3.1. Results
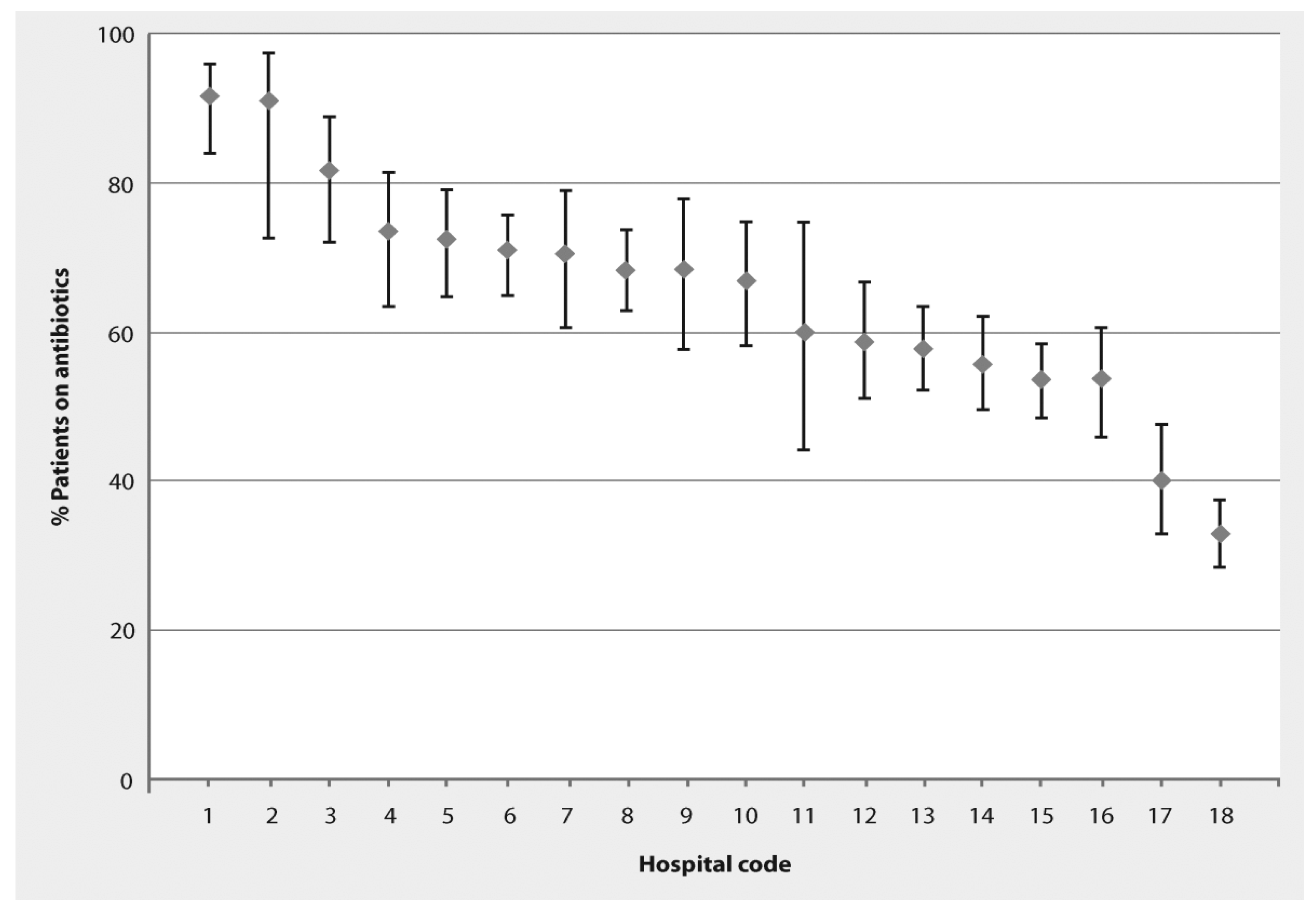
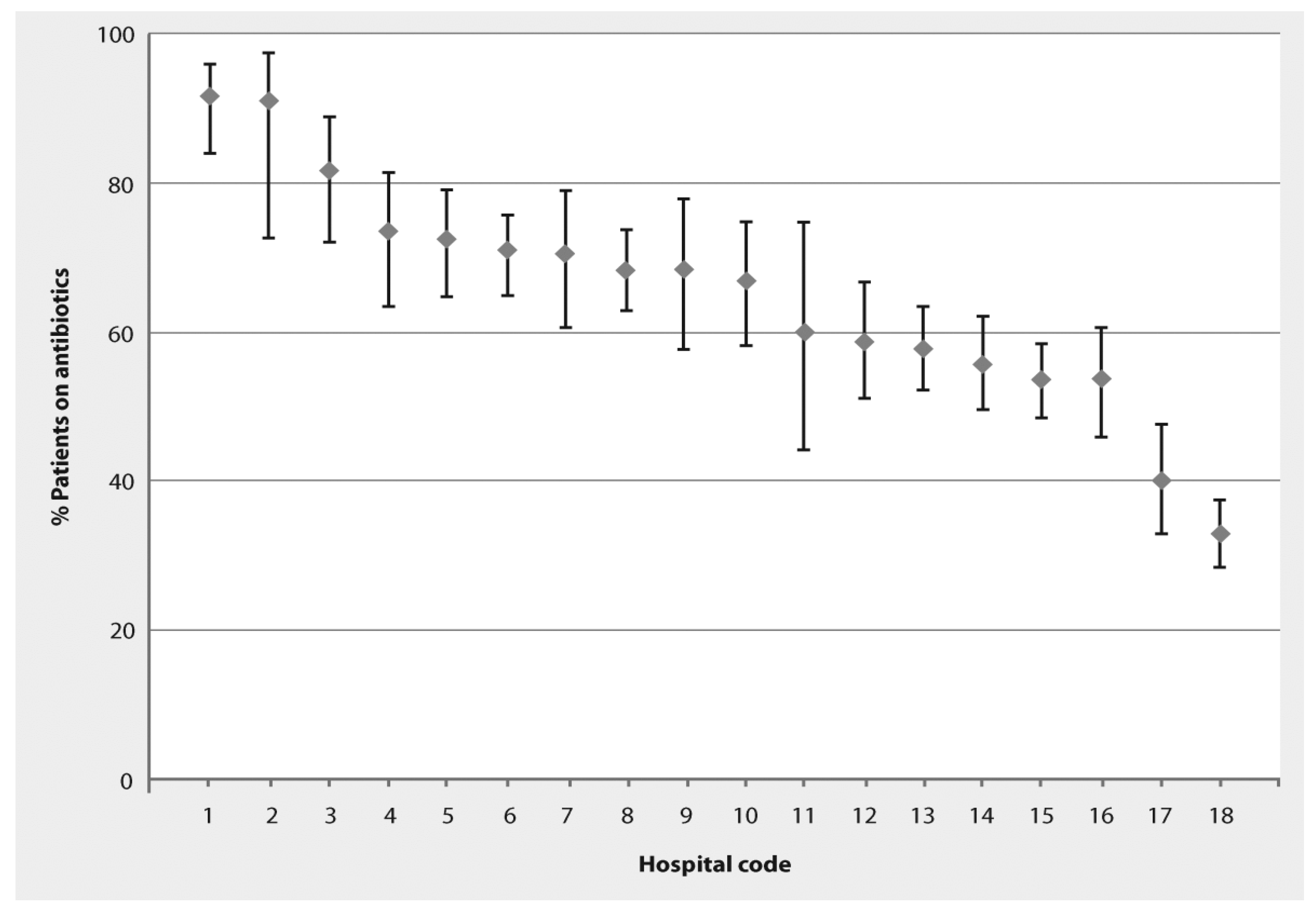
The study was completed during the period March 13–27, 2011. The 18 participating hospitals included five Ministry of Health and 13 university hospitals. Hospitals were classified as general hospitals (11), obstetrics and gynaecology (3), pediatric (2), general surgery (1) and orthopedic (1). The participating hospitals had a total of 7204 beds (mean 400 