1. Introduction
For more than two decades, the safety of fluoroquinolones (FQs) was under investigation. These commonly used antibiotics are now advocated only when no alternatives are available, due to adverse effects, by recent warnings, for common conditions like uncomplicated urinary tract infections (UTIs) and acute bacterial infections of the sinus and bronchi [
1]. Lomefloxacin, sparfloxacin, gatifloxacin, temafloxacin, grepafloxacin, and clenafloxacin were withdrawn from the market due to their fatal side effects [
2,
3]. Since 2008, the United States Food and Drug Administration (US FDA) mandated black-box warnings which were revised over the years. They were kept in place for warning the potential risks of tendinitis, worsening of myasthenia gravis, and peripheral neuropathy.
Even though FQs have great pharmacokinetic properties, there are concerns for human wellbeing. A few unfavourable responses were accounted by FQs in the final phases of clinical trials, and most of these included the skin, musculoskeletal, hepatic, gastrointestinal tract (GIT), and central nervous systems (CNS) [
4]. Modifications in the FQ structure may be responsible for the development of adverse drug reactions (ADRs) such as phototoxicity, prolonged corrected Q-wave to T-wave (QT) interval (QTc), and CNS adverse effects [
5,
6]. FQs are lipoidal in nature, which accounts for their increased affinity in both cartilage and bone. This property can ultimately affect the tendons, muscles, and joints. The possible underlying mechanism for muscle pain and muscle weakness may be cellular apoptosis. The most severe ADRs associated with FQs are tendinitis or tendon rupture, while other reactions include joint pain, myalgia, arthralgia, neck pain, and muscle spasms.
The varying affinity for the γ-aminobutyric acid (GABA) receptor determines the likelihood of seizure occurrence. CNS stimulation, which results from GABA displacement by the FQs from their receptor, can trigger various symptoms, including anxiety, hallucination, paranoia, delirium, tremors, and insomnia [
7]. Warnings were given on the possible dizziness which can occur from ciprofloxacin (CFX) and moxifloxacin (MFX). The development of dizziness was also reported after the levofloxacin (LFX) use [
8,
9,
10]. Other symptoms that can be precipitated due to increased cerebrospinal fluid (CSF) pressure around the brain include headache, lightheadedness, and double vision. Dermatological problems are another frequently reported ADR with FQ use. Symptoms like rash and pruritus can develop even after administration of a single dose of the drug.
In 2004, warning labels of FQs included peripheral neuropathy, which is characterized by numbness, tingling, or pricking sensation [
1]. It is perceived to be caused mainly due to systemic FQs. The symptoms of peripheral neuropathy are usually quick and appear within a couple of days after use, but its identification may be delayed due to its vague clinical manifestation [
11]. In some instances, the adverse effects progressed for over a year, regardless of stopping the medication [
12]. A nested case-control study reported that the use of oral FQs was associated with a higher risk of peripheral neuropathy, which depends on the exposure time and cumulative dose [
13]. A survey on FQ-associated adverse event cases posted online and a case series contributed significantly to the FDA label changes. The survey established a conceivable relationship between FQ use and adverse effects involving the peripheral nervous system (PNS). The latter highlighted that healthy individuals developed delayed reactions after FQ use. These reactions led to severe impairment of multiple organ systems [
14,
15]. Few case reports suggest that FQs such as CFX, LFX, and MFX cause syndrome of inappropriate antidiuretic hormone (SIADH) [
16,
17,
18]. This mechanism is likely to be due to the involvement of GABA and
N-methyl-
d-aspartate (NMDA) receptors, which leads to the increased release of anti-diuretic hormone (ADH), which in turn causes water retention, thereby prompting hyponatremia [
19].
The benefits of FQs showed that these were proved to be useful in both ocular infections and surgical prophylaxis in ophthalmology. However, there were reports of FQs causing eye injury, varying from eye pain to damage to the ocular muscles and retina. Additionally, there were reports on visual impairments. Double vision can occur due to an impairment of coordination between nerves of both eyes and an increase in intraocular pressure [
20].
Nausea and vomiting are the most common gastrointestinal adverse reactions. Similar to other antibiotics, FQs can cause
Clostridium difficile-associated diarrhea (CDAD) due to alteration of the gut’s flora, which ultimately promotes the growth of
Clostridium difficile. Inhibition of potassium channels in the mechanism is mainly responsible for QTc prolongation and arrhythmia. Sparfloxacin and grepafloxacin were removed from the market due to their cardiotoxic properties [
5]. Also, other symptoms that were reported include hepatotoxicity, alteration of blood glucose levels, and renal injury. Recently, the FDA warned against the use of systemic FQs. However, the majority of the studies conducted on FQ safety were from the Western population. Extrapolating Western data in South Asians, especially in Indians, may not be pragmatic. There are differences among regions or even countries in the occurrences of ADRs due to differences in diseases, prescribing practices, genetics, diet and tradition of the people, drug distribution, use indications, dose, availability, and regulatory policies. Similarly, there is a paucity of evidence regarding the disabling adverse effects of FQs in the Asian populace. Almost all antibiotics, including FQs, are easily accessible to the public in India. However, stronger warnings were not implemented regarding their usage. Therefore, this study was designed to investigate the risk of the development of adverse effects following FQ use and to determine whether their route of administration, dose, and duration play a significant role in the development of adverse effects.
3. Discussion
The present study addresses the rarity of data on the safety attributes of FQs in the Indian setting. This is very important as resistance to FQs among various pathogens increased in India, while quinolone consumption is also high and rising in India [
21]. In this study, the incidence of ADRs among FQ users was higher compared to other antibiotics users (8.5 vs. 4.1) and more in the age group of 61–70 years for both groups. A Japan study reported an increased incidence of ADRs among children (<15 years) and elderly people (≥75 years) [
22]. This may be because the mean age of our study population was 50.9 ± 17.8 years. We observed a male predominance in the occurrence of the ADRs among FQs users (78.1%) and other antibiotics users (53.9%), since a majority of the subjects were male (67.4% vs. 63.8%) in both groups. This may be because gender differences exist concerning health-seeking behavior in developing countries, indicating that women utilize formal healthcare to a lesser extent compared to men [
23]. On the other hand, in a study by Lapi et al., females (53.8%) accounted for a more significant portion of the ADRs [
24].
