
Hypothetical Mechanism of Skin Argyria


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
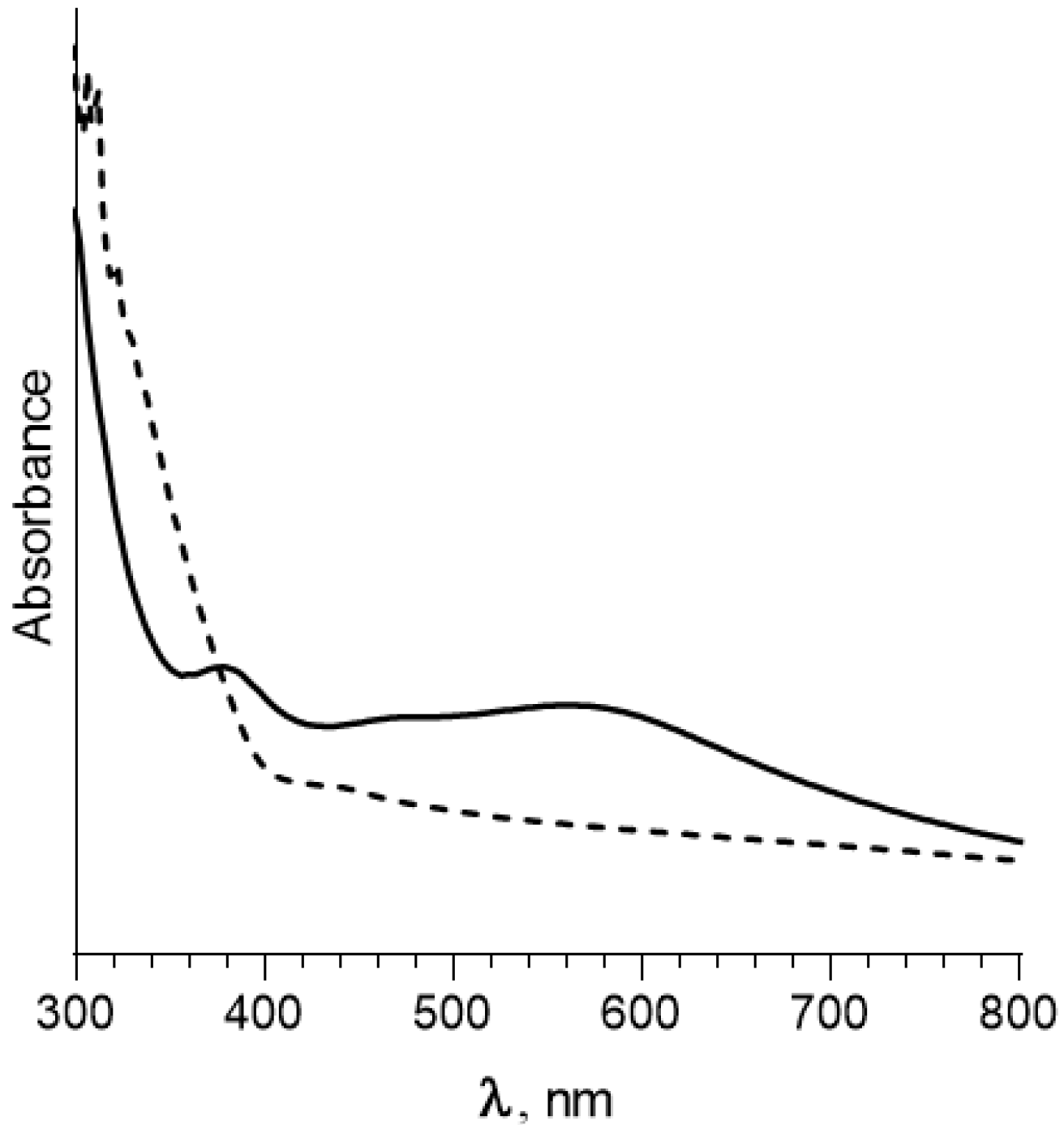
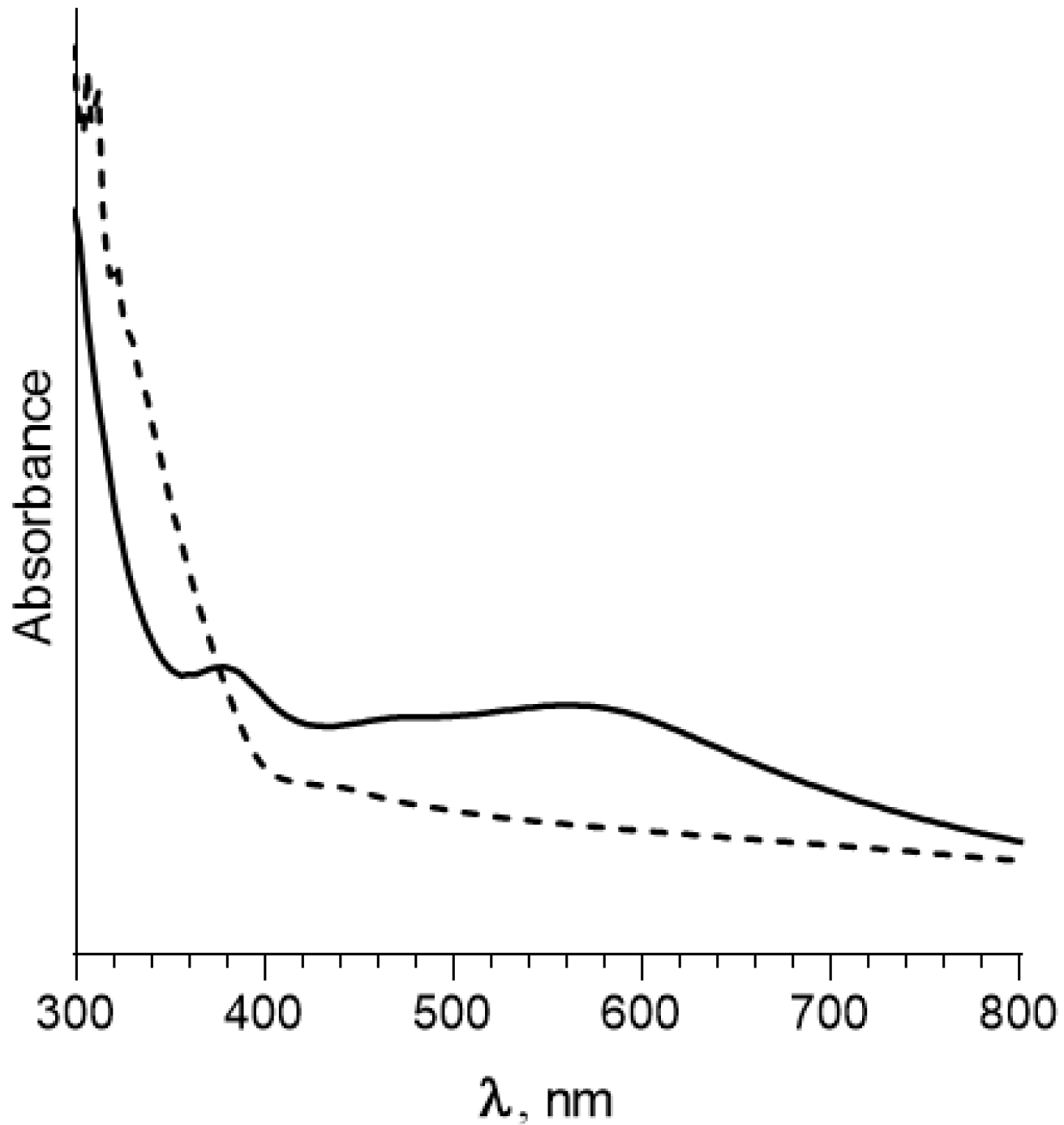
3.1. Experiment No. 1. Effect of Illumination on Silver Chloride in Solution
