Abstract
Background/Objectives: ESKAPE pathogens (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter spp.) pose a serious public health threat as they are resistant to multiple antimicrobial agents. Bloodstream infections (BSIs) caused by ESKAPE bacteria have high mortality rates due to the limited availability of effective antimicrobials. This study aimed to evaluate the prevalence and susceptibility of ESKAPE pathogens causing BSIs over three years in a large tertiary hospital in Salerno. Methods: Conducted at the Clinical Microbiology Laboratory of San Giovanni di Dio e ‘‘Ruggi D’Aragona’’ Hospital from January 2020 to December 2022, blood culture samples from different departments were incubated in the BD BACTEC™ system for 5 days. Species identification was performed using MALDI-TOF MS, and antimicrobial resistance patterns were determined by the VITEK2 system. Results: Out of 3197 species isolated from positive blood cultures, 38.7% were ESKAPE bacteria. Of these, 59.9% were found in blood culture samples taken from men, and the most affected age group was those aged >60 years. (70.6%). Staphylococcus aureus was the main BSI pathogen (26.3%), followed by Klebsiella pneumoniae (15.8%). Significant resistance rates were found, including 35% of Staphylococcus aureus being resistant to oxacillin and over 90% of Acinetobacter baumannii being resistant to carbapenems. Conclusions: These results highlight the urgent need for antimicrobial stewardship programs to prevent incurable infections.
1. Introduction
Bloodstream infections (BSIs) account for 15% of all nosocomial infections and are among the leading causes of mortality in hospitalized patients, representing a serious international health problem [1,2]. In Europe and North America, BSIs rank among the top seven causes of death and contribute to approximately a quarter of a million fatalities each year [3,4,5]. In Italy, 3056 cases of BSI were reported in 2022. In 2021, there were 2396 reported cases; this number has since increased, probably due to the large use of antibiotics during the COVID-19 pandemic period [6]. Most BSIs were caused by Klebsiella pneumoniae, with 95.2% of these isolates producing the carbapenemase (KPC) enzyme [7]. Antimicrobial resistance (AMR) poses a serious potential threat to global health, leading to high mortality and morbidity rates. Each year, antibiotic-resistant infections result in approximately 33.000 deaths in Europe and 700,000 worldwide. Projections indicate that by 2050, these infections could cause up to 10 million deaths per year worldwide [8]. In Italy, the situation is particularly concerning, as the country ranks among the highest in Europe for both antimicrobial consumption and the prevalence of resistant bacterial strains [9]. The rapid spread of AMR presents profound clinical and economic challenges, necessitating urgent international intervention [10]. The most common bacteria isolated in BSIs are the ESKAPE bacteria, which are a major concern due to their multidrug resistance (MDR) profiles and their relevance in nosocomial settings. The Infectious Diseases Society of America coined the acronym ESKAPE to emphasize these pathogens’ ability to evade common therapies through various drug resistance mechanisms [11]. These mechanisms include enzymatic inactivation, alteration of drug targets, changes in cell permeability (such as loss of porins or increased efflux pump expression), and protective mechanisms like biofilm formation [12]. The ESKAPE group includes a range of Gram-positive and Gram-negative species, including Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter spp. [12]. In a multicentre study involving 193 hospitals across the US, Marturano and Lowery found that 42.2% of the bacteria isolated from BSIs belonged to the ESKAPE group [13]. According to the latest European Centre for Disease Prevention and Control (ECDC) report on AMR surveillance, these pathogens continue to exhibit high levels of resistance to last-line antibiotics, as highlighted in previous reports from 2019. Increasing trends in resistance have been noted, particularly in carbapenem and third-generation-cephalosporin resistance among Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii, as well as vancomycin resistance in Enterococcus faecium, which has shown a significant rise. In Italy, data reported by Italian National Institute of Health, indicate a concerning increase in vancomycin resistance among Enterococcus faecium isolates, rising from 23.6% in 2020 to 28.2% in 2021 [14]. Therefore, continued vigilant monitoring of these trends is essential. In Europe, the prevalence of methicillin-resistant Staphylococcus aureus isolates (MRSA) has been declining. However, in Italy, after a stability period, there was an uptick in MRSA isolates in 2021. Additionally, over the past four years, in multiple European countries, including Italy, there has been a significant rise in the annual number of invasive Acinetobacter baumannii isolated [15,16]. Given the epidemiology of BSIs caused by ESKAPE pathogens and the clear limitations of current antimicrobial strategies, there is an urgent need to enhance empirical therapeutic approaches, while also developing new antimicrobial agents to combat the global health crisis associated with antibiotic resistance. The aim of this study was to evaluate the prevalence of BSIs caused by ESKAPE pathogens and to investigate their antimicrobial susceptibility patterns at San Giovanni di Dio e Ruggi d’Aragona University hospital, from 2020 to 2022.