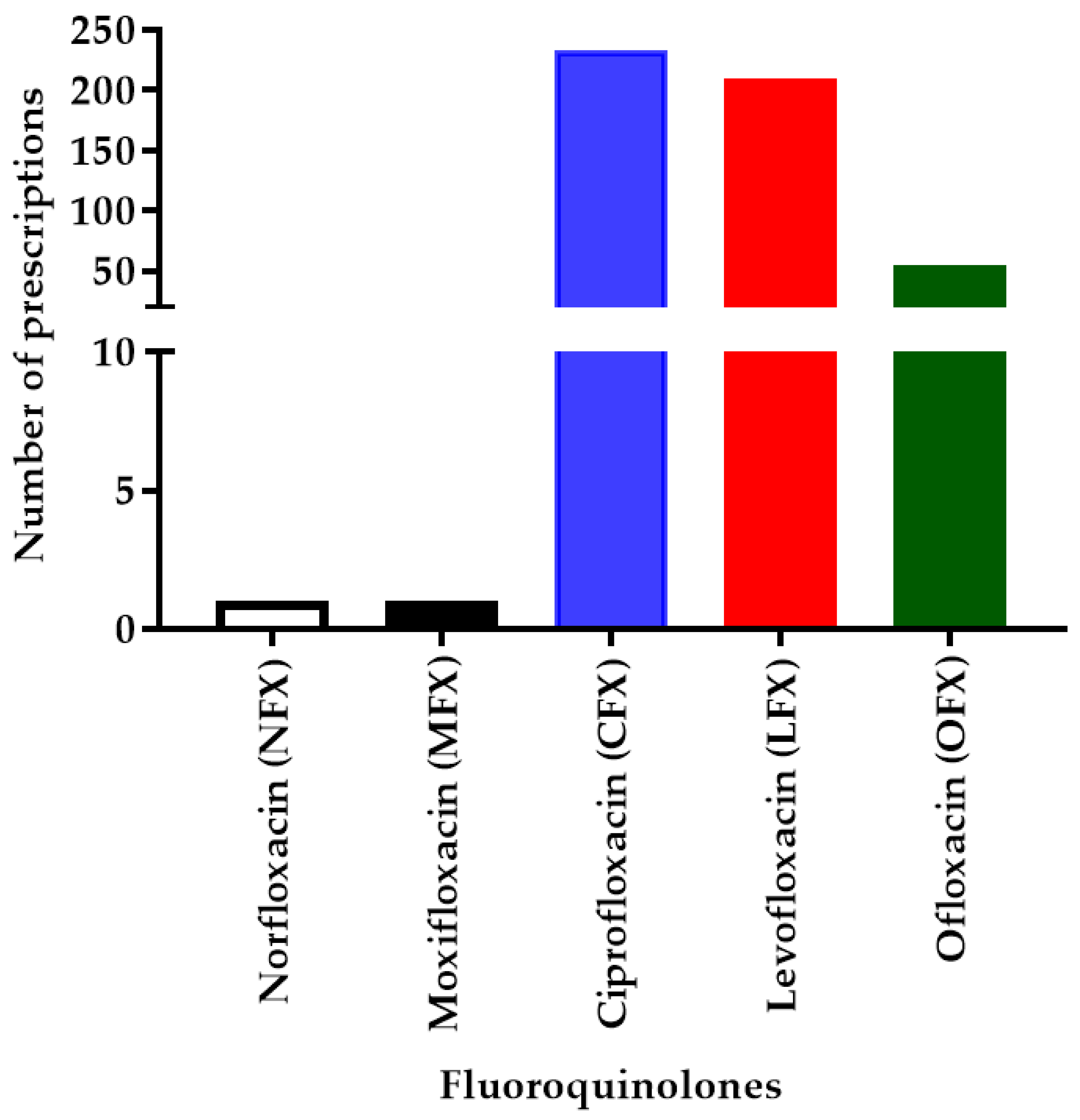
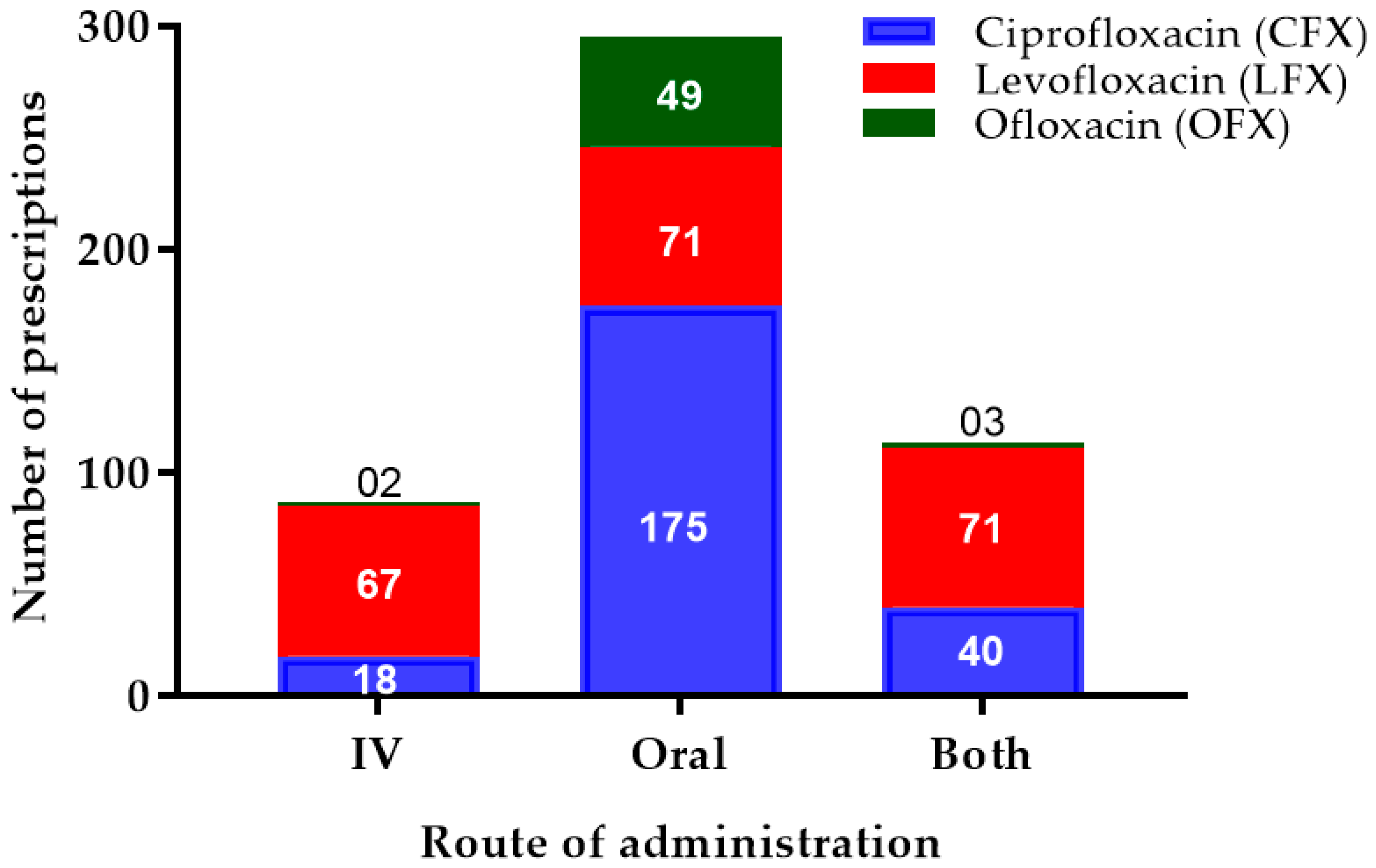
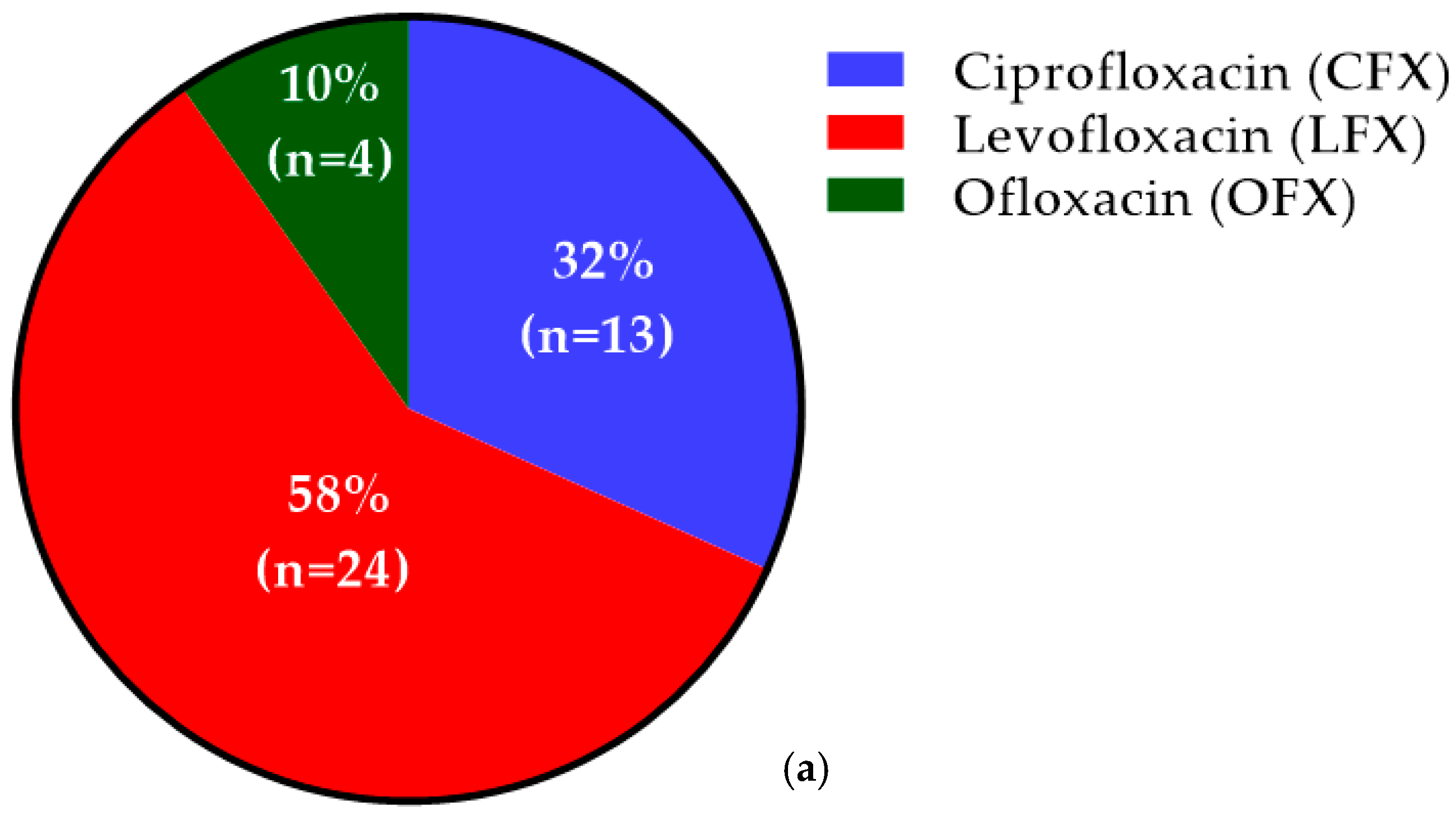
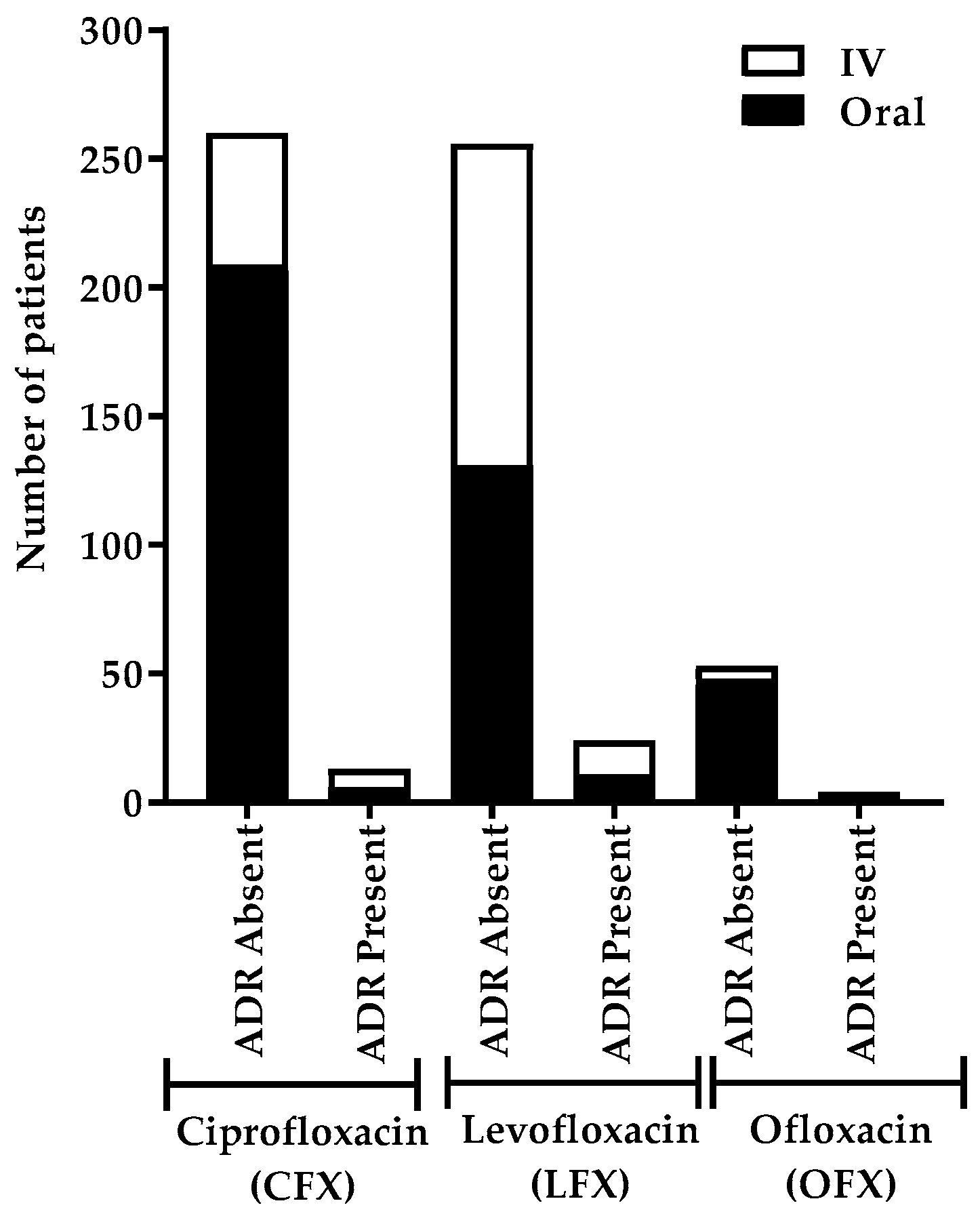
We found that a majority of the ADRs were due to LFX followed by CFX and OFX. This may be due to common ADRs such as nausea, vomiting, and diarrhea, which are mainly associated with LFX. Previous studies by Oreagba et al. and Jose et al. also showed a similar predominance of LFX [
4,
25]. Many FQs are available in IV, as well as formulations, providing flexibility in administration and offering the potential for IV–oral switch, once the patient improves. However, in our findings, the highest number of patients developed ADRs after IV LFX administration. Although the maximum number of ADRs was developed with 500 mg of oral LFX, the highest incidence (75%) of ADR was among high-dose (750 mg) oral LFX users. Piscitelli et al. reported an overall incidence of any ADR as 95% for oral 750-mg LFX-treated patients [
26]. However, there is a paucity of studies that associate the dose of FQs and ADRs [
27].
