
The Assessment of the Usefulness of Platelet-Rich Fibrin in the Healing Process Bone Resorption


Abstract
:1. Introduction
- Can the insertion of the PRF to the post-extraction socket enhance soft tissue and bone healing?
- How does the insertion of the PRF to the post-extraction socket affect the CBCT measured grayscale values?
- How does the insertion of the PRF to the post-extraction socket affect the post-extraction bone loss?
2. Materials and Methods
- The presence of two maxillary or mandibular homonymous teeth qualified for extraction (teeth with pulp gangrene with or without periapical lesions with a diameter of no more than 1 cm, which cannot be treated conservatively due to the fact of considerable damage to the crowns of the teeth; teeth after the failures and complications of endodontic treatment with considerable damage to the tooth crown);
- The bony walls of the alveolus are intact during extraction and the adjacent teeth are preserved;
- The extraction of two teeth in the same patient comparable concerning surgical procedure in duration;
- The lack of local and general contraindications for tooth extraction;
- Patients without systemic diseases.
2.1. Surgical Procedure
2.2. Postoperative Care
- The appearance of the wound: infected—0 points, clean—1 point;
- Oedema: present—0 points, not present—1 point;
- Discharge from the wound: present—0 points, not present—1 point;
- The tightness of wound closure: wound dehiscence—0 points, tight wound closure—1 point;