2. Results
2.1. Prevalence of BSIs in Studied Patients
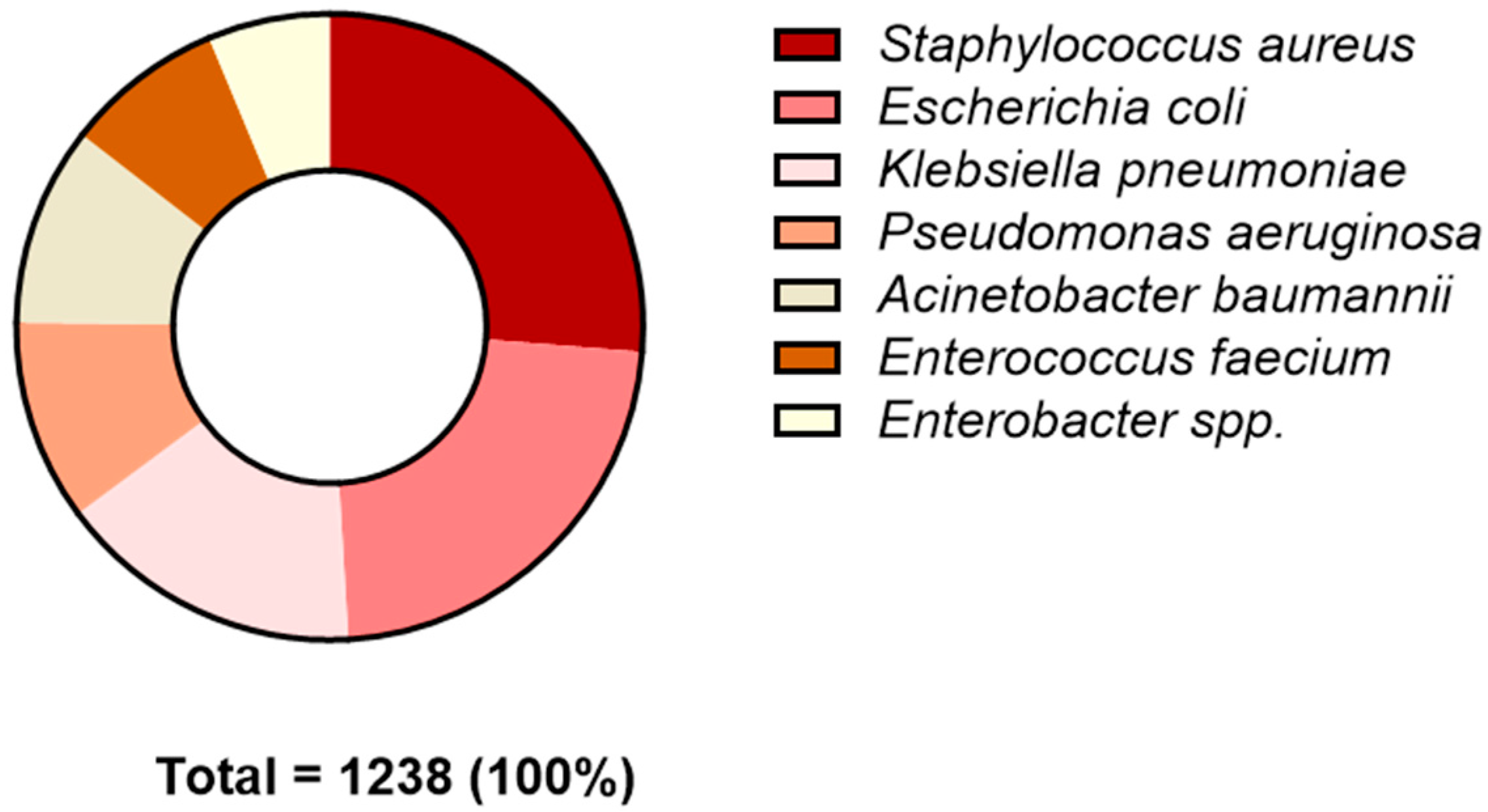
In the present study, blood cultures were examined to diagnose BSIs based on patients’ clinical symptoms, including: (i) fever (>38 °C), (ii) chills, (iii) hypotension, (iv) elevated white blood cell count, and (v) increased concentrations of inflammatory markers. Out of the blood cultures processed, 3197 tested positive. Among these, 1238 (38.7%) were positive for ESKAPE bacteria, and 1959 (61.3%) were positive for other pathogens (Table 1). Regarding gender distribution, of the 2087 BSI-positive patients, 837 (40.1%) and 1250 (59.9%) were from women and men, respectively. The difference between positive males and females was not statistically significant. Analyzing the age distribution of infections, the majority of positive cases were found in the elderly (≥60 years) (70.6%); followed by middle-aged adults (40–59 years) (19.5%); infants, children, and adolescents (0–19 years) 5%); and young adults (20–39 years) (Table 2). Our data indicate that the predominant bacterium isolated from blood samples was Staphylococcus aureus, with a prevalence of 26.3%. This was followed by Escherichia coli (22.8%), Klebsiella pneumoniae (15.8%), Pseudomonas aeruginosa (10.4%), Acinetobacter baumannii (10.3%), Enterococcus faecium (8.2%), and Enterobacter spp. (6.3%) (Figure 1).

Table 1.
BSI distribution of ESKAPE and non-ESKAPE pathogens among positive blood cultures.
Table 2.
Gender and age distribution in patients with positive blood cultures.
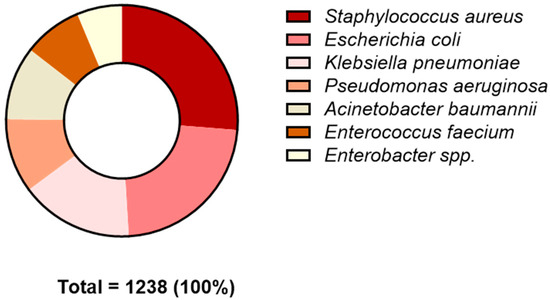
Figure 1.
