (first corrosion and then swelling). Then, the thresholding images were partitioned through the region growing manner to remove the floating pixel. The Calculate 3D Modles was adopted to complete the 3D reconstruction of the CT model. Finally, the 3D reconstructed implant model was processed with smoothing and denoising, so as to obtain the optimized 3D model, as presented in Figure 3b.
- ④
- The 3D reconstructed tibial implant model was imported into the Geomagic Studio for grid doctor repair, denoising, smoothing, simulation of bone cutting, and substantiation. The position of the simulated bone cutting line is shown in Figure 3c.
- ⑤
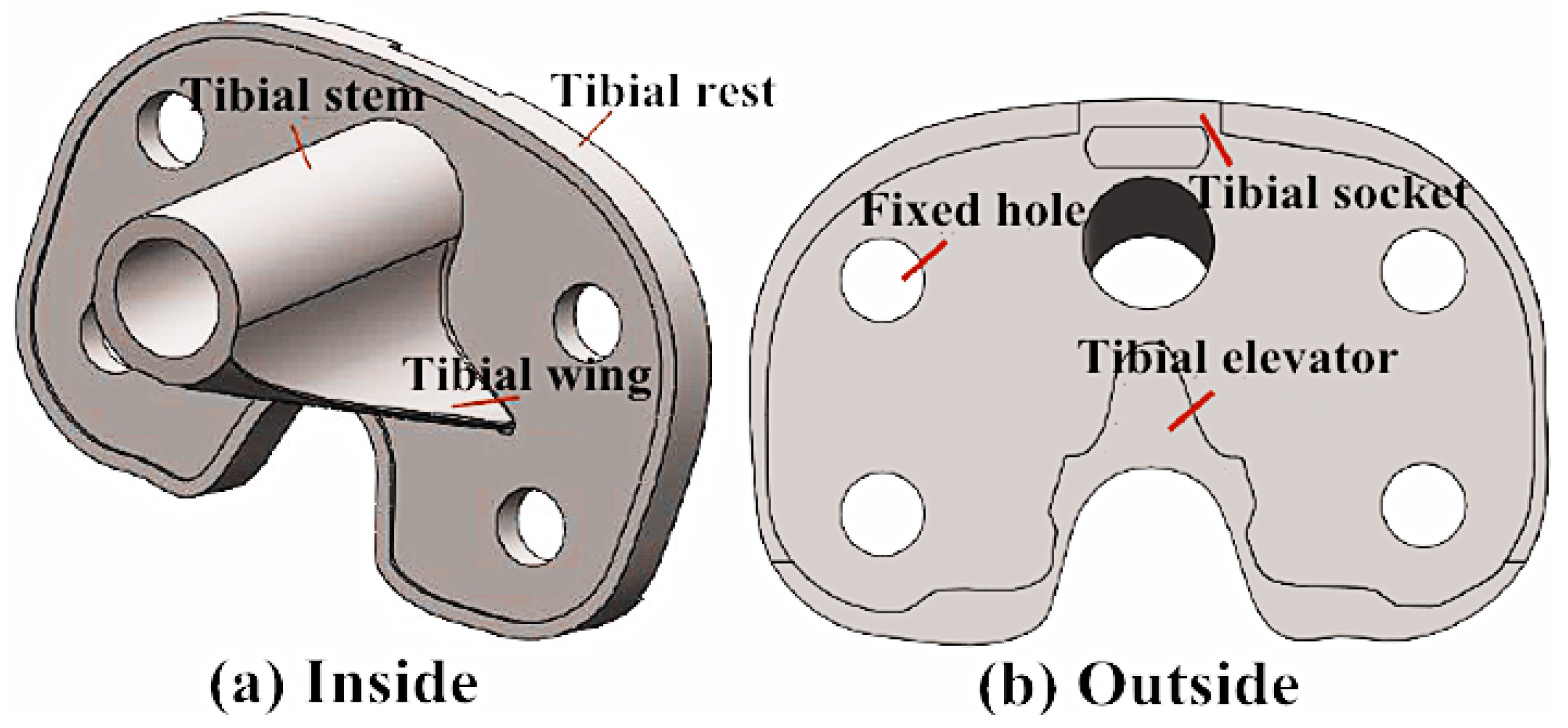
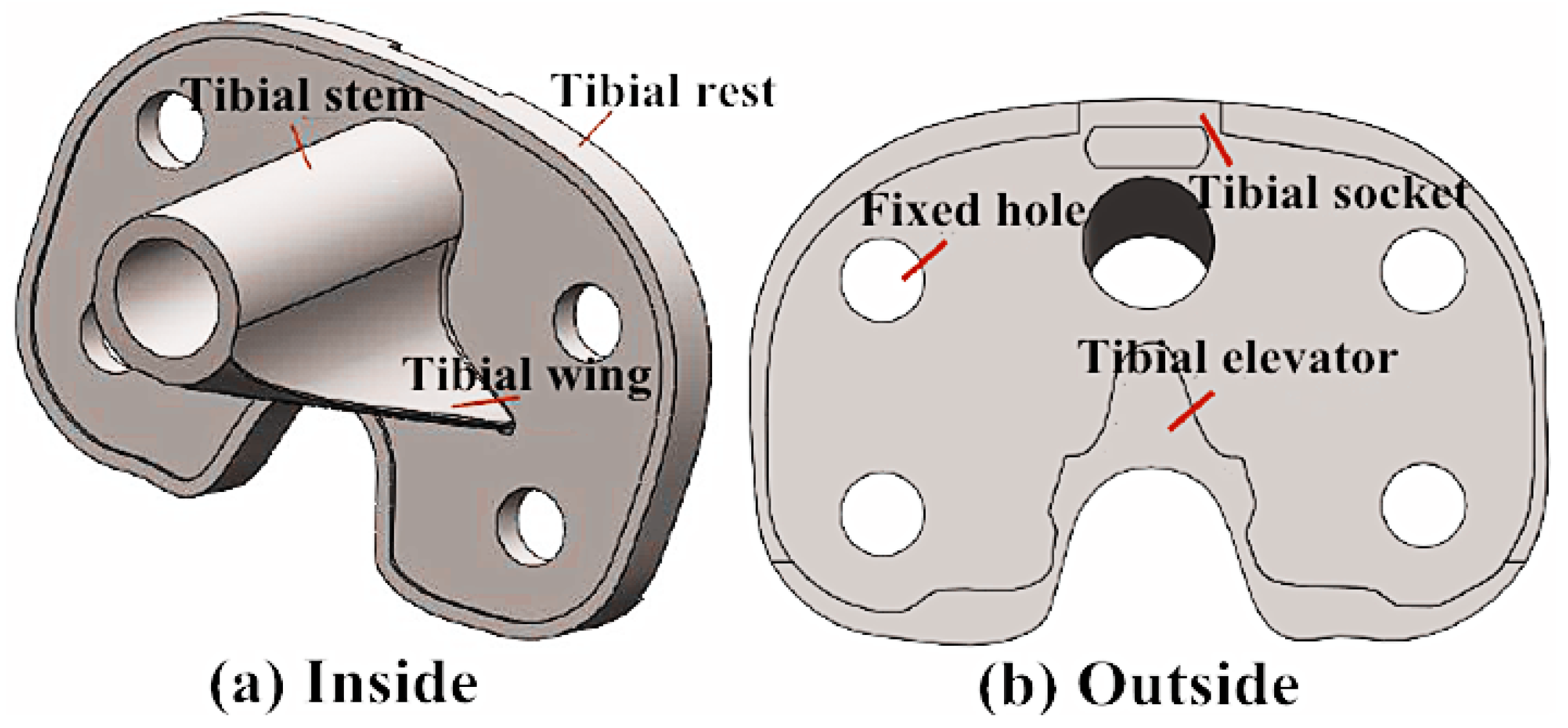
- The substantialized tibial implant bone cutting model was imported into the Rhinocero software for forward design, and the corresponding tibial implant model was selected based on the bone cutting surface size and status. Meanwhile, the size and shape of the tibial stem, tibial wing, tibial convex plate, tibial groove and tibial articular surface were adjusted to adapt to the tibial articular surface and complete the forward design of the tibial implant, as displayed in Figure 4.