- Pain reported by the patient on the VAS scale: 5 or more—0 points, less than 5—1 point.
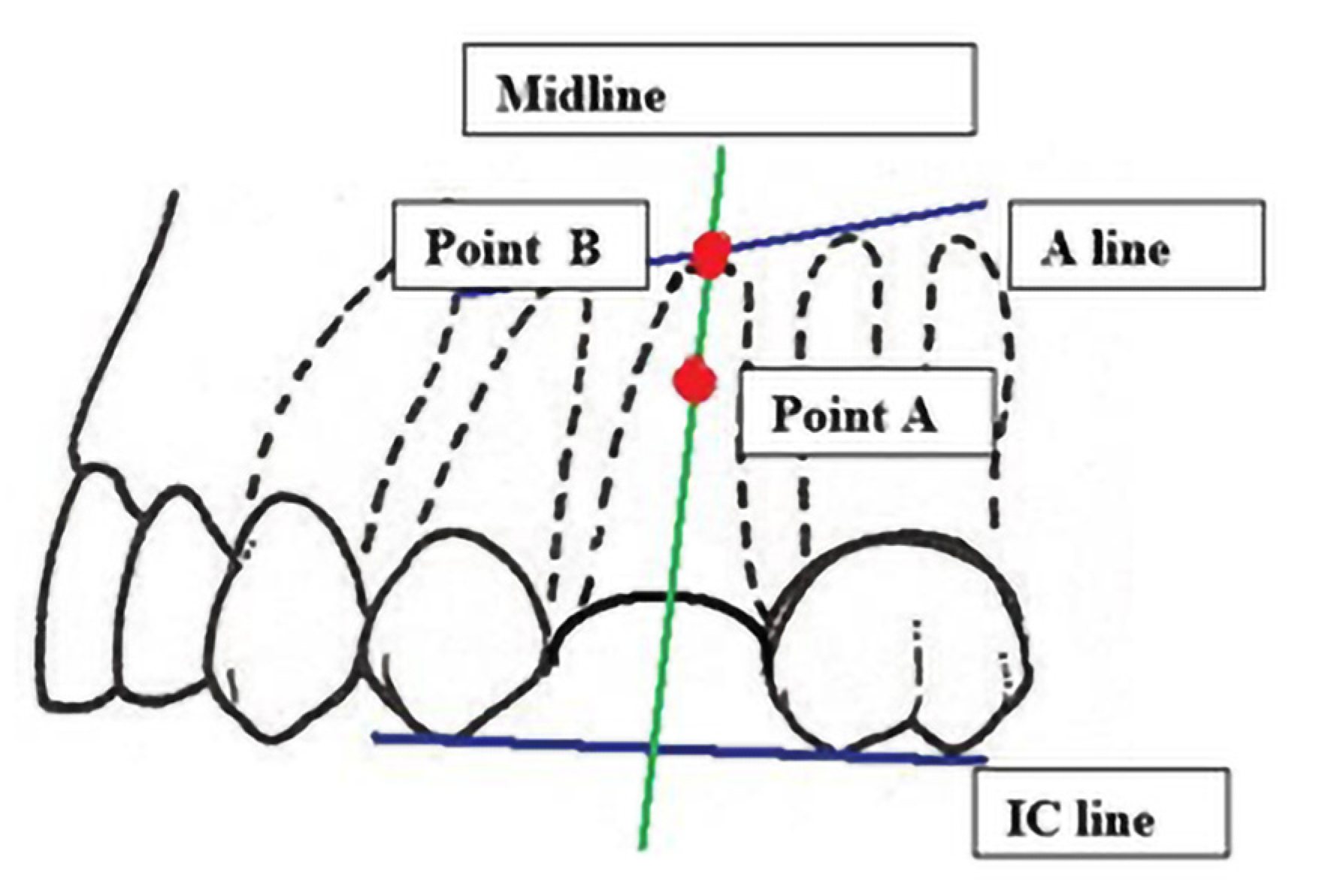
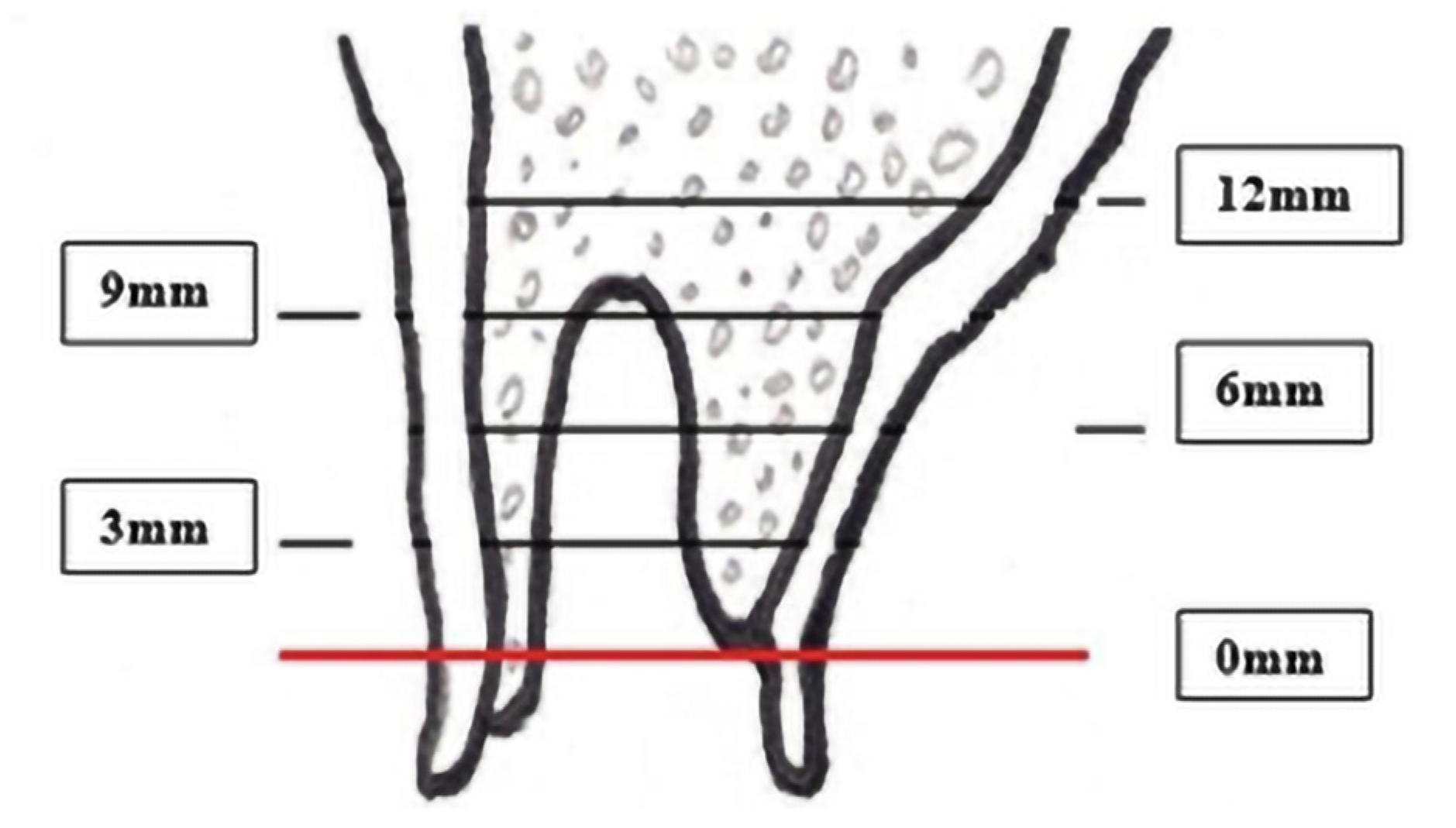
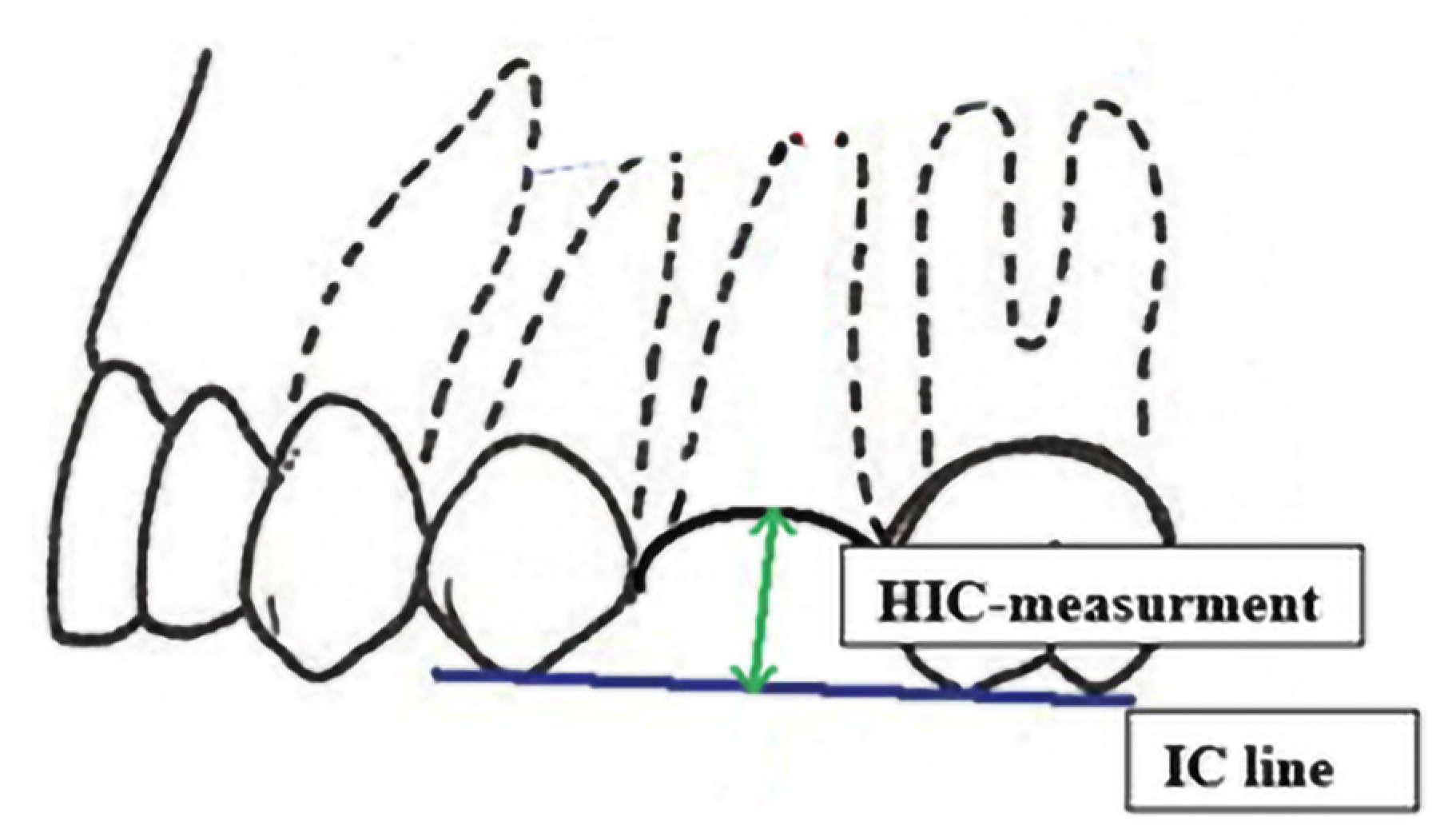
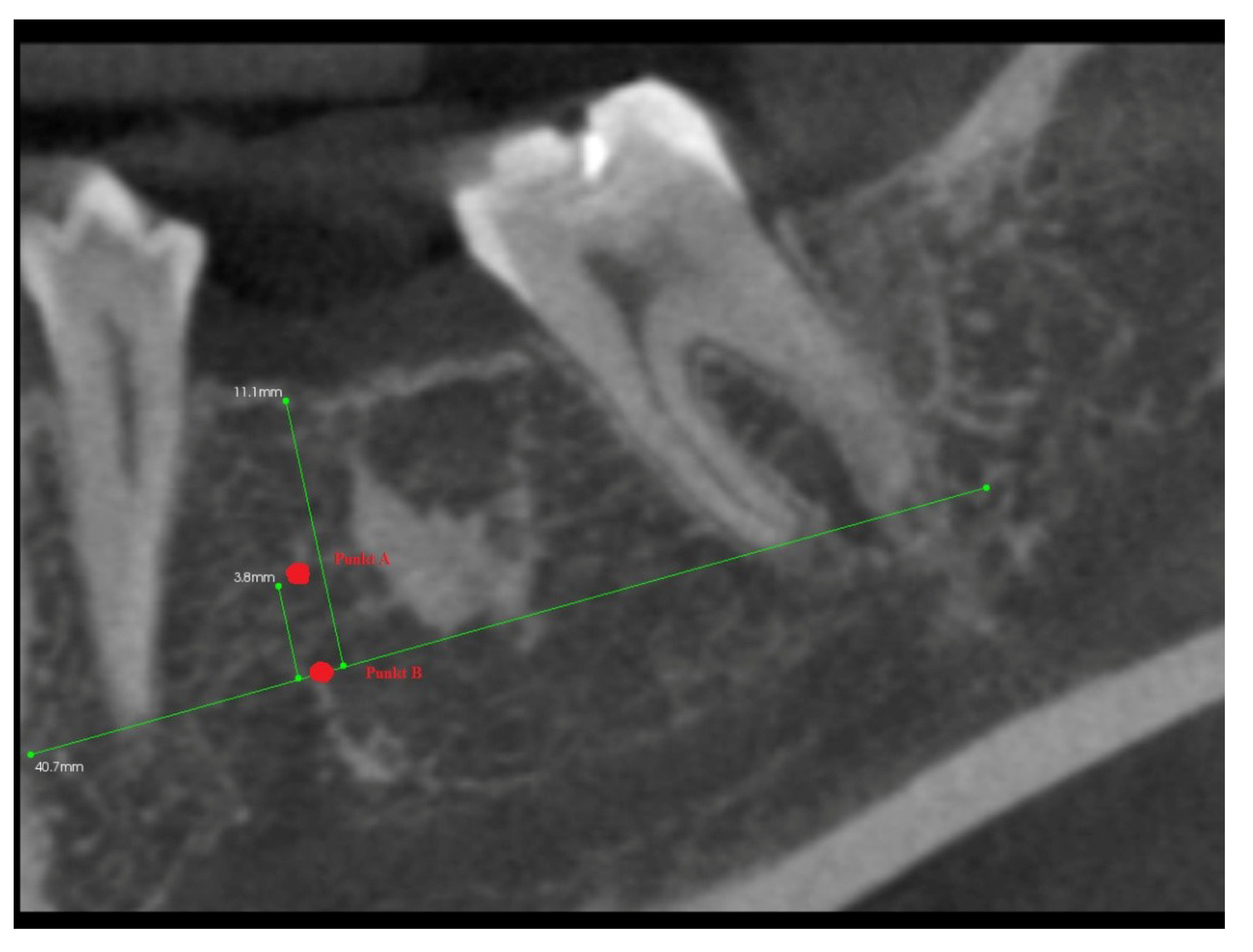
- The A line drawn through the apexes of the teeth adjacent to the post-extraction socket;
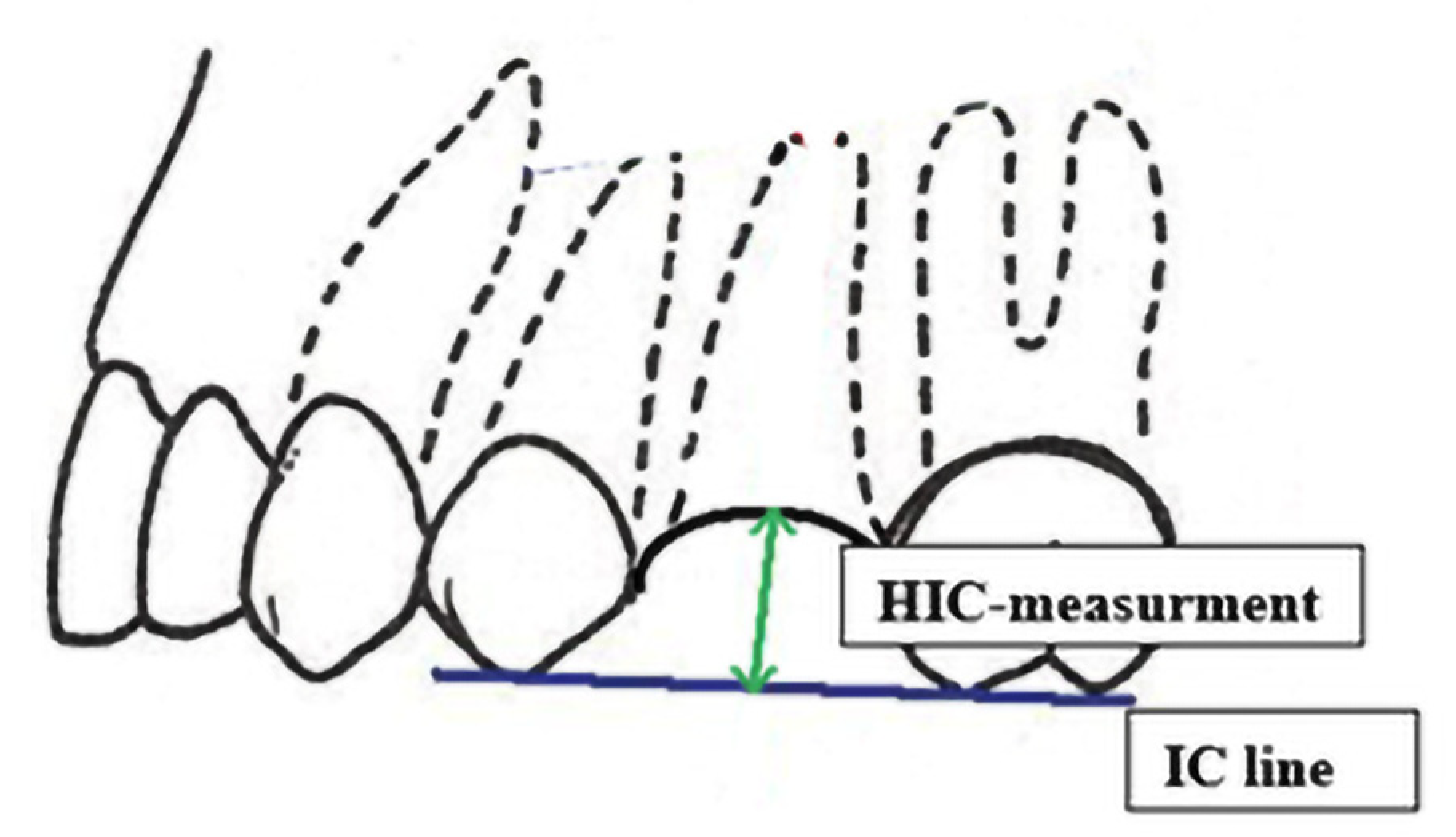
- The IC line drawn through the top of the buccal cusps of the teeth adjacent to the pos-extraction socket;
- The midline of the post-extraction socket (alveolus).
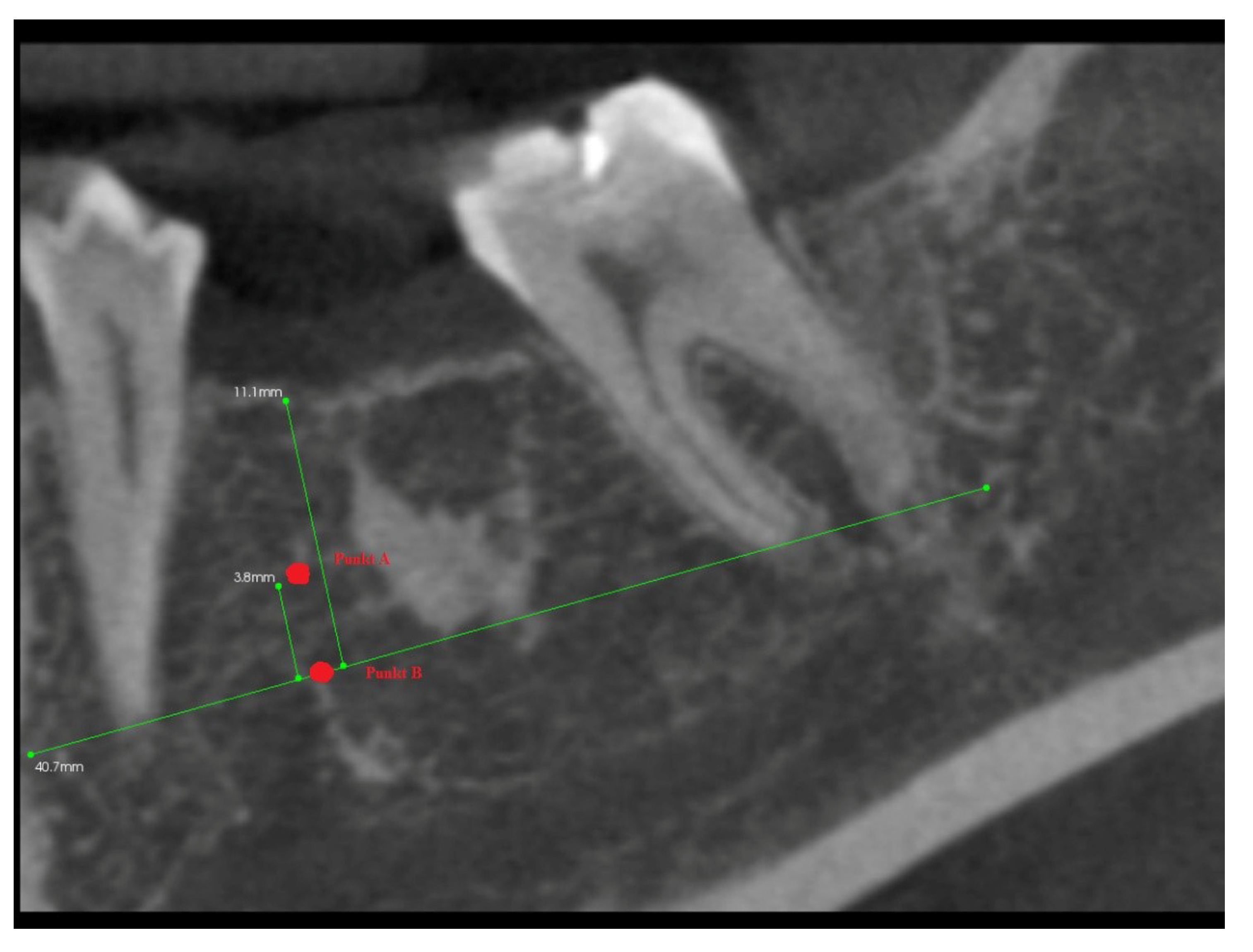
- Point (A)
- 1/3 of the distance between the A line and the IC line following the midline;
- Point (B)
- At the intersection of the midline and the A line.