Prevalence of ESKAPE species from patients at San Giovanni di Dio and ‘‘Ruggi D’Aragona’’ University Hospital in Salerno from January 2020 to December 2022.
2.2. Prevalence of Antimicrobial Resistance among Pathogens Identified in BSIs
The detailed antimicrobial resistance profiles of ESKAPE pathogens identified in our study are presented in Table 3 and Table 4. All isolated bacteria demonstrated a high level of resistance to the antibiotics tested. Acinetobacter baumannii exhibited resistance rates exceeding 78.8% to amikacin, ciprofloxacin, gentamicin, imipenem, meropenem, tobramycin, and trimethoprim/sulfamethoxazole. However, resistance to colistin was notably low, at less than 2.9%. Escherichia coli demonstrated a lower resistance rate of 63.5% to a range of antibiotics, including amikacin, amoxicillin/clavulanic acid, cefepime, ciprofloxacin, colistin, gentamicin, imipenem, meropenem, piperacillin/tazobactam, tobramycin, trimethoprim/sulfamethoxazole, ceftazidime, ceftazidime/avibactam, and ceftolozane/tazobactam. A significant decrease in gentamicin resistance was observed from 2020 to 2022, dropping from 31.5% to 19.4% (p-value = 0.046). Similarly, resistance to tobramycin significantly decreased from 32.3% to 19.2% during the same period (p-value = 0.032). In contrast, resistance to ceftazidime/avibactam notably increased, with resistant isolates rising from 0% in 2020 to 5.6% in 2022 (p-value = 0.020). Strains of Klebsiella pneumoniae exhibited resistance rates greater than 60% to various antibiotics, such as amoxicillin/clavulanic acid, cefepime, cefotaxime, ciprofloxacin, and piperacillin/tazobactam. Between 2020 and 2022, the prevalence of Klebsiella pneumoniae strains resistant to amikacin significantly decreased from 35.8% to 20.8% (p-value = 0.047). Resistance to ciprofloxacin also declined, with 82.4% of strains resistant in 2020 compared with 63.9% in 2022 (p-value = 0.020). Similarly, resistance to meropenem significantly dropped from 57.4% in 2020 to 36% in 2022. Resistance to colistin also showed a notable reduction, with colistin-resistant strains decreasing from 32.3% in 2020 to just 7% in 2022 (p-value < 0.001). Low antibiotic resistance rates were associated with Pseudomonas aeruginosa strains. In detail, a resistance rate of less than 44.7% was found for antibiotics including amikacin, cefepime, ceftazidime, ceftazidime/avibactam, ceftolozane/tazobactam, ciprofloxacin, colistin, imipenem, meropenem, tobramycin, and trimethoprim/sulfamethoxazole. Resistance to carbapenems (meropenem and imipenem) and tobramycin increased significantly from 2020 to 2022. Specifically, resistance to tobramycin rose from 12.5% in 2020 to 28.3% in 2022. For imipenem, resistance among Pseudomonas aeruginosa strains increased from 18.3% in 2020 to 34% in 2022. Similarly, resistance to meropenem escalated from 5.9% in 2020 to 32% in 2022. Among the Gram-positive strains, Enterococcus faecium demonstrated resistance rates exceeding 87.5% to penicillins and greater than 85.7% to quinolones. Resistance to glycopeptides was below 28.6%, while resistance to the sole active macrolide was less than 12.5%. Additionally, resistance to linezolid was less than 14.3%, and resistance to tigecycline was 6.3%. A significant increase in resistance to kanamicin was observed over the study period, with resistance rates rising from 81.3% in 2020 to 100% in 2022. Strains of Staphylococcus aureus exhibited resistance rates below 80.7% to a range of antibiotics, including trimethoprim/sulfamethoxazole, tigecycline, vancomycin, teicoplanin, tetracycline, rifampin, penicillin, oxacillin, mupirocin, linezolid, levofloxacin, daptomycin, erythromycin, gentamicin, and fosfomycin. Over the study period, levels of resistance to fosfomycin and vancomycin increased significantly. Throughout the study period, resistance to fosfomycin and vancomycin increased significantly. Specifically, resistance to fusidic acid rose from 2.4% in 2020 to 7.4% in 2022. Similarly, the prevalence of vancomycin-resistant strains increased from 1.2% in 2020 to 12.5% in 2022.
Table 3.
Resistant ESKAPE Gram-negative strains isolated from blood cultures.
Table 4.
Resistant ESKAPE Gram-positive strains isolated from blood cultures.
