Impact and Sustainability of Antibiotic Stewardship in Pediatric Emergency Departments: Why Persistence Is the Key to Success

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Results
2.1. Pharyngitis
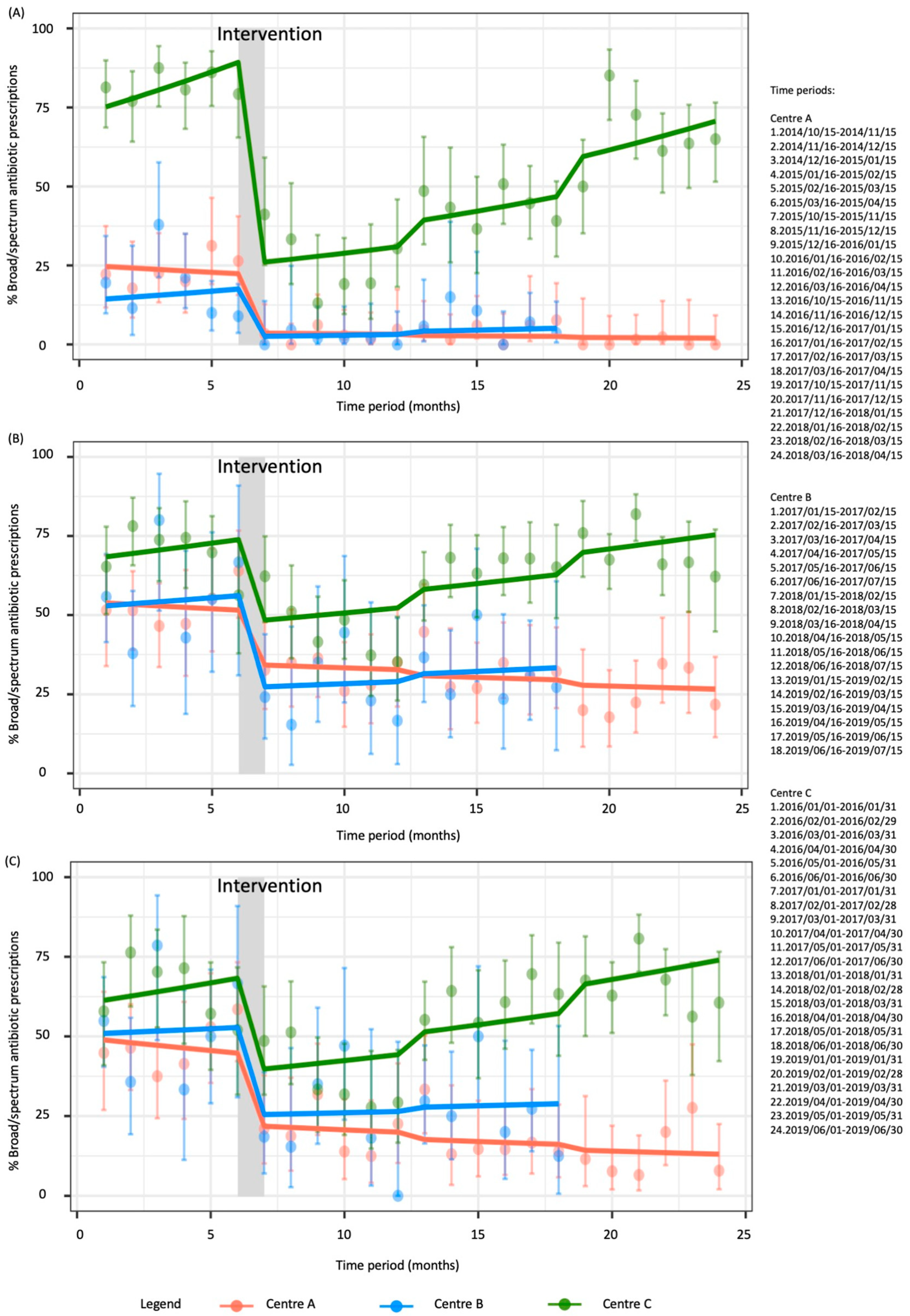
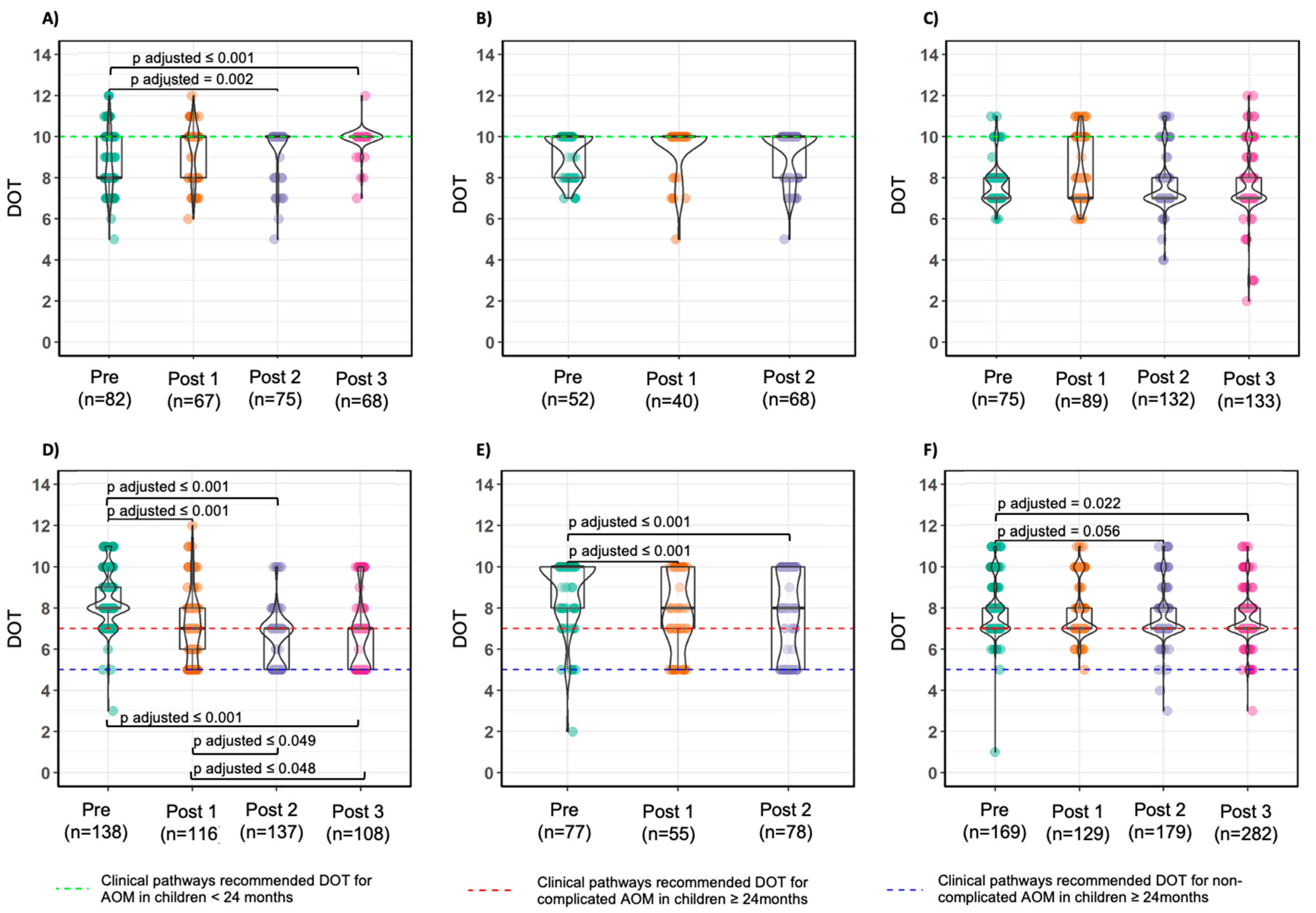
2.2. Acute Otitis Media—Total
2.3. Acute Otitis Media—Sensitivity Analysis
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Intervention
4.3. Population and Case Definition
4.4. Outcomes
- “Wait-and-see” approach rates (AOM only);
- Broad-spectrum antibiotic prescriptions rates;
- Rates by active agent;
- Amoxicillin and co-amoxiclav dosage, expressed in mg/kg/day (Center A and Center B only);
- Duration of therapy expressed in DOT.