3. Results
3.1. The Assessment of Soft Tissues Healing (ARSTH) for the Alveolar Area (with and without PRF Insertion) Assessed after 10 Days from Tooth Extraction
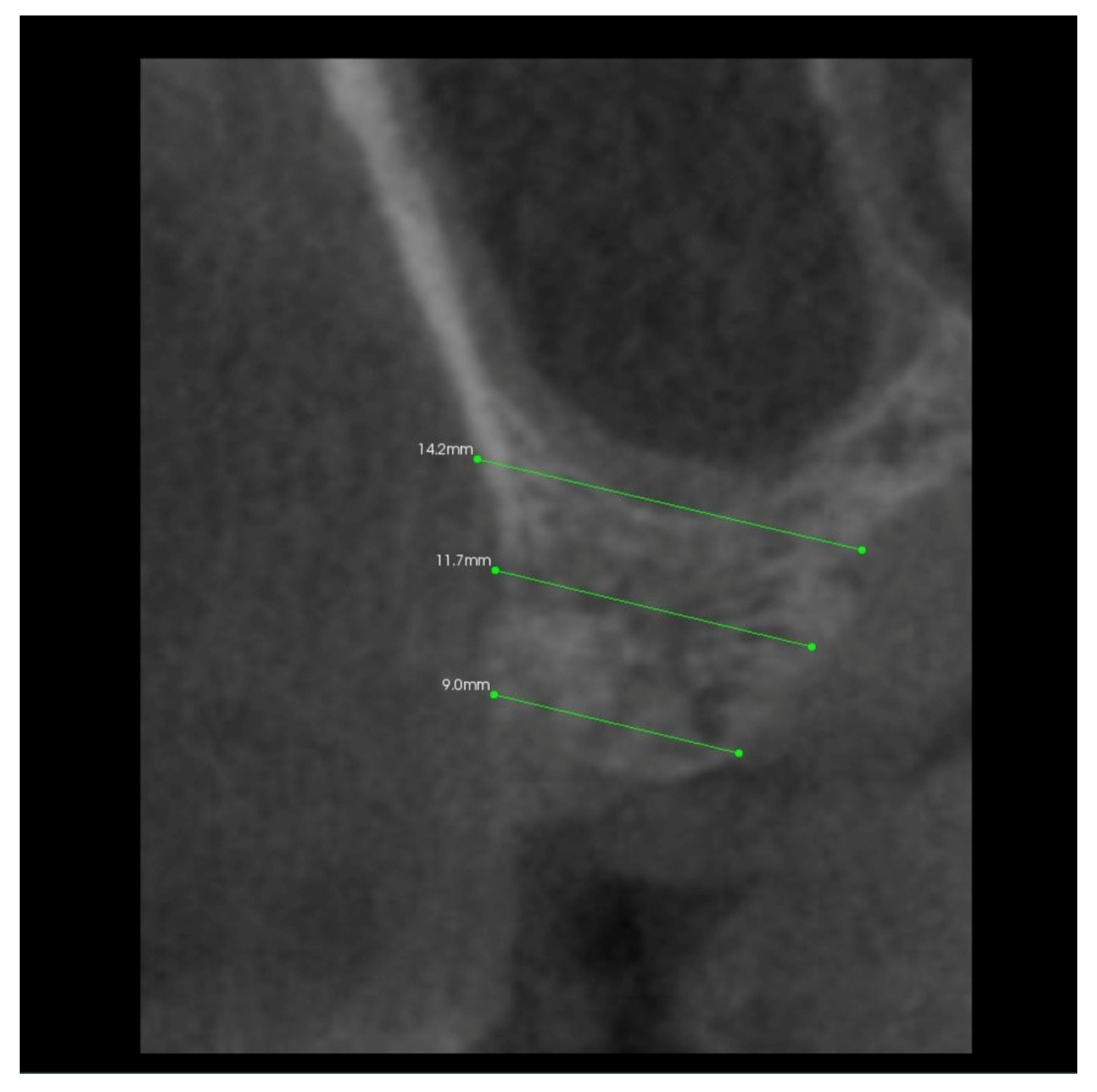
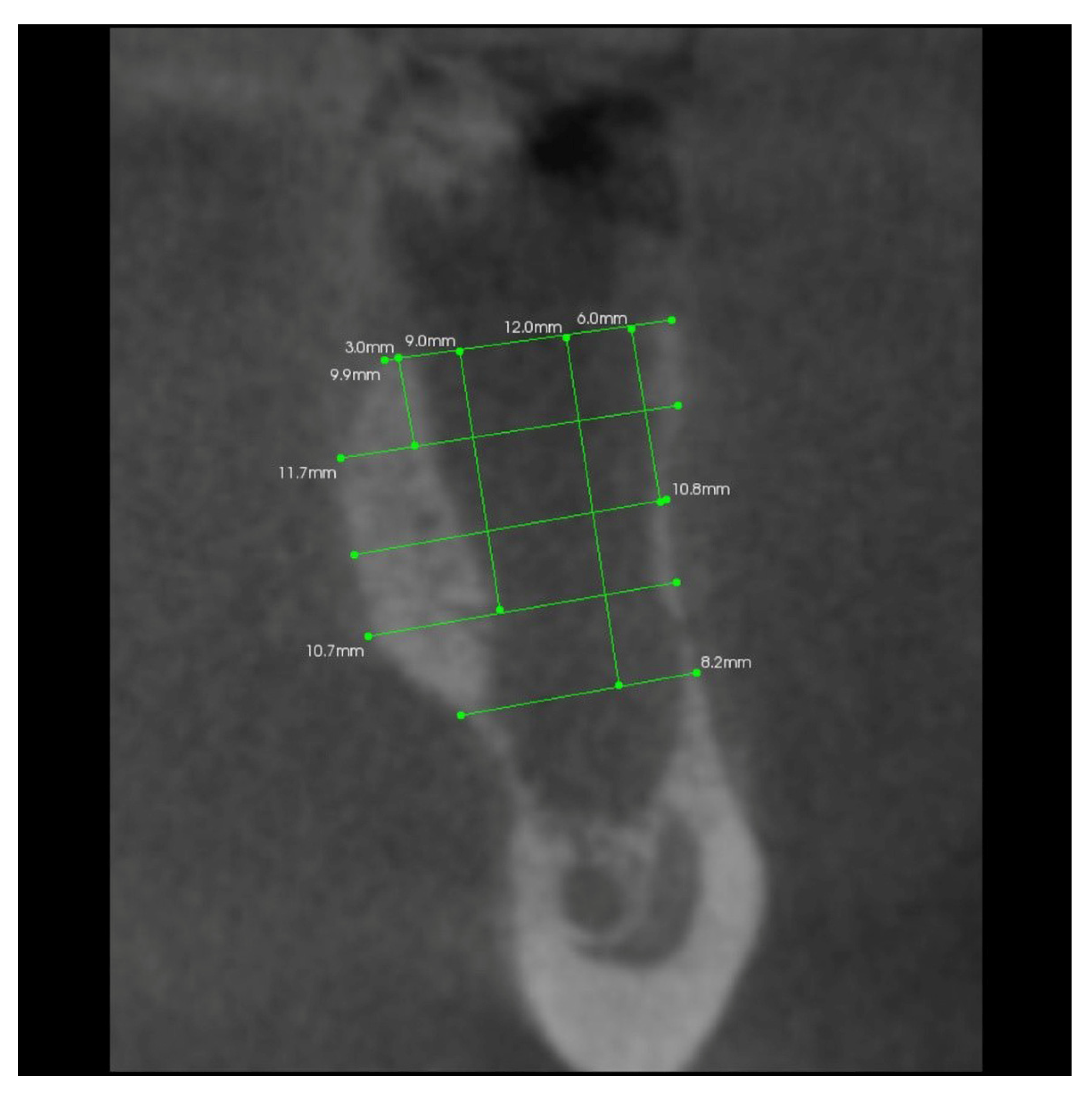
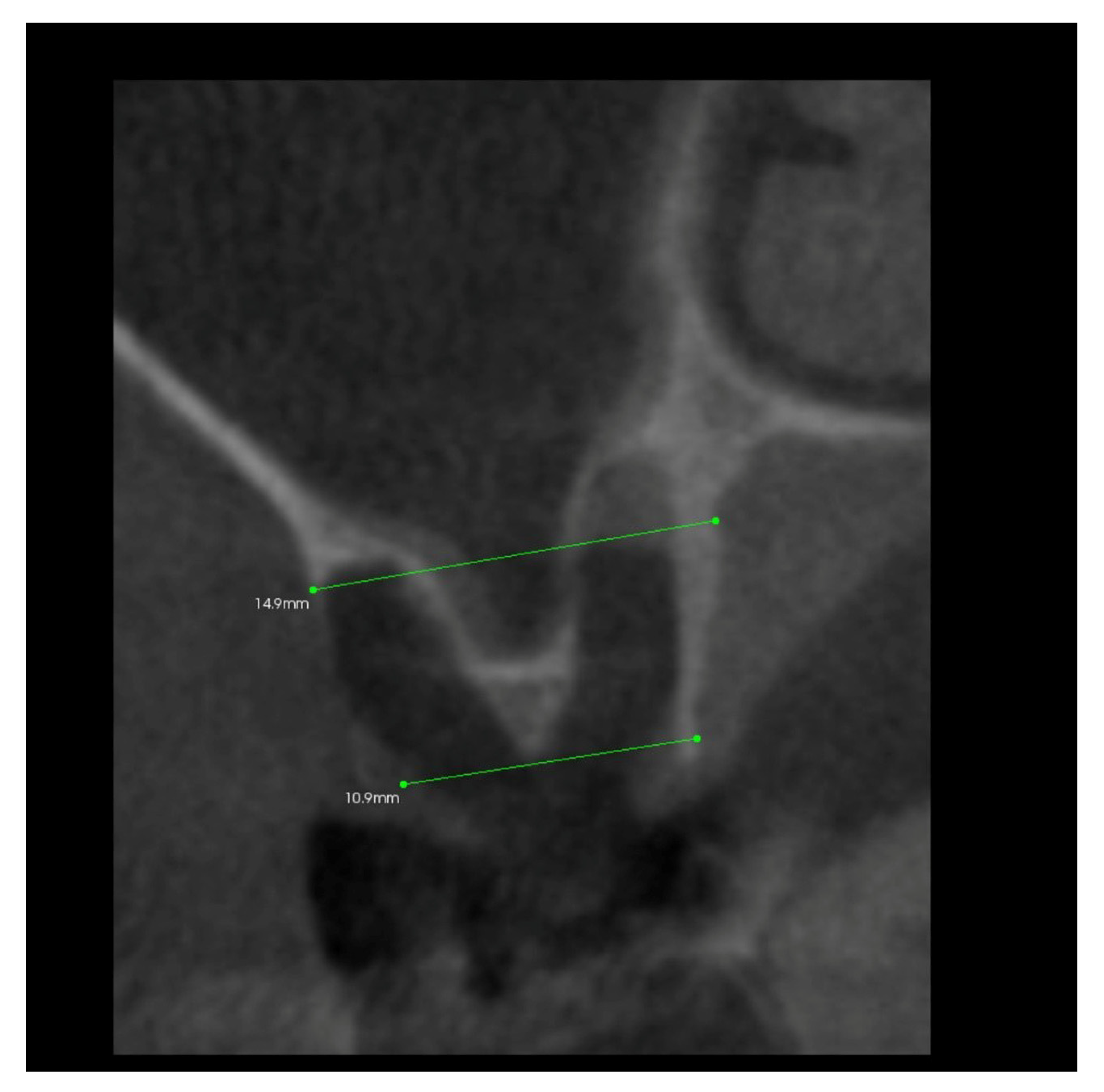
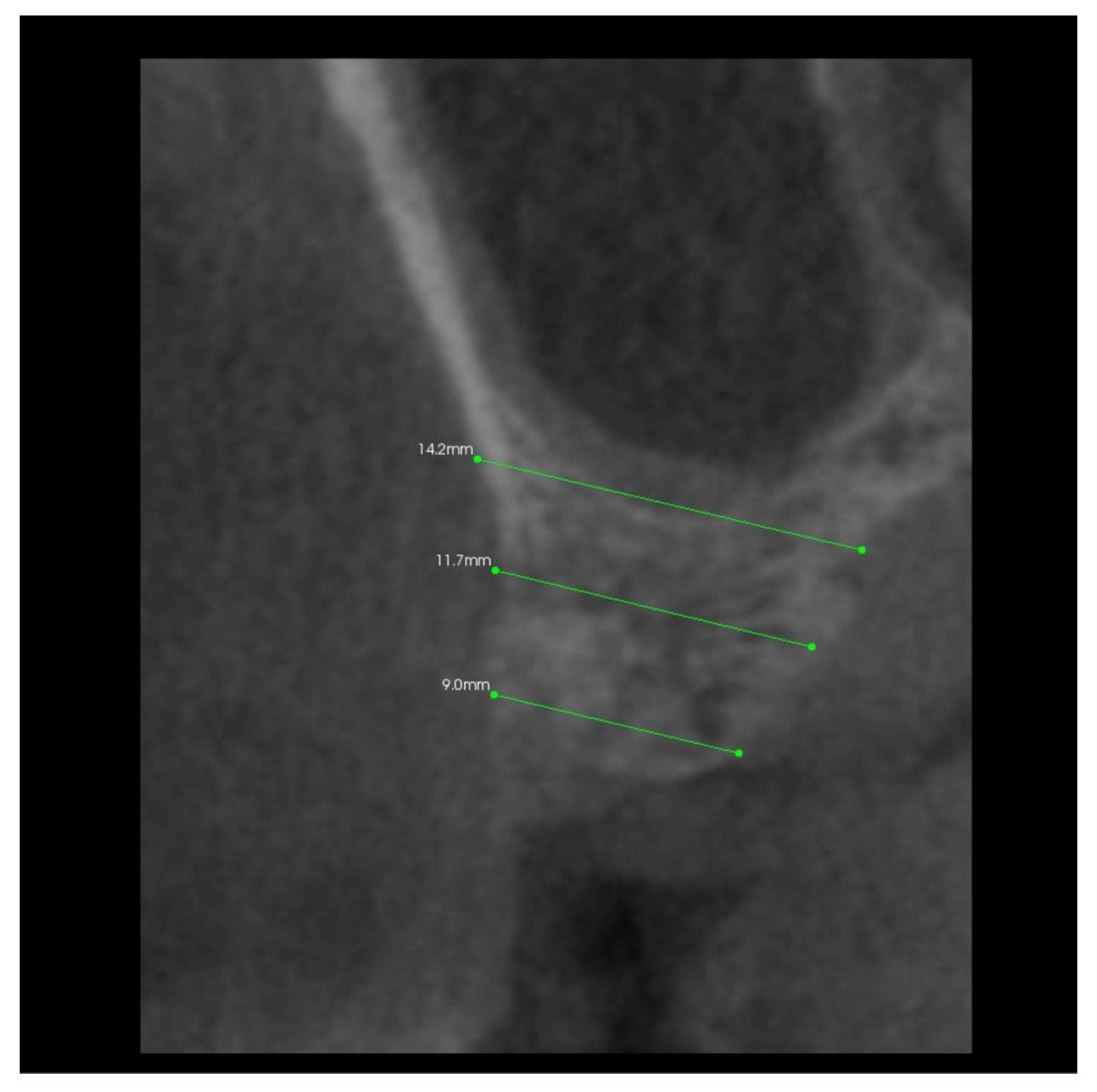
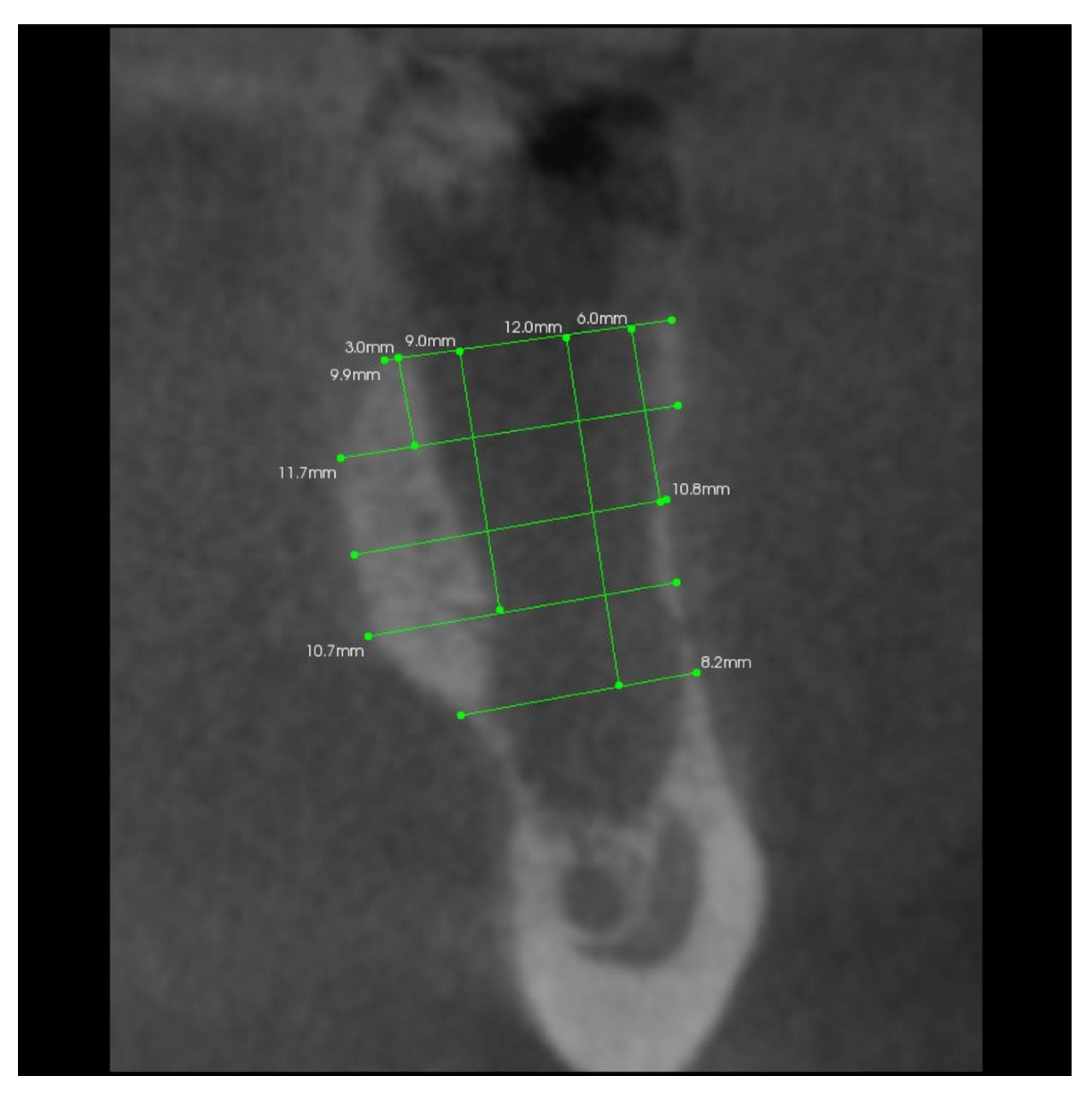
3.2. The Results of Mean Values of the Alveolar Process Width and Height Measurements Performed after Tooth Extraction within the Space of 6 Months for Two Different Alveoli in the Same Patient
3.3. The Results of Mean Values of Grayscale Value Measurements for Two Alveoli (with/without PRF Insertion) after 6 Months
3.4. The Results of Mean Measurements of Height and Width of the Alveolar Processes of Two Extraction Sites (with and without PRF) in the Same Patient after 6 Months from Tooth Extraction Based on the Analysis of Volumetric Tomography
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Araújo, M.G.; Lindhe, J. Dimensional Ridge Alterations Following Tooth Extraction. An Experimental Study in the Dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Nevins, M.; Mellonig, J. Implant Therapy: Clinical Approaches and Evidence of Success; Quintessence Publishing Co. Inc.: Chicago, IL, USA, 1998; Volume 2, pp. 23–28. [Google Scholar]
- Dominiak, M.; Łysiak, K. Odbudowa struktury kostnej w ubytkach poekstrakcyjnych-aspekty procesów fizjologicznych i regeneracyjnych po zastosowaniu biomateriałów-przegląd piśmiennictwa. Porad. Stomatol. 2004, 4, 5–12. [Google Scholar]
- Ashman, A. Ridge Preservation: Important Buzzwords in Dentistry. Gen. Dent. 2000, 48, 304–312. [Google Scholar] [PubMed]
- Lekovic, V.; Camargo, P.M.; Klokkevold, P.R.; Weinlaender, M.; Kenney, E.B.; Dimitrijevic, B.; Nedic, M. Preservation of Alveolar Bone in Extraction Sockets Using Bioabsorbable Membranes. J. Periodontol. 1998, 69, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- Darby, I.; Chen, S.T.; Buser, D. Ridge Preservation Techniques for Implant Therapy. Int. J. Oral Maxillofac. Implant. 2009, 24 (Suppl), 260–271. [Google Scholar]
- Araújo, M.G.; Lindhe, J. Ridge Alterations Following Tooth Extraction with and without Flap Elevation: An Experimental Study in the Dog. Clin. Oral Implants Res. 2009, 20, 545–549. [Google Scholar] [CrossRef]
- Simon, B.I.; Von Hagen, S.; Deasy, M.J.; Faldu, M.; Resnansky, D. Changes in Alveolar Bone Height and Width Following Ridge Augmentation Using Bone Graft and Membranes. J. Periodontol. 2000, 71, 1774–1791. [Google Scholar] [CrossRef]
- Zubillaga, G.; Von Hagen, S.; Simon, B.I.; Deasy, M.J. Changes in Alveolar Bone Height and Width Following Post-Extraction Ridge Augmentation Using a Fixed Bioabsorbable Membrane and Demineralized Freeze-Dried Bone Osteoinductive Graft. J. Periodontol. 2003, 74, 965–975. [Google Scholar] [CrossRef]
- Marciniak, J. Biomateriały; Wydawnictwo Politechniki Śląskiej: Gliwice, Poland, 2002. [Google Scholar]
- Choukroun, J.; Adda, F.; Schoeffler, C.; Vervelle, A. Une Opportunite’ En Paro-Implantologie: Le PRF. Implantodontie 2001, 42, e62. [Google Scholar]
- Diss, A.; Dohan, D.M.; Mouhyi, J.; Mahler, P. Osteotome Sinus Floor Elevation Using Choukroun’s Platelet-Rich Fibrin as Grafting Material: A 1-Year Prospective Pilot Study with Microthreaded Implants. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 105, 572–579. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Gogly, B. Platelet-Rich Fibrin (PRF): A Second-Generation Platelet Concentrate. Part II: Platelet-Related Biologic Features. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e45–e50. [Google Scholar] [CrossRef] [PubMed]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Gogly, B. Platelet-Rich Fibrin (PRF): A Second-Generation Platelet Concentrate. Part III: Leucocyte Activation: A New Feature for Platelet Concentrates? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e51–e55. [Google Scholar] [CrossRef] [PubMed]