3. Discussion
BSIs pose an increasing threat to public health globally. In Europe, 2 million BSI cases annually result in 250,000 deaths, making BSIs the leading cause of infection-related mortality [17]. In our retrospective study, the number of positive blood cultures increased over the study period, with 820 in 2020, 1039 in 2021, and 1338 in 2022. The low number of blood cultures collected during the first wave of COVID-19 has also been reported in other studies [18,19]. This decrease can be attributed to a reduced access to healthcare departments and a decline in scheduled surgeries during the pandemic. Our data indicate that males were the most affected by BSIs, a finding also demonstrated by Uslan et al. In their study, nosocomial BSIs were more prevalent in males (23.8%) compared with females (13.9%), although this difference was not significant [20]. A prospective study conducted in Norway similarly found that men were at greater risk of experiencing a BSI than women [21]. This disparity can be attributed to physiological differences influencing susceptibility to infections, as well as extrinsic factors such as smoking, alcohol consumption, and recreational activities, which vary between sexes and contribute to the onset of blood infections. Furthermore, our study found that the age group most affected by BSIs was 60 to 79, representing more than 50% of cases. This is consistent with other studies, which have demonstrated that the incidence of bacteremia increases with age [20,22]. The increased incidence of MDR infections in older adults is primarily due to several age-related factors. Immune senescence significantly weakens the immune system, reducing both innate and adaptive immune responses. This leads to decreased production of naive T cells and diminished functionality of existing T and B cells, impairing the body’s ability to combat new and resistant pathogens. Additionally, older adults often have comorbidities such as diabetes, chronic obstructive pulmonary disease (COPD), and cardiovascular diseases, which further compromise their immune defenses. These conditions often necessitate medical interventions involving invasive devices like catheters or mechanical ventilators, which can increase infection risk. Anatomical and functional changes also contribute to increased vulnerability; for instance, thinning skin and mucosal membranes reduce physical barriers, while reduced lung function and bladder control lead to fluid stasis, promoting bacterial growth [23,24]. Moreover, older adults frequently encounter healthcare settings, which are hotspots for MDR organisms due to high antibiotic use and the presence of vulnerable populations. Frequent hospitalizations or stays in long-term care facilities further expose them to healthcare-associated infections (HAIs) caused by MDR pathogens. Collectively, these factors significantly elevate the risk of MDR infections in older adults [25]. BSIs caused by drug-resistant bacteria are linked to significant morbidity and mortality, extended hospital stays, and higher healthcare costs [26]. Among the most prevalent multidrug-resistant bacteria causing BSIs are the ESKAPE pathogens. In our study, ESKAPE pathogens were responsible for 38.7% of BSIs, while other pathogens accounted for 61.3% of cases. Within the ESKAPE group, Staphylococcus aureus was the most frequently isolated species from blood cultures, with a prevalence of 28%. This was followed by Escherichia coli (24.3%), Klebsiella pneumoniae (16.8%), Pseudomonas aeruginosa (11.1%), Acinetobacter baumannii (10.9%), and Enterococcus faecium (8.8%).
Consistent with our previous research, Staphylococcus aureus remains a leading cause of BSIs, with an average prevalence of 12.8% observed from 2015 to 2019 at San Giovanni di Dio and Ruggi D’Aragona Hospital. In line with the findings of Marturano et al., Staphylococcus aureus and Escherichia coli were the most prevalent ESKAPE pathogens in BSIs, comprising 21.9% and 22.6% of the total pathogens isolated from blood cultures, respectively [13]. In a study conducted in Iran, the prevalent species associated with BSIs were Staphylococcus aureus (30%), Acinetobacter baumannii (22%), Pseudomonas aeruginosa (17%), Klebsiella pneumoniae (13%), Enterobacter aerogenes (10.3%), and Enterococcus faecium (7.7%). The resistance patterns of the main ESKAPE strains have been reported. Our study revealed significant resistance patterns in Staphylococcus aureus, with high rates of resistance to erythromycin (48.1%), oxacillin (35.2%), and levofloxacin (34.4%). These findings are consistent with previous research by Licata et al. [27]. However, resistance to gentamicin decreased from 13.3% in 2015 to 5.7% in 2021, as noted by Santella et al. [28]. The COVID-19 pandemic has affected resistance trends, leading to increased resistance to linezolid, rifampicin, and teicoplanin, as shown by Golli et al. However, resistance to oxacillin decreased slightly from 36.1% in 2020 to 33.8% in 2022. Despite the stable or declining MRSA rates in several EU/EEA countries [16], resistance to teicoplanin increased at Ruggi D’Aragona Hospital. Notably, Staphylococcus aureus strains remain highly sensitive to vancomycin (92.7%) and daptomycin (94.2%), essential for treating MRSA infections. Antimicrobial resistance in Enterococcus species represents a significant global challenge due to their intrinsic resistance to multiple classes of antibiotics and limited effective therapeutic options. Our study detected vancomycin-resistant enterococci (VRE) in 21.2% of E. faecium strains. Resistance to vancomycin, mainly due to the vanA and vanB genes, is more common in Enterococcus faecium isolates. Epidemiological data from ECDC show a 33.2% increase in VRE strains in Europe from 2018 to 2022, with a slight decline of 4% from 2021 to 2022. Italy saw an increasing trend from 23.6% in 2020 to 30.7% in 2022, while countries such as France and Austria report lower resistance levels than Italy and Germany. Compared with previous data, our study was in line with Boccella et al., who reported an increase in vancomycin resistance in enterococci at Ruggi D’Aragona Hospital, from 3.7% to 18.75% for Enterococcus faecium [29]. Similarly, Lupia et al. found vancomycin resistance in 23.3% of E. faecium isolates. Despite the increase in VRE, our study showed that isolates remain highly sensitive to linezolid and tigecycline, although resistance to teicoplanin is almost as high as to vancomycin. Treatment for VRE BSIs has evolved, with recent evidence suggesting that high-dose daptomycin may