beds; median 292 beds; range 156–853 beds). Fifty-six intensive care units (39 adult, eight pediatric, and nine neonatal) were present in the 18 hospitals. Six of the hospitals (33%) reported that antibiotic use guidelines were available, but did not present the guidelines when asked for them. On the days of the survey, there were 3408 patients in the participating hospitals. Within the individual hospitals, the number of patients ranged from 23–447. A total of 2017 patients (59%) were receiving one or more antibiotics. The prevalence of antibiotic use in the participating hospitals ranged from 32.9%–91.7% (
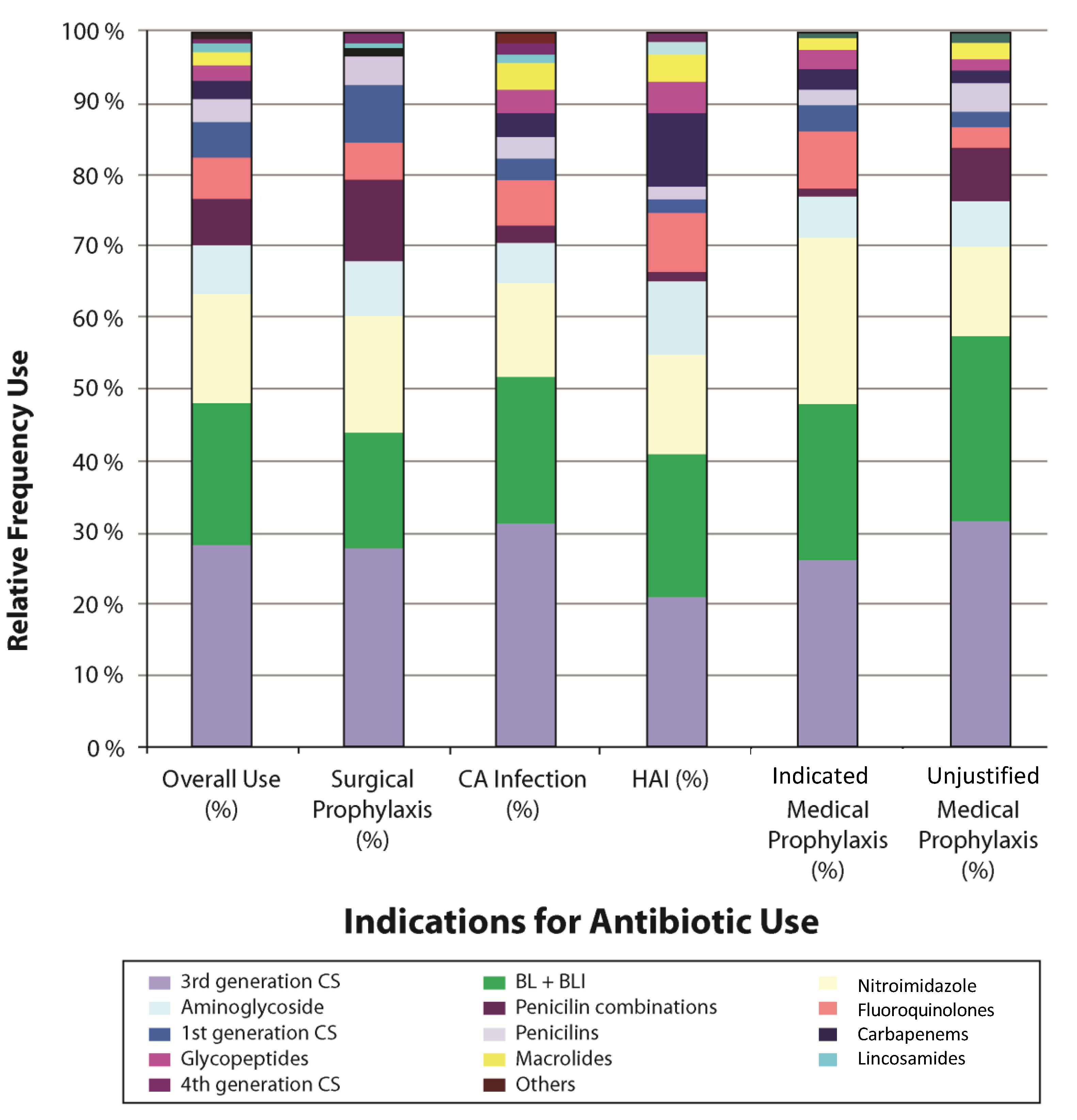
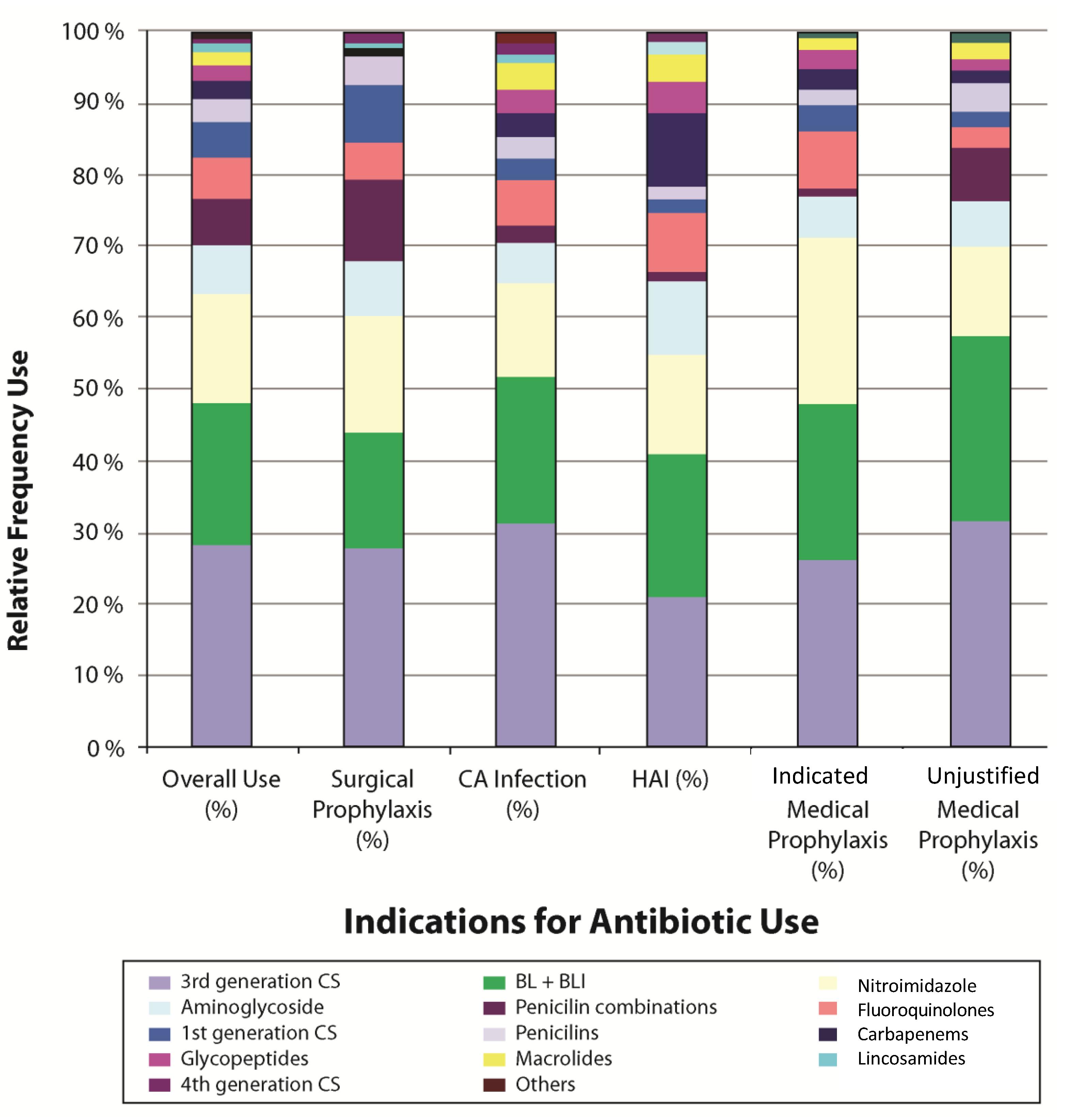
Figure 1). The 2017 treated patients received a total of 3194 antibiotic drugs (1.6 antibiotics per patient). The prevalence of combination therapy, defined as receipt of two or more antibiotics, was 28.4%. As shown in
Figure 2, the most commonly prescribed antibiotics were broad-spectrum agents. Third generation cephalosporins were the most commonly prescribed antibiotics for all indications of antibiotic use, accounting for 28.7% of all antibiotic prescriptions. Penicillins with beta-lactamase inhibitors and mitronidazole derivatives accounted for 19.7% and 15.2%; respectively, and were almost equally prescribed for all indications (
Figure 2).