4.5. Data Collection and Sample Size Calculation
4.6. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

References
- Sturkenboom, M.C.J.M.; Verhamme, K.M.C.; Nicolosi, A.; Murray, M.L.; Neubert, A.; Caudri, D.; Picelli, G.; Sen, E.F.; Giaquinto, C.; Cantarutti, L.; et al. Drug use in children: Cohort study in three European countries. BMJ 2008, 337, 2245. [Google Scholar] [CrossRef] [PubMed]
- Messina, F.; Clavenna, A.; Cartabia, M.; Piovani, D.; Bortolotti, A.; Fortino, I.; Merlino, L.; Bonati, M. Antibiotic prescription in the outpatient paediatric population attending emergency departments in Lombardy, Italy: A retrospective database review. BMJ Paediatr. Open 2019, 3, e000546. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, E.; Donà, D.; Cantarutti, A.; Lundin, R.; Scamarcia, A.; Corrao, G.; Giaquinto, C. Antibiotic prescriptions in acute otitis media and pharyngitis in Italian pediatric outpatients. Italy J. Pediatr. 2019, 45, 103. [Google Scholar] [CrossRef] [PubMed]
- Marchisio, P.; Esposito, S.; Picca, M.; Baggi, E.; Terranova, L.; Orenti, A.; Biganzoli, E.; Principi, N.; Gallia, P.; Mazzucchi, E.; et al. Prospective evaluation of the aetiology of acute otitis media with spontaneous tympanic membrane perforation. Clin. Microbiol. Infect. 2017, 23, 486.e1–486.e6. [Google Scholar] [CrossRef]
- Kronman, M.P.; Zhou, C.; Mangione-Smith, R. Bacterial prevalence and antimicrobial prescribing trends for acute respiratory tract infections. Pediatrics 2014, 134, e956–e965. [Google Scholar] [CrossRef]
- Donà, D.; Barbieri, E.; Daverio, M.; Lundin, R.; Giaquinto, C.; Zaoutis, T.; Sharland, M. Implementation and impact of pediatric antimicrobial stewardship programs: A systematic scoping review. Antimicrob Resist. Infect Control 2020, 9, 3. [Google Scholar] [CrossRef]
- Samore, M.H.; Bateman, K.; Alder, S.C.; Hannah, E.; Donnelly, S.; Stoddard, G.J.; Haddadin, B.; Rubin, M.A.; Williamson, J.; Stults, B.; et al. Clinical decision support and appropriateness of antimicrobial prescribing: A randomized trial. JAMA 2005, 294, 2305–2314. [Google Scholar] [CrossRef]
- Donà, D.; Zingarella, S.; Gastaldi, A.; Lundin, R.; Perilongo, G.; Frigo, A.C.; Hamdy, R.F.; Zaoutis, T.; Da Dalt, L.; Giaquinto, C. Effects of clinical pathway implementation on antibiotic prescriptions for pediatric community-acquired pneumonia. PLoS ONE 2018, 13, e0193581. [Google Scholar] [CrossRef]
- Donà, D.; Luise, D.; Barbieri, E.; Masiero, N.; Maita, S.; Antoniello, L.; Zaoutis, T.; Giaquinto, C.; Gamba, P. Effectiveness and Sustainability of an Antimicrobial Stewardship Program for Perioperative Prophylaxis in Pediatric Surgery. Pathogens 2020, 9, 490. [Google Scholar] [CrossRef]