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.-O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Dohan, D.M. Platelet-Rich Fibrin (PRF): A Second-Generation Platelet Concentrate. Part IV: Clinical Effects on Tissue Healing. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e56–e60. [Google Scholar] [CrossRef]
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.-O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Dohan, D.M. Platelet-Rich Fibrin (PRF): A Second-Generation Platelet Concentrate. Part V: Histologic Evaluations of PRF Effects on Bone Allograft Maturation in Sinus Lift. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 299–303. [Google Scholar] [CrossRef]
- Carroll, R.; Amoczky, S.; Graham, S.; O’Connell, S. Characterization of Autologous Growth Factors in Cascade Platelet Rich Fibrin Matrix (PRFM); Musculoskeletal Transplant Foundation: Edison, NJ, USA, 2005. [Google Scholar]
- Dohan Ehrenfest, D.M.; Bielecki, T.; Jimbo, R.; Barbé, G.; Del Corso, M.; Inchingolo, F.; Sammartino, G. Do the Fibrin Architecture and Leukocyte Content Influence the Growth Factor Release of Platelet Concentrates? An Evidence-Based Answer Comparing a Pure Platelet-Rich Plasma (P-PRP) Gel and a Leukocyte- and Platelet-Rich Fibrin (L-PRF). Curr. Pharm. Biotechnol. 2012, 13, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Dohan, D.M.; Del Corso, M.; Charrier, J.-B. Cytotoxicity Analyses of Choukroun’s Platelet-Rich Fibrin (PRF) on a Wide Range of Human Cells: The Answer to a Commercial Controversy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 587–593. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Gogly, B. Platelet-Rich Fibrin (PRF): A Second-Generation Platelet Concentrate. Part I: Technological Concepts and Evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e37–e44. [Google Scholar] [CrossRef]
- Bilgen, F.; Ural, A.; Bekerecioglu, M. Platelet-Rich Fibrin: An Effective Chronic Wound Healing Accelerator. J. Tissue Viability 2021, 30, 616–620. [Google Scholar] [CrossRef]
- Thorat, M.; Pradeep, A.R.; Pallavi, B. Clinical Effect of Autologous Platelet-Rich Fibrin in the Treatment of Intra-Bony Defects: A Controlled Clinical Trial. J. Clin. Periodontol. 2011, 38, 925–932. [Google Scholar] [CrossRef]
- Sharma, A.; Pradeep, A.R. Treatment of 3-Wall Intrabony Defects in Patients with Chronic Periodontitis with Autologous Platelet-Rich Fibrin: A Randomized Controlled Clinical Trial. J. Periodontol. 2011, 82, 1705–1712. [Google Scholar] [CrossRef]
- Heggendorn, F.L.; Heggendorn, C.; Vidal, F.; de Carvalho Silva, G.C.; Gonçalves, L.S.; de Oliveira Freitas Lione, V. Leukocyte-Platelet Rich Fibrin on the Treatment of a Large Paradental Cyst: A Novel Regenerative Approach. Blood Coagul. Fibrinolysis 2021, 32, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Nagaraja, S.; Mathew, S.; Jain, N.; Jethani, B.; Nambiar, S.; Kumari, M.; Nair, S. Study of Antibacterial and Antifungal Efficacy of Platelet-Rich Fibrin and Platelet-Rich Fibrin Matrix. J. Conserv. Dent. 2019, 22, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Petrescu, B.N.; Mirica, I.C.; Miron, R.; Campian, R.S.; Lucaciu, O. Platelet Rich Fibrin as a Gingival Tissue Regeneration Enhancer. J. Dent. Sci. 2021, 16, 536–539. [Google Scholar] [CrossRef] [PubMed]
- Kempraj, J.; Sundaram, S.S.; Doss, G.P.T.; Nakeeran, K.P.; Raja, V.B.K.K. Maxillary Sinus Augmentation Using Xenograft and Choukroun’s Platelet-Rich Fibrin as Grafting Material: A Radiological Study. J. Maxillofac. Oral Surg. 2020, 19, 263–268. [Google Scholar] [CrossRef]
- Sunitha Raja, V.; Munirathnam Naidu, E. Platelet-Rich Fibrin: Evolution of a Second-Generation Platelet Concentrate. Indian J. Dent. Res. 2008, 19, 42–46. [Google Scholar] [CrossRef]
