
Breaking Through Resistance: A Comparative Review of New Beta-Lactamase Inhibitors (Avibactam, Vaborbactam, Relebactam) Against Multidrug-Resistant Superbugs



Abstract
1. Introduction
2. Epidemiological Data
3. Differences Between Newer Inhibitors (Avibactam, Vaborbactam, Relebactam)
3.1. General Management Recommendations
- Suspected or confirmed pathogen—The selection should be guided by local epidemiology and known resistance mechanisms, as well as the presence of carbapenemases.
- Severity and site of infection—The pharmacokinetic/pharmacodynamic (PK/PD) properties of the chosen agent should align with the infection’s anatomical site and severity.
- History of prior MDR infections—A previous infection with an MDR pathogen within the past six months may necessitate a more targeted approach.
- Previous exposure to carbapenems and other antibiotics—Recent treatment with carbapenems, quinolones, or other broad-spectrum antibiotics within the past three months may influence resistance selection and treatment efficacy.
- History of ICU admission—Prior hospitalization in an ICU is a known risk factor for infections caused by carbapenem-resistant organisms.
- Hospital and regional epidemiology—The prevalence of carbapenemase-producing Enterobacterales in the hospital should be factored into empirical antibiotic selection.
- Known colonization with carbapenemase-producing bacteria—Patients with documented colonization may require preemptive adjustments to empiric therapy.
- Recent hospitalization in a ward with carbapenemase-producing outbreaks—Close contact with patients infected or colonized with carbapenemase-producing bacteria increases the likelihood of acquiring a resistant strain.
- Transfer from long-term care facilities or rehabilitation centers—Patients transferred from these settings often have prolonged antibiotic exposure and a higher risk of colonization with MDR pathogens.
- Hospital-acquired septic shock—In cases of septic shock, early and aggressive antimicrobial intervention with broad-spectrum agents, including BLBLIs, is critical for improving patient outcomes.
3.2. Real-Life Clinical Studies of Novel BLBLI Agents
3.2.1. Ceftazidime/Avibactam
3.2.2. Meropenem/Vaborbactam
3.2.3. Imipenem/Cilastatin/Relebactam
3.3. Comparative Efficacy and Key Considerations
3.4. Management Recommendations for MBL-Producing Strains
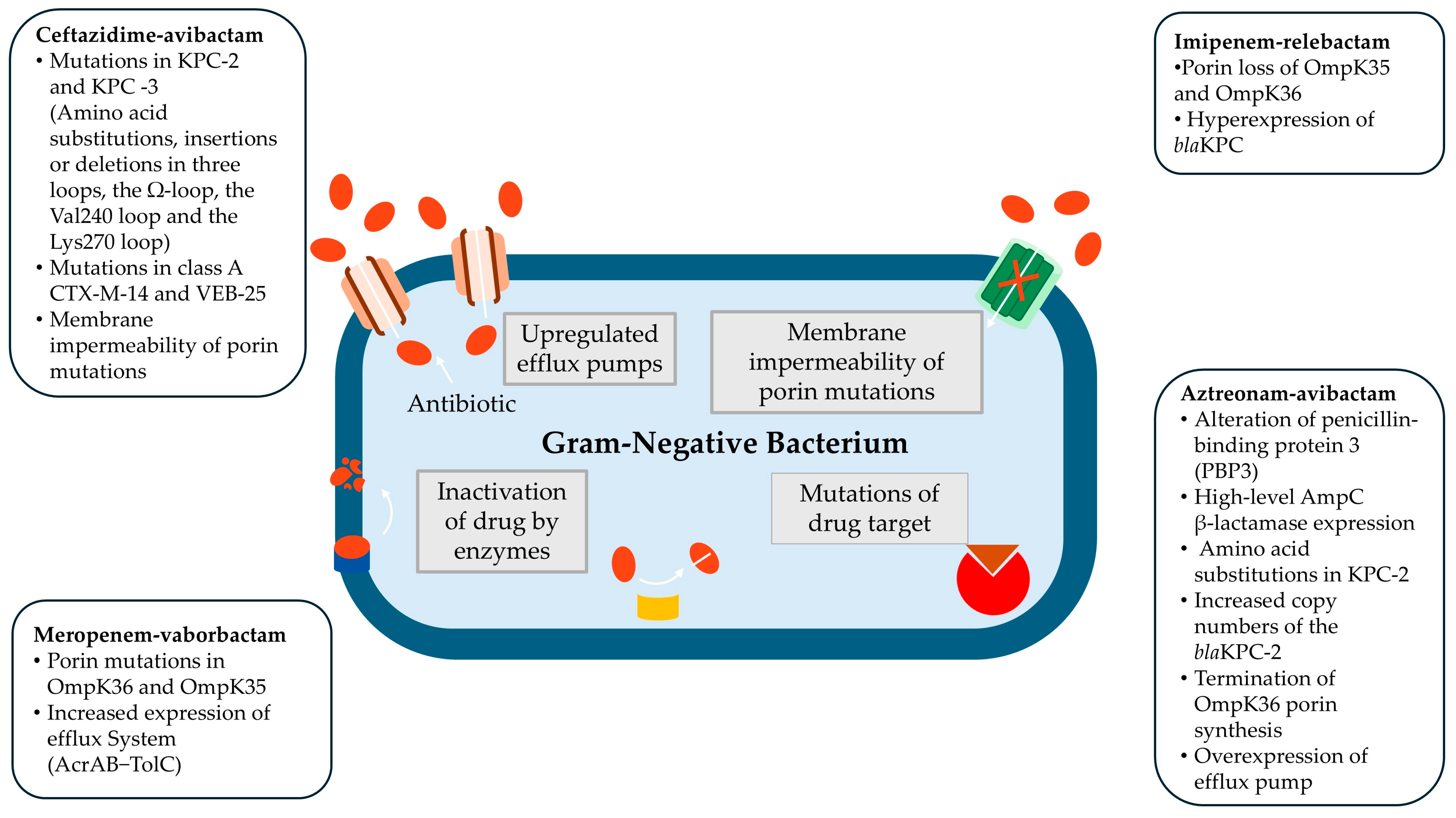
4. Development of Resistance
- Reduced porin expression—Decreased outer membrane permeability limits intracellular drug penetration, reducing the efficacy of β-lactams.
- Increased expression of carbapenemases and/or mutations in β-lactamase enzymes—Enhanced enzymatic activity contributes to β-lactam degradation and resistance development.