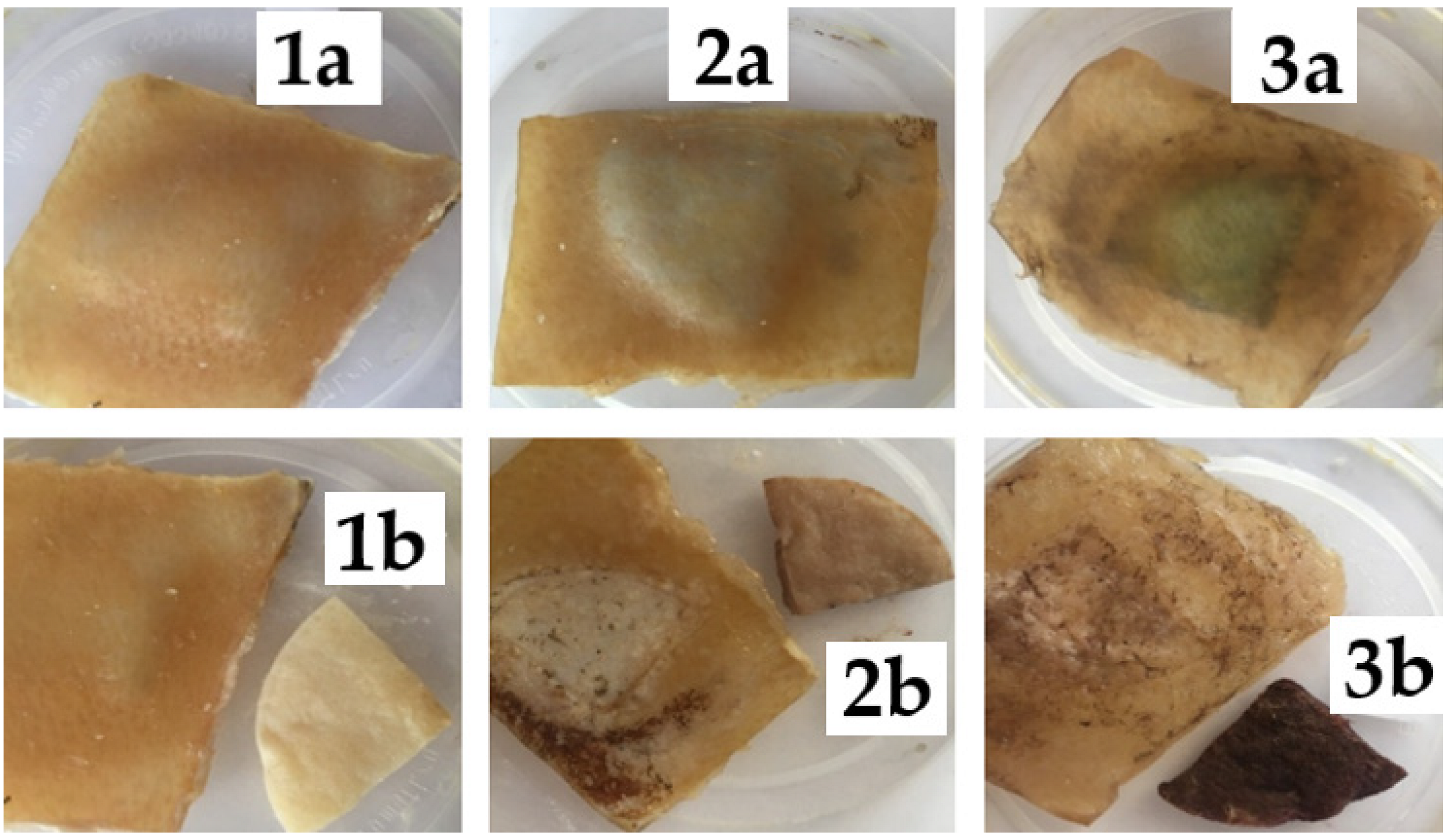
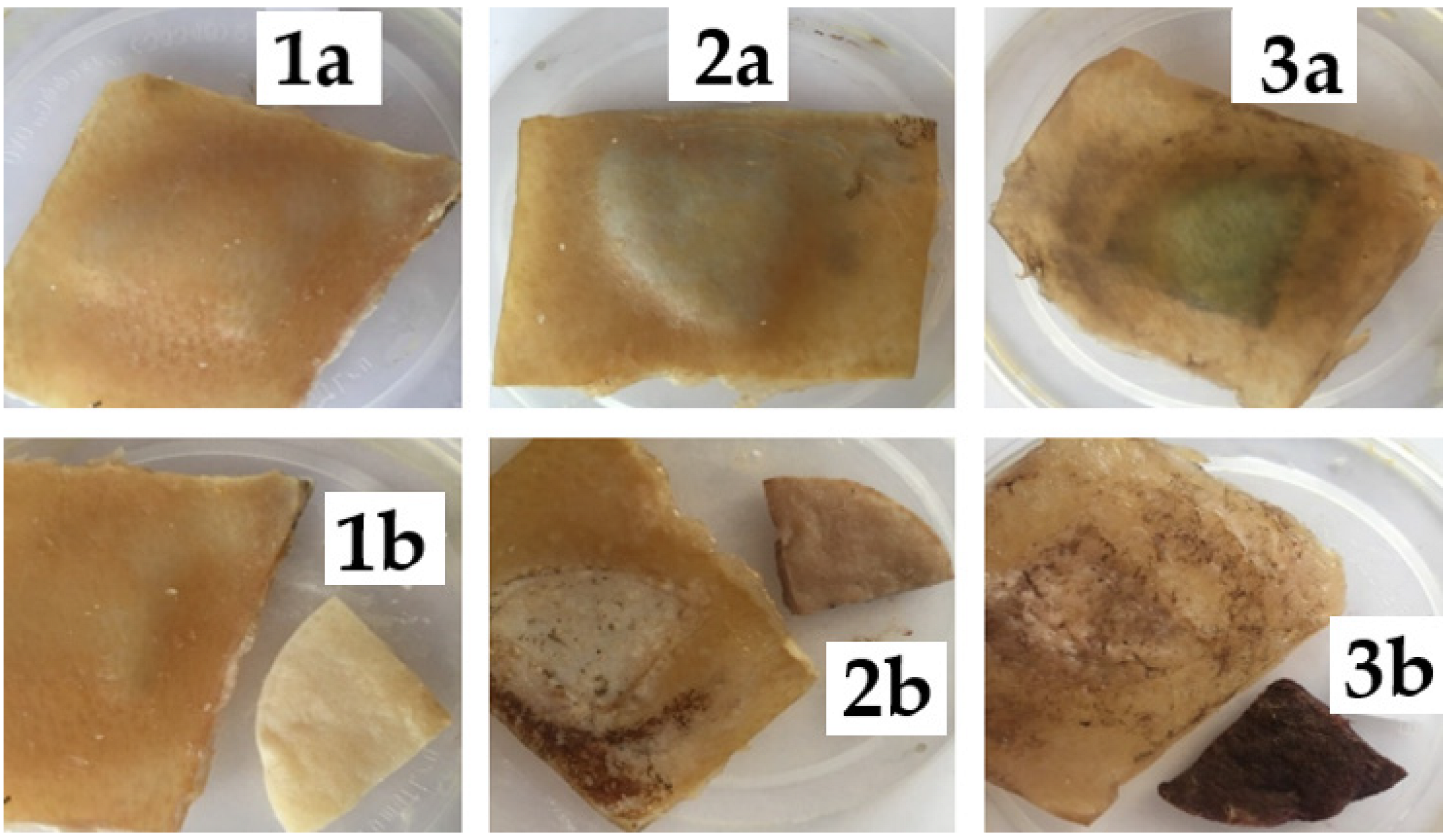
3.2. Experiment No. 2. Effect of Illumination on Silver Chloride under Pig Skin
3.3. Experiment No. 3. Storage under Different Conditions of Silver Chloride Sol in a Solution Simulating Sweat