reduce mortality more effectively than linezolid [30]. Escherichia coli is a major cause of BSIs in Europe, although it was the second most frequently isolated pathogen in our study. This bacterium represents a serious public health problem due to its reservoir of resistance genes. In 2022, we observed a marked increase in resistance among Escherichia coli isolates to third-generation cephalosporins, aminopenicillins, fluoroquinolones, and aminoglycosides, as reported by EARS-NET [31]. Despite this, carbapenem resistance remains low, with rates of 0.5% for imipenem and 1.1% for meropenem. The highest resistance rate was reported for third-generation cephalosporins (40.75%), followed by fluoroquinolones (36.4%), aminoglycosides (17%), and beta-lactam/beta-lactamase inhibitors (17%). These findings are consistent with Canadian studies linking resistance to increased mortality in Escherichia coli-related bacteremia [32]. The impact of COVID-19 on Escherichia coli infections has been mixed. An English study reported a decrease in Escherichia coli BSIs and resistance to piperacillin–tazobactam and ciprofloxacin in 2020 compared with 2019 [33]. In contrast, data from a New York hospital highlighted a slight increase in Escherichia coli-related bacteremia during the pandemic. The same trend was observed at the Ruggi D’Aragona Hospital, where Escherichia coli represented 10.71% of BSIs in 2019 and 8.9% in 2020 [28,34]. For E. coli infections resistant to third-generation cephalosporins, the AIFA guidelines recommend imipenem–cilastatin or meropenem as first-line treatments. Alternatives include cefepime and fosfomycin for AmpC-producing strains, or ceftazidime–avibactam and ceftolozane–tazobactam if other options are not suitable [35]. Our study found resistance rates to these alternative treatments of 2.9% and 6.3%, respectively. Antimicrobial resistance and virulence are critical factors influencing the pathogenicity of Klebsiella pneumoniae. This pathogen presents significant therapeutic challenges due to the limited efficacy of available antibiotics. In our study, Klebsiella pneumoniae isolates showed high rates of resistance to third-generation cephalosporins (72.9%), fluoroquinolones (68.9%), aminoglycosides (39.2%), and carbapenems (36.9%). These resistance patterns are consistent with global trends reported in the literature [36,37]. Resistance to third-generation cephalosporins, largely due to their widespread administration as first-choice empirical therapy, has a highly resonant global impact, affecting public health expenditure, and the spread of resistance by nosocomial infections with high death rates. Resistance to cephalosporins has led to an ever-increasing use of carbapenems over time, inducing resistance also for this class of molecules, leading to serious limitations in treatment options and representing a global call for the development of new antimicrobial molecules [14,38]. Carbapenem resistance showed an inconsistent trend during the study period. In 2020, resistance rates were approximately 42.5% for imipenem and 57.3% for meropenem. However, a notable decrease in resistance was observed in 2021, followed by a resurgence in 2022. This increase during the COVID-19 pandemic can be attributed to the excessive use of carbapenems to treat coinfected patients, as reported by Petrakis et al. [39]. In contrast, Italian data from 2020–2022 indicate a recent decline in carbapenem resistance among Klebsiella pneumoniae isolates. Given the complexity of treating carbapenem-resistant Klebsiella pneumoniae (CRE) infections, the use of ceftazidime/avibactam is recommended. Our study supports this approach, showing a high sensitivity of Klebsiella pneumoniae isolates to this combination of antibiotics (91.1%) [40]. An international cohort study conducted by EUROBACT 5 identified Acinetobacter baumannii as the most prevalent pathogen in BSIs in intensive care units (ICUs) [41]. Infections caused by Acinetobacter baumannii are associated with high mortality rates, with a 14-day mortality of 61.2% and a 30-day mortality of 73.6% reported in a study conducted in 12 Italian hospitals [42]. The multidrug resistance of the bacterium complicates treatment, leading to its classification by the WHO in 2018 as a “critical priority” pathogen due to carbapenem resistance. In our study, carbapenem resistance rates were alarmingly high, at 95% for imipenem and 95.5% for meropenem, consistent with other research but lower than EARS-NET surveillance data [31]. Resistance to aminoglycosides and fluoroquinolones also exceeded 80%, making colistin the most effective treatment, with a sensitivity rate of 97.5%. However, colistin resistance has been reported, with an overall rate of 4% and increasing prevalence from 2001 to 2023, as highlighted by a recent meta-analysis [43]. For the treatment of carbapenem-resistant A. baumannii BSI (CRAB), combination therapies such as ampicillin–sulbactam with minocycline or colistin are recommended [44]. EARS-NET data reveal that 32.4% of Pseudomonas aeruginosa isolates are resistant to at least one class of antibiotics (piperacillin–tazobactam, fluoroquinolones, ceftazidime, aminoglycosides, or carbapenems), with 19.7% resistant to two or multiple classes [31]. In Italy, resistance rates are highest for piperacillin–tazobactam (24.1%), followed by ceftazidime (19.0%), fluoroquinolones (18.5%), carbapenems (16.4%), and aminoglycosides (4%) [40]. Our study was in line with these findings, although fluoroquinolone resistance was higher, at 31.8%. During the study period, Pseudomonas aeruginosa retained significant susceptibility to colistin (93.3%) and amikacin (89.9%), with a notable decrease in amikacin resistance compared with the 2015–2019 period. Resistance to piperacillin–tazobactam remained stable, while resistance to ciprofloxacin and carbapenems showed a decline [45]. In contrast, a study conducted in southwestern China reported increased resistance to ciprofloxacin and gentamicin, but decreased resistance to piperacillin–tazobactam and imipenem during the pandemic [46]. This discrepancy in antimicrobial resistance and susceptibility profiles may be due to the different global localization and different therapeutic protocols implemented during the pandemic period. For BSIs from Pseudomonas aeruginosa with multidrug-resistant strains, ceftolozane–tazobactam, which showed a sensitivity of 86.9% in our study, is recommended. Resistance to ceftazidime–avibactam was found in 11.2% of isolates, while imipenem–relebactam was not tested at Ruggi D’Aragona Hospital.