- Overexpression of efflux pumps—Increased antibiotic efflux mechanisms lower intracellular drug concentrations, diminishing therapeutic effectiveness.
- A combination of the above mechanisms—The interplay of multiple resistance pathways further compromises the effectiveness of BLBLI therapy, leading to high-level resistance.
4.1. Development of Resistance to Ceftazidime/Avibactam
4.2. Development of Resistance to Meropenem/Vaborbactam and Imipenem/Cilastatin/Relebactam
4.3. Development of Resistance to Aztreonam/Avibactam
4.4. Risk Factors for Treatment Failures and Resistance
5. Laboratory Management of New BLBLI Agents
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AmpC | AmpC β-lactamase |
| AMR | Antimicrobial Resistance |
| ATM-AVI | Aztreonam/Avibactam |
| BSI | Bloodstream Infection |
| BLBLI | β-lactam–β-lactamase Inhibitor |
| CAZ-AVI | Ceftazidime/Avibactam |
| cIAI | Complicated Intra-abdominal Infection |
| CrCl | Creatinine Clearance |
| CRE | Carbapenem-Resistant Enterobacterales |
| CRRT | Continuous Renal Replacement Therapy |
| CPE | Carbapenemase-producing Enterobacterales |
| CVVH | Continuous Veno-Venous Hemofiltration |
| CVVHDF | Continuous Veno-Venous Hemodiafiltration |
| DBO | Diazabicycloocatane |
| DTR | Difficult-to-Treat Resistant |
| ELF | Epithelial Lining Fluid |
| ESBL | Extended-Spectrum β-Lactamase |
| EU/EAA | European Union/European Economic Area |
| GES | Guiana extended-spectrum β-lactamase |
| ICU | Intensive Care Unit |
| IMI-REL | Imipenem/Cilastatin/Relebactam |
| KPC | Klebsiella pneumoniae Carbapenemase |
| MBL | Metallo-β-lactamase |
| MDR | Multidrug-Resistant |
| MER-VAB | Meropenem/Vaborbactam |
| MIC | Minimum Inhibitory Concentration |
| NDM | New Delhi Metallo-β-lactamase |
| OXA | Oxacillinase (OXA-48-like) |
| PK/PD | Pharmacokinetics/Pharmacodynamics |
| RRT | Renal Replacement Therapy |
| VIM | Verona Integron-encoded Metallo-β-lactamase |
References
- Jean, S.S.; Harnod, D.; Hsueh, P.R. Global Threat of Carbapenem-Resistant Gram-Negative Bacteria. Front. Cell. Infect. Microbiol. 2022, 12, 823684. [Google Scholar] [CrossRef]
- ECDC. Antimicrobial Resistance in the EU/EEA (EARS-Net) Annual Epidemiological Report for 2023. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/antimicrobial-resistance-annual-epidemiological-report-EARS-Net-2023.pdf (accessed on 30 April 2025).
- Karaiskos, I.; Lagou, S.; Pontikis, K.; Rapti, V.; Poulakou, G. The “Old” and the “New” Antibiotics for MDR Gram-Negative Pathogens: For Whom, When, and How. Front. Public Health 2019, 7, 151. [Google Scholar] [CrossRef] [PubMed]
- Karaiskos, I.; Galani, I.; Souli, M.; Giamarellou, H. Novel β-lactam-β-lactamase inhibitor combinations: Expectations for the treatment of carbapenem-resistant Gram-negative pathogens. Expert. Opin. Drug Metab. Toxicol. 2019, 15, 133–149. [Google Scholar] [CrossRef]
- Tumbarello, M.; Raffaelli, F.; Giannella, M.; Mantengoli, E.; Mularoni, A.; Venditti, M.; De Rosa, F.G.; Sarmati, L.; Bassetti, M.; Brindicci, G.; et al. Ceftazidime-Avibactam Use for Klebsiella pneumoniae Carbapenemase-Producing K. pneumoniae Infections: A Retrospective Observational Multicenter Study. Clin. Infect. Dis. 2021, 73, 1664–1676. [Google Scholar] [CrossRef] [PubMed]
- Karaiskos, I.; Daikos, G.L.; Gkoufa, A.; Adamis, G.; Stefos, A.; Symbardi, S.; Chrysos, G.; Filiou, E.; Basoulis, D.; Mouloudi, E.; et al. Ceftazidime/avibactam in the era of carbapenemase-producing Klebsiella pneumoniae: Experience from a national registry study. J. Antimicrob. Chemother. 2021, 76, 775–778. [Google Scholar] [CrossRef] [PubMed]
- Tiseo, G.; Galfo, V.; Riccardi, N.; Suardi, L.R.; Pogliaghi, M.; Giordano, C.; Leonildi, A.; Barnini, S.; Falcone, M. Real-world experience with meropenem/vaborbactam for the treatment of infections caused by ESBL-producing Enterobacterales and carbapenem-resistant Klebsiella pneumoniae. Eur. J. Clin. Microbiol. Infect. Dis, 2024; online ahead of print. [Google Scholar] [CrossRef]
- Machuca, I.; Dominguez, A.; Amaya, R.; Arjona, C.; Gracia-Ahufinger, I.; Carralon, M.; Giron, R.; Gea, I.; De Benito, N.; Martin, A.; et al. Real-World Experience of Imipenem-Relebactam Treatment as Salvage Therapy in Difficult-to-Treat Pseudomonas aeruginosa Infections (IMRECOR Study). Infect. Dis. Ther. 2025, 14, 283–292. [Google Scholar] [CrossRef]
- Li, J.; Shi, Y.; Song, X.; Yin, X.; Liu, H. Mechanisms of Antimicrobial Resistance in Klebsiella: Advances in Detection Methods and Clinical Implications. Infect. Drug Resist. 2025, 18, 1339–1354. [Google Scholar] [CrossRef]
- Grabein, B.; Arhin, F.F.; Daikos, G.L.; Moore, L.S.P.; Balaji, V.; Baillon-Plot, N. Navigating the Current Treatment Landscape of Metallo-β-Lactamase-Producing Gram-Negative Infections: What are the Limitations? Infect. Dis. Ther. 2024, 13, 2423–2447. [Google Scholar] [CrossRef]
- Giamarellou, H.; Galani, L.; Karavasilis, T.; Ioannidis, K.; Karaiskos, I. Antimicrobial Stewardship in the Hospital Setting: A Narrative Review. Antibiotics 2023, 12, 1557. [Google Scholar] [CrossRef]
- ECDC. Rapid Risk Assessment—Carbapenem-Resistant Enterobacterales—Third Update. 2025. Available online: https://www.ecdc.europa.eu/en/publications-data/carbapenem-resistant-enterobacterales-rapid-risk-assessment-third-update (accessed on 30 April 2025).
