Impact of the COVID-19 Pandemic on Antimicrobial Consumption and Hospital-Acquired Candidemia and Multidrug-Resistant Bloodstream Infections

 , , , , , , , and
, , , , , , , and
Abstract
1. Introduction
2. Results
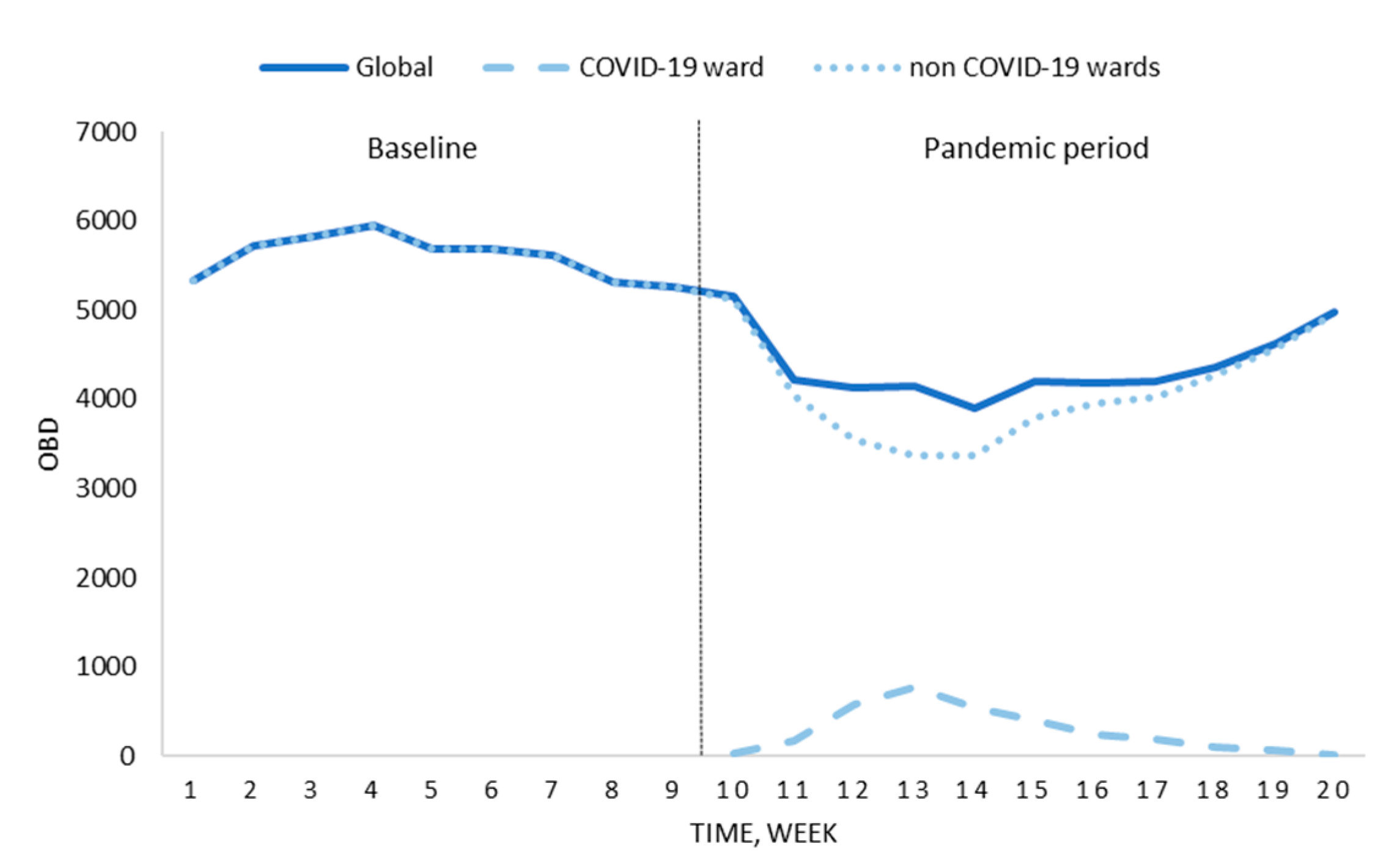
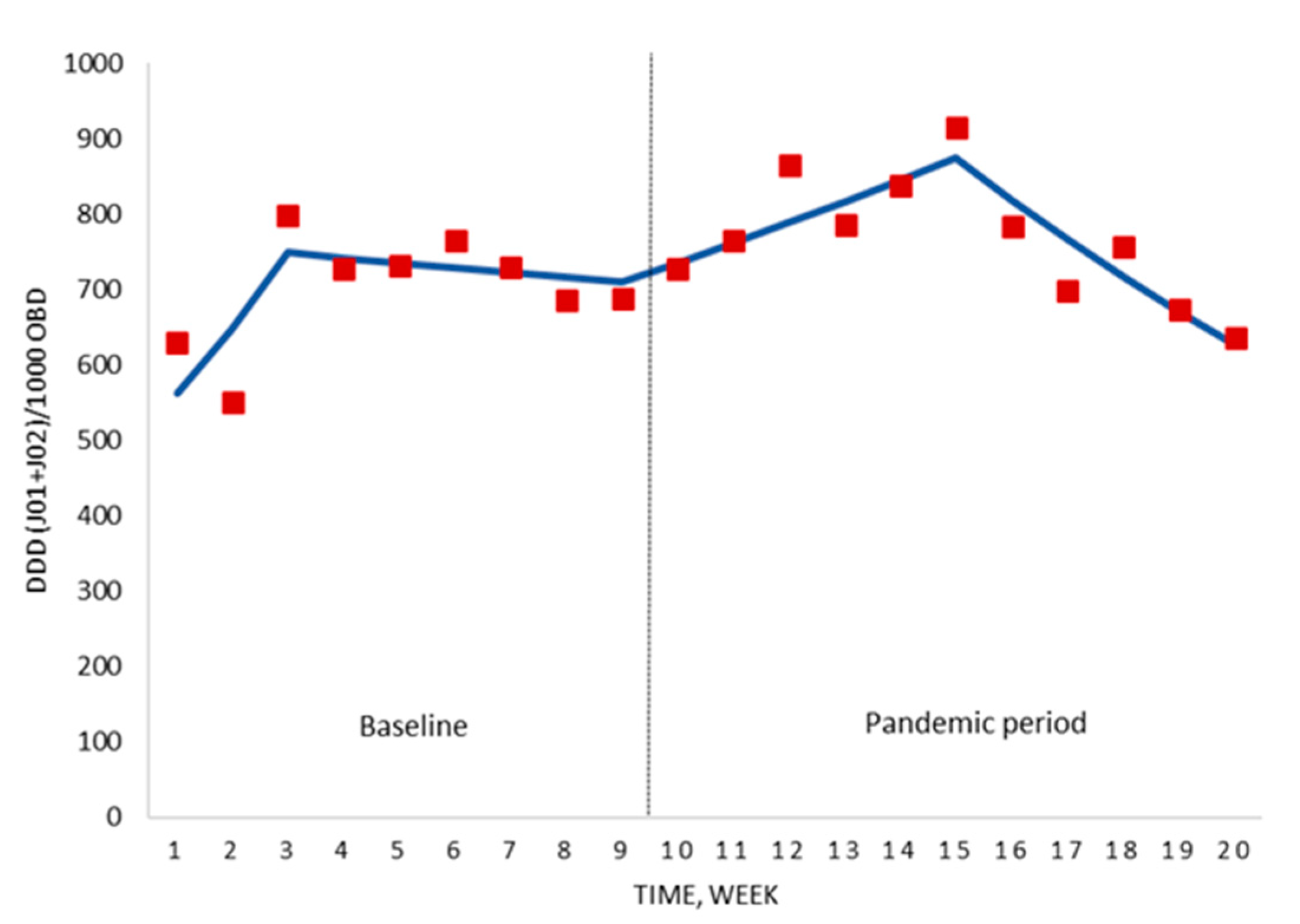
2.1. Antimicrobial Consumption
2.2. Incidence of Hospital-Acquired Candidemia and MDR Bacterial BSI
2.3. Death Rate of Hospital-Acquired Candidemia and MDR Bacterial BSI
3. Discussion
4. Materials and Methods
4.1. Setting
4.2. Study Design and Period
4.3. Hospital Response for the COVID-19 Pandemic
4.4. Study Measures
4.5. Microbiological Information
4.6. Statistical Analysis
4.7. Ethics Approval
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 8 November 2020).