3.4. Experiment No. 4. “Interaction of Silver Chloride Sol with Sodium Thiosulfate Solution”
4. Discussion
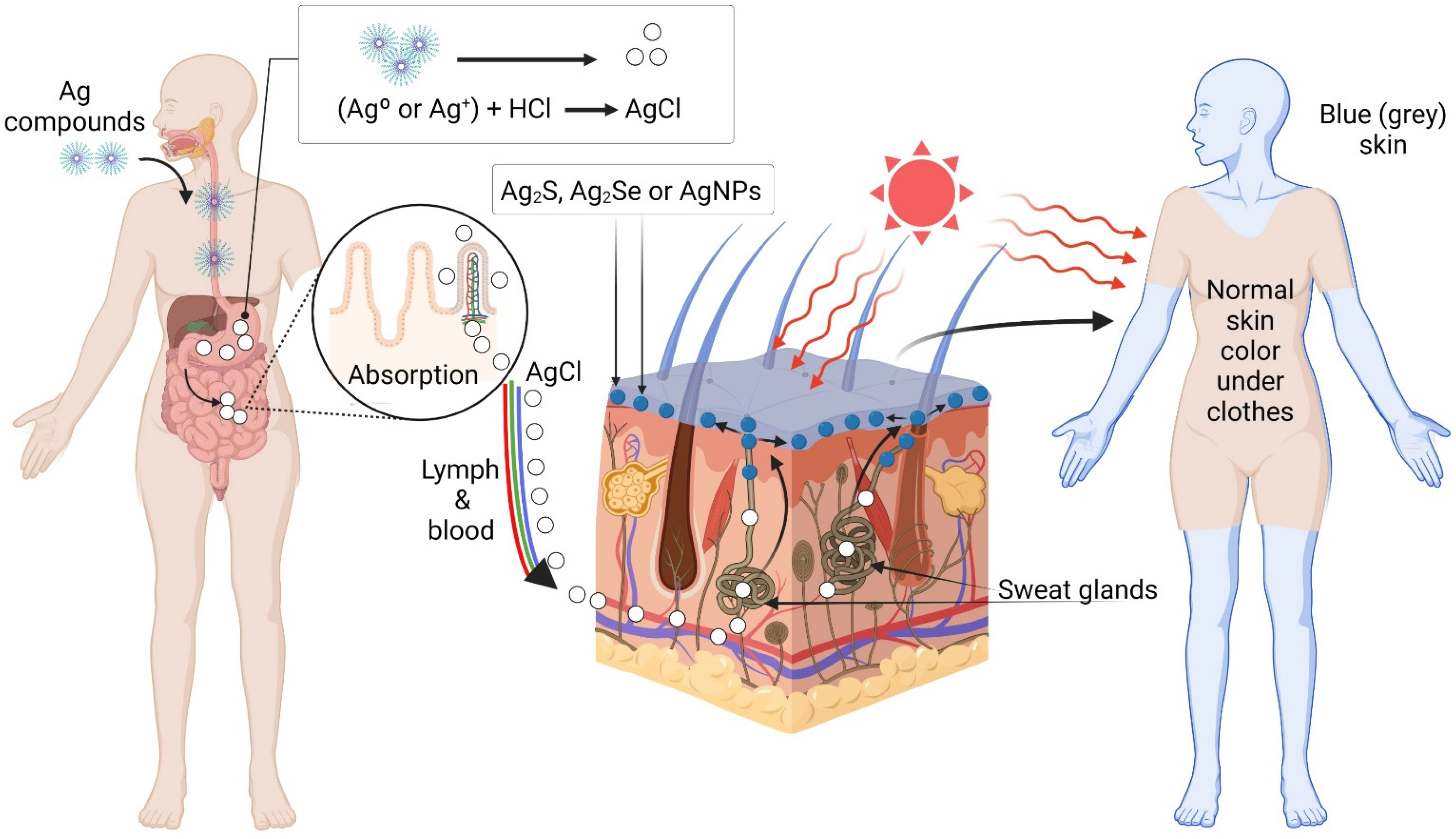
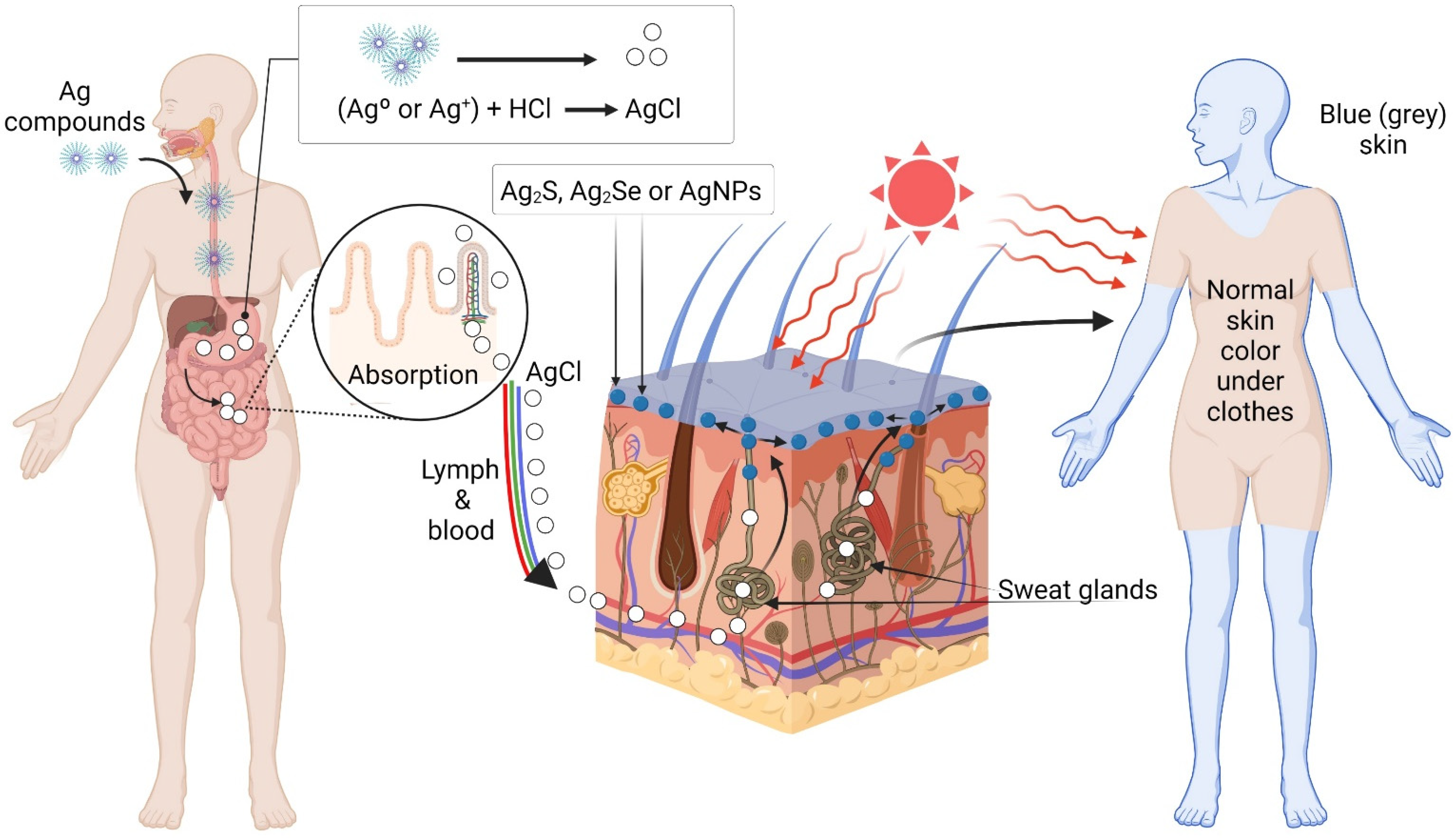
- Silver particles are predominantly located near the mouth and in the area of the sweat gland membranes [39]. This indicates that the delivery of silver compounds (from which metallic silver particles are formed) directly to the skin occurs along with sweat through the perspiration system.