- Budia-Silva, M.; Kostyanev, T.; Ayala-Montaño, S.; Bravo-Ferrer Acosta, J.; Garcia-Castillo, M.; Cantón, R.; Goossens, H.; Rodriguez-Baño, J.; Grundmann, H.; Reuter, S. International and regional spread of carbapenem-resistant Klebsiella pneumoniae in Europe. Nat. Commun. 2024, 15, 5092. [Google Scholar] [CrossRef]
- Boyd, S.E.; Holmes, A.; Peck, R.; Livermore, D.M.; Hope, W. OXA-48-Like β-Lactamases: Global Epidemiology, Treatment Options, and Development Pipeline. Antimicrob. Agents Chemother. 2022, 66, e0021622. [Google Scholar] [CrossRef]
- ECDC. Regional Outbreak of New Delhi Metallo-Beta-Lactamase-Producing Carbapenem-Resistant Enterobacteriaceae, Italy, 2018–2019. 2019. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/04-Jun-2019-RRA-Carbapenems%2C%20Enterobacteriaceae-Italy.pdf (accessed on 30 April 2025).
- Whonet Greece. Greek System for the Surveillance of Antimicrobial Resistance. July—December 2023. Available online: https://www.mednet.gr/whonet/ (accessed on 30 April 2025).
- Galani, I.; Karaiskos, I.; Karantani, I.; Papoutsaki, V.; Maraki, S.; Papaioannou, V.; Kazila, P.; Tsorlini, H.; Charalampaki, N.; Toutouza, M.; et al. Epidemiology and resistance phenotypes of carbapenemase-producing Klebsiella pneumoniae in Greece, 2014 to 2016. Eurosurveillance 2018, 23, 31. [Google Scholar] [CrossRef] [PubMed]
- Maraki, S.; Mavromanolaki, V.E.; Stafylaki, D.; Scoulica, E. In vitro activity of newer β-lactam/β-lactamase inhibitor combinations, cefiderocol, plazomicin and comparators against carbapenemase-producing Klebsiella pneumoniae isolates. J. Chemother. 2023, 35, 596–600. [Google Scholar] [CrossRef] [PubMed]
- Tryfinopoulou, K.; Linkevicius, M.; Pappa, O.; Alm, E.; Karadimas, K.; Svartström, O.; Polemis, M.; Mellou, K.; Maragkos, A.; Brolund, A.; et al. Greek CCRE study group, & Members of the Greek CCRE study group. Emergence and persistent spread of carbapenemase-producing Klebsiella pneumoniae high-risk clones in Greek hospitals, 2013 to 2022. Eurosurveillance 2023, 28, 2300571. [Google Scholar] [PubMed]
- Galani, I.; Souli, M.; Nafplioti, K.; Adamou, P.; Karaiskos, I.; Giamarellou, H.; Antoniadou, A. In vitro activity of imipenem-relebactam against non-MBL carbapenemase-producing Klebsiella pneumoniae isolated in Greek hospitals in 2015–2016. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1143–1150. [Google Scholar] [CrossRef]
- Yahav, D.; Giske, C.G.; Grāmatniece, A.; Abodakpi, H.; Tam, V.H.; Leibovici, L. New β-Lactam-β-Lactamase Inhibitor Combinations. Clin. Microbiol. Rev. 2020, 34, e00115-20. [Google Scholar] [CrossRef]
- Zhou, H.; Buetti, N.; Pérez-Galera, S.; Bravo-Ferrer, J.; Gutiérrez-Gutiérrez, B.; Paniagua-García, M.; Feifel, J.; Sauser, J.; Kostyanev, T.; Canton, R.; et al. Risk factors for bloodstream infections due to carbapenem-resistant Enterobacterales: A nested case-control-control study. J. Antimicrob. Chemother. 2024, 79, 2132–2141. [Google Scholar] [CrossRef]
- Pérez-Galera, S.; Bravo-Ferrer, J.M.; Paniagua, M.; Kostyanev, T.; de Kraker, M.E.A.; Feifel, J.; Sojo-Dorado, J.; Schotsman, J.; Cantón, R.; Daikos, G.L.; et al. Risk factors for infections caused by carbapenem-resistant Enterobacterales: An international matched case-control-control study (EURECA). eClinicalMedicine 2023, 57, 101871. [Google Scholar] [CrossRef]
- Tamma, P.D.; Heil, E.L.; Justo, J.A.; Mathers, A.J.; Satlin, M.J.; Bonomo, R.A. Infectious Diseases Society of America 2024 Guidance on the Treatment of Antimicrobial-Resistant Gram-Negative Infections. Clin. Infect. Dis, 2024; online ahead of print. [Google Scholar] [CrossRef]
- Shields, R.K. Emerging β-lactamases in Pseudomonas aeruginosa that threaten the utility of new β-Lactam/β-Lactamase inhibitors. Contagion 2023, 5, 20–21. [Google Scholar]
- Galani, I.; Papoutsaki, V.; Karantani, I.; Karaiskos, I.; Galani, L.; Adamou, P.; Deliolanis, I.; Kodonaki, A.; Papadogeorgaki, E.; Markopoulou, M.; et al. In vitro activity of ceftolozane/tazobactam alone and in combination with amikacin against MDR/XDR Pseudomonas aeruginosa isolates from Greece. J. Antimicrob. Chemother. 2020, 75, 2164–2172. [Google Scholar] [CrossRef]
- Zavicefta. Ceftazidime-Avibactam—Summary of Product Characteristics. 2021. Available online: https://www.ema.europa.eu/en/documents/product-information/zavicefta-epar-product-information_en.pdf (accessed on 30 April 2025).
- Vaborem. Meropenem-Vaborbactam—Summary of Product Characteristics. 2023. Available online: https://www.ema.europa.eu/en/documents/product-information/vaborem-epar-product-information_en.pdf (accessed on 30 April 2025).
- Recarbio. Imipenem-Cilastatin-Relebactam—Summary of Product Characteristics. 2020. Available online: https://ec.europa.eu/health/documents/community-register/2020/20201116149798/anx_149798_en.pdf (accessed on 30 April 2025).
- Emblavio. Aztreonam-Avibactam—Summary of Products Characteristics. 2025. Available online: https://ec.europa.eu/health/documents/community-register/2024/20240422162367/anx_162367_en.pdf (accessed on 30 April 2025).