4. Materials and Methods
4.1. Sample Collection
A blood samples were collected from patients at San Giovanni di Dio and ‘‘Ruggi D’Aragona’’ University Hospital in Salerno, from January 2020 to December 2022. The blood cultures were subsequently transported to the microbiology laboratory and processed.
4.2. Inclusion and Exclusion Criteria
The inclusion criteria were defined as follows: (i) enrolment of patients ranging in age from 0 to 99 years; (ii) inclusion of patients presenting with clinical and/or laboratory indicators indicative of bloodstream infection; and (iii) inclusion of patients from whom blood samples were collected specifically for requested microbiological analysis. Exclusion criteria were as follows: (i) patients with previous antimicrobial therapy that could have influenced antimicrobial susceptibility results; and (ii) positive blood cultures for non-ESKAPE-group pathogens.
4.3. Bacterial Culture and Identification
Blood cultures were incubated in the BD BACTEC™ Automated Blood Culture Monitoring System (Becton Dickinson Diagnostic Instrument Systems). The incubation protocol lasted 5 days, during which the system identified positive blood cultures. Subsequently, one drop from each flask was plated onto agar media, including chocolate agar, CNA blood agar, MacConkey agar, and Sabouraud Glucose agar (Oxoid, Hampshire, UK) for the detection of aerobic pathogens. In cases of positivity for anaerobic bacteria, chocolate agar and Schaedler Blood Agar media were used. All plates were incubated overnight at 37 °C under aerobic conditions, except for chocolate agar plates, which were incubated in 5% CO2, and Schaedler Blood Agar medium, which was incubated under anaerobic conditions. Bacterial identification was achieved using matrix-assisted laser desorption/ionization time-of- flight mass spectrometry (MALDI-TOF MS) (bioMérieux, Marcy l’Etoile, France). Two colonies from an agar plate culture were transferred to VITEK MS-DS slide (bioMérieux). Each well was coated with 1 μL of matrix solution (VITEK MS-CHCA, bioMérieux, Marcy l’Etoile, France), a saturated solution of alpha-cyano-4-hydroxycinnamic acid, and dried for 5 min. The resulting spectra were imported into MYLA (bioMérieux, Marcy l’Etoile, France) and analyzed using standard pattern matching against reference spectra. The percentage probability range of between 60 and 99% showed a good level of identification.
4.4. Antibiotic Susceptibility Assays
The VITEK2 system (bioMérieux, Marcy l’Etoile, France) was utilized for confirming species identification obtained via MALDI-TOF MS and for conducting antibiotic susceptibility testing. Pure bacterial colonies were inoculated into a test tube containing 3 mL of a 0.45% sodium chloride solution. A Densichek (bioMérieux, Marcy l’Etoile, France) was used to adjust the bacterial suspension to a McFarland standard of 0.5. The identification cards (ID-GN for Gram-negative bacteria and ID-GP for Gram-positive bacteria) were placed in the tubes containing the inoculum, while the sensitivity cards (AST-658, AST-659, and AST-397) were inserted inside the empty test tubes. The results of antimicrobial susceptibility tests were interpreted according to EUCAST guidelines. The following antimicrobials were assessed in this study: amoxicillin/clavulanic acid, cefepime, cefotaxime, ceftazidime, ciprofloxacin, colistin, imipenem, meropenem, gentamicin, levofloxacin, kanamicin high level, oxacillin, and streptomycin.
4.5. Data Analysis
The Cochrane–Armitage test was employed to evaluate the statistical significance of trends. XLSTAT was used to conduct statistical analysis (Lumivero (2024). XLSTAT statistical and data analysis solution. Paris, France). An alpha level of 0.05 was considered significant. Ethical approval was waived for this retrospective analysis of anonymized data.
5. Conclusions
Antimicrobial resistance represents a silent pandemic poised to cause more deaths than cancer. This study evaluated the resistance patterns of ESKAPE pathogens responsible for BSIs. The primary pathogens involved were Staphylococcus aureus and Escherichia coli, with prevalences of 26.3% and 22.8%, respectively. Unfortunately, the mismanagement of antibiotics has not only led to increased resistance to common antibiotics, but also compromised the efficacy of newer drugs. For instance, Staphylococcus aureus exhibited a significant rise in resistance to fosfomycin and vancomycin between 2020 and 2022. Similarly, Escherichia coli showed increased resistance to the latest-generation antibiotic ceftazidime/avibactam, highlighting the consequences of poor management of new antibiotics. The significant rise in resistance to both common and newer antibiotics underscores the urgent need for improved antibiotic stewardship. Addressing this issue is critical to preserving the efficacy of existing treatments and preventing a future dominated by untreatable infections.