3.2. Simulation Optimization Design of Tibial Implant
- ①
- The 3D reconstructed tibial model was imported into the Autodesk Inventor Professiona software, and all features of the reconstructed model were read, which were delivered to the Autodesk Simulation Mechanical for finite element simulation in the manner of document delivery.
- ②
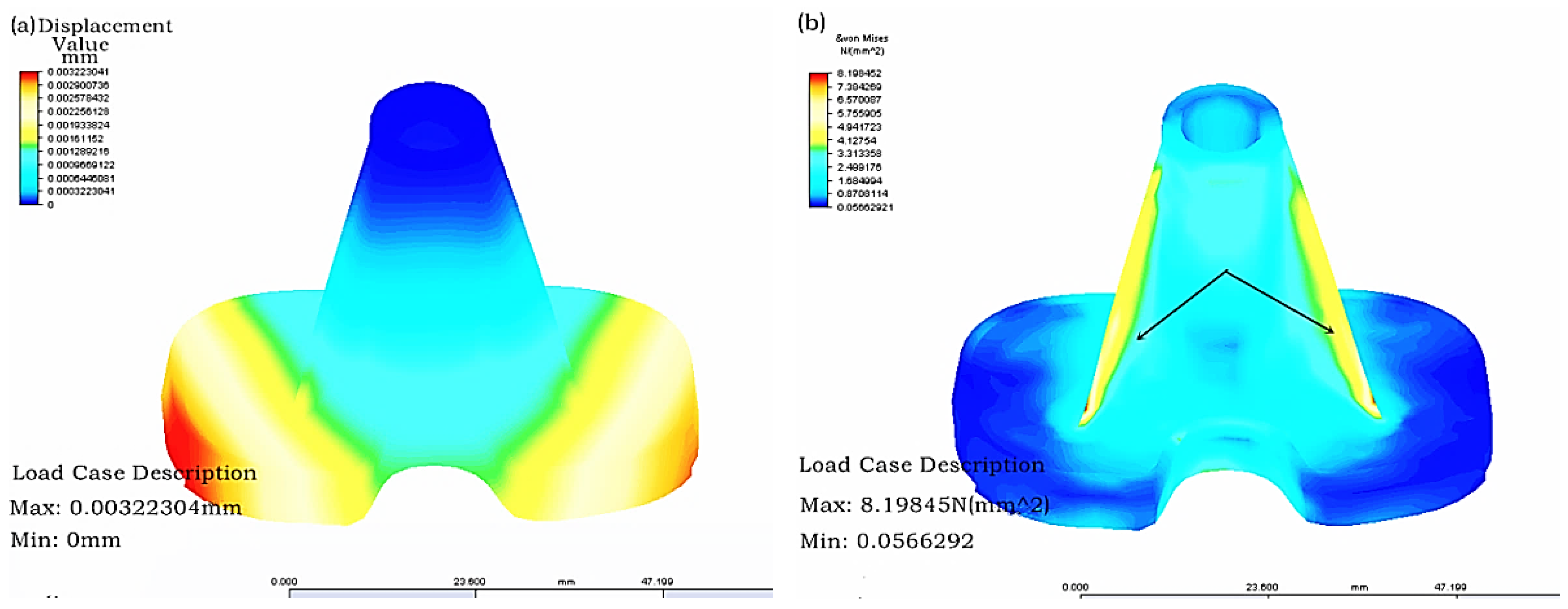
- First, grid partition was carried out, then the constraint conditions of the model with the material of CoCrMo alloy after grid partition were set, the proximal tibia was fixed and 20 N loading was applied on the tibial articular surface. Finally, the time step and solution manner were set for solving. The finite element stress analysis results of the tibial implant were displayed in Figure 5. As can be observed in Figure 5, the tibial implant displacement mainly took place in the tibial articular surface border, while stress concentration mainly happened in the tibial tendon. Therefore, the tibial strength could be increased while stress concentration could be reduced through increasing the tendon thickness and distribution area.
- ③
- The parameter control table in Autodesk Simulation Mechanical was opened to find the height and thickness parameters controlling the tibial tendon. The parameters were adjusted, the tendon thickness and distribution area were increased, and the updated model was confirmed.