- Tsolaki, V.; Mantzarlis, K.; Mpakalis, A.; Malli, E.; Tsimpoukas, F.; Tsirogianni, A.; Papagiannitsis, C.; Zygoulis, P.; Papadonta, M.E.; Petinaki, E.; et al. Ceftazidime-Avibactam To Treat Life-Threatening Infections by Carbapenem-Resistant Pathogens in Critically Ill Mechanically Ventilated Patients. Antimicrob. Agents Chemother. 2020, 64, e02320-19. [Google Scholar] [CrossRef] [PubMed]
- Castón, J.J.; Cano, A.; Pérez-Camacho, I.; Aguado, J.M.; Carratalá, J.; Ramasco, F.; Soriano, A.; Pintado, V.; Castelo-Corral, L.; Sousa, A.; et al. Impact of ceftazidime/avibactam versus best available therapy on mortality from infections caused by carbapenemase-producing Enterobacterales (CAVICOR study). J. Antimicrob. Chemother. 2022, 77, 1452–1460. [Google Scholar] [CrossRef]
- Shields, R.K.; Nguyen, M.H.; Chen, L.; Press, E.G.; Potoski, B.A.; Marini, R.V.; Doi, Y.; Kreiswirth, B.N.; Clancy, C.J. Ceftazidime-Avibactam is superior to other treatment regimens against carbapenem-resistant Klebsiella pneumoniae bacteremia. Antimicrob. Agents Chemother. 2017, 61, e00883-17. [Google Scholar] [CrossRef]
- Van Duin, D.; Lok, J.J.; Earley, M.; Cober, E.; Richter, S.S.; Perez, F.; Salata, R.A.; Kalayjian, R.C.; Watkins, R.R.; Doi, Y.; et al. Colistin Versus Ceftazidime-Avibactam in the Treatment of Infections Due to Carbapenem-Resistant Enterobacteriaceae. Clin. Infect. Dis. 2018, 66, 163–171. [Google Scholar] [CrossRef]
- Shields, R.K.; Horcajada, J.P.; Kamat, S.; Irani, P.M.; Tawadrous, M.; Welte, T. Ceftazidime-Avibactam in the Treatment of Patients with Bacteremia or Nosocomial Pneumonia: A Systematic Review and Meta-analysis. Infect. Dis. Ther. 2024, 13, 1639–1664. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; Marelli, C.; Cattardico, G.; Fanelli, C.; Signori, A.; Di Meco, G.; Di Pilato, V.; Mikulska, M.; Mazzitelli, M.; Cattelan, A.M.; et al. Mortality in KPC-producing Klebsiella pneumoniae bloodstream infections: A changing landscape. J. Antimicrob. Chemother. 2023, 78, 2505–2514. [Google Scholar] [CrossRef]
- Falcone, M.; Tiseo, G.; Carbonara, S.; Marino, A.; Di Caprio, G.; Carretta, A.; Mularoni, A.; Mariani, M.F.; Maraolo, A.E.; Scotto, R.; et al. Mortality Attributable to Bloodstream Infections Caused by Different Carbapenem-Resistant Gram-Negative Bacilli: Results From a Nationwide Study in Italy (ALARICO Network). Clin. Infect. Dis. 2023, 76, 2059–2069. [Google Scholar] [CrossRef]
- Shields, R.K.; McCreary, E.K.; Marini, R.V.; Kline, E.G.; Jones, C.E.; Hao, B.; Chen, L.; Kreiswirth, B.N.; Doi, Y.; Clancy, C.J.; et al. Early Experience with Meropenem-Vaborbactam for Treatment of Carbapenem-resistant Enterobacteriaceae Infections. Clin. Infect. Dis. 2020, 71, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Alosaimy, S.; Lagnf, A.M.; Morrisette, T.; Scipione, M.R.; Zhao, J.J.; Jorgensen, S.C.J.; Mynatt, R.; Carlson, T.J.; Jo, J.; Garey, K.W.; et al. Real-world, Multicenter Experience with Meropenem-Vaborbactam for Gram-Negative Bacterial Infections Including Carbapenem-Resistant Enterobacterales and Pseudomonas aeruginosa. Open Forum Infect. Dis. 2021, 8, ofab371. [Google Scholar] [CrossRef]
- Zhang, H.L.; Cressman, L.; Lautenbach, E. Real-world clinical outcomes of meropenem/vaborbactam for treatment of carbapenem-resistant Enterobacterales infections. J. Glob. Antimicrob. Resist. 2021, 27, 299–302. [Google Scholar] [CrossRef]
- Tumbarello, M.; Raffaelli, F.; Cascio, A.; Falcone, M.; Signorini, L.; Mussini, C.; De Rosa, F.G.; Losito, A.R.; De Pascale, G.; Pascale, R.; et al. Compassionate use of meropenem/vaborbactam for infections caused by KPC-producing Klebsiella pneumoniae: A multicentre study. JAC Antimicrob. Resist. 2022, 4, dlac022. [Google Scholar] [CrossRef] [PubMed]
- Tumbarello, M.; Raffaelli, F.; Giannella, M.; De Pascale, G.; Cascio, A.; De Rosa, F.G.; Cattelan, A.M.; Oliva, A.; Saracino, A.; Bassetti, M.; et al. Outcomes and Predictors of Mortality in Patients with KPC-Kp Infections Treated with Meropenem Vaborbactam: An Observational Multicenter Study. Open Forum Infect. Dis. 2024, 11, ofae273. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Giacobbe, D.R.; Vena, A.; Poulakou, G.; Rossolini, G.M.; Soriano, A.; Nicolau, D.P. Meropenem-Vaborbactam for Treatment of Carbapenem-Resistant Enterobacterales: A Narrative Review of Clinical Practice Evidence. Infect. Dis. Ther, 2025; online ahead of print. [Google Scholar] [CrossRef]