- European Centre for Disease Prevention and Control. COVID-19 Situation Update for the EU/EEA and the UK. 2020. Available online: https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea (accessed on 8 November 2020).
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Phelan, A.L.; Katz, R.; Gostin, L.O. The Novel Coronavirus Originating in Wuhan, China: Challenges for Global Health Governance. JAMA 2020, 323, 709–710. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J. Covid-19 and the Stiff Upper Lip—The Pandemic Response in the United Kingdom. N. Engl. J. Med. 2020, 382, e31. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Castro-Sanchez, E.; Charani, E.; Davies, F.; Satta, G.; Ellington, M.J.; Holmes, A.H. COVID-19 and the potential long-term impact on antimicrobial resistance. J. Antimicrob. Chemother. 2020, 75, 1681–1684. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and fungal co-infection in individuals with coronavirus: A rapid review to support COVID-19 antimicrobial prescribing. Clin. Infect. Dis. 2020, ciaa530. [Google Scholar] [CrossRef]
- World Health Organization. Q&A on Coronaviruses (COVID-19). 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/q-a-coronaviruses (accessed on 8 November 2020).
- Youngs, J.; Wyncoll, D.; Hopkins, P.; Arnold, A.; Ball, J.; Bicanic, T. Improving antibiotic stewardship in COVID-19: Bacterial co-infection is less common than with influenza. J. Infect. 2020, 81, e55–e57. [Google Scholar] [CrossRef]
- Hsu, J. How COVID-19 is accelerating the threat of antimicrobial resistance. BMJ 2020, 369, m1983. [Google Scholar] [CrossRef]
- Rawson, T.M.; Ming, D.; Ahmad, R.; Moore, L.S.P.; Holmes, A.H. Antimicrobial use, drug-resistant infections and COVID-19. Nat. Rev. Microbiol. 2020, 18, 409–410. [Google Scholar] [CrossRef]
- Rossato, L.; Negrão, F.J.; Simionatto, S. Could the COVID-19 pandemic aggravate antimicrobial resistance? Am. J. Infect. Control 2020, 48, 1129–1130. [Google Scholar] [CrossRef]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an antibiotic stewardship program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Huttner, B.D.; Catho, G.; Pano-Pardo, J.R.; Pulcini, C.; Schouten, J. COVID-19: Don’t neglect antimicrobial stewardship principles! Clin. Microbiol. Infect. 2020, 26, 808–810. [Google Scholar] [CrossRef] [PubMed]
- Spernovasilis, N.A.; Kofteridis, D.P. COVID-19 and antimicrobial stewardship: What is the interplay? Infect. Control Hosp. Epidemiol. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Mazdeyasna, H.; Nori, P.; Patel, P.; Doll, M.; Godbout, E.; Lee, K.; Noda, A.J.; Bearman, G.; Stevens, M.P. Antimicrobial Stewardship at the Core of COVID-19 Response Efforts: Implications for Sustaining and Building Programs. Curr. Infect. Dis. Rep. 2020, 22, 23. [Google Scholar] [CrossRef]
- Stevens, M.P.; Patel, P.K.; Nori, P. Involving antimicrobial stewardship programs in COVID-19 response efforts: All hands on deck. Infect. Control Hosp. Epidemiol. 2020, 41, 744–745. [Google Scholar] [CrossRef]
- Martin, E.; Philbin, M.; Hughes, G.; Bergin, C.; Talento, A.F. Antimicrobial stewardship challenges and innovative initiatives in the acute hospital setting during the COVID-19 pandemic. J. Antimicrob. Chemother. 2020, dkaa400. [Google Scholar] [CrossRef]
- Cisneros, J.M.; Neth, O.; Gil-Navarro, M.V.; Lepe, J.A.; Jiménez-Parrilla, F.; Cordero, E.; Rodríguez-Hernández, M.J.; Amaya-Villar, R.; Cano, J.; Gutiérrez-Pizarraya, A.; et al. Global impact of an educational antimicrobial stewardship program on prescribing practice in a tertiary hospital centre. Clin. Microbiol. Infect. 2014, 20, 82–88. [Google Scholar] [CrossRef]
- Molina, J.; Peñalva, G.; Gil-Navarro, M.V.; Praena, J.; Lepe, J.A.; Pérez-Moreno, M.A.; Ferrándiz, C.; Aldabó, T.; Aguilar, M.; Olbrich, P.; et al. Long-Term Impact of an educational antimicrobial stewardship program on hospital-acquired candidemia and multidrug-resistant bloodstream infections: A quasi-experimental study of interrupted time-series analysis. Clin. Infect. Dis. 2017, 65, 1992–1999. [Google Scholar] [CrossRef]
- Plan Nacional Frente a la Resistencia a Los Antibióticos (PRAN). Noticias. 2020. Available online: http://resistenciaantibioticos.es/es/noticias/espana-reduce-un-54-el-consumo-de-antibioticos-en-salud-humana-y-un-136-las-ventas-de (accessed on 8 November 2020).