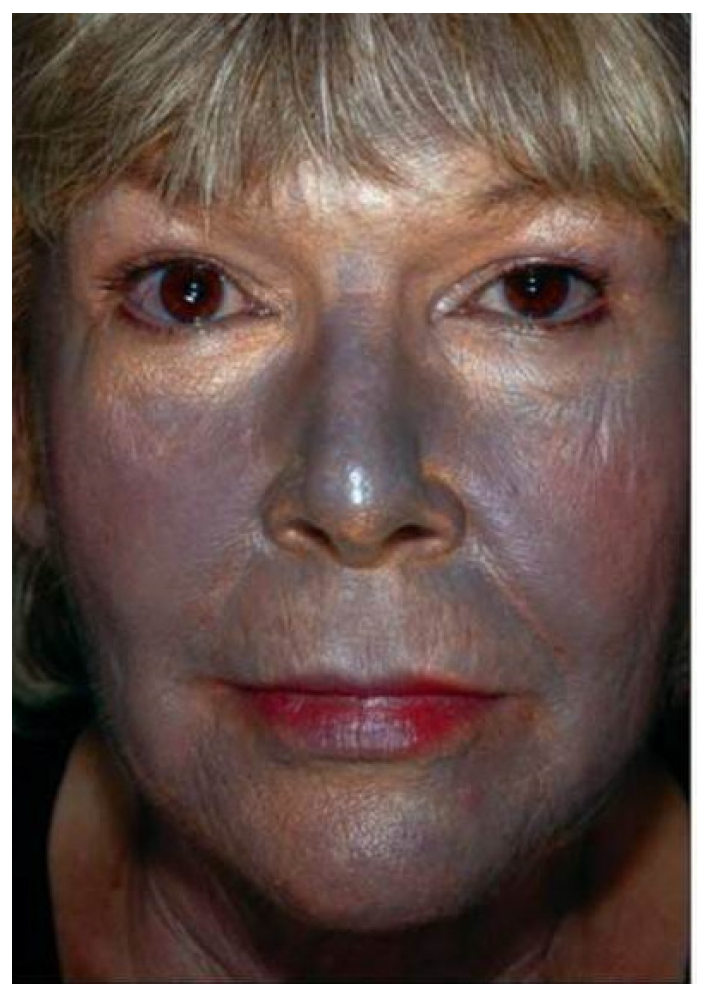
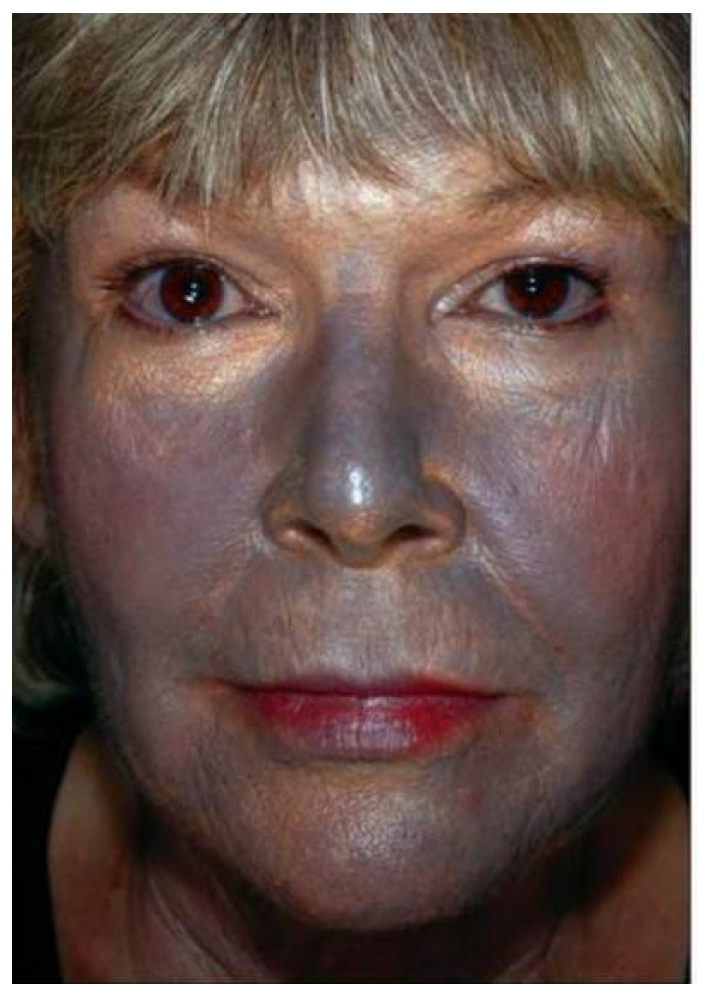
- Skin discoloration was observed predominantly on the body areas exposed to direct sunlight. The skin on the parts of the body covered by clothing (buttocks, thighs, etc.) retained its natural flesh color [40]. This indicates that sunlight is involved in the emergence and development of skin argyria.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blagitko, E.M.; Burmistrov, V.A.; Kolesnikov, A.P.; Mikhailov, Y.u.I.; Rodionov, P.P. Silver in Medicine; Nauka-Centr: Novosibirsk, Russia, 2004. [Google Scholar]
- Ahamed, M.; AlSalhi, M.; Siddiqui, M. Silver nanoparticle applications and human health. Clin. Chim. Acta 2010, 411, 1841–1848. [Google Scholar] [CrossRef] [PubMed]
- Burmistrov, V.A.; Burmistrov, A.V. Biosilver Is Good to Health! 2014. Available online: http://vector-vita.narod.ru/Documents/papers/2014-biosilver.pdf (accessed on 18 December 2021).
- Zhang, C.; Hu, Z.; Deng, B. Silver nanoparticles in aquatic environments: Physiochemical behavior and antimicrobial mechanisms. Water Res. 2016, 88, 403–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klippstein, R.; Fernandez-Montesinos, R.; Castillo, P.M.; Zaderenko Ana, P.; Pozo, D. Silver Nanoparticles Interactions with the Immune System: Implications for Health and Disease. In Silver Nanoparticles; Perez, I.D.P., Ed.; IntechOpen: Rijeka, Croatia, 2020; p. 309. [Google Scholar]
- Galdiero, S.; Falanga, A.; Vitiello, M.; Cantisani, M.; Marra, V.; Galdiero, M. Silver Nanoparticles as Potential Antiviral Agents. Molecules 2011, 16, 8894–8918. [Google Scholar] [CrossRef] [Green Version]
- Valenzuela-Salas, L.M.; Girón-Vázquez, N.G.; García-Ramos, J.C.; Torres-Bugarín, O.; Gómez, C.; Pestryakov, A.; Villarreal-Gómez, L.J.; Toledano-Magaña, Y.; Bogdanchikova, N. Antiproliferative and Antitumour Effect of Nongenotoxic Silver Nanoparticles on Melanoma Models. Oxidative Med. Cell. Longev. 2019, 2019, 4528241. [Google Scholar] [CrossRef]
- Rai, M.K.; Deshmukh, S.D.; Ingle, A.P.; Gade, A.K. Silver nanoparticles: The powerful nanoweapon against multidrug-resistant bacteria. J. Appl. Microbiol. 2012, 112, 841–852. [Google Scholar] [CrossRef]
- Vazquez-Munoz, R.; Avalos-Borja, M.; Castro-Longoria, E. Ultrastructural Analysis of Candida albicans When Exposed to Silver Nanoparticles. PLoS ONE 2014, 9, e108876. [Google Scholar] [CrossRef]
- Dos Santos, C.A.; Seckler, M.; Ingle, A.P.; Gupta, I.; Galdiero, S.; Galdiero, M.; Gade, A.; Rai, M. Silver Nanoparticles: Therapeutical Uses, Toxicity, and Safety Issues. J. Pharm. Sci. 2014, 103, 1931–1944. [Google Scholar] [CrossRef]
- Valenzuela-Salas, L.M.; Blanco-Salazar, A.; Perrusquía-Hernández, J.D.; Nequiz-Avendaño, M.; Mier-Maldonado, P.A.; Ruiz-Ruiz, B.; Campos-Gallegos, V.; Arellano-García, M.E.; García-Ramos, J.C.; Pestryakov, A.; et al. New Protein-Coated Silver Nanoparticles: Characterization, Antitumor and Amoebicidal Activity, Antiproliferative Selectivity, Genotoxicity, and Biocompatibility Evaluation. Pharmaceutics 2021, 13, 65. [Google Scholar] [CrossRef]
- Semenov, F.V.; Kachanova, O.A.; Fidarova, K.M. Experimental base for use of topical prescriptions containing silver nanoparticles in treatment of P. Aeruginosa and Acinetobacter Sp. infections in otorhinolaryngology. Russ. Otorhinolaryngol. 2013, 5, 88–90. [Google Scholar]
- Fidarova, K.M.; Babichev, S.A.; Kachanova, O.A. Perspectives of Ag-nanoparticles containing medications in the treatment of ENT infections caused by S. aureus. Russ. Otorhinolaryngol. 2015, 5, 127–129. [Google Scholar]