- Leanza, C.; Mascellino, M.T.; Volpicelli, L.; Covino, S.; Falletta, A.; Cancelli, F.; Franchi, C.; Carnevalini, M.; Mastroianni, C.M.; Oliva, A. Real-world use of imipenem/cilastatin/relebactam for the treatment of KPC-producing Klebsiella pneumoniae complex and difficult-to-treat resistance (DTR) Pseudomonas aeruginosa infections: A single-center preliminary experience. Front. Microbiol. 2024, 15, 1432296. [Google Scholar] [CrossRef] [PubMed]
- Rebold, N.; Morrisette, T.; Lagnf, A.M.; Alosaimy, S.; Holger, D.; Barber, K.; Justo, J.A.; Antosz, K.; Carlson, T.J.; Frens, J.J.; et al. Early Multicenter Experience with Imipenem-Cilastatin-Relebactam for Multidrug-Resistant Gram-Negative Infections. Open Forum Infect. Dis. 2021, 8, ofab554. [Google Scholar] [CrossRef]
- Caniff, K.E.; Rebold, N.; Xhemali, X.; Tran, N.; Eubank, T.A.; Garey, K.W.; Guo, Y.; Chang, M.; Barber, K.E.; Krekel, T.; et al. Real-World Applications of Imipenem-Cilastatin-Relebactam: Insights From a Multicenter Observational Cohort Study. Open Forum Infect. Dis. 2025, 12, ofaf112. [Google Scholar] [CrossRef]
- Shields, R.K. Is There a Preferred β-Lactam/β-Lactamase Inhibitor Agent for Treatment of KPC-Producing Enterobacterales Infection? Contagion 2023, 8, 16–17. [Google Scholar]
- Ackley, R.; Roshdy, D.; Meredith, J.; Minor, S.; Anderson, W.E.; Capraro, G.A.; Polk, C. Meropenem-Vaborbactam versus Ceftazidime-Avibactam for Treatment of Carbapenem-Resistant Enterobacteriaceae Infections. Antimicrob. Agents Chemother. 2020, 64, e02313-19. [Google Scholar] [CrossRef]
- Zilberberg, M.D.; Nathanson, B.H.; Redell, M.A.; Sulham, K.; Shorr, A.F. Comparative Outcomes of Meropenem-Vaborbactam vs. Ceftazidime-Avibactam Among Adults Hospitalized with an Infectious Syndrome in the US, 2019–2021. Antibiotics 2025, 14, 29. [Google Scholar] [CrossRef]
- Shields, R.K.; Abbo, L.M.; Ackley, R.; Aitken, S.L.; Albrecht, B.; Babiker, A.; Burgoon, R.; Cifuentes, R.; Claeys, K.C.; Curry, B.N.; et al. Effectiveness of ceftazidime-avibactam versus ceftolozane-tazobactam for multidrug-resistant Pseudomonas aeruginosa infections in the USA (CACTUS): A multicentre, retrospective, observational study. Lancet Infect. Dis. 2025, 25, 574–584. [Google Scholar] [CrossRef]
- O’Donnell, J.N.; Lodise, T.P. New Perspectives on Antimicrobial Agents: Imipenem-Relebactam. Antimicrob. Agents Chemother. 2022, 66, e0025622. [Google Scholar] [CrossRef]
- Gorham, J.; Taccone, F.S.; Hites, M. Drug Regimens of Novel Antibiotics in Critically Ill Patients with Varying Renal Functions: A Rapid Review. Antibiotics 2022, 11, 546. [Google Scholar] [CrossRef] [PubMed]
- Picard, M.; Robitaille, G.; Karam, F.; Daigle, J.M.; Bédard, F.; Biron, É.; Tardif, M.R.; Lacombe-Barrios, J.; Bégin, P. Cross-Reactivity to Cephalosporins and Carbapenems in Penicillin-Allergic Patients: Two Systematic Reviews and Meta-Analyses. J. Allergy Clin. Immunol. Pract. 2019, 7, 2722–2738.e5. [Google Scholar] [CrossRef] [PubMed]
- Cannon, J.P.; Lee, T.A.; Clark, N.M.; Setlak, P.; Grim, S.A. The risk of seizures among the carbapenems: A meta-analysis. J. Antimicrob. Chemother. 2014, 69, 2043–2055. [Google Scholar] [CrossRef]
- Clancy, C.J.; Nguyen, M.H. Estimating the size of the United States market for new antibiotics with activity against carbapenem-resistant Enterobacteriaceae. Antimicrob. Agents Chemother. 2019, 63, e01733-19. [Google Scholar] [CrossRef] [PubMed]
- Caffrey, A.R.; Appaneal, H.J.; Lopes, V.V.; Riccobene, T.A.; LaPlante, K.L. Real-world utilization of ceftazidime/avibactam among inpatients in the national Veterans Affairs Healthcare System. Am. J. Health Syst. Pharm. 2024, 81, 509–520. [Google Scholar] [CrossRef]
- Harris, A.D.; Goodman, K.E.; Pineles, L.; Walker, M.; Bork, J.T.; Heil, E.L.; Claeys, K.C.; Brooks, J.; Kadri, S.; Maron, B.A.; et al. New Kids on the Block: Estimating Use of Next-generation Gram-negative Antibiotics Across Greater Than 700 Hospitals in the United States. Open Forum Infect. Dis. 2025, 12, ofaf079. [Google Scholar] [CrossRef]
- FDA. Aztreonam-Avibactam. EMBLAVIO. Summary of Products Characteristics. 2025. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/217906Orig1s000lbl.pdf (accessed on 30 April 2025).