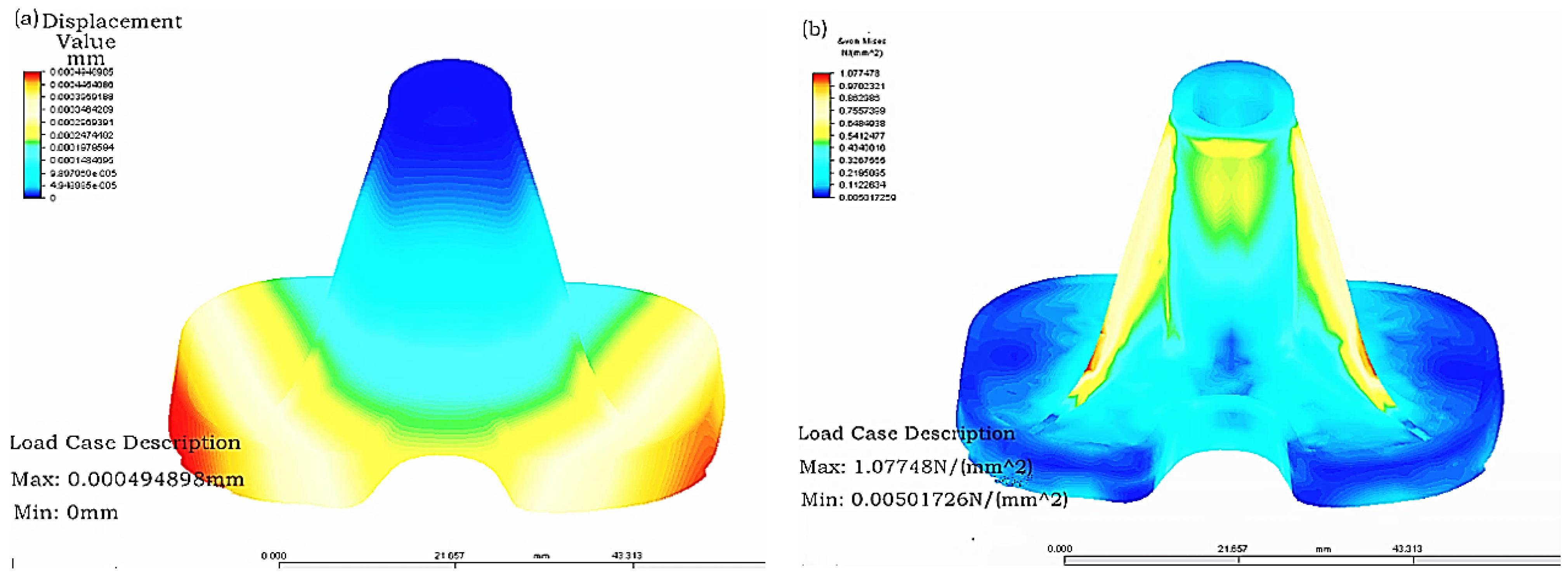
- ④
- The updated tibial model was carried out with grid partition, and the constraint conditions, loading, time step and solution manner of the model with the material of CoCrMo alloy after grid partition were set before finding a solution. The finite element stress analysis results of the