Figure 1.
Percentage of patients in 18 Egyptian hospitals receiving antibiotics presented as actual measured percentage (diamond) with 95% confidence intervals (vertical lines).
Figure 1.
Percentage of patients in 18 Egyptian hospitals receiving antibiotics presented as actual measured percentage (diamond) with 95% confidence intervals (vertical lines).
The prevalence of antibiotic use was significantly more common among males, younger age groups, and intensive care unit patients (
Table 1). The most common indication for antibiotic use, observed in 38.4% of antibiotic prescriptions, was surgical prophylaxis (
Table 2). Other indications for antibiotic use included treatment of community-acquired infection (27.3%), medical prophylaxis (23%), and treatment of hospital-acquired infection (HAI) (11.3%). The relative frequency of each indication for antibiotic use varied among the different types of hospital locations. For example, the most common indication for antibiotic use among patients on medical wards was treatment of community-acquired infection (43.6%) whereas surgical prophylaxis was the most common indication for antibiotic use on surgical wards (66.5%). In intensive care units, 29.6% of antibiotics were administered for treatment of community-acquired infections and 27.3% were provided for hospital-acquired infections. Differences of antibiotic indications at various hospital locations were statistically significant. Among the 736 antibiotics given for medical prophylaxis, only 291 (39.5%) were given in association with a documented, medically-accepted indication for antibiotic prophylaxis.
Figure 2.
Frequency of use of individual antibiotic classes for prophylaxis and treatment among 3408 patients in 18 Egyptian hospitals—March 2011.
Figure 2.
Frequency of use of individual antibiotic classes for prophylaxis and treatment among 3408 patients in 18 Egyptian hospitals—March 2011.
Others include: Tetracyclins, Sulfonamides, Nitrofurans, antifungals, and second generation cephalosporins Bl + BLI: Drugs that have beta-lactam antibiotics (e.g., Penicillins or Cephalosporins) in addition to beta-lactamase inhibitor agents (sulbactam or clavulanic acid). Penicillin combinations: Drugs that have penicillin antibiotic combination to provide an extended spectrum of efficacy, particularly against penicillin-resistant infections (Ampicillin and cloxacillin combination).
Table 1.
Prevalence of Antibiotic Use in 18 Egyptian Hospitals, March 2011.
Table 1.
Prevalence of Antibiotic Use in 18 Egyptian Hospitals, March 2011.
| Patient Characteristics | Total No. of Patients (n = 3408) | No. of Patients on Antibiotics | Prevalence of Antibiotic use (%) | p-Value |
|---|
| Sex | Male | 1563 | 973 | 62.3 | p < 0.001 |
| | Female | 1845 | 1044 | 56.6 | |
| Age | <5 years | 389 | 313 | 80.5 | p < 0.01 |
| | 5–12 years | 163 | 111 | 68.1 | |
| | >12–65 | 2734 | 1521 | 55.6 | |
| | >65 | 112 | 67 | 59.8 | |
| | Surgical Ward | 1572 | 979 | 62.3 | |
| | Medical Ward | 1409 | 713 | 50.6 | |
Table 2.