- Dona, D.; Baraldi, M.; Brigadoi, G.; Lundin, R.; Perilongo, G.; Hamdy, R.F.; Zaoutis, T.; Da Dalt, L.; Giaquinto, C. The Impact of Clinical Pathways on Antibiotic Prescribing for Acute Otitis Media and Pharyngitis in the Emergency Department. Pediatr. Infect Dis. J. 2018, 37, 901–907. [Google Scholar] [CrossRef]
- Spuesens, E.B.M.; Fraaij, P.L.A.; Visser, E.G.; Hoogenboezem, T.; Hop, W.C.J.; Van Adrichem, L.N.A.; Weber, F.; Moll, H.A.; Broekman, B.; Berger, M.Y.; et al. Carriage of Mycoplasma pneumoniae in the upper respiratory tract of symptomatic and asymptomatic children: An observational study. PLoS Med. 2013, 10, e1001444. [Google Scholar] [CrossRef] [PubMed]
- Ståhlgren, G.S.; Tyrstrup, M.; Edlund, C.; Giske, C.G.; Mölstad, S.; Norman, C.; Rystedt, K.; Sundvall, P.-D.; Hedin, K. Penicillin V four times daily for five days versus three times daily for 10 days in patients with pharyngotonsillitis caused by group A streptococci: Randomised controlled, open label, non-inferiority study. BMJ 2019, 367, l5337. [Google Scholar] [CrossRef] [PubMed]
- Pichichero, M.E. Treatment and prevention of streptococcal pharyngitis. In Up to Date; Post, T.W., Ed.; UpToDate: Waltham, MA, USA, 2015. [Google Scholar]
- Lieberthal, A.S.; Carroll, A.E.; Chonmaitree, T.; Ganiats, T.G.; Hoberman, A.; Jackson, M.A.; Joffe, M.D.; Miller, D.T.; Rosenfeld, R.M.; Sevilla, X.D.; et al. The diagnosis and management of acute otitis media. Pediatrics 2013, 131, e964–e999. [Google Scholar] [CrossRef]
- SIP Guidelines. Available online: https://sip.it/2019/06/17/gestione-otite-media-acuta-linee-guida/ (accessed on 1 December 2020). (In Italian).
- Fischer, T.; Singer, A.J.; Lee, C.; Thode, H.C., Jr. National trends in emergency department antibiotic prescribing for children with acute otitis media, 1996–2005. Acad. Emerg. Med. 2007, 14, 1172–1175. [Google Scholar] [CrossRef]
- Arguedas, A.; Dagan, R.; Leibovitz, E.; Hoberman, A.; Pichichero, M.; Paris, M. A multicenter, open label, double tympanocentesis study of high dose cefdinir in children with acute otitis media at high risk of persistent or recurrent infection. Pediatr. Infect Dis. J. 2006, 25, 211–218. [Google Scholar] [CrossRef]
- Agenzia Italiana del Farmaco—Italian Medicine Agency. Available online: https://farmaci.agenziafarmaco.gov.it/bancadatifarmaci/cerca-per-principioattivo?princ_att=Amoxicillina%20e%20inibitori%20enzimatici (accessed on 31 July 2020).