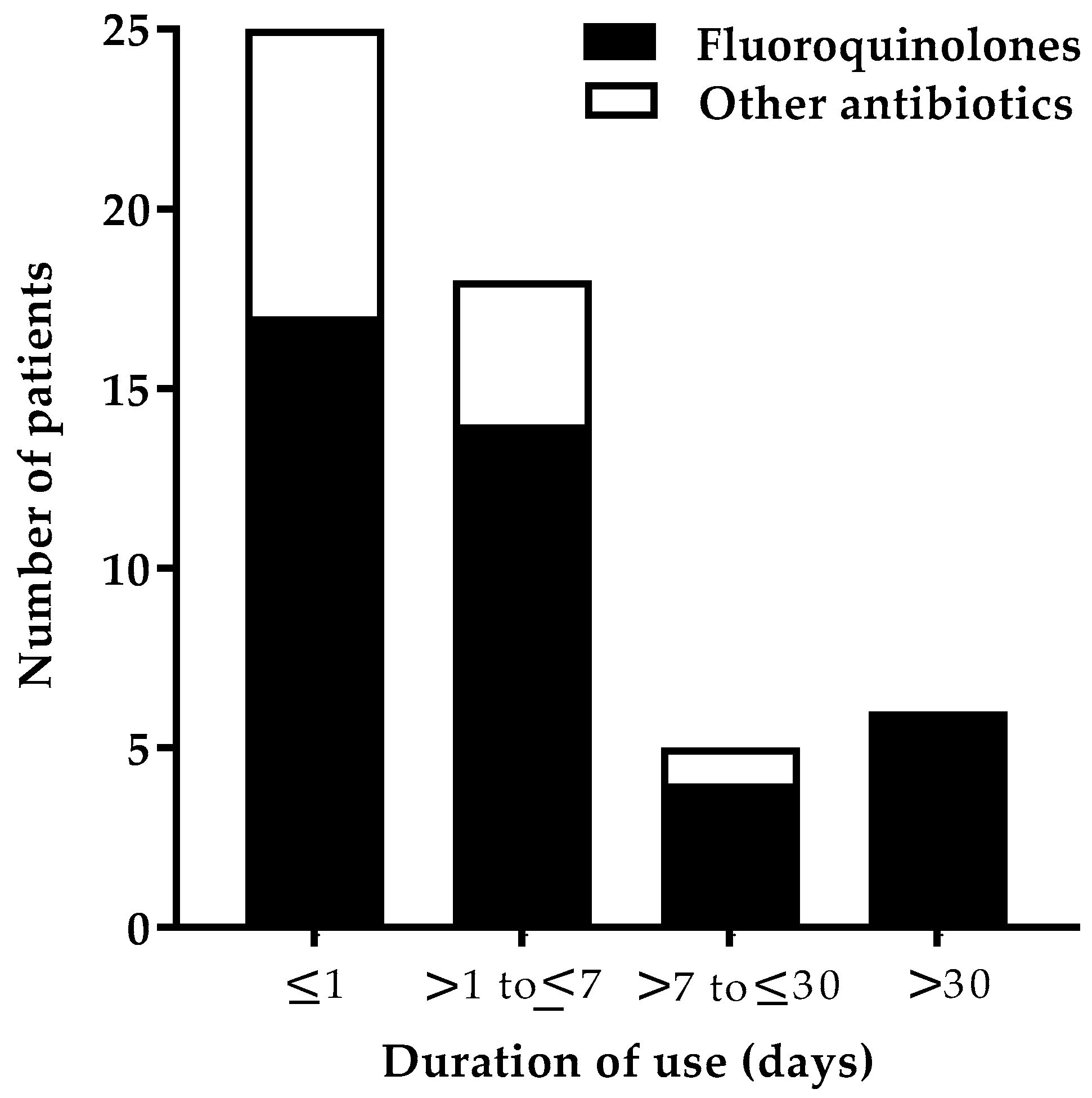
The majority of the ADRs, as a function of the duration of FQ therapy, were found to be ≤1 day (41.5%, 17) and within a week (34.1%, 14). On the contrary, in a study of the Nigerian population, only 13.6% experienced the ADR in <1 day, and the majority of the onset of ADRs (74.5%) was seen within 1–10 days of the start of FQ therapy [
4]. The most common organ systems affected were dermatological and others (each 20.3%) after FQ use. Similarly, in another study, dermatological reactions (25%) were the most reported adverse reactions [
28]. In a study conducted by Jose et al., a higher proportion of reactions was reported to involve the dermatological system than in our study [
20]. CFX was found to be responsible for most skin reactions, as seen in other studies [
28,
29]. Only 6.8% of the patients experienced musculoskeletal adverse effects in our study. There is robust evidence regarding the association between LFX and tendon injury [
15]. Several case reports showed the development of tendinitis following LFX treatment [
30,
31,
32]. The FDA reported that musculoskeletal adverse effects occur in 97% of the cases. This variation in result may be due to differences in the inclusion criteria of the study population.
The percentage of adverse reactions involving the CNS (11.9%) in our study was found to be comparable to the results obtained by Leone et al. (12.2%) [
28]. In this study, CFX (1.7%) was associated with an effect on the PNS. According to a study by Etminan et al., FQs showed a higher risk of causing peripheral neuropathy (relative risk (RR) = 1.83, 95% CI 1.49–2.27) [
33]. A case report published by Francis et al. presented a case with CFX-induced peripheral neuropathy [
11]. The increased reports of neurological-related ADRs to FQs compared to other antibiotics may be due to a periodic warning by the FDA and recent changes in the labeling of the FQ class. Ptosis was seen in one of the patients who was administered with OFX. Jones et al. found an association of FQs with ptosis [
19]. A total of 4.7% (10) of patients who were administered with LFX experienced adverse effect related to the cardiovascular system (CVS), of which five symptoms were related to arrhythmia. A systematic review and meta-analysis by Liu et al. reported that MFX and LFX had a higher chance of causing irregular heartbeat [
34]. In a randomized trial involving elderly patients, MFX (8.3%) and LVX (5.1%) were shown to develop adverse cardiac problems [
35]. A review article by Rubinstein et al. suggested that FQs are safe, although they require surveillance in the presence of any cardiac disease, cardiac drug, or electrolyte imbalance [
5]. A population-based study by Lapi et al. suggested that the use of LFX was safe and MFX, CFX, and gatifloxacin were seen with severe dysrhythmia [
36]. In our study, only one case of nausea (2.4%) was reported, and CFX was responsible for this reaction. According to a study by Chodosh et al., nausea was observed in 27 out of 213 (12.8%) people using CFX [
37].