Indications for Antibiotic Use Stratified by Type of Hospital Ward.
Table 2.
Indications for Antibiotic Use Stratified by Type of Hospital Ward.
| Indications for Antibiotic Use | Antibiotic Prescriptions (number, (%)) | p-value |
|---|
| Medical wards n = 1127 | Surgical wards n = 1470 | Intensive care units n = 597 | Total n = 3194 |
|---|
| Community-acquired infection | 492 (43.6) | 202 (13.7) | 177 (29.6) | 871 (27.3) | <0.01 |
| Hospital-acquired infection | 117 (10.4) | 82 (5.6) | 163 (27.3) | 362 (11.3) | <0.01 |
| Medical Prophylaxis | | | | | |
| Medically accepted indication for medical prophylaxis | 200 (17.8) | 23 (1.6) | 68 (11.4) | 291 (9.1) | <0.01 |
| Unjustified indication for medical prophylaxis | 149 (13.3) | 186 (12.6) | 110 (18.4) | 445 (13.9) | <0.01 |
| Surgical prophylaxis | 169 (14.9) | 977 (66.5) | 79 (13.2) | 1225 (38.4) | <0.01 |
The most common anatomical sites involved in the prophylactic use of antibiotics were the gynecologic tract (23.9%), gastrointestinal tract (16.3%), and skin, bone, and joints (14.8%) (
Table 3). Among patients receiving antibiotics for treatment of infection, the most common anatomical sites of suspected or proven infection were the respiratory tract (39.2%), gastrointestinal tract (16%), and skin, bone and joints (15.7%) (
Table 3).
Table 3.
Distribution of Antibiotic Treatment and Prophylaxis by Diagnosis.
Table 3.
Distribution of Antibiotic Treatment and Prophylaxis by Diagnosis.
| Diagnosis Group | Antibiotic Use |
|---|
| Total (n = 3194) No. (%) | Prophylaxis (n = 1961) No. (%) | Treatment (n = 1233) No. (%) |
|---|
| Respiratory tract | 597 (18.7) | 114 (5.8) | 483 (39.2) |
| Gastrointestinal tract | 516 (16.2) | 319 (16.3) | 197 (16.0) |
| Gynaecology | 508 (15.9) | 469 (23.9) | 39 (3.2) |
| Skin, Bone & Joint | 484 (15.2) | 290 (14.8) | 194 (15.7) |
| Central nervous system | 232 (7.3) | 188 (9.6) | 44 (3.6) |
| No defined site | 230 (7.2) | 133 (6.7) | 97 (7.8) |
| Cardiovascular system | 217 (6.8) | 174 (8.9) | 43 (3.5) |
| Urinary tract | 151 (4.7) | 59 (3.0) | 92 (7.5) |
| Immunology | 147 (4.6) | 127 (6.5) | 20 (1.6) |
| Eye | 63 (2.0) | 55 (2.8) | 8 (0.65) |
| Ear, nose, and throat | 49 (1.5) | 33 (1.7) | 16 (1.3) |
Out of 1572 patients in the surgery wards, 802 patients (51%) received antibiotics for surgical prophylaxis. Among these 802 patients, 702 (87.5%) had information in their medical charts regarding the start time of the prophylactic antibiotic(s). The duration of antibiotic prophylaxis, however, could be determined for only 333 patients (41.5%) (
Table 4). Out of 702 patients who received surgical prophylaxis, 156 (22.2%) received an antibiotic more than 2 h before the surgical incision, 252 (35.9%) received the antibiotic within two hours prior to the incision, and 294 (41.9%) received the antibiotic after the surgical incision had been made. The percentage of surgical antibiotic prophylaxis courses initiated more than 2 h before the incision varied greatly among the different surgical specialties, ranging from 0%–55.6%, and was highest in the burn and plastic surgery departments. Out of 333 surgeries with a known duration for surgical prophylaxis, 18 (5.4%) were prescribed a single dose of antibiotics, whereas 73.6% of patients were prescribed antibiotics for more than 24 h.