- Carmeli, Y.; Cisneros, J.M.; Paul, M.; Daikos, G.L.; Wang, M.; Torre-Cisneros, J.; Singer, G.; Titov, I.; Gumenchuk, I.; Zhao, Y.; et al. Aztreonam-avibactam versus meropenem for the treatment of serious infections caused by Gram-negative bacteria (REVISIT): A descriptive, multinational, open-label, phase 3, randomised trial. Lancet Infect. Dis. 2025, 25, 218–230. [Google Scholar] [CrossRef]
- Daikos, G.L.; Cisneros, J.M.; Carmeli, Y.; Wang, M.; Leong, C.L.; Pontikis, K.; Anderzhanova, A.; Florescu, S.; Kozlov, R.; Noriega, E.R.; et al. Efficacy and safety of aztreonam–avibactam for the treatment of serious infections caused by metallo-β lactamase (MBL) producing multidrug resistant Gram-negative bacteria: Phase 3 ASSEMBLE trial. Abstract Number: E0846. In Proceedings of the 34th European Society of Clinical Microbiology and Infectious Diseases Global (ECCMID GLOBAL), Barcelona, Spain, 27–30 March 2024. [Google Scholar]
- Falcone, M.; Giordano, C.; Leonildi, A.; Galfo, V.; Lepore, A.; Suardi, L.R.; Riccardi, N.; Barnini, S.; Tiseo, G. Clinical Features and Outcomes of Infections Caused by Metallo-β-Lactamase-Producing Enterobacterales: A 3-Year Prospective Study From an Endemic Area. Clin. Infect. Dis. 2024, 78, 1111–1119. [Google Scholar] [CrossRef]
- Falcone, M.; Daikos, G.L.; Tiseo, G.; Bassoulis, D.; Giordano, C.; Galfo, V.; Leonildi, A.; Tagliaferri, E.; Barnini, S.; Sani, S.; et al. Efficacy of Ceftazidime-avibactam Plus Aztreonam in Patients with Bloodstream Infections Caused by Metallo-β-lactamase-Producing Enterobacterales. Clin. Infect. Dis. 2021, 72, 1871–1878. [Google Scholar] [CrossRef]
- Galani, I.; Karaiskos, I.; Giamarellou, H. Multidrug-resistant Klebsiella pneumoniae: Mechanisms of resistance including updated data for novel β-lactam-β-lactamase inhibitor combinations. Expert. Rev. Anti Infect. Ther. 2021, 19, 1457–1468. [Google Scholar] [CrossRef]
- Shields, R.K.; Chen, L.; Cheng, S.; Chavda, K.D.; Press, E.G.; Snyder, A.; Pandey, R.; Doi, Y.; Kreiswirth, B.N.; Nguyen, M.H.; et al. Emergence of Ceftazidime-Avibactam Resistance Due to Plasmid-Borne blaKPC-3 Mutations during Treatment of Carbapenem-Resistant Klebsiella pneumoniae Infections. Antimicrob. Agents Chemother. 2017, 61, e02097-16. [Google Scholar] [PubMed]
- National Center for Biotechnology Information (NCBI) Reference Sequence (Refseq) Database USA: U.S. National Library of Medicine. Available online: https://www.ncbi.nlm.nih.gov/pathogens/refgene/#KPC (accessed on 30 April 2025).
- Haidar, G.; Clancy, C.J.; Chen, L.; Samanta, P.; Shields, R.K.; Kreiswirth, B.N.; Nguyen, M.H. Identifying Spectra of Activity and Therapeutic Niches for Ceftazidime-Avibactam and Imipenem-Relebactam against Carbapenem-Resistant Enterobacteriaceae. Antimicrob. Agents Chemother. 2017, 61, e00642-17. [Google Scholar] [CrossRef] [PubMed]
- Voulgari, E.; Kotsakis, S.D.; Giannopoulou, P.; Perivolioti, E.; Tzouvelekis, L.S.; Miriagou, V. Detection in two hospitals of transferable ceftazidime-avibactam resistance in Klebsiella pneumonia due to a novel VEB beta-lactamase variant with a Lys234Arg substitution, Greece, 2019. Eurosurveillance 2020, 25, 1900766. [Google Scholar] [CrossRef]
- Galani, I.; Karaiskos, I.; Souli, M.; Papoutsaki, V.; Galani, L.; Gkoufa, A.; Antoniadou, A.; Giamarellou, H. Outbreak of KPC-2-producing Klebsiella pneumoniae endowed with ceftazidime-avibactam resistance mediated through a VEB-1-mutant (VEB-25), Greece, September to October 2019. Eurosurveillance 2020, 25, 2000028. [Google Scholar] [CrossRef]
- Zarras, C.; Iosifidis, E.; Simitsopoulou, M.; Pappa, S.; Kontou, A.; Roilides, E.; Papa, A. Neonatal Bloodstream Infection with Ceftazidime-Avibactam-Resistant blaKPC-2-Producing Klebsiella pneumoniae Carrying blaVEB-25. Antibiotics 2023, 12, 1290. [Google Scholar] [CrossRef]
- Galani, I.; Karaiskos, I.; Souli, M.; Papoutsaki, V.; Gkoufa, A.; Antoniadou, A.; Giamarellou, H. Outbreak of High-Risk Clone ST323 Klebsiella pneumoniae Resistant to Ceftazidime–Avibactam Due to Acquisition of blaVEB-25 and to Cefiderocol Due to Mutated fiu Gene. Antibiotics 2025, 14, 223. [Google Scholar] [CrossRef]
- Findlay, J.; Poirel, L.; Bouvier, M.; Gaia, V.; Nordmann, P. Resistance to ceftazidime-avibactam in a KPC-2-producing Klebsiella pneumoniae caused by the extended-spectrum beta-lactamase VEB-25. Eur. J. Clin. Microbiol. Infect. Dis. 2023, 42, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Di Bella, S.; Giacobbe, D.R.; Maraolo, A.E.; Viaggi, V.; Luzzati, R.; Bassetti, M.; Luzzaro, F.; Principe, L. Resistance to ceftazidime/avibactam in infections and colonisations by KPC-producing Enterobacterales: A systematic review of observational clinical studies. J. Glob. Antimicrob. Resist. 2021, 25, 268–281. [Google Scholar] [CrossRef]
- Lomovskaya, O.; Sun, D.; Rubio-Aparicio, D.; Nelson, K.; Tsivkovski, R.; Griffith, D.C.; Dudley, M.N. Vaborbactam: Spectrum of β-lactamase inhibition and impact of resistance mechanisms on activity in Enterobacteriaceae. Antimicrob. Agents Chemother. 2017, 61, e01443-17. [Google Scholar] [CrossRef]
- Dulyayangkul, P.; Wan Nur Ismah, W.A.K.; Douglas, E.J.A.; Avison, M.B. Mutation of kvrA Causes OmpK35 and OmpK36 Porin Downregulation and Reduced Meropenem-Vaborbactam Susceptibility in KPC-Producing Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2020, 64, e02208-19. [Google Scholar] [CrossRef]