- Barone, A.; Aldini, N.N.; Fini, M.; Giardino, R.; Calvo Guirado, J.L.; Covani, U. Xenograft versus Extraction Alone for Ridge Preservation after Tooth Removal: A Clinical and Histomorphometric Study. J. Periodontol. 2008, 79, 1370–1377. [Google Scholar] [CrossRef]
- Iasella, J.M.; Greenwell, H.; Miller, R.L.; Hill, M.; Drisko, C.; Bohra, A.A.; Scheetz, J.P. Ridge Preservation with Freeze-Dried Bone Allograft and a Collagen Membrane Compared to Extraction Alone for Implant Site Development: A Clinical and Histologic Study in Humans. J. Periodontol. 2003, 74, 990–999. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Gherlone, E. Dental Implants Placed in Extraction Sites Grafted with Different Bone Substitutes: Radiographic Evaluation at 24 Months. J. Periodontol. 2009, 80, 1616–1621. [Google Scholar] [CrossRef]
- Nevins, M.; Mellonig, J.T.; Clem, D.S.; Reiser, G.M.; Buser, D.A. Implants in Regenerated Bone: Long-Term Survival. Int. J. Periodontics Restor. Dent. 1998, 18, 34–45. [Google Scholar]
- Sclar, A.G. The Bio-Col Technique. In Soft Tissue and Esthetic Considerations in Implant Therapy; Quintessence Publishing Co. Inc.: Chicago, IL, USA, 2003; pp. 75–112. [Google Scholar]
- Lekovic, V.; Kenney, E.B.; Weinlaender, M.; Han, T.; Klokkevold, P.; Nedic, M.; Orsini, M. A Bone Regenerative Approach to Alveolar Ridge Maintenance Following Tooth Extraction. Report of 10 Cases. J. Periodontol. 1997, 68, 563–570. [Google Scholar] [CrossRef]
- Brownfield, L.A.; Weltman, R.L. Ridge Preservation with or without an Osteoinductive Allograft: A Clinical, Radiographic, Micro-Computed Tomography, and Histologic Study Evaluating Dimensional Changes and New Bone Formation of the Alveolar Ridge. J. Periodontol. 2012, 83, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Trisi, P.; Rebaudi, A.; Calvari, F.; Lazzara, R.J. Sinus Graft with Biogran, Autogenous Bone, and PRP: A Report of Three Cases with Histology and Micro-CT. Int. J. Periodontics Restor. Dent. 2006, 26, 113–125. [Google Scholar]
- Marsell, R.; Einhorn, T.A. The biology of fracture healing. Injury 2011, 42, 551–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dohan Ehrenfest, D.M.; Rasmusson, L.; Albrektsson, T. Classification of Platelet Concentrates: From Pure Platelet-Rich Plasma (P-PRP) to Leucocyte- and Platelet-Rich Fibrin (L-PRF). Trends Biotechnol. 2009, 27, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Diss, A.; Mouhyi, J.; Charrier, J.-B. Three-Dimensional Architecture and Cell Composition of a Choukroun’s Platelet-Rich Fibrin Clot and Membrane. J. Periodontol. 2010, 81, 546–555. [Google Scholar] [CrossRef]
- El-Sharkawy, H.; Kantarci, A.; Deady, J.; Hasturk, H.; Liu, H.; Alshahat, M.; Van Dyke, T.E. Platelet-Rich Plasma: Growth Factors and pro- and Anti-Inflammatory Properties. J. Periodontol. 2007, 78, 661–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werther, K.; Christensen, I.J.; Nielsen, H.J. Determination of Vascular Endothelial Growth Factor (VEGF) in Circulating Blood: Significance of VEGF in Various Leucocytes and Platelets. Scand. J. Clin. Lab. Investig. 2002, 62, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Becker, W.; Dahlin, C.; Becker, B.E.; Lekholm, U.; van Steenberghe, D.; Higuchi, K.; Kultje, C. The Use of E-PTFE Barrier Membranes for Bone Promotion around Titanium Implants Placed into Extraction Sockets: A Prospective Multicenter Study. Int. J. Oral Maxillofac. Implant. 1994, 9, 31–40. [Google Scholar]
- Dohan Ehrenfest, D.M.; Doglioli, P.; de Peppo, G.M.; Del Corso, M.; Charrier, J.-B. Choukroun’s Platelet-Rich Fibrin (PRF) Stimulates in Vitro Proliferation and Differentiation of Human Oral Bone Mesenchymal Stem Cell in a Dose-Dependent Way. Arch. Oral Biol. 2010, 55, 185–194. [Google Scholar] [CrossRef]