- Rai, M.; Deshmukh, S.D.; Ingle, A.P.; Gupta, I.R.; Galdiero, M.; Galdiero, S. Metal nanoparticles: The protective nanoshield against virus infection. Crit. Rev. Microbiol. 2016, 42, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.; Wang, P.; Bai, R.; Cong, Y.; Suo, S.; Ren, X.; Chen, C. Inhibitory effect of silver nanomaterials on transmissible virus-induced host cell infections. Biomaterials 2014, 35, 4195–4203. [Google Scholar] [CrossRef] [PubMed]
- Khandelwal, N.; Kaur, G.; Chaubey, K.K.; Singh, P.; Sharma, S.; Tiwari, A.; Singh, S.V.; Kumar, N. Silver nanoparticles impair Peste des petits ruminants virus replication. Virus Res. 2014, 190, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Speshock, J.L.; Murdock, R.C.; Braydich-Stolle, L.K.; Schrand, A.M.; Hussain, S.M. Interaction of silver nanoparticles with Tacaribe virus. J. Nanobiotechnol. 2010, 8, 19. [Google Scholar] [CrossRef] [Green Version]
- Borrego, B.; Lorenzo, G.; Mota-Morales, J.D.; Almanza-Reyes, H.; Mateos, F.; López-Gil, E.; de la Losa, N.; Burmistrov, V.A.; Pestryakov, A.; Brun, A.; et al. Potential application of silver nanoparticles to control the infectivity of Rift Valley fever virus in vitro and in vivo. Nanomed. Nanotechnol. Biol. Med. 2016, 12, 1185–1192. [Google Scholar] [CrossRef]
- Almanza-Reyes, H. Evaluation of silver nanoparticles for the prevention of SARS-CoV-2 infection in health workers: In vitro and in vivo. PLoS ONE 2021, 16, e0256401. [Google Scholar] [CrossRef]
- Almonaci-Hernández, C.A.; Clinic, E.I.A.A.; Juarez-Moreno, K.O.; ECastañeda-Juarez, M.E.; Almanza-Reyes, H.; Pestryakov, A.; Bogdanchikova, N. Silver Nanoparticles for the Rapid Healing of Diabetic Foot Ulcers. Int. J. Med. Nano Res. 2017, 4, 19. [Google Scholar] [CrossRef] [Green Version]
- Gyusan, A.O.; Uraskulova, B.B.; Academy, F.S.B.E.I.O.H.V.E.N.C.S.H.T.; Hospital, C.R.S.B.P.A.T.F.R.C.; Dispensary, C.R.S.B.P.A.T.F.K.-C.R.A. The Problems of Tuberculosis in Otorhinolaryngology. Russ. Otorhinolaryngol. 2017, 89, 32–38. [Google Scholar] [CrossRef]
- Uraskulova, B.B.; Gyusan, A.O. The clinical and bacteriological study of the effectiveness of the application of silver nanoparticle for the treatment of tuberculosis. Vestnik Otorinolaringol. 2017, 82, 54–57. [Google Scholar] [CrossRef]
- Cruz-Ramirez, O.U. Antitumor Activity against Human Colorectal Adenocarcinoma of Silver Nanoparticles: Influence of [Ag]/[PVP] Ratio. Pharmaceutics 2021, 13, 1000. [Google Scholar] [CrossRef]
- Kwon, H.B.; Lee, J.H.; Lee, S.H.; Lee, A.Y.; Choi, J.S.; Ahn, Y.S. A Case of Argyria Following Colloidal Silver Ingestion. Ann. Dermatol. 2009, 21, 308–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgiadou, N.; Singh, S.; Wagner, B.; Goggin, P.; Katsarma, E.; Singh, M. Occupational Localized Cutaneous Argyria With Pseudo-Ochronosis in a Jeweler. Am. J. Dermatopathol. 2021, 43, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Suh, H.S.; Cha, H.J.; Kim, S.H.; Jeong, K.S.; Kim, D.H. A case of generalized argyria after ingestion of colloidal silver solution. Am. J. Ind. Med. 2008, 52, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Korgavkar, K.; DiMarco, C.; Robinson-Bostom, L. Localized argyria with pseudo-ochronosis. J. Cutan. Pathol. 2020, 47, 671–674. [Google Scholar] [CrossRef] [PubMed]
- Kino, F.U. Argyria universalis. Frankf. Z. Path. 1909, 3, 398–412. [Google Scholar]
- Mota, L.; Dinis-Oliveira, R.J. Clinical and Forensic Aspects of the Different Subtypes of Argyria. J. Clin. Med. 2021, 10, 2086. [Google Scholar] [CrossRef] [PubMed]
- Lopatina, I.A.; Vinogradov, D.L. Argyros. Literature review and case description. Russ. Med. J. 2009. 17, 85–89.