- Abelenda-Alonso, G.; Padullés, A.; Rombauts, A.; Gudiol, C.; Pujol, M.; Alvarez-Pouso, C.; Jodar, R.; Carratalà, J. Antibiotic prescription during the COVID-19 pandemic: A biphasic pattern. Infect. Control Hosp. Epidemiol. 2020, 1371–1372. [Google Scholar] [CrossRef]
- Liew, Y.; Lee, W.H.L.; Tan, L.; Kwa, A.L.H.; Thien, S.Y.; Cherng, B.P.Z.; Chung, S.J. Antimicrobial stewardship program: A vital resource for hospitals during the global outbreak of coronavirus disease 2019 (COVID-19). Int. J. Antimicrob. Agents 2020, 56, 106145. [Google Scholar] [CrossRef]
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Ortwine, J.K.; Mang, N.S.; Joseph, C.; Hall, B.C.; Prokesch, B.C. Limited Role for Antibiotics in COVID-19: Scarce Evidence of Bacterial Coinfection. SSRN 2020. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Stevens, R.W.; Jensen, K.; O’Horo, J.C.; Shah, A. Antimicrobial prescribing practices at a tertiary care center in patients diagnosed with COVID-19 across the continuum of care. Infect. Control Hosp. Epidemiol. 2020, 1–14. [Google Scholar] [CrossRef]
- Tiri, B.; Sensi, E.; Marsiliani, V.; Cantarini, M.; Priante, G.; Vernelli, C.; Martella, L.A.; Costantini, M.; Mariottini, A.; Andreani, P.; et al. Antimicrobial Stewardship Program, COVID-19, and Infection Control: Spread of Carbapenem-Resistant Klebsiella Pneumoniae Colonization in ICU COVID-19 Patients. What Did Not Work? J. Clin. Med. 2020, 9, 2744. [Google Scholar] [CrossRef]
- WHO Collaborating Center for Drug Statistics Methodology. DDD Definition and General Considerations. 2019. Available online: https://www.whocc.no/ddd/ (accessed on 8 November 2020).
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 10.0. 2020. Available online: www.eucast.org (accessed on 8 November 2020).
- The European Committee on Antimicrobial Susceptibility Testing. EUCAST Guideline for the Detection of Resistance Mechanisms and Specific Resistances of Clinical and/or Epidemiological Importance. Version 2.0. 2017. Available online: www.eucast.org/resistance_mechanisms/ (accessed on 8 November 2020).
- Mattner, F.; Bange, F.C.; Meyer, E.; Seifert, H.; Wichelhaus, T.A.; Chaberny, I.F. Preventing the spread of multidrug-resistant gram-negative pathogens: Recommendations of an expert panel of the German Society for Hygiene and Microbiology. Dtsch. Arztebl. Int. 2012, 109, 39–45. [Google Scholar]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation Tests for Joinpoint Regression with Applications to Cancer Rates. Stat. Med. 2000, 19, 335–351, Correction in 2001, 20, 655. [Google Scholar] [CrossRef]
- Joinpoint Regression Program, Version 4.7.0.0—April 2019; Statistical Methodology and Applications Branch, Surveillance Research Program; National Cancer Institute: Bethesda, MD, USA, 2019.