- Leitner, G.C.; Gruber, R.; Neumüller, J.; Wagner, A.; Kloimstein, P.; Höcker, P.; Körmöczi, G.F.; Buchta, C. Platelet Content and Growth Factor Release in Platelet-Rich Plasma: A Comparison of Four Different Systems. Vox Sang. 2006, 91, 135–139. [Google Scholar] [CrossRef]
- O’Connell, S.; Carroll, R.; Beavis, A.; Arnoczky, S.P. Flow Cytometric Characterization of Cascade Platelet-Rich Fibrin Matrix (PRFM); The Impact of Exogenous Thrombin on Platelet Concentrates (PC); Musculoskeletal Transplant Foundation: Edison, NJ, USA, 2006; Volume 4, p. 66. [Google Scholar]
- Taylor, T.; Gans, S.; Jones, E.; Firestone, A.; Johnston, W.; Kim, D.-G. Comparison of Micro-CT and Cone Beam CT-Based Assessments for Relative Difference of Grey Level Distribution in a Human Mandible. Dentomaxillofac. Radiol. 2013, 42, 25117764. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-G. Can Dental Cone Beam Computed Tomography Assess Bone Mineral Density? J. Bone Metab. 2014, 21, 117–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eguren, M.; Holguin, A.; Diaz, K.; Vidalon, J.; Linan, C.; Pacheco-Pereira, C.; Lagravere Vich, M.O. Can Gray Values Be Converted to Hounsfield Units? A Systematic Review. Dentomaxillofac. Radiol. 2022, 51, 20210140. [Google Scholar] [CrossRef] [PubMed]
- Abdulkarim, H.H.; Zeng, R.; Pazdernik, V.K.; Davis, J.M. Effect of Bone Graft on the Correlation between Clinical Bone Quality and CBCT-Determined Bone Density: A Pilot Study. J. Contemp. Dent. Pract. 2021, 22, 756–762. [Google Scholar] [CrossRef]
- Schnutenhaus, S.; Götz, W.; Dreyhaupt, J.; Rudolph, H.; Luthardt, R.G.; Edelmann, C. Associations among Primary Stability, Histomorphometric Findings, and Bone Density: A Prospective Randomized Study after Alveolar Ridge Preservation with a Collagen Cone. Dent. J. 2020, 8, 112. [Google Scholar] [CrossRef] [PubMed]
- Ivanova, V.; Chenchev, I.; Zlatev, S.; Mijiritsky, E. Correlation between Primary, Secondary Stability, Bone Density, Percentage of Vital Bone Formation and Implant Size. Int. J. Environ. Res. Public Health 2021, 18, 6994. [Google Scholar] [CrossRef]
- Al-Jamal, M.F.J.; Al-Jumaily, H.A. Can the Bone Density Estimated by CBCT Predict the Primary Stability of Dental Implants? A New Measurement Protocol. J. Craniofac. Surg. 2021, 32, e171–e174. [Google Scholar] [CrossRef]
- Isoda, K.; Ayukawa, Y.; Tsukiyama, Y.; Sogo, M.; Matsushita, Y.; Koyano, K. Relationship between the Bone Density Estimated by Cone-Beam Computed Tomography and the Primary Stability of Dental Implants. Clin. Oral Implants Res. 2012, 23, 832–836. [Google Scholar] [CrossRef]
- Salimov, F.; Tatli, U.; Kürkçü, M.; Akoğlan, M.; Oztunç, H.; Kurtoğlu, C. Evaluation of Relationship between Preoperative Bone Density Values Derived from Cone Beam Computed Tomography and Implant Stability Parameters: A Clinical Study. Clin. Oral Implants Res. 2014, 25, 1016–1021. [Google Scholar] [CrossRef]
- Wada, M.; Suganami, T.; Sogo, M.; Maeda, Y. Can We Predict the Insertion Torque Using the Bone Density around the Implant? Int. J. Oral Maxillofac. Surg. 2016, 45, 221–225. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Teeth Extraction Day | 10th Day after the Extraction | 6 Months after Extraction |
|---|---|---|
|
|
|
| Factor | Group I * | Group II * | McNemar Test | ||
|---|---|---|---|---|---|
| Number | % | Number | % | ||
| Clean wound | 48 | 96.0 | 41 | 82.0 | Chi2 = 5.14, p = 0.0233 |
| Infected wound | 2 | 4.0 | 9 | 18.0 | |
| No swelling | 37 | 74.0 | 32 | 64.0 | Chi2 = 2.29, p = 0.1306 |
| Swelling | 13 | 26.0 | 18 | 36.0 | |
| No discharge | 48 | 96.0 | 41 | 82.0 | Chi2 = 5.14, p = 0.0233 |
| Discharge | 2 | 4.0 | 9 | 18.0 | |
| VAS pain < 5 | 38 | 76.0 | 29 | 58.0 | Chi2 = 4.92, p = 0.0265 |
| VAS pain > 5 | 12 | 24.0 | 21 | 42.0 | |
| Tight wound | 48 | 96.0 | 44 | 88.0 | Chi2 = 1.50, p = 0.2207 |
| Wound dehiscence | 2 | 4.0 | 6 | 12.0 | |