- Hoberman, A.; Paradise, J.L.; Rockette, H.E.; Jeong, J.-H.; Kearney, D.H.; Bhatnagar, S.; Shope, T.R.; Muñiz, G.; Martin, J.M.; Kurs-Lasky, M.; et al. Reduced-Concentration Clavulanate for Young Children with Acute Otitis Media. Antimicrob. Agents Chemother. 2017, 61, e00238-17. [Google Scholar] [CrossRef]
- Gerber, J.S.; Prasad, P.A.; Fiks, A.G.; Localio, A.R.; Bell, L.M.; Keren, R.; Zaoutis, T.E. Durability of benefits of an outpatient antimicrobial stewardship intervention after discontinuation of audit and feedback. JAMA 2014, 312, 2569–2570. [Google Scholar] [CrossRef] [PubMed]
- Linder, J.A.; Meeker, D.; Fox, C.R.; Friedberg, M.W.; Persell, S.D.; Goldstein, N.J.; Doctor, J.N. Effects of Behavioral Interventions on Inappropriate Antibiotic Prescribing in Primary Care 12 Months After Stopping Interventions. JAMA 2017, 318, 1391–1392. [Google Scholar] [CrossRef] [PubMed]
- Velasco-Arnaiz, E.; Simó-Nebot, S.; Ríos-Barnés, M.; Ramos, M.G.L.; Monsonís, M.; Urrea-Ayala, M.; Jordan, I.; Mas-Comas, A.; Casadevall-Llandrich, R.; Ormazábal-Kirchner, D.; et al. Benefits of a Pediatric Antimicrobial Stewardship Program in Antimicrobial Use and Quality of Prescriptions in a Referral Children’s Hospital. J. Pediatr. 2020, 225, 222–230.e1. [Google Scholar] [CrossRef] [PubMed]
- De Luca, M.; Donà, D.; Montagnani, C.; Vecchio, A.L.; Romanengo, M.; Tagliabue, C.; Centenari, C.; D’Argenio, P.; Lundin, R.; Giaquinto, C.; et al. Antibiotic Prescriptions and Prophylaxis in Italian Children. Is It Time to Change? Data from the ARPEC Project. PLoS ONE 2016, 11, e0154662. [Google Scholar] [CrossRef] [PubMed]
- Hsia, Y.; Lee, B.R.; Versporten, A.; Yang, Y.; Bielicki, J.; Jackson, C.; Newland, J.; Goossens, H.; Magrini, N.; Sharland, M. Use of the WHO Access, Watch, and Reserve classification to define patterns of hospital antibiotic use (AWaRe): An analysis of paediatric survey data from 56 countries. Lancet Glob. Health 2019, 7, e861–e871. [Google Scholar] [CrossRef]
- Bremmer, D.N.; Trienski, T.L.; Walsh, T.L.; Moffa, M.A. Role of Technology in Antimicrobial Stewardship. Med. Clin. N. Am. 2018, 102, 955–963. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2017, 46, 348–355. [Google Scholar] [CrossRef]
- Kang, H. The prevention and handling of the missing data. Korean J. Anesthesiol. 2013, 64, 402–406. [Google Scholar] [CrossRef]
- Kleinke, K. Multiple imputation by predictive mean matching when sample size is small. Methodol. Eur. J. Res. Methods Behav. Soc. Sci. 2018, 14, 3–15. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 1 December 2020).
- Van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45. [Google Scholar] [CrossRef]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; Available online: https://ggplot2-book.org/ (accessed on 1 December 2020).