Table 4.
Timing of First Dose and Duration of Surgical Antibiotic Prophylaxis.
Table 4.
Timing of First Dose and Duration of Surgical Antibiotic Prophylaxis.
| Type of surgery | No. of operations with known start time | >2 h before incision No. (%) | ≤2 h before incision No. (%) | After incision No. (%) | No. of operations with known duration of antibiotic prophylaxis | Single dose No. (%) | ≤24 h after incision No. (%) | >24 h after incision No. (%) |
|---|
| Cardiothoracic surgery | 43 | 10 (23.3) | 14 (32.5) | 19 (44.2) | 29 | 0 | 0 | 29 (100) |
| ENT surgery | 28 | 5 (17.9) | 16 (57.1) | 7 (25) | 11 | 0 | 2 (18.2) | 9 (81.8) |
| Burns and plastic surgery | 9 | 5 (55.6) | 1 (11.1) | 3 (33.3) | 2 | 0 | 0 | 2 (100) |
| General surgery | 122 | 37 (30.3) | 35 (28.7) | 50 (41.0) | 67 | 1 (1.5) | 12 (17.9) | 54 (80.6) |
| Neurosurgery | 41 | 12 (29.3) | 2 (4.9) | 27 (65.9) | 4 | 0 | 0 | 4 (100) |
| OB/GYN | 267 | 44 (16.5) | 99 (37.1) | 124 (46.4) | 76 | 11 (14.5) | 49 (64.5) | 16 (21.1) |
| Ophthalmology | 40 | 2 (5.0) | 16 (40.0) | 22 (55.0) | 40 | 2(5.0) | 2(5.0) | 36 (90.0) |
| Orthopedic surgery | 83 | 22 (26.5) | 46 (55.4) | 15 (18.1) | 74 | 4 (5.3) | 5(6.8) | 65 (87.9) |
| Urology | 22 | 4 (18.2) | 8 (36.4) | 10 (45.5) | 11 | 0 | 0 | 11 (100) |
| Vascular surgery | 5 | 0 | 5 (100) | 0 | 6 | 0 | 0 | 6 (100) |
| Other * | 42 | 15 (35.7) | 10 (23.8) | 17 (40.5) | 13 | 0 | 0 | 13 (100) |
| Total | 702 | 156 (22.2) | 252 (35.9) | 294 (41.9) | 333 | 18 (5.4) | 70 (21.0) | 245 (73.6) |
3.2. Discussion
To our knowledge, this is the first large scale assessment of antibiotic use practices outside of North America and Europe. In this project, we applied the same survey method for the assessment of the prevalence of and indications for antibiotic use as that used by the European Surveillance of Antimicrobial Consumption (ESAC) Project [
5] to characterize the use of antibiotic agents in hospitals in Egypt. The ESAC methodology including the time frame and the census of the patients on the day of the survey was applicable and feasible and the data collection tools were simple and easy to use. While the European survey was completed using a web-based format, this study used a paper-based format in order to allow participation by facilities in which access to the internet was limited, or not available. This and other minor modifications may allow this methodology to be used in other countries and regions, including resource-limited areas, in which the prevalence of antibiotic use has not yet been characterized.