- Crispo, M.; Barba, M.; Malvezzi, G.; Arpino, M.; Grimaldi, T.; Rosso, E.; Esposito, D.; Sergi, G.; Ciliberto, A.; Giordano, A.; et al. Cancer mortality trends between 1988 and 2009 in the metropolitan area of naples and caserta, southern Italy: Results from a joinpoint regression analysis. Cancer. Biol. Ther. 2013, 14, 1113–1122. [Google Scholar] [CrossRef]
- Wilson, L.; Bhatnagar, P.; Townsend, N. Comparing trends in mortality from cardiovascular disease and cancer in the United Kingdom, 1983–2013: Joinpoint regression analysis. Popul. Health Met. 2017, 15, 23. [Google Scholar] [CrossRef]
- Dyvesether, S.; Nordentoft, M.; Forman, J.; Erlangsen, A. Joinpoint regression analysis of suicides in Denmark during 1980–2015. Danish. Med. J. 2018, 65, A5477. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Time, Weeks | COVID-19 Ward | Non COVID-19 Wards | Difference of Means (95% CI) | p-Value |
|---|---|---|---|---|
| 10–15 | 503.8 ± 362.3 | 848.5 ± 86.0 | 344.6 (−34.5–723.8) | 0.067 |
| 16–20 | 936.0 ± 152.5 | 701.9 ± 56.2 | −234.1 (−420.1–−48.0) | 0.023 |
| 10–20 | 700.3 ± 354.8 | 781.8 ± 104.0 | 81.6 (−162.0–325.1) | 0.479 |
| Outcomes | Baseline | COVID-19 Period | p-Value |
|---|---|---|---|
| ID MDR | 0.33 ± 0.28 | 0.36 ± 0.42 | 0.890 |
| ID total | 1.06 ± 0.49 | 1.10 ± 0.62 | 0.827 |
| CDR on day +14 MDR | 0.06 ± 0.09 | 0.07 ± 0.16 | 0.653 |
| CDR on day +14 total | 0.16 ± 0.14 | 0.13 ± 0.20 | 0.570 |
| CDR on day +30 MDR | 0.08 ± 0.09 | 0.11 ± 0.17 | 0.732 |
| CDR on day +30 total | 0.24 ± 0.17 | 0.26 ± 0.23 | 0.789 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guisado-Gil, A.B.; Infante-Domínguez, C.; Peñalva, G.; Praena, J.; Roca, C.; Navarro-Amuedo, M.D.; Aguilar-Guisado, M.; Espinosa-Aguilera, N.; Poyato-Borrego, M.; Romero-Rodríguez, N.; et al. Impact of the COVID-19 Pandemic on Antimicrobial Consumption and Hospital-Acquired Candidemia and Multidrug-Resistant Bloodstream Infections. Antibiotics 2020, 9, 816. https://doi.org/10.3390/antibiotics9110816
Guisado-Gil AB, Infante-Domínguez C, Peñalva G, Praena J, Roca C, Navarro-Amuedo MD, Aguilar-Guisado M, Espinosa-Aguilera N, Poyato-Borrego M, Romero-Rodríguez N, et al. Impact of the COVID-19 Pandemic on Antimicrobial Consumption and Hospital-Acquired Candidemia and Multidrug-Resistant Bloodstream Infections. Antibiotics. 2020; 9(11):816. https://doi.org/10.3390/antibiotics9110816
Chicago/Turabian StyleGuisado-Gil, Ana Belen, Carmen Infante-Domínguez, Germán Peñalva, Julia Praena, Cristina Roca, María Dolores Navarro-Amuedo, Manuela Aguilar-Guisado, Nuria Espinosa-Aguilera, Manuel Poyato-Borrego, Nieves Romero-Rodríguez, and et al. 2020. "Impact of the COVID-19 Pandemic on Antimicrobial Consumption and Hospital-Acquired Candidemia and Multidrug-Resistant Bloodstream Infections" Antibiotics 9, no. 11: 816. https://doi.org/10.3390/antibiotics9110816
APA StyleGuisado-Gil, A. B., Infante-Domínguez, C., Peñalva, G., Praena, J., Roca, C., Navarro-Amuedo, M. D., Aguilar-Guisado, M., Espinosa-Aguilera, N., Poyato-Borrego, M., Romero-Rodríguez, N., Aldabó, T., Salto-Alejandre, S., Ruiz-Pérez de Pipaón, M., Lepe, J. A., Martín-Gutiérrez, G., Gil-Navarro, M. V., Molina, J., Pachón, J., Cisneros, J. M., & On behalf of the PRIOAM Team. (2020). Impact of the COVID-19 Pandemic on Antimicrobial Consumption and Hospital-Acquired Candidemia and Multidrug-Resistant Bloodstream Infections. Antibiotics, 9(11), 816. https://doi.org/10.3390/antibiotics9110816