- Patil, I. Ggstatsplot: “ggplot2” Based Plots with Statistical Details. CRAN 2018. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Center A | Center B | Center C | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Period | Pre | Post 1 | Post 2 | Post 3 | p-Value | Pre | Post 1 | Post 2 | p-Value | Pre | Post 1 | Post 2 | Post 3 | p-Value |
| 298 | 364 | 326 | 264 | 290 | 241 | 251 | 363 | 217 | 316 | 319 | ||||
| No antibiotic, N (%) | 147 (49.3) | 198 (54.4) | 120 (36.8) | 129 (48.9) | <0.001 | 135 (46.6) | 140 (58.1) | 122 (48.6) | 0.021 | 23 (6.3) | 15 (6.9) | 44 (13.9) | 23 (7.2) | 0.002 |
| Antibiotic therapy, N (%) | 151 (50.7) | 166 (45.6) | 206 (63.2) | 135 (51.1) | 155 (53.4) | 101 (41.9) | 129 (51.4) | 340 (93.7) | 202 (93.1) | 272 (86.1) | 296 (92.8) | |||
| Amoxicillin, N (%) | 81 (53.6) | 155 (93.4) | 192 (93.2) | 133 (98.5) | <0.001 | 108 (69.7) | 97 (96.0) | 114 (88.4) | <0.001 | 42 (12.4) | 144 (71.3) | 133 (48.9) | 84 (28.4) | <0.001 |
| Broad spectrum, N (%) | 70 (46.4) | 11 (6.6) | 14 (6.8) | 2 (1.5) | 47 (30.3) | 4 (4.0) | 15 (11.6) | 298 (87.6) | 58 (28.7) | 139 (51.1) | 212 (71.6) | |||
| Co-amoxiclav, N (%) | 60 (39.7) | 5 (3.0) | 9 (4.4) | 1 (0.7) | <0.001 | 28 (18.1) | 1 (1.0) | 5 (3.9) | <0.001 | 249 (73.2) | 45 (22.3) | 102 (37.5) | 170 (57.4) | <0.001 |
| Cephalosporins, N (%) | 10 (6.6) | 6 (3.6) | 4 (1.9) | 1 (0.7) | 0.029 | 14 (9.0) | 3 (3.0) | 7 (5.4) | 0.131 | 17 (5.0) | 4 (2.0) | 25 (9.2) | 33 (11.1) | <0.001 |
| Macrolides, N (%) | 0 (0.0) | 0 (0.0) | 1 (0.5) | 0 (0.0) | 5 (3.2) | 0 (0.0) | 3 (2.3) | 0.203 | 32 (9.4) | 9 (4.5) | 12 (4.4) | 9 (3.0) | 0.004 | |
| Amoxicillin dosage, Median [IQR], mg/kg/die | 50.0 [0.0] | 50.0 [0.0] | 50.0 [1.0] | 50.0 [0.0] | 0.288 | 53.7 [7.0] | 50.6 [3.5] | 51.6 [3.8] | <0.001 | / | / | / | / | / |
| Days of therapy, Median [IQR] | 8.0 [3.0] | 10.0 [0.0] | 10.0 [0.0] | 10.0 [0.0] | <0.001 | 10.0 [1.0] | 10.0 [0.0] | 10.0 [0.0] | 0.622 | 7.0 [0.0] | 7.0 [3.0] | 8.00 [1.0] | 7.0 [1.0] | <0.001 |
| Center A | Center B | Center C | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Period | Pre | Post 1 | Post 2 | Post 3 | p-Value | Pre | Post 1 | Post 2 | p-Value | Pre | Post 1 | Post 2 | Post 3 | p-Value |
| 281 | 273 | 299 | 267 | 139 | 105 | 151 | 302 | 324 | 387 | 481 | ||||
| Wait and see, N (%) | 61 (21.7) | 90 (33.0) | 87 (29.1) | 91 (34.1) | 0.006 | 10 (7.2) | 10 (9.5) | 5 (3.3) | 0.116 | 58 (19.2) | 106 (32.7) | 76 (19.6) | 66 (13.7) | <0.001 |
| Antibiotic treatment, N (%) | 220 (78.3) | 183 (67.0) | 212 (70.9) | 176 (65.9) | 129 (92.8) | 95 (90.5) | 146 (96.7) | 244 (80.8) | 218 (67.3) | 311 (80.4) | 415 (86.3) | |||
| Amoxicillin, N (%) | 72 (32.7) | 95 (51.9) | 113 (53.3) | 109 (61.9) | <0.001 | 56 (43.4) | 66 (69.5) | 97 (66.4) | <0.001 | 30 (12.3) | 69 (31.7) | 59 (19.0) | 73 (17.6) | <0.001 |
| Broad spectrum, N (%) | 148 (67.3) | 88 (48.1) | 99 (46.7) | 67 (38.1) | 73 (56.6) | 29 (30.5) | 49 (33.6) | 214 (87.7) | 149 (68.3) | 252 (81.0) | 342 (82.4) | |||