optimized tibial implant were displayed in Figure 6. As can be seen in the figure, the maximal displacement of the optimized tibial model was changed from 0.00322 mm in the original model to 0.00049 mm. In addition, the maximal stress of the optimized tibial model was changed from 8.198 N (mm2) in the original model to 1.077 (mm2). Clearly, the displacement strain of the optimized model was greatly reduced, and the stress distribution was more homogeneous and had achieved the goal of increasing tibial strength and reducing stress concentration.
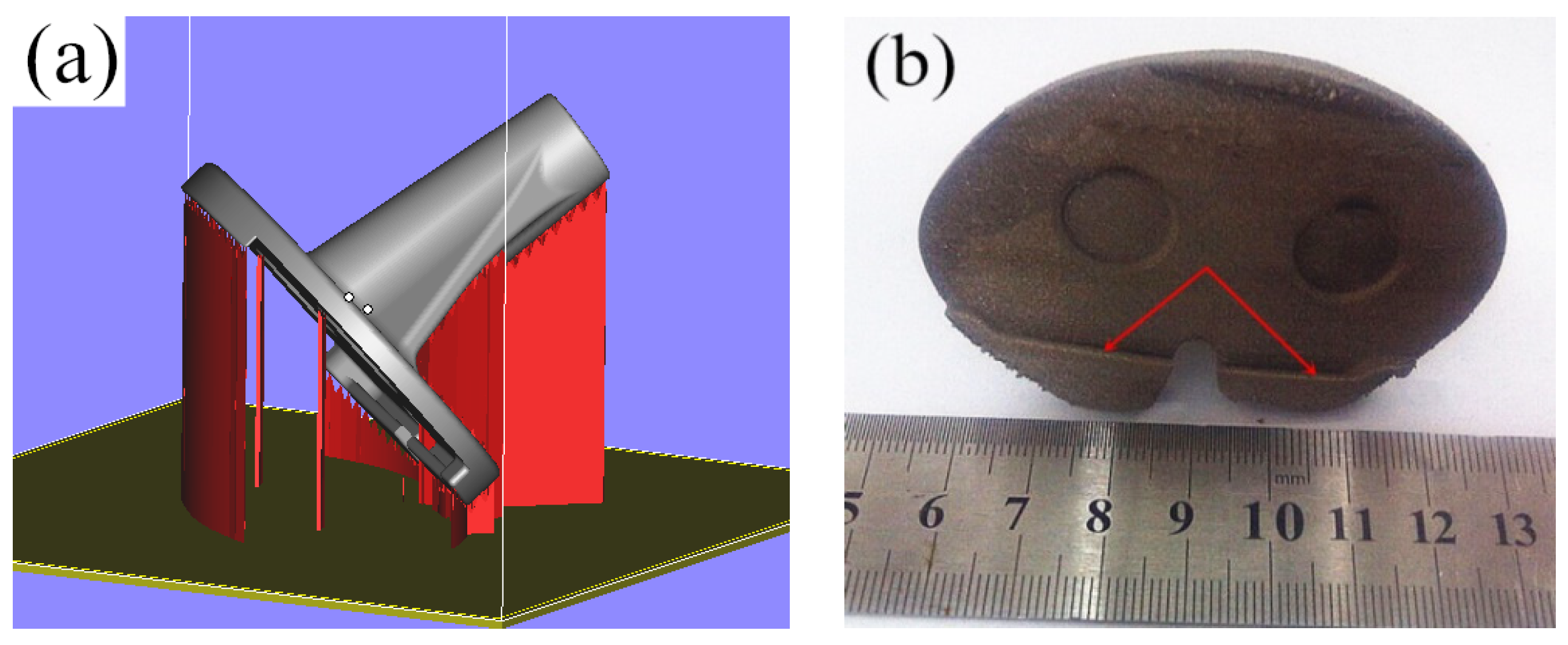
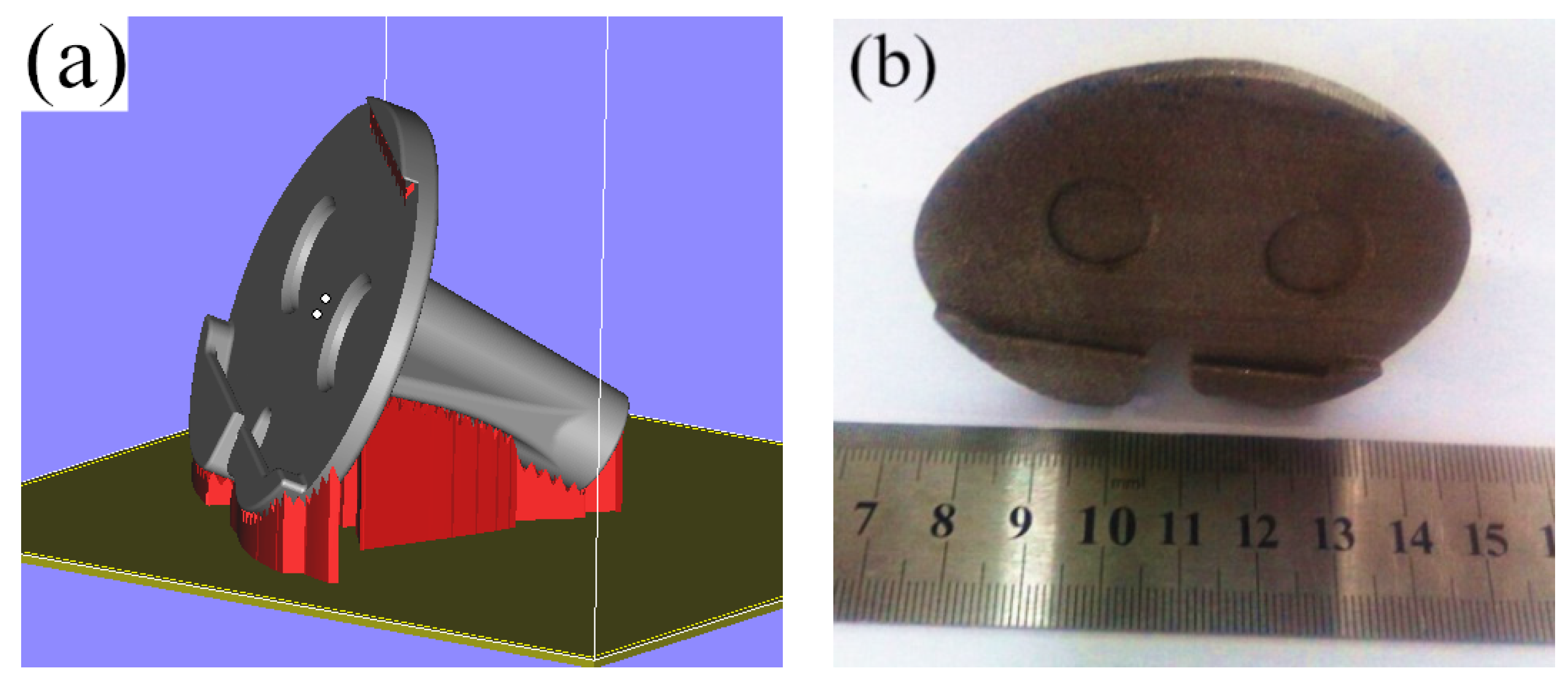
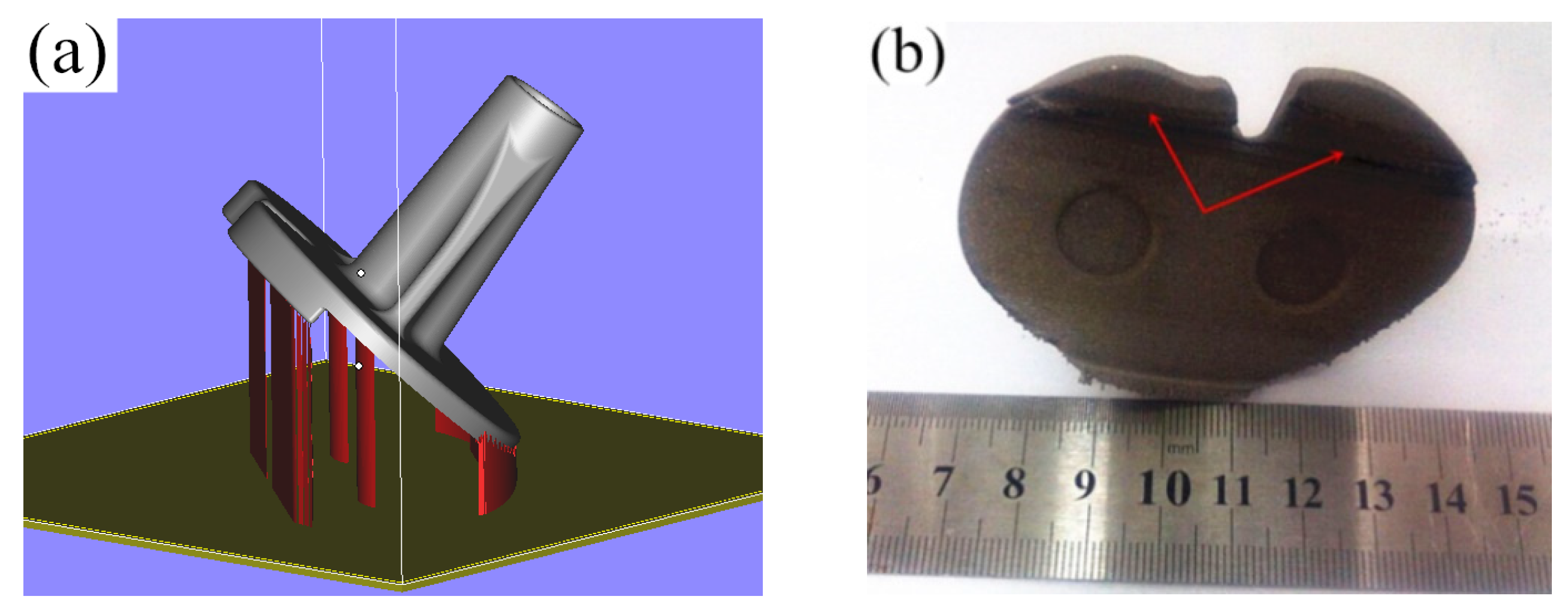