Author Contributions
Conceptualization, V.F. and G.F.; software, B.S.; validation, G.F.; formal analysis, B.S. and F.D.; investigation, V.F.; resources, G.F.; data curation, B.S.; writing—original draft preparation, M.D.P. and R.M.; writing—review and editing, V.F. and E.S.; visualization, F.F.B., E.S. (Enrica Serretiello), E.S. (Emanuela Santoro) and C.D.; supervision, G.F., G.B., P.P. and A.P.; project administration, G.F. and V.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hugonnet, S.; Sax, H.; Eggimann, P.; Chevrolet, J.C.; Pittet, D. Nosocomial bloodstream infection and clinical sepsis. Emerg. Infect. Dis. 2004, 10, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Martinez, R.M.; Wolk, D.M. Bloodstream Infections. Microbiol. Spectr. 2016, 4, 653–689. [Google Scholar] [CrossRef] [PubMed]
- Goto, M.; Al-Hasan, M.N. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2013, 19, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Schechner, V.; Wulffhart, L.; Temkin, E.; Feldman, S.F.; Nutman, A.; Shitrit, P.; Schwaber, M.J.; Carmeli, Y. One-year mortality and years of potential life lost following bloodstream infection among adults: A nation-wide population based study. Lancet Reg. Health–Eur. 2022, 23, 100511. [Google Scholar] [CrossRef]
- Raoofi, S.; Pashazadeh Kan, F.; Rafiei, S.; Hosseinipalangi, Z.; Noorani Mejareh, Z.; Khani, S.; Abdollahi, B.; Seyghalani Talab, F.; Sanaei, M.; Zarabi, F.; et al. Global prevalence of nosocomial infection: A systematic review and meta-analysis. PLoS ONE 2023, 18, e0274248. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità; EpiCentro—L’epidemiologia per la Sanità Pubblica. Rapporto CRE—I Dati 2022. Available online: https://www.epicentro.iss.it/antibiotico-resistenza/cre-dati (accessed on 27 July 2024).
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. Infect. Drug Resist. 2019, 12, 3903–3910. [Google Scholar] [CrossRef]
- Ratia, C.; Soengas, R.G.; Soto, S.M. Gold-Derived Molecules as New Antimicrobial Agents. Front. Microbiol. 2022, 13, 846959. [Google Scholar] [CrossRef]
- del Farmaco, A.I. The Medicines Utilisation Monitoring Centre. In National Report on Antibiotics Use in Italy; Italian Medicines Agency: Rome, Italy, 2024. [Google Scholar]
- Arbune, M.; Gurau, G.; Niculet, E.; Iancu, A.V.; Lupasteanu, G.; Fotea, S.; Vasile, M.C.; Tatu, A.L. Prevalence of Antibiotic Resistance of ESKAPE Pathogens over Five Years in an Infectious Diseases Hospital from South-East of Romania. Infect. Drug Resist. 2021, 14, 2369–2378. [Google Scholar] [CrossRef]
- Rice, L.B. Federal funding for the study of antimicrobial resistance in nosocomial pathogens: No ESKAPE. J. Infect. Dis. 2008, 197, 1079–1081. [Google Scholar] [CrossRef]
- Santajit, S.; Indrawattana, N. Mechanisms of Antimicrobial Resistance in ESKAPE Pathogens. BioMed Res. Int. 2016, 2016, 2475067. [Google Scholar] [CrossRef]
- Marturano, J.E.; Lowery, T.J. ESKAPE Pathogens in Bloodstream Infections Are Associated with Higher Cost and Mortality but Can Be Predicted Using Diagnoses Upon Admission. Open Forum Infect. Dis. 2019, 6, ofz503. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Antimicrobial Resistance Surveillance in Europe. Available online: https://iris.who.int/bitstream/handle/10665/351141/9789289056687-eng.pdf?sequence=1&isAllowed=y (accessed on 26 June 2024).
- European Centre for Disease Prevention and Control. Antimicrobial Resistance (AMR). Available online: https://www.ecdc.europa.eu/en/antimicrobial-resistance (accessed on 26 June 2024).
- European Centre for Disease Prevention and Control. Antimicrobial Resistance Surveillance in Europe 2023–2021 Data. Available online: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistance-surveillance-europe-2023-2021-data (accessed on 26 June 2024).