| Co-amoxiclav, N (%) | 100 (45.5) | 68 (37.2) | 83 (39.2) | 62 (35.2) | 0.169 | 44 (34.1) | 22 (23.2) | 34 (23.3) | 0.081 | 165 (67.6) | 121 (55.5) | 184 (59.2) | 293 (70.6) | <0.001 |
| Cephalosporins, N (%) | 44 (20.0) | 16 (8.7) | 14 (6.6) | 5 (2.8) | <0.001 | 28 (21.7) | 5 (5.3) | 15 (10.3) | <0.001 | 43 (17.6) | 26 (11.9) | 62 (19.9) | 45 (10.8) | 0.002 |
| Macrolides, N (%) | 4 (1.8) | 4 (2.2) | 1 (0.5) | 0 (0.0) | 0.119 | 1 (0.8) | 2 (2.1) | 0 (0.0) | 0.187 | 6 (2.5) | 2 (0.9) | 6 (1.9) | 4 (1.0) | 0.364 |
| Fluoroquinolones, N (%) | 0 (0.0) | 0 (0.0) | 1 (0.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| Amoxicillin dosage, Median [IQR], mg/kg/die | 50.0 [0.0] | 75.0 [25.0] | 75.0 [4.0] | 75.0 [0.0] | <0.001 | 57.6 [14.3] | 73.0 [8.6] | 75.0 [7.1] | <0.001 | / | / | / | / | |
| Co-amoxiclav dosage, Median [IQR], mg/kg/die | 50.0 [10.0] | 75.0 [25.0] | 73.0 [15.2] | 75.0 [5.0] | <0.001 | 56.7 [7.9] | 63.1 [23.9] | 68.6 [15.2] | <0.001 | / | / | / | / | |
| Days of therapy, Median [IQR], 2–23 months | 8.0 [2.0] | 10.0 [2.0] | 10.0 [0.0] | 10.0 [0.0] | <0.001 | 10.0 [2.0] | 10.0 [0.0] | 10.0 [2.0] | 0.170 | 7.0 [1.0] | 7.0 [3.0] | 7.0 [1.0] | 7.0 [1.0] | 0.024 |
| Days of therapy, Median [IQR], ≥24 months | 8.0 [1.0] | 7.0 [2.0] | 7.0 [2.0] | 7.0 [2.0] | <0.001 | 10.0 [2.0] | 8.0 [3.0] | 8.0 [5.0] | <0.001 | 7.0 [1.0] | 7.0 [1.0] | 7.0 [1.0] | 7.0 [1.0] | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbieri, E.; De Luca, M.; Minute, M.; D’Amore, C.; Ciofi Degli Atti, M.L.; Martelossi, S.; Giaquinto, C.; Da Dalt, L.; Zaoutis, T.; Dona, D. Impact and Sustainability of Antibiotic Stewardship in Pediatric Emergency Departments: Why Persistence Is the Key to Success. Antibiotics 2020, 9, 867. https://doi.org/10.3390/antibiotics9120867
Barbieri E, De Luca M, Minute M, D’Amore C, Ciofi Degli Atti ML, Martelossi S, Giaquinto C, Da Dalt L, Zaoutis T, Dona D. Impact and Sustainability of Antibiotic Stewardship in Pediatric Emergency Departments: Why Persistence Is the Key to Success. Antibiotics. 2020; 9(12):867. https://doi.org/10.3390/antibiotics9120867
Chicago/Turabian StyleBarbieri, Elisa, Maia De Luca, Marta Minute, Carmen D’Amore, Marta Luisa Ciofi Degli Atti, Stefano Martelossi, Carlo Giaquinto, Liviana Da Dalt, Theoklis Zaoutis, and Daniele Dona. 2020. "Impact and Sustainability of Antibiotic Stewardship in Pediatric Emergency Departments: Why Persistence Is the Key to Success" Antibiotics 9, no. 12: 867. https://doi.org/10.3390/antibiotics9120867
APA StyleBarbieri, E., De Luca, M., Minute, M., D’Amore, C., Ciofi Degli Atti, M. L., Martelossi, S., Giaquinto, C., Da Dalt, L., Zaoutis, T., & Dona, D. (2020). Impact and Sustainability of Antibiotic Stewardship in Pediatric Emergency Departments: Why Persistence Is the Key to Success. Antibiotics, 9(12), 867. https://doi.org/10.3390/antibiotics9120867