- Findlay, J.; Poirel, L.; Nordmann, P. In vitro-obtained meropenem-vaborbactam resistance mechanisms among clinical Klebsiella pneumoniae carbapenemase-producing K. pneumoniae isolates. J. Glob. Antimicrob. Resist. 2023, 32, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Gaibani, P.; Bianco, G.; Amadesi, S.; Boattini, M.; Ambretti, S.; Costa, C. Increased bla(KPC) Copy Number and OmpK35 and OmpK36 Porins Disruption Mediated Resistance to Imipenem/Relebactam and Meropenem/Vaborbactam in a KPC-Producing Klebsiella pneumoniae Clinical Isolate. Antimicrob. Agents Chemother. 2022, 66, e0019122. [Google Scholar] [CrossRef]
- Gaibani, P.; Bovo, F.; Bussini, L.; Lazzarotto, T.; Amadesi, S.; Bartoletti, M.; Viale, P.; Ambretti, S. Dynamic evolution of imipenem/relebactam resistance in a KPC-producing Klebsiella pneumoniae from a single patient during ceftazidime/avibactam-based treatments. J. Antimicrob. Chemother. 2022, 77, 1570–1577. [Google Scholar] [CrossRef] [PubMed]
- Lob, S.H.; Karlowsky, J.A.; Young, K.; Motyl, M.R.; Hawser, S.; Kothari, N.D.; Sahm, D.F. In vitro activity of imipenem-relebactam against resistant phenotypes of Enterobacteriaceae and Pseudomonas aeruginosa isolated from intraabdominal and urinary tract infection samples–SMART Surveillance Europe 2015–2017. J. Med. Microbiol. 2020, 69, 207–217. [Google Scholar] [CrossRef]
- Shields, R.K.; Stellfox, M.E.; Kline, E.G.; Samanta, P.; Van Tyne, D. Evolution of Imipenem-Relebactam Resistance Following Treatment of Multidrug-Resistant Pseudomonas aeruginosa Pneumonia. Clin. Infect. Dis. 2022, 75, 710–714. [Google Scholar] [CrossRef]
- Bianco, G.; Boattini, M.; Lupo, L.; Ambretti, S.; Greco, R.; Degl’Innocenti, L.; Chiatamone Ranieri, S.; Fasciana, T.; Mazzariol, A.; Gibellini, D.; et al. In vitro activity and genomic characterization of KPC-producing Klebsiella pneumoniae clinical blood culture isolates resistant to ceftazidime/avibactam, meropenem/vaborbactam, imipenem/relebactam: An Italian nationwide multicentre observational study (2022-23). J. Antimicrob. Chemother. 2025, 80, 583–592. [Google Scholar]
- Baltas, I.; Vrioni, G.; Skiadas, I.; Grammelis, V.; Vourli, S.; Smyrni, N.; Hatcher, J.; Tsakris, A.; Grandjean, L. The INCREASE(ingly) difficult battle with carbapenem-resistant Klebsiella pneumoniae: Insights into novel treatment options from Greek ICUs. Abstract Number: P5063. In Proceedings of the 35th European Society of Clinical Microbiology and Infectious Diseases Global (ECCMID GLOBAL), Vienna, Austria, 11–15 April 2025. [Google Scholar]
- Livermore, D.M.; Mushtaq, S.; Vickers, A.; Woodford, N. Activity of aztreonam/avibactam against metallo-β-lactamase-producing Enterobacterales from the UK: Impact of penicillin-binding protein-3 inserts and CMY-42 β-lactamase in Escherichia coli. Int. J. Antimicrob. Agents 2023, 61, 106776. [Google Scholar] [CrossRef]
- Xiang, X.; Kong, J.; Zhang, J.; Zhang, X.; Qian, C.; Zhou, T.; Sun, Y. Multiple mechanisms mediate aztreonam-avibactam resistance in Klebsiella pneumoniae: Driven by KPC-2 and OmpK36 mutations. Int. J. Antimicrob. Agents 2025, 65, 107425. [Google Scholar] [CrossRef] [PubMed]
- Shields, R.K.; Nguyen, M.H.; Chen, L.; Press, E.G.; Kreiswirth, B.N.; Clancy, C.J. Pneumonia and Renal Replacement Therapy Are Risk Factors for Ceftazidime-Avibactam Treatment Failures and Resistance among Patients with Carbapenem-Resistant Enterobacteriaceae Infections. Antimicrob. Agents Chemother. 2018, 6, e02497-17. [Google Scholar] [CrossRef]
- Berkhout, J.; Melchers, M.J.; van Mil, A.C.; Seyedmousavi, S.; Lagarde, C.M.; Nichols, W.W.; Mouton, J.W. Pharmacokinetics and penetration of ceftazidime and avibactam into epithelial lining fluid in thigh- and lung-infected mice. Antimicrob. Agents Chemother. 2015, 59, 2299–2304. [Google Scholar] [CrossRef]
- Nicolau, D.P.; Siew, L.; Armstrong, J.; Li, J.; Edeki, T.; Learoyd, M.; Das, S. Phase 1 study assessing the steady-state concentration of ceftazidime and avibactam in plasma and epithelial lining fluid following two dosing regimens. J. Antimicrob. Chemother. 2015, 70, 2862–2869. [Google Scholar] [CrossRef] [PubMed]
- Wenzler, E.; Gotfried, M.H.; Loutit, J.S.; Durso, S.; Griffith, D.C.; Dudley, M.N.; Rodvold, K.A. Meropenem-RPX7009 Concentrations in Plasma, Epithelial Lining Fluid, and Alveolar Macrophages of Healthy Adult Subjects. Antimicrob. Agents Chemother. 2015, 59, 7232–7239. [Google Scholar] [CrossRef]
- O’Jeanson, A.; Ioannidis, K.; Nielsen, E.I.; Galani, L.; Ginosyan, A.; Paskalis, H.; Loryan, I.; Giamarellou, H.; Friberg, L.E.; Karaiskos, I. Ceftazidime-avibactam (CAZ-AVI) pharmacokinetics in critically ill patients undergoing continuous venovenous hemodiafiltration (CVVHDF). Int. J. Antimicrob. Agents 2025, 65, 107394S. [Google Scholar] [CrossRef] [PubMed]
- Soukup, P.; Faust, A.C.; Edpuganti, V.; Putnam, W.C.; McKinnell, J. A Steady-State Ceftazidime-Avibactam Serum Concentrations and Dosing Recommendations in a Critically Ill Patient Being Treated for Pseudomonas aeruginosa Pneumonia and Undergoing Continuous Venovenous Hemodiafiltration. Pharmacotherapy 2019, 39, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- Paudel, R.; Shrestha, E.; Chapagain, B.; Tiwari, B. Carbapenemase producing Gram negative bacteria: Review of resistance and detection methods. Diagn. Microbiol. Infect. Dis. 2024, 110, 116370. [Google Scholar] [CrossRef]