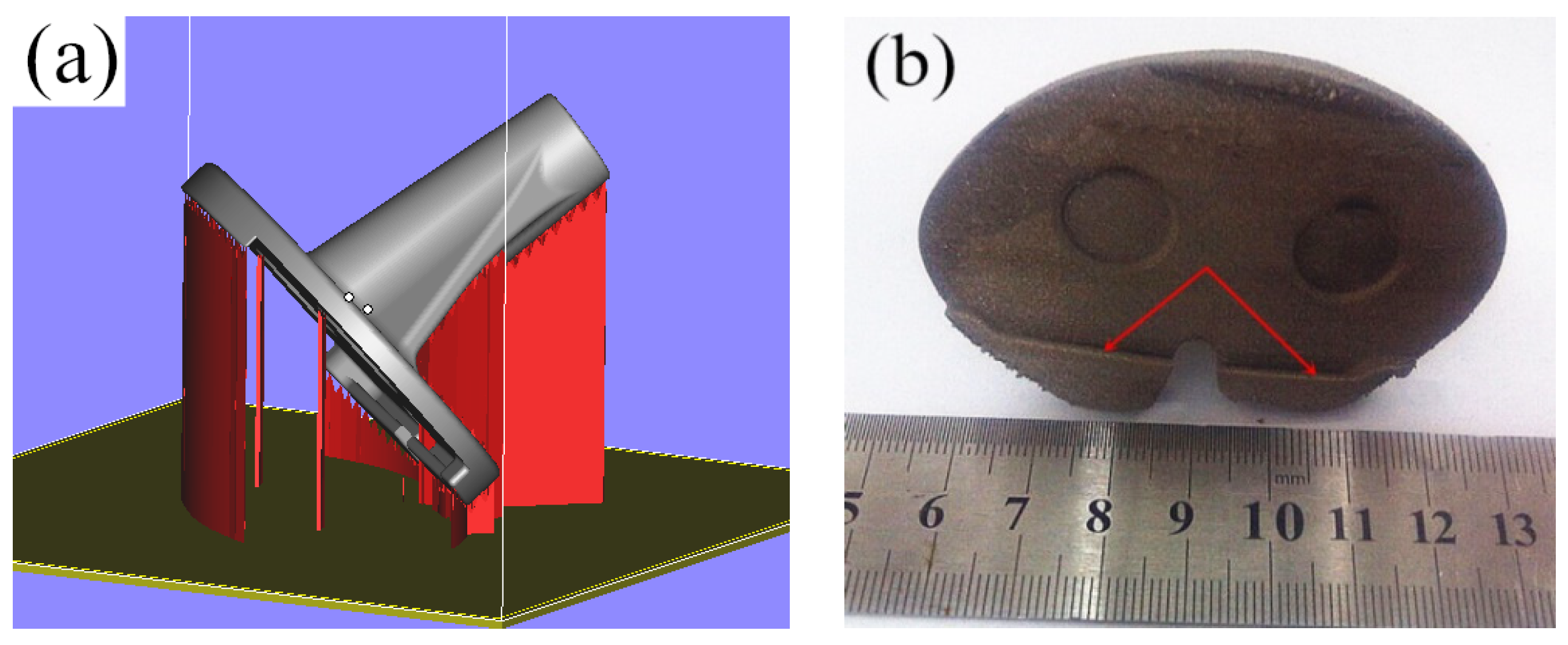
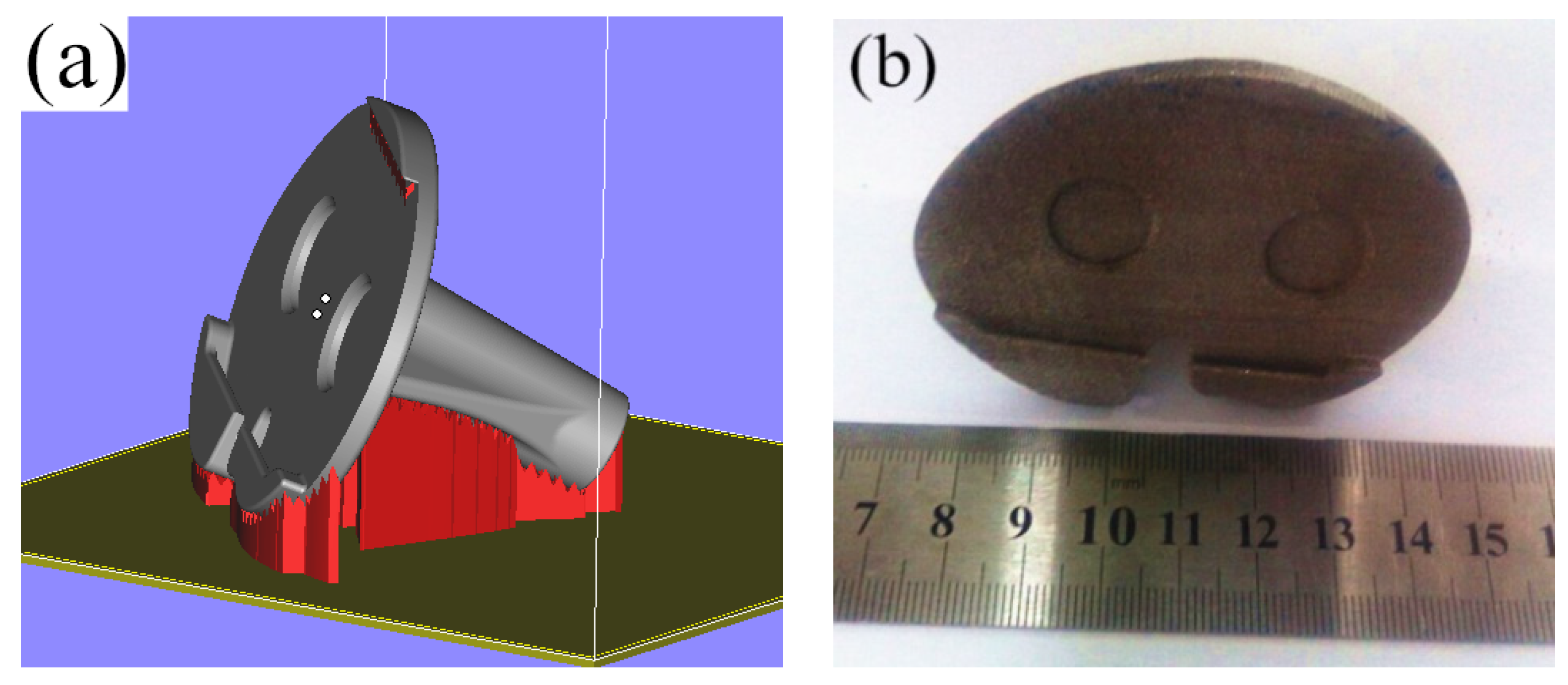
3.3. SLM Molding Tibial Implant Process Study
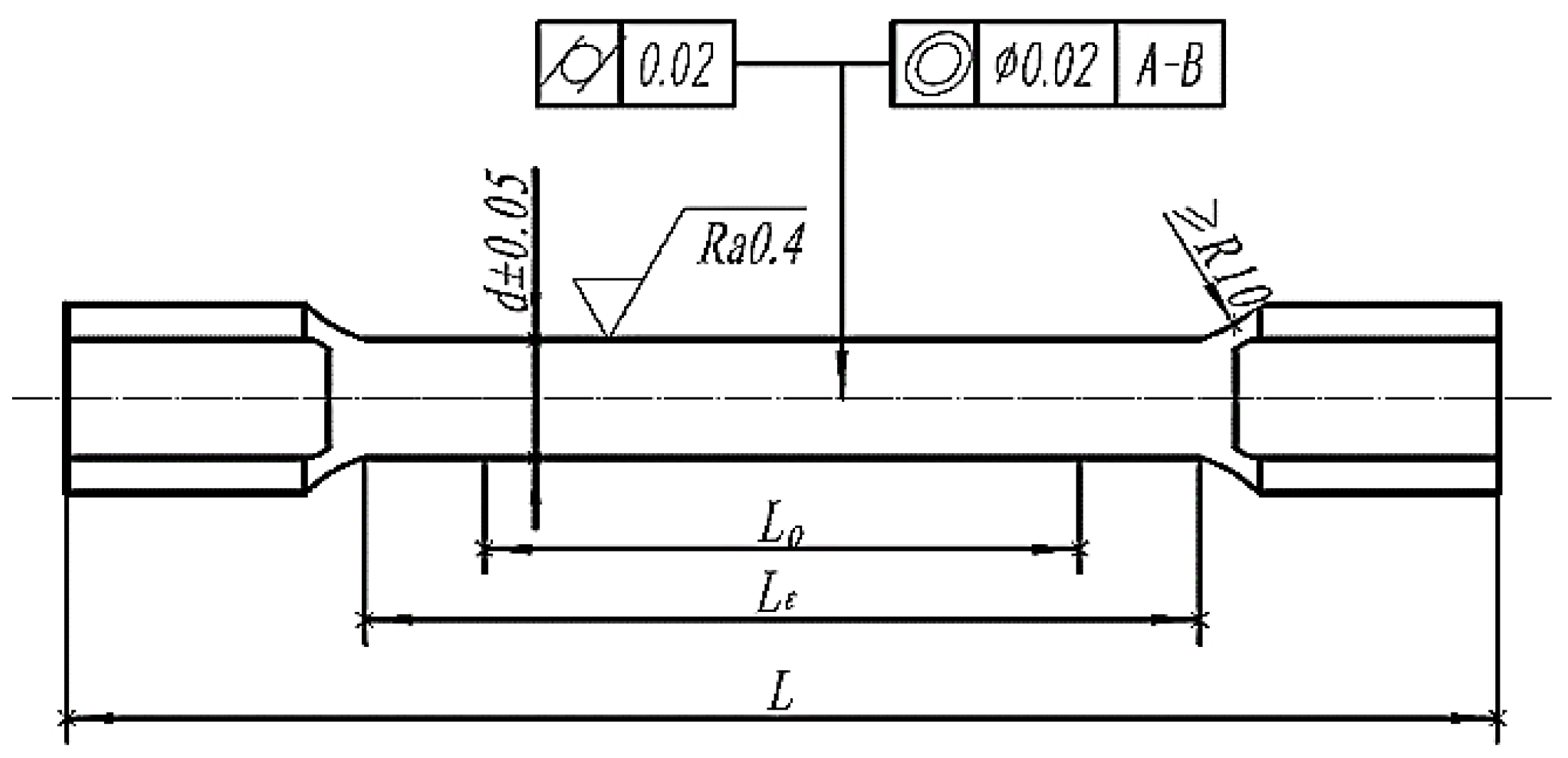
3.4. Tensile Property Study of the CoCrMo Alloy Part
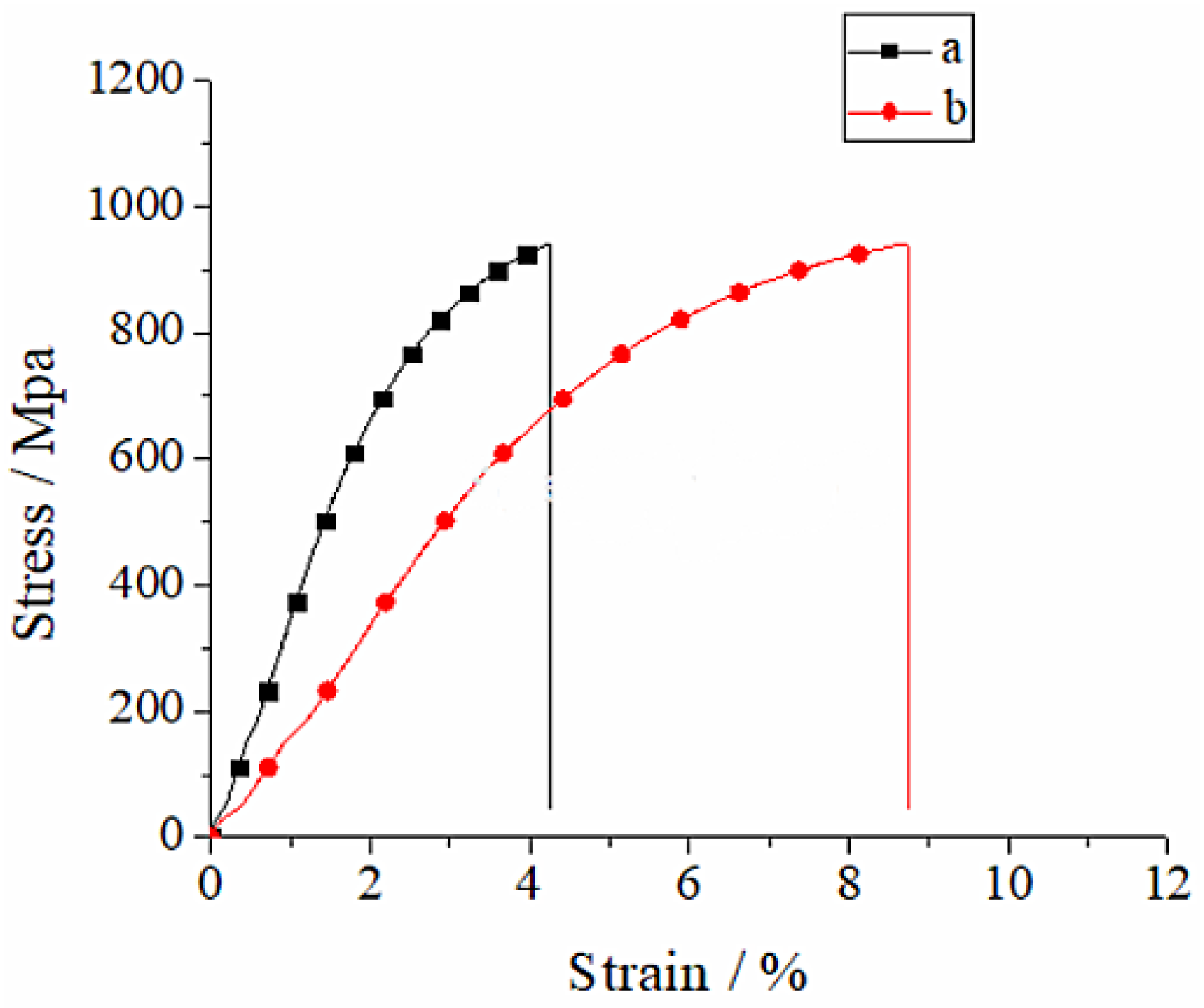
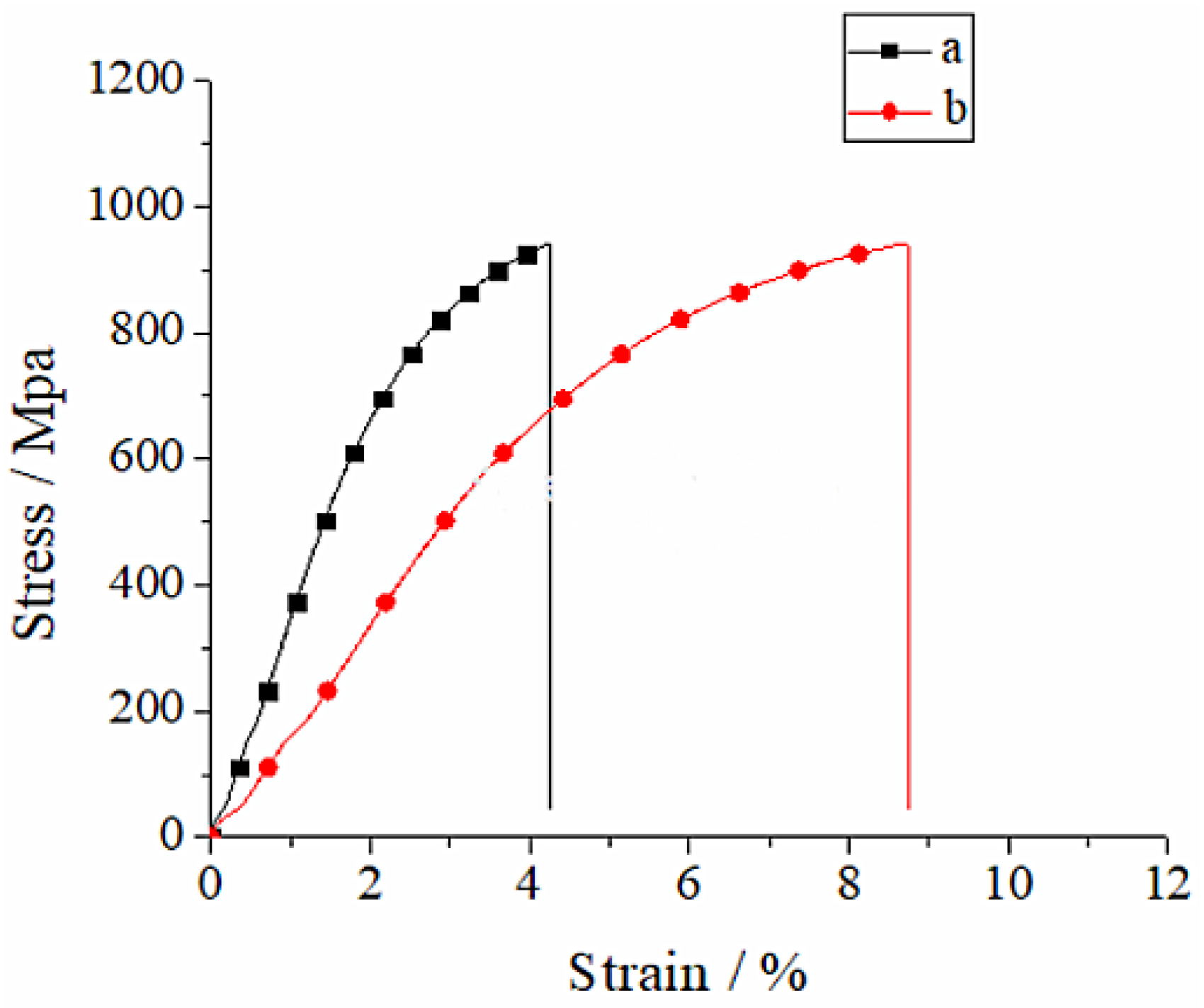
3.4.1. Stress–Strain Curve Analysis
3.4.2. Tensile Strength Analysis
4. Conclusions
- (1)
- Tibial implant is designed through the reversed combined with forward design methods, and the tibial implant model is optimized using the parametric FEM, which can minimize the stress concentration phenomenon of the implant part and realize the optimal distribution of force.