This study identified that 59% of patients in the participating Egyptian hospitals were receiving one or more antibiotic agents at the time of survey completion. This is substantially higher than the prevalence of antibiotic use reported in similar studies performed in Europe and the US [
6,
7,
8]. Although the prevalence of antibiotic use was quite variable among participating hospitals, ranging from 32.9%–91.7%, all of the participating hospitals exceeded the 29% prevalence reported in the 2009 ESAC Survey conducted in 172 hospitals representing 29 European countries [
6]. It is important to note that the differences in the prevalence of antibiotic use do not necessarily indicate that there is more inappropriate use of antibiotic agents in Egyptian hospitals. Some of these differences may be due to differences in patient populations or in the prevalence of infectious diseases among hospitalized patients or to the inclusion of a larger proportion of teaching hospitals among our participating hospitals. Our data do suggest, however, that not all of the differences can be attributed to such population differences. In fact, although specific data regarding appropriateness of individual antibiotic prescriptions were not collected, the survey data have identified a number of opportunities for improvement in antibiotic use practices. International antibiotic use guidelines were known to clinicians in only a limited number of hospitals. The translation of such guidelines into active antibiotic use policies could lead to improvements in antibiotic use practices, which could result in reductions in overall antibiotic use and its associated complications within these hospitals.
Evaluation of the specific indications for antibiotic use revealed several specific opportunities for improvement. Surgical prophylaxis was the most common indication for antibiotic administration reported, accounting for 38.4% of all antibiotic prescriptions. A review of the details of surgical prophylaxis prescribing revealed that the selection, timing, and duration of administration were frequently inconsistent with the evidence-based practices recommended in Europe and the US [
9]. For example, the first dose of antibiotic was administered either more than 2 h before incision or after incision in 64% of patients receiving antibiotics for surgical prophylaxis. In addition, 74% of patients received prolonged courses of prophylactic antibiotic therapy (
i.e., more than 24 h). Recent European studies have also demonstrated that prolonged administration of antibiotics for surgical prophylaxis is common. In the 2009 ESAC Survey, surgical antibiotic prophylaxis was administered for >24 h in 53% of patients [
6] whereas this type of prolonged prophylaxis was observed in 21% patients receiving surgical prophylaxis in 38 French hospitals [
8]. Regarding choice of therapy, first-generation cephalosporins, penicillins, and vancomycin accounted for only 12% of all antibiotic agents given for surgical prophylaxis even though these are the recommended agents for a large proportion of surgical procedures. Broad-spectrum agents such as third-generation cephalosporins and beta-lactam plus beta-lactamase inhibitor combinations, on the other hand, accounted for 44% of surgical prophylaxis prescriptions, which might have serious implications on the emergence of multidrug-resistant organisms. Informal discussions with clinicians provided some misconceptions, e.g., prolonging the duration of antibiotic prophylaxis and selecting a broad-spectrum agent for prophylaxis were practices commonly used to reduce the risk of surgical site infections and other healthcare-associated infections in the post-operative period. In response to these findings, a quality improvement project focused on improving surgical site infection prevention practices, including surgical antibiotic prophylaxis, is currently being implemented in several Egyptian hospitals.
We also identified that a large proportion of patients receiving antibiotics for “medical prophylaxis” had no justification of a medically-accepted indication for prophylaxis. This group of patients accounted for 14% of all antibiotic use and 60% of patients who were receiving antibiotic therapy for the purpose of medical prophylaxis. Discussions with clinicians suggested that it was relatively common practice in some of the participating hospitals for patients to be given antibiotics during their hospital stay to reduce the risk of acquiring healthcare-associated infection. This suggests that efforts to strengthen basic infection prevention practices would eventually improve clinicians’ confidence in infection prevention and control program which could result in substantial reductions in the use of antibiotic agents and the associated complications among hospitalized patients.
Although this study provides novel data that will be useful for quality improvement initiatives in individual hospitals and for the Egyptian healthcare system in general, a few limitations should be noted. First, data were collected from only 5% of the hospitals in Egypt. The data may therefore not be representative of antibiotic use in all hospitals throughout the country. In addition, the data were collected from a convenience sample rather than a random sample of Egyptian hospitals. The distribution of hospital types among those that participated in the survey is quite different from the overall distribution of hospital types in Egypt. We sampled approximately 30% of the university hospitals but less than 2.5% of the Ministry of Health hospitals. Finally, although all persons involved in data collection had completed a formal training program prior to participating in the survey, there was no central validation of the submitted data.


{kind=link}
{kind=link}