In our study, hyperglycemia was observed following the use of OFX in a diabetic patient. According to a study by Chou et al., FQs had a higher risk of causing both hyperglycemia and hypoglycemia in diabetic patients [
38]. Warnings of altered blood glucose level were issued on OFX use in patients with an antidiabetic agent [
39]. Of the 28 respiratory tract infection patients treated with FQs, 23 received LFX, and only four received OFX. ADRs were seen only in three patients taking LFX (13%). In a double-blind study, the extent of side effects was slightly higher in patients taking OFX (11.1%) than those taking LFX (6.4%) [
34]. In our study, CFX caused hyponatremia and SIADH in a 58-year-old man, which was similar to the case reported by Mancano et al. [
16]. The author suggested that the elderly were at higher risk (66–73 years). In other case reports, patients developed hyponatremia and SIADH due to MFX and LFX [
17,
18]. The ADRs developed in 17.1% (7) of patients who were concurrently administered with systemic steroids. A report by Khaliq and Zhanel showed that 40 patients who received FQs concurrently with steroids developed tendon rupture [
40]. In another study, the occurrence of tendinitis with concomitant steroid use was reported as 31% [
28].
Using the WHO–UMC criteria scale, the highest number of FQ-related adverse reactions were in the possible (60.9%) category. According to the Naranjo probability scale, the reactions were mainly categorized as probable (60.9%), whereas contrasting results were seen in other studies [
25,
28]. The ADRs reported on FQs use were of moderate (65.9%; 27) severity. According to Oreagba et al., ADRs of mild severity were relatively more frequent than ADRs of moderate severity [
4]. In our study, the incidence of ADRs was observed more among FQs (8.5%) compared to other antibiotics (4.1%). FQ use had a higher risk of causing ADRs as compared to other antibiotics (OR = 2.391, 95% CI: 1.245, 4.592). There is a harmful association between FQ use and development of ADRs (
p = 0.015). Contrasting results were noted from various studies in different tertiary care hospitals across India. Shamna et al. and Jayanthi et al. reported a higher incidence of ADRs using cephalosporin than FQs [
41,
42]. Dhar et al. reported a higher incidence of ADRs with beta-lactams and aminoglycosides [