- (2)
- SLM molding tibial implant has a favorable molding effect after optimization of the molding techniques, with high tibial implant surface finish, but with no buckling deformation or obvious adhering slag.
- (3)
- The intensity of the SLM molding tibial implant can satisfy the implantation requirements, but it has a relatively high elasticity modulus, which should be solved with the heat treatment method in the future.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knutson, K.; Lewold, S.; Robertsson, O.; Lidgren, L. The swedish knee arthroplasty register. a nation-wide study of 30,003 knees 1976-1992. Acta Orthop. Scand. 1994, 65, 375–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blunn, G.W.; Joshi, A.B.; Minns, R.J.; Lidgren, L.; Lilley, P.; Ryd, L.; Engelbrecht, E.; Walker, P. Wear in retrieved condylar knee arthroplasties. a comparison of wear in different designs of 280 retrieved condylar knee prostheses. J. Arthroplast. 1997, 12, 281–290. [Google Scholar] [CrossRef]
- Bandyopadhyay, A.; Espana, F.; Balla, V.K.; Bose, S.; Ohgami, Y.; Davies, N.M. Influence of porosity on mechanical properties and in vivo response of ti6al4v implants. Acta Biomater. 2010, 6, 1640–1648. [Google Scholar] [CrossRef] [Green Version]
- Zhang, G.; Yang, Y.; Song, C.; Fu, F.; Zhang, Z. Study on biocompatibility of cocrmo alloy parts manufactured by selective laser melting. J. Med. Biol. Eng. 2018, 38, 76–86. [Google Scholar]
- Wei, L.; Liu, T.; Liao, W.; Jiang, L. Study on selective laser melting forming process of cobalt chromium alloy. Chin. J. Lasers 2015, 42, 63–70. [Google Scholar]
- Yang, Y.; Wang, D.; Wu, W. Research progress of direct manufacturing of metal parts by selective laser melting. Chin. J. Lasers 2011, 38, 0601007. [Google Scholar] [CrossRef]
- Song, C. Study on Digital Design and Direct Manufacturing of Customized Implant Based on Selective Laser Melting; South China University of Technology: Guangzhou, China, 2011. [Google Scholar]
- Chen, Z.; Zhang, Q.; Zhou, G.; Pang, Z.; Wei, Q. Three-dimensional parametric modeling during unicompartmental knee arthroplasty. Chin. J. Tissue Eng. Res. 2013, 4, 695. [Google Scholar]
- Wei, Z.; Li, H.; Xiong, X.; Zou, F.; Zou, Y. Treatment of severe tibial plateau fractures with 3D printed personalized plate internal fixation. Chin. J. Bone Jt. Inj. 2021, 36, 3. (In Chinese) [Google Scholar]
- Han, Y.; Kaken, H.; Zhao, W.; Wang, W.; Wang, L. Meta analysis of clinical efficacy of 3D printing assisted total knee arthroplasty. Biol. Orthop. Mater. Clin. Res. 2021, 18, 10. (In Chinese) [Google Scholar]
- Kumar, V.J.; Reddy, P.S.; Murthy, N.G. Modeling and biomechanical analysis of human knee joint. Int. J. Sci. Eng. Adv. Technol. 2014, 2, 246–252. [Google Scholar]
- Kumbhalkar, M.A.; Nawghare, U.; Ghode, R.; Deshmukh, Y.; Armarkar, B. Modeling and finite element analysis of knee prosthesis with and without implant. Univers. J. Comput. Math. 2013, 1, 56–66. [Google Scholar] [CrossRef]
- Abe, F.; Santos, E.C.; Kitamura, Y.; Osakada, K.; Shiomi, M. Influence of forming conditions on the titanium model in rapid prototyping with the selective laser melting process. Proc. Inst. Mech. Eng. Part C J. Mech. Eng. Sci. 2013, 217, 119–126. [Google Scholar] [CrossRef]
- Calignano, F. Design optimization of supports for overhanging structures in aluminum and titanium alloys by selective laser melting. Mater. Des. 2014, 64, 203–213. [Google Scholar] [CrossRef]
- Attarilar, S.; Ebrahimi, M.; Djavanroodi, F.; Fu, Y.; Wang, L.; Yang, J. 3D Printing technologies in metallic implants: A thematic review on the techniques and procedures. Int. J. Bioprint. 2021, 7, 306. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Experimental Direction | Modulus of Elasticity (Gpa) | Compressive Strength (Mpa) |
|---|---|---|---|
| Tibia | Longitudinal | 18.1 | 159 |
| Element | CoCrMo Powder | ASTM F1377 Standard | Element | CoCrMo Powder | ASTM F1377 Standard |
|---|---|---|---|---|---|
| Cr | 29.4% | 27–30% | C | 0.15% | <0.35% |
| Mo | 6% | 5–7% | Ni | 0.09% | <0.5% |
| Si | 0.8% | <1% | Al | <0.010% | <0.1% |
| Mn | 0.75% | <1% | Ti | <0.010% | <0.1% |
| Fe | 0.26% | <0.75% | W | <0.010% | <0.2% |
| N | 0.19% | <0.25% | Co | Balance | Balance |
| Sample | Tensile Strength (Mpa) | Modulus of Elasticity (Gpa) | Extensibility A(%) |
|---|---|---|---|
| Cast | 985.92 | 264.4 | 8.76 |
| SLM | 978.96 | 627.8 | 4.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, G.; Li, J.; Zhou, X.; Zhou, Y.; Wang, A. Optimal Design and Processing Technology of 3D Printed Tibial Implants. Coatings 2022, 12, 561. https://doi.org/10.3390/coatings12050561
Zhang G, Li J, Zhou X, Zhou Y, Wang A. Optimal Design and Processing Technology of 3D Printed Tibial Implants. Coatings. 2022; 12(5):561. https://doi.org/10.3390/coatings12050561
Chicago/Turabian StyleZhang, Guoqing, Junxin Li, Xiaoyu Zhou, Yongsheng Zhou, and Anmin Wang. 2022. "Optimal Design and Processing Technology of 3D Printed Tibial Implants" Coatings 12, no. 5: 561. https://doi.org/10.3390/coatings12050561
APA StyleZhang, G., Li, J., Zhou, X., Zhou, Y., & Wang, A. (2022). Optimal Design and Processing Technology of 3D Printed Tibial Implants. Coatings, 12(5), 561. https://doi.org/10.3390/coatings12050561