- Kim, J.J.; Konkel, K.; McCulley, L.; Diak, I.-L. Cases of Argyria Associated With Colloidal Silver Use. Ann. Pharmacother. 2019, 53, 867–870. [Google Scholar] [CrossRef]
- Molina-Hernandez, A.I.; Diaz-Gonzalez, J.M.; Saeb-Lima, M.; Dominguez-Cherit, J. Argyria after silver nitrate intake: Case report and brief review of literature. Indian J. Dermatol. 2015, 60, 520. [Google Scholar] [CrossRef]
- Raimondo, L.; Garzaro, M.; Molinaro, L.; Bartoli, C.; Provenzano, E.; Pecorari, G. Iatrogenic Rhinopharyngeal Isolated Argyria Induced by Silver-Containing Nasal Drug. J. Craniofacial Surg. 2014, 25, e149–e151. [Google Scholar] [CrossRef]
- Seitz, I.P.; Kowarik, M.C.; Sartor-Pfeiffer, J.; Ziemann, U.; Wilhelm, H.; Bartz-Schmidt, K.U. Occurrence of primary progressive multiple sclerosis in a patient with argyria: Causality or coincidence? Mult. Scler. Relat. Disord. 2020, 46, 102465. [Google Scholar] [CrossRef]
- Drake, P.L.; Hazelwood, K.J. Exposure-Related Health Effects of Silver and Silver Compounds: A Review. Ann. Occup. Hyg. 2005, 49, 575–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadrup, N.; Sharma, A.K.; Loeschner, K. Toxicity of silver ions, metallic silver, and silver nanoparticle materials after in vivo dermal and mucosal surface exposure: A review. Regul. Toxicol. Pharmacol. 2018, 98, 257–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeinalov, O.; Kombarova, S.P.; Bagrov, D.V.; Petrosyan, A.M.; Tolibova, G.H.; Feofanov, A.V.; Shaitan, K.V. About the Influence of Silver Nanoparticles on Living Organisms Physiology. Rev. Clin. Pharmacol. Drug Ther. 2016, 14, 42–51. [Google Scholar] [CrossRef]
- Krivosheev, A.B.; Kondratova, M.A.; Khvan, L.A.; Kuzminykh, N.V. Liver cirrhosis and generalized argyria (review of literature and analysis of own observation). Med. Alph. 2017, 4, 28–32. [Google Scholar]
- Krivosheev, A.B.; Khwang, L.A.; Bobokhidze, D.N.; Krivosheeva, I.A.; Morozov, D.V.; Artyushin, V.A. Generalized argyria. Russ. J. Ski. Sex. Transm. Dis. 2018, 21, 101–105. Available online: https://rjsvd.com/1560-9588/article/view/37345#! (accessed on 7 April 2022). [CrossRef]
- Almurayshid, A.; Park, S.; Oh, S.H. Effective laser treatment options for argyria: Review of literatures. J. Cosmet. Dermatol. 2020, 19, 1877–1882. [Google Scholar] [CrossRef]
- Arunkajohnsak, S.; Thanomkitti, K.; Kasemsarn, P.; Pattanaprichakul, P.; Jiamton, S.; Eimpunth, S. Successful treatment of acupuncture-induced argyria using Q-switched 1064-nm Nd:YAG laser. JAAD Case Rep. 2020, 6, 984–987. [Google Scholar] [CrossRef]
- Gill, P.; Richards, K.; Cho, W.C.; Nagarajan, P.; Aung, P.P.; Ivan, D.; Curry, J.L.; Prieto, V.G.; Torres-Cabala, C.A. Localized cutaneous argyria: Review of a rare clinical mimicker of melanocytic lesions. Ann. Diagn. Pathol. 2021, 54, 151776. [Google Scholar] [CrossRef]
- Ferdous, Z.; Nemmar, A. Health Impact of Silver Nanoparticles: A Review of the Biodistribution and Toxicity Following Various Routes of Exposure. Int. J. Mol. Sci. 2020, 21, 2375. [Google Scholar] [CrossRef] [Green Version]
- Antsiferova, A.A.; Kopaeva, M.Y.; Kochkin, V.N.; Kashkarov, P.K. Kinetics of Silver Accumulation in Tissues of Laboratory Mice after Long-Term Oral Administration of Silver Nanoparticles. Nanomaterials 2021, 11, 3204. [Google Scholar] [CrossRef] [PubMed]
- Rudi, L.; Zinicovscaia, I.; Cepoi, L.; Chiriac, T.; Peshkova, A.; Cepoi, A.; Grozdov, D. Accumulation and Effect of Silver Nanoparticles Functionalized with Spirulina platensis on Rats. Nanomaterials 2021, 11, 2992. [Google Scholar] [CrossRef] [PubMed]
- Carnovale, C.; Guarnieri, D.; Di Cristo, L.; De Angelis, I.; Veronesi, G.; Scarpellini, A.; Malvindi, M.; Barone, F.; Pompa, P.; Sabella, S. Biotransformation of Silver Nanoparticles into Oro-Gastrointestinal Tract by Integrated In Vitro Testing Assay: Generation of Exposure-Dependent Physical Descriptors for Nanomaterial Grouping. Nanomaterials 2021, 11, 1587. [Google Scholar] [CrossRef] [PubMed]
- Cueva, C. Gastrointestinal digestion of food-use silver nanoparticles in the dynamic SIMulator of the GastroIntestinal tract (simgi®). Impact on human gut microbiota. Food Chem. Toxicol. 2019, 132, 110657. [Google Scholar] [CrossRef]
- Mashkovsky, M.D. Medicines; New Wave Publishing House LLC: Moscow, Russia, 2005; Volume 2, p. 1200. [Google Scholar]
- Daupor, H.; Chenea, A. Degradation of blue and red inks by Ag/AgCl photocatalyst under UV light irradiation. In AIP Conference Proceedings; AIP Publishing LLC: New York, NY, USA, 2017. [Google Scholar] [CrossRef] [Green Version]
- Karpov, S.V. Optical effects in metal nanocolloids. Photonics 2012, 32, 40–51. [Google Scholar]
- Vilamová, Z.; Konvičková, Z.; Mikeš, P.; Holišová, V.; Mančík, P.; Dobročka, E.; Kratošová, G.; Seidlerová, J. Ag-AgCl Nanoparticles Fixation on Electrospun PVA Fibres: Technological Concept and Progress. Sci. Rep. 2019, 9, 15520. [Google Scholar] [CrossRef] [Green Version]
- Petrov, Y.I. Small Particle Physics; Nauka: Moscow, Russia, 1982; p. 359. [Google Scholar]
- Cinotti, E.; Labeille, B.; Douchet, C.; Cambazard, F.; Perrot, J.-L. Dermoscopy, reflectance confocal microscopy, and high-definition optical coherence tomography in the diagnosis of generalized argyria. J. Am. Acad. Dermatol. 2017, 76, S66–S68. [Google Scholar] [CrossRef]