43].
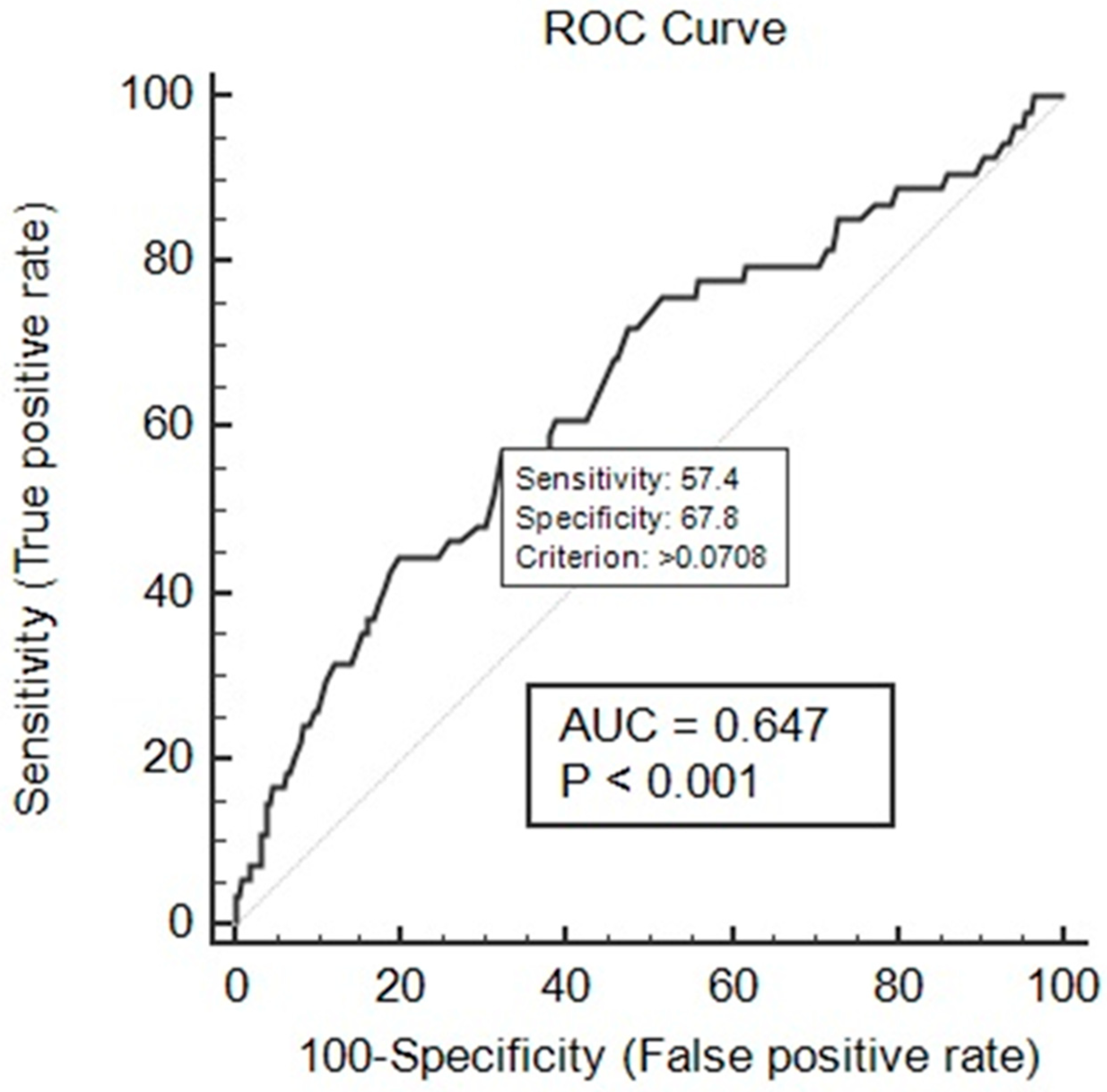
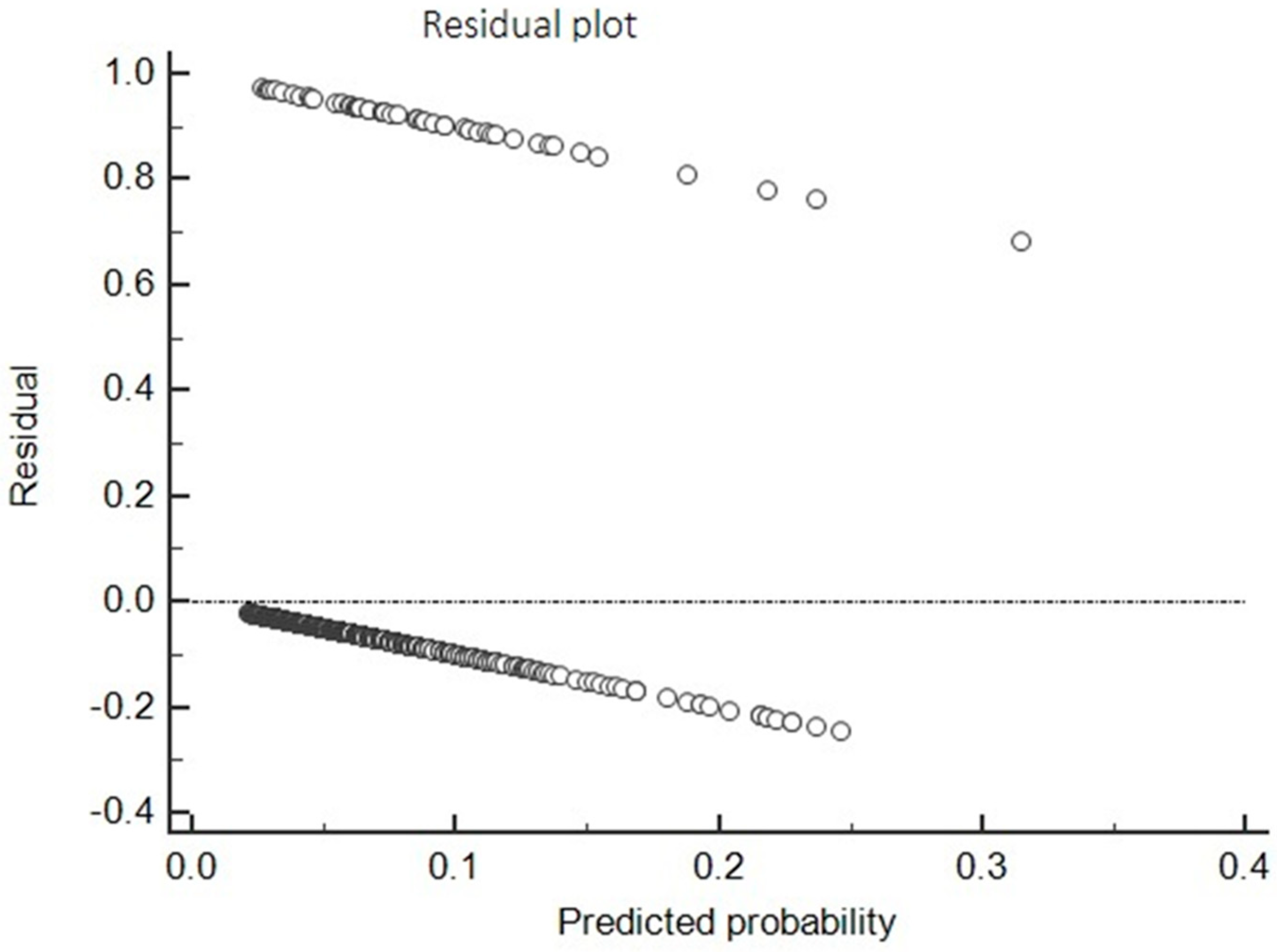
Univariate and multivariate analyses were used to find the association between risk factors and the incidence of ADRs, and adjusted OR was calculated. Based on multiple logistic regression, an ADR prediction model was developed. FQ use and the concomitant use of steroid were independent risk factors, and age was a protective factor for the development of ADRs. The developed model was evaluated using the Hosmer and Lemeshow test, ROC curve, and residual analysis. The developed model showed an acceptable match between predicted ADRs and observed ADRs (chi-square = 8.95; p-value = 0.346). The non-significant p-value for the Hosmer and Lemeshow measure demonstrated that the observed rates were statistically the same across the risk group defined by the test, which shows that the model had a good fit. The ROC curve analysis was performed for predicted probability and occurrences of ADRs. It showed good discriminating power for the developed prediction model of 0.647 at p < 0.001. The residual analysis showed that the model can predict the presence and absence of ADR outcome.
This study highlights the importance of spontaneous reports of adverse effects of FQs. The research made an interesting comparison with other classes of antibiotics in terms of cohort event reporting of ADRs. The observations should encourage healthcare professionals and stakeholders at the institutional and the national levels to conduct periodic antibiotic utilization audits. The findings reveal the necessity of antibiotic stewardship and educational intervention. These are important to optimize FQ prescriptions and for sustainable behavior changes of clinicians toward rational antibiotic use, especially in developing countries. Since this was a retrospective cohort study, the investigators did not have access to other parameters which might influence the development of ADRs. This is one of the major limitations of the study. Apart from this, certain ADRs, especially those of mild severity, may be overlooked due to the retrospective nature of the study design as compared to a prospective study. Moreover, missing information related to adverse events interfere with the causality assessment of ADRs.