| Variable | Time Post-Extraction | Group * | Descriptive Statistics | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Standard Deviation | Minimum | Lower Quartile | Median | Upper Quartile | Maximum | Wilcoxon Signed-Rank Test | |||
| Alveolar width | 0 days | I | 10.92 | 2.15 | 7.0 | 9.0 | 11.3 | 13.0 | 14.5 | Z = 0.83 p = 0.4043 |
| II | 11.01 | 1.95 | 7.0 | 10.0 | 11.0 | 12.0 | 14.0 | |||
| 6 months | I | 9.43 | 1.74 | 5.5 | 8.0 | 9.8 | 11.0 | 12.5 | Z = 2.63 p = 0.0085 | |
| II | 9.16 | 1.51 | 6.0 | 8.0 | 9.5 | 10.0 | 12.0 | |||
| HIC | 0 days | I | 9.05 | 1.27 | 7.0 | 8.5 | 9.0 | 10.0 | 12.0 | Z = 0.47 p = 0.6402 |
| II | 9.01 | 1.21 | 7.0 | 8.0 | 9.0 | 10.0 | 12.0 | |||
| 6 months | I | 10.84 | 1.19 | 9.0 | 10.0 | 11.0 | 11.5 | 13.0 | Z = 1.17 p = 0.2418 | |
| II | 11.01 | 1.26 | 8.5 | 10.0 | 11.0 | 12.0 | 14.5 | |||
| Width change (bone loss) | - | I | 1.49 | 0.84 | 0.5 | 1.0 | 1.5 | 2.0 | 4.5 | Z = 3.16 p = 0.0016 |
| II | 1.85 | 0.86 | 0.0 | 1.5 | 2.0 | 2.5 | 4.5 | |||
| Height change (bone loss) | - | I | 1.79 | 0.61 | 0.5 | 1.5 | 1.5 | 2.0 | 3.0 | Z = 2.03 p = 0.0426 |
| II | 1.98 | 0.76 | 0.5 | 1.5 | 2.0 | 2.5 | 4.5 | |||
| Variable | Group * | Descriptive Statistics | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Standard Deviation | Minimum | Lower Quartile | Median | Upper Quartile | Maximum | Wilcoxon Signed-Rank Test | ||
| GV (point A) | I | 308.16 | 128.15 | 55.0 | 226.0 | 282.5 | 441.0 | 557.0 | Z = 2.59 p = 0.0097 |
| II | 279.40 | 136.23 | 75.0 | 162.0 | 256.0 | 390.0 | 576.0 | ||
| GV (point B) | I | 331.10 | 131.22 | 98.0 | 250.0 | 301.5 | 473.0 | 636.0 | Z = 2.59 p = 0.0097 |
| II | 305.54 | 139.12 | 87.0 | 187.0 | 289.0 | 428.0 | 623.0 | ||
| Variable | Time Post-Extraction | Group * | Descriptive Statistics | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Standard Deviation | Minimum | Lower Quartile | Median | Upper Quartile | Maximum | Wilcoxon Signed-Rank Test | |||
| Alveolar width | 0 days | I | 12.53 | 2.51 | 8.0 | 10.5 | 12.0 | 14.5 | 17.5 | Z = 1.49 p = 0.1357 |
| II | 12.70 | 2.32 | 8.5 | 11.0 | 12.0 | 15.0 | 18.0 | |||
| 6 months | I | 11.66 | 2.34 | 7.0 | 10.0 | 11.5 | 13.0 | 16.0 | Z = 0.51 p = 0.6105 | |
| II | 11.52 | 1.96 | 8.0 | 10.0 | 11.0 | 13.0 | 16.0 | |||
| Alveolar height | 0 days | I | 9.70 | 1.95 | 6.0 | 8.0 | 9.5 | 11.0 | 14.0 | Z = 0.72 p = 0.4692 |
| II | 9.71 | 1.87 | 6.0 | 8.0 | 9.5 | 11.0 | 14.0 | |||
| 6 months | I | 8.09 | 1.91 | 4.5 | 7.0 | 8.0 | 9.5 | 12.5 | Z = 1.07 p = 0.2854 | |
| II | 7.96 | 2.00 | 4.0 | 6.5 | 7.8 | 10.0 | 12.0 | |||
| Width change (bone loss) | - | I | 0.87 | 0.60 | 0.0 | 0.5 | 1.0 | 1.0 | 3.0 | Z = 1.78 p = 0.0749 |
| II | 1.18 | 1.10 | 0.0 | 0.5 | 1.0 | 2.0 | 4.0 | |||
| Height change (bone loss) | - | I | 1.59 | 0.49 | 0.5 | 1.0 | 1.5 | 2.0 | 2.5 | Z = 2.44 p = 0.0148 |
| II | 1.85 | 0.75 | 0.0 | 1.5 | 2.0 | 2.0 | 4.0 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niedzielska, I.; Ciapiński, D.; Bąk, M.; Niedzielski, D. The Assessment of the Usefulness of Platelet-Rich Fibrin in the Healing Process Bone Resorption. Coatings 2022, 12, 247. https://doi.org/10.3390/coatings12020247
Niedzielska I, Ciapiński D, Bąk M, Niedzielski D. The Assessment of the Usefulness of Platelet-Rich Fibrin in the Healing Process Bone Resorption. Coatings. 2022; 12(2):247. https://doi.org/10.3390/coatings12020247
Chicago/Turabian StyleNiedzielska, Iwona, Daniel Ciapiński, Michał Bąk, and Damian Niedzielski. 2022. "The Assessment of the Usefulness of Platelet-Rich Fibrin in the Healing Process Bone Resorption" Coatings 12, no. 2: 247. https://doi.org/10.3390/coatings12020247
APA StyleNiedzielska, I., Ciapiński, D., Bąk, M., & Niedzielski, D. (2022). The Assessment of the Usefulness of Platelet-Rich Fibrin in the Healing Process Bone Resorption. Coatings, 12(2), 247. https://doi.org/10.3390/coatings12020247