- Tibbetts, R.; George, S.; Burwell, R.; Rajeev, L.; Rhodes, P.A.; Singh, P.; Samuel, L. Performance of the Reveal Rapid Antibiotic Susceptibility Testing System on Gram-Negative Blood Cultures at a Large Urban Hospital. J. Clin. Microbiol. 2022, 60, e0009822. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Burns, K.; Rodríguez Baño, J.; Borg, M.; Daikos, G.; Dumpis, U.; Lucet, J.C.; Moro, M.L.; Tacconelli, E.; Simonsen, G.S.; et al. Infection prevention and control measures and tools for the prevention of entry of carbapenem-resistant Enterobacteriaceae into healthcare settings: Guidance from the European Centre for Disease Prevention and Control. Antimicrob. Resist. Infect. Control. 2017, 6, 113. [Google Scholar] [CrossRef]
- Mills, J.P.; Marchaim, D. Multidrug-Resistant Gram-Negative Bacteria: Infection Prevention and Control Update. Infect. Dis. Clin. 2021, 35, 969–994. [Google Scholar]

{kind=link}
| Antimicrobial Agents | Enterobacterales | Carbapenem Resistant | |||
|---|---|---|---|---|---|
| KPC | MBL 1 | OXA-48 | P. aeruginosa | A. baumannii | |
| Ceftazidime/avibactam | + | − | + | + 3 | − |
| Meropenem/vaborbactam | + | − | − | − | − |
| Imipenem/cilastatin/relebactam 2 | + | − | − | + 3 | − |
| Aztreonam/avibactam | + | + | + | − | − |
| Drug | Dose | Renal Adjustment | CRRT |
|---|---|---|---|
| Ceftazidime/avibactam | 2.5 g (2 g/0.5 g) q8h (infusion over 3 h) | CrCl > 50: 2.5 g q8h CrCl 31–50: 1.25 g q8h CrCl 10–30: 0.94 g q12h CrCl < 10: 0.94 g q48h CrCl 6–15 (±HD): 0.94 g q24h CrCl ≤ 5 (±HD): 0.94 g q48h | CVVH: 1.25 g q8h CVVHDF: 2.5 g q8h |
| Meropenem/vaborbactam | 4 g (2 g/2 g) q8h (infusion over 3 h) | CrCl > 50: 4 g q8h CrCl 30–49: 2 g q8h CrCl 15–29: 2 g q12h CrCl < 15: 1 g q12h HD: 1 g q12h (AD) | No data |
| Imipenem/cilastatin/relebactam | 1.25 g (0.5 g/0.5 g/0.25 g) q6h infusion 30 min | CrCl ≥ 90: 1.25 g q6h CrCl 60–89: 1 g q6h CrCl 30–59: 0.75 g q6h CrCl 15–29: 0.5 g q6h CrCl < Not recommended HD: 0.5 g q6h (AD) | No data |
| Aztreonam/avibactam * | 2.67 g (2 g/0.67 g) loading dose, then 2 g (1.5 g/0.5 g) q6h (infusion 3 h) | CrCl > 50: 2.67 g × 1, then 2 g q6h CrCl > 30–50: 2.67 g × 1 then 1 g q6h CrCl > 15–30: 1.8 g × 1, then 0.9 g q8h CrCl ≤ 15: 1.33 g × 1, then 0.9 g q12h HD: 1.33 g × 1, then 0.9 g q12h (AD) | No data |
| Ceftazidime/ Avibactam | Aztreonam/ Avibactam | Meropenem/ Vaborbactam | Imipenem/ Relebactam | |
|---|---|---|---|---|
| Mechanism of action | Diazabicyclooctane non-β-lactam–β-lactamase inhibitor | Diazabicyclooctane non-β-lactam–β-lactamase inhibitor | Cyclic boronic acid inhibitor | Diazabicyclooctane non-β-lactam–β-lactamase inhibitor, structurally related to avibactam, differing by the addition of a piperidine ring to the 2-position of the carbonyl group |
| Spectrum | Enterobacterales and P. aeruginosa producing ESBL, KPC, AmpC, and some class D enzymes (OXA-48) Not active against MBL, Acinetobacter spp., and no activity against anaerobes | Enterobacterales producing ESBL, KPC, AmpC, OXA-48, and MBL As active as aztreonam alone against P. aeruginosa and A. baumannii, including MBL-producing isolate | Enterobacterales producing ESBL, KPC, and AmpC Not active against OXA-48-like or MBL As active as meropenem alone against P. aeruginosa, Acinetobacter spp. | Enterobacterales and P. aeruginosa producing ESBL, KPC, AmpC, and porin mutations Diminished inhibitor activity against OXA-48 No activity against MBL, A. baumannii, Proteus spp., Providencia spp., and Morganella spp. |
| Indications | cUTI, cIAI, HAP/VAP, bacteremia associated with cUTI, cIAI, HAP/VAP, infections by Gram-negative pathogens with limited treatment options | cUTI, cIAI, HAP/VAP, infections by Gram-negative pathogens with limited treatment options | cUTI, cIAI, HAP/VAP, bacteremia associated with cUTI, cIAI, HAP/VAP, infections by Gram-negative pathogens with limited treatment options | HAP/VAP, bacteremia associated with HAP/VAP, infections by Gram-negative pathogens with limited treatment options |
| Efficacy | Enterobacterales: 75–80% P.aeruginosa: 50–85% | Enterobacterales: 75% | Enterobacterales: 60–75% | Enterobacterales and P. aeruginosa: 70% |
| Comments | Preferred agent in penicillin allergy Approved in pediatric patients (≥3 months) | Only agent active against MBL | High sodium load | Neurologic side effects, i.e., seizure |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karaiskos, I.; Galani, I.; Daikos, G.L.; Giamarellou, H. Breaking Through Resistance: A Comparative Review of New Beta-Lactamase Inhibitors (Avibactam, Vaborbactam, Relebactam) Against Multidrug-Resistant Superbugs. Antibiotics 2025, 14, 528. https://doi.org/10.3390/antibiotics14050528
Karaiskos I, Galani I, Daikos GL, Giamarellou H. Breaking Through Resistance: A Comparative Review of New Beta-Lactamase Inhibitors (Avibactam, Vaborbactam, Relebactam) Against Multidrug-Resistant Superbugs. Antibiotics. 2025; 14(5):528. https://doi.org/10.3390/antibiotics14050528
Chicago/Turabian StyleKaraiskos, Ilias, Irene Galani, George L. Daikos, and Helen Giamarellou. 2025. "Breaking Through Resistance: A Comparative Review of New Beta-Lactamase Inhibitors (Avibactam, Vaborbactam, Relebactam) Against Multidrug-Resistant Superbugs" Antibiotics 14, no. 5: 528. https://doi.org/10.3390/antibiotics14050528
APA StyleKaraiskos, I., Galani, I., Daikos, G. L., & Giamarellou, H. (2025). Breaking Through Resistance: A Comparative Review of New Beta-Lactamase Inhibitors (Avibactam, Vaborbactam, Relebactam) Against Multidrug-Resistant Superbugs. Antibiotics, 14(5), 528. https://doi.org/10.3390/antibiotics14050528