4. Materials and Methods
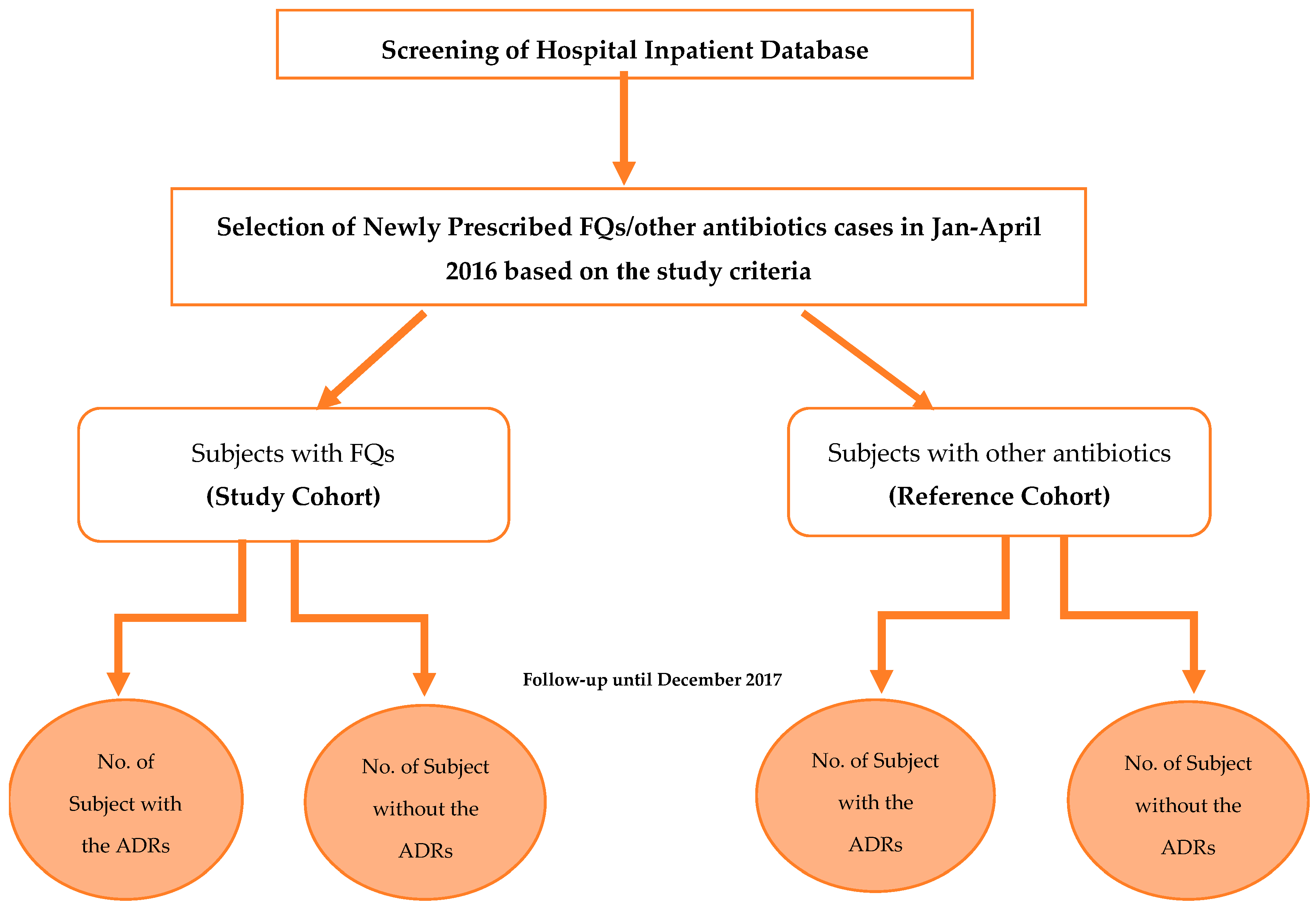
A retrospective cohort study was carried out for seven months (September 2017 to March 2018) in Kasturba Hospital, Manipal, a 2032-bed tertiary care teaching hospital in Udupi District, Karnataka, India. The study was carried out after receiving ethical approval from the Institutional Ethics Committee (IEC) of Kasturba Hospital, Manipal (IEC reference No. 578/2017 dated 13 September 2017). The data collections were carried out following the rules of the Declaration of Helsinki of 1975, revised in 2013. A total of 800 patients admitted in various departments of the hospital from January 2016 to April 2016 were included. These patients were categorized into two cohorts: study cohort (SC) and reference cohort (RC) (
Figure 8). The SC included patients (
n = 482) who were prescribed with FQs, and the RC included patients (
n = 318) who were prescribed with antibiotics other than FQs. In-patients of both genders, irrespective of the age, who were newly prescribed with FQs or other antibiotics for treatment or prophylactic use for infectious diseases, were included. Out-patient cases, those with incomplete medical records, and patients prescribed a combination of FQs or together with other antibiotics were excluded.
Demographical details were recorded along with the clinical symptoms and lab investigations. Details regarding the diagnosis, route of administration, dose, frequency and duration of antibiotics, supportive treatment provided, duration of hospitalization, and ADRs such as symptoms and onset details were collected. Causality assessment for the ADRs was performed by the Naranjo probability scale (definite, probable, possible, or unlikely) and the World Health Organization Collaborating Center for International Drug Monitoring, the Uppsala Monitoring Centre (WHO–UMC) criteria scale (certain, probable/likely, possible, unlikely, unclassified, or unclassifiable). Hartwig’s severity assessment scale was used to classify the severity of reaction into mild (levels 1 and 2), moderate (levels 3, 4a, and 4b), or severe (levels 5, 6, and 7).
4.1. Sample Size
By using the comparison of the proportion method, the sample size was estimated with 80% power and 5% level of significance as 800 consisting of both cohorts.
4.2. Statistical Analysis
Data analysis was performed using the Statistical Package for Social Sciences (IBM SPSS) version 20.0. Cross-tabulation was used to calculate the incidence of ADRs across the different routes of administration, dose, and duration of FQs. Initially, univariate analysis was used to identify the risk factors associated with the incidence of ADRs among the groups. Multiple logistic regression was performed to analyze the association between risk factors and the incidence of ADRs, and to obtain an adjusted odds ratio at 95% CI. A p-value <0.05 was considered statistically significant for all the statistical analysis. The developed multiple logistic regression model was evaluated using the Hosmer and Lemeshow test, ROC curve, and residual analysis. GraphPad Prism version 7.0 was used to generate the graphs.












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}