- Gülseren, D.; Arzberger, E.; Cerroni, L.; Richtig, E.; Hofmann-Wellenhof, R. Reflectance confocal microscopy and dermatopathologic findings of cutaneous argyria after colloidal silver ingestion. J. Eur. Acad. Dermatol. Venereol. 2017, 31, e178–e179. [Google Scholar] [CrossRef]
- Shelley, W.B.; Shelley, E.D.; Burmeister, V. Argyria: The intradermal “photograph,” a manifestation of passive photosensitivity. J. Am. Acad. Dermatol. 1987, 16, 211–217. [Google Scholar] [CrossRef]
- Photokinotechnics Encyclopedia. In Soviet Encyclopedia; Iophis, E.A. (Ed.) Macmillan: Moskow, Russia, 1981; p. 447. [Google Scholar]
- Hedgecoe, J. John Hedgecoe’s New Book of Photography; Dorling Kindersley: London, UK, 1994; 264p. [Google Scholar]
- Redko, A.V. Chemistry of photographic processes. In New Handbook of Chemist and Technologist; MMVI: St. Petersburg, Russia, 2007; pp. 836–918. [Google Scholar]
- Nagami, G.T. Hyperchloremia—Why and how. Nefrología 2016, 36, 347–353. [Google Scholar] [CrossRef] [Green Version]
- Turell, L.; Radi, R.; Alvarez, B. The thiol pool in human plasma: The central contribution of albumin to redox processes. Free Radic. Biol. Med. 2013, 65, 244–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Wang, Z.; Liu, F.D.; Kane, A.B.; Hurt, R.H. Chemical Transformations of Nanosilver in Biological Environments. ACS Nano 2012, 6, 9887–9899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolsky, B.P. Handbook of Chemist; Khimiya: Leningrad, Russia, 1971; Volume 2, p. 1168. [Google Scholar]
- Simon, M.; Buchanan, J.A. Argyria, an Unexpected Case of Skin Discoloration From Colloidal Silver Salt Ingestion. J. Emerg. Med. 2020, 59, e39–e41. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M. Generalized Argyria after Habitual Use of AgNO3. J. Dermatol. 1994, 21, 50–53. [Google Scholar] [CrossRef]
- Fan, Y.; Bao, Y.; Song, Z.; Sun, Z.; Wang, D.; Han, D.; Niu, L. Controllable synthesis of coloured Ag0/AgCl with spectral analysis for photocatalysis. RSC Adv. 2018, 8, 24812–24818. [Google Scholar] [CrossRef] [Green Version]
- Encyclopedia, G.M. Sweat, Sweating, Sweat glands. In Great Medical Encyclopedia; Petrovsky, B.V., Ed.; Soviet Encyclopedia: Moscow, Russia, 1983; p. 560. [Google Scholar]
- Goldman, J.G. What Our Perspiration Reveals about Us. 2015. Available online: https://www.bbc.com/russian/science/2015/08/150821_vert_fut_what_our_perspiration_reveals (accessed on 1 December 2021).
- Buzulukov, Y.u.P.; Gmoshinskii, I.V.; Raspopov, R.V.; Dyomin, V.F.; Solov’yov, V.Y.; Kuzmin, P.G.; Shafeev, G.A.; Khotimchenko, S.A. Studies of Some Inorganic Nanoparticles after Intragastric Administration to Rats Using Radioactive Tracers. Med. Radiol. Radiat. Saf. 2012, 57, 5–12. [Google Scholar]
- Hadrup, N.; Sharma, A.K.; Loeschner, K.; Jacobsen, N.R. Pulmonary toxicity of silver vapours, nanoparticles and fine dusts: A review. Regul. Toxicol. Pharmacol. 2020, 115, 104690. [Google Scholar] [CrossRef]
- Krutyakov, Y.A.; Kudrinskiy, A.A.; Olenin, A.Y.; Lisichkin, G.V. Synthesis and properties of silver nanoparticles: Advances and prospects. Russ. Chem. Rev. 2008, 77, 233. [Google Scholar] [CrossRef]
- Boix-Vilanova, J.; Del Pozo, L.J.; Martinez, M.; Ramos, D.; Izquierdo, N. Dermoscopy of localised argyria: Apropos of five cases. Australas. J. Dermatol. 2019, 61, e122–e123. [Google Scholar] [CrossRef]
- Isak, V.; Beerli, T.; Cozzio, A.; Flatz, L. A Rare Case of Localized Argyria on the Face. Case Rep. Dermatol. 2019, 11, 23–27. [Google Scholar] [CrossRef]
- McCague, A.; Joe, V.C. A Case of Argyria and Acute Leukopenia Associated with the Use of an Antimicrobial Soft Silicone Foam Dressing. J. Burn Care Res. 2016, 37, e493–e496. [Google Scholar] [CrossRef] [PubMed]
- Rojanapanthu, P.; Sampattavanich, N.; Aunhachoke, K. Argyria from Overindulgence of a Breath Freshener. Thai J. Dermatol. 2018, 34, 217–224. [Google Scholar]
- Fung, M.C.; Bowen, D.L. Silver products for medical indications: Risk-benefit assessment. J. Toxicol. Clin. Toxicol. 1996, 34, 119–126. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Silver Concentration, mg/mL | Storage, Days | |
|---|---|---|---|
| In the Dark | In the Sunlight | ||
| 0 | 1 | 3 | 0 |
| 1 | 1 | 2 | 1 |
| 2 | 1 | 1 | 2 |
| 3 | 1 | 0 | 3 |
| 4 | 0.2 | 0 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burmistrov, V.; Burmistrov, A.; Odegova, G.; Pestryakov, A.; Luna-Vázquez-Gómez, R.; Bogdanchikova, N. Hypothetical Mechanism of Skin Argyria. Coatings 2022, 12, 532. https://doi.org/10.3390/coatings12040532
Burmistrov V, Burmistrov A, Odegova G, Pestryakov A, Luna-Vázquez-Gómez R, Bogdanchikova N. Hypothetical Mechanism of Skin Argyria. Coatings. 2022; 12(4):532. https://doi.org/10.3390/coatings12040532
Chicago/Turabian StyleBurmistrov, Vasily, Alexander Burmistrov, Galina Odegova, Alexey Pestryakov, Roberto Luna-Vázquez-Gómez, and Nina Bogdanchikova. 2022. "Hypothetical Mechanism of Skin Argyria" Coatings 12, no. 4: 532. https://doi.org/10.3390/coatings12040532
APA StyleBurmistrov, V., Burmistrov, A., Odegova, G., Pestryakov, A., Luna-Vázquez-Gómez, R., & Bogdanchikova, N. (2022). Hypothetical Mechanism of Skin Argyria. Coatings, 12(4), 532. https://doi.org/10.3390/coatings12040532