- Verway, M.; Brown, K.A.; Marchand-Austin, A.; Diong, C.; Lee, S.; Langford, B.; Schwartz, K.L.; MacFadden, D.R.; Patel, S.N.; Sander, B.; et al. Prevalence and Mortality Associated with Bloodstream Organisms: A Population-Wide Retrospective Cohort Study. J. Clin. Microbiol. 2022, 60, e0242921. [Google Scholar] [CrossRef] [PubMed]
- Andrei, A.I.; Popescu, G.A.; Popoiu, M.A.; Mihai, A.; Talapan, D. Changes in Use of Blood Cultures in a COVID-19-Dedicated Tertiary Hospital. Antibiotics 2022, 11, 1694. [Google Scholar] [CrossRef] [PubMed]
- Mormeneo Bayo, S.; Palacian Ruiz, M.P.; Moreno Hijazo, M.; Villuendas Uson, M.C. Bacteremia during COVID-19 pandemic in a tertiary hospital in Spain. Enfermedades Infecc. Microbiol. Clin. 2022, 40, 183–186. [Google Scholar] [CrossRef]
- Uslan, D.Z.; Crane, S.J.; Steckelberg, J.M.; Cockerill, F.R., 3rd; St Sauver, J.L.; Wilson, W.R.; Baddour, L.M. Age- and sex-associated trends in bloodstream infection: A population-based study in Olmsted County, Minnesota. Arch. Intern. Med. 2007, 167, 834–839. [Google Scholar] [CrossRef]
- Mohus, R.M.; Gustad, L.T.; Furberg, A.S.; Moen, M.K.; Liyanarachi, K.V.; Askim, A.; Asberg, S.E.; DeWan, A.T.; Rogne, T.; Simonsen, G.S.; et al. Explaining sex differences in risk of bloodstream infections using mediation analysis in the population-based HUNT study in Norway. Sci. Rep. 2022, 12, 8436. [Google Scholar] [CrossRef]
- Kontula, K.S.K.; Skogberg, K.; Ollgren, J.; Järvinen, A.; Lyytikäinen, O. Population-Based Study of Bloodstream Infection Incidence and Mortality Rates, Finland, 2004–2018. Emerg. Infect. Dis. 2021, 27, 2560–2569. [Google Scholar] [CrossRef]
- Lawry, L.L.; Lugo-Robles, R.; McIver, V. Improvements to a framework for gender and emerging infectious diseases. Bull. World Health Organ. 2021, 99, 682–684. [Google Scholar] [CrossRef]
- Migliore, L.; Nicoli, V.; Stoccoro, A. Gender Specific Differences in Disease Susceptibility: The Role of Epigenetics. Biomedicines 2021, 9, 652. [Google Scholar] [CrossRef]
- Quiros-Roldan, E.; Sottini, A.; Natali, P.G.; Imberti, L. The Impact of Immune System Aging on Infectious Diseases. Microorganisms 2024, 12, 775. [Google Scholar] [CrossRef]
- Leal, H.F.; Azevedo, J.; Silva, G.E.O.; Amorim, A.M.L.; de Roma, L.R.C.; Arraes, A.C.P.; Gouveia, E.L.; Reis, M.G.; Mendes, A.V.; de Oliveira Silva, M.; et al. Bloodstream infections caused by multidrug-resistant gram-negative bacteria: Epidemiological, clinical and microbiological features. BMC Infect. Dis. 2019, 19, 609. [Google Scholar] [CrossRef] [PubMed]
- Licata, F.; Quirino, A.; Pepe, D.; Matera, G.; Bianco, A.; Collaborative, G. Antimicrobial Resistance in Pathogens Isolated from Blood Cultures: A Two-Year Multicenter Hospital Surveillance Study in Italy. Antibiotics 2020, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Santella, B.; Folliero, V.; Pirofalo, G.M.; Serretiello, E.; Zannella, C.; Moccia, G.; Santoro, E.; Sanna, G.; Motta, O.; De Caro, F.; et al. Sepsis-A Retrospective Cohort Study of Bloodstream Infections. Antibiotics 2020, 9, 851. [Google Scholar] [CrossRef] [PubMed]
- Boccella, M.; Santella, B.; Pagliano, P.; De Filippis, A.; Casolaro, V.; Galdiero, M.; Borrelli, A.; Capunzo, M.; Boccia, G.; Franci, G. Prevalence and Antimicrobial Resistance of Enterococcus Species: A Retrospective Cohort Study in Italy. Antibiotics 2021, 10, 1552. [Google Scholar] [CrossRef] [PubMed]
- White, B.P.; Barber, K.E.; Chastain, D.B. Treatment decisions in VRE bacteraemia: A survey of infectious diseases pharmacists. JAC-Antimicrob. Resist. 2023, 5, dlad063. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control European Antimicrobial Resistance Surveillance Network (EARS-Net)—Annual Epidemiological Report for 2022. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/AER-antimicrobial-resistance.pdf (accessed on 26 June 2024).
- Daneman, N.; Fridman, D.; Johnstone, J.; Langford, B.J.; Lee, S.M.; MacFadden, D.M.; Mponponsuo, K.; Patel, S.N.; Schwartz, K.L.; Brown, K.A. Antimicrobial resistance and mortality following E. coli bacteremia. eClinicalMedicine 2023, 56, 101781. [Google Scholar] [CrossRef]
- Stanley, J.; Sullivan, B.; Dowsey, A.W.; Jones, K.; Beck, C.R. Epidemiology of Escherichia coli bloodstream infection antimicrobial resistance trends across South West England during the first 2 years of the coronavirus disease 2019 pandemic response. Clin. Microbiol. Infect. 2024, 30, 1291–1297. [Google Scholar] [CrossRef]
- Afzal, A.; Gutierrez, V.P.; Gomez, E.; Mon, A.M.; Sarmiento, C.M.; Khalid, A.; Polishchuk, S.; Al-Khateeb, M.; Yankulova, B.; Yusuf, M.; et al. Bloodstream infections in hospitalized patients before and during the COVID-19 surge in a community hospital in the South Bronx. Int. J. Infect. Dis. 2022, 116, 43–46. [Google Scholar] [CrossRef]
- AIFA. Agenzia Italiana Del Farmaco Terapia Mirata Delle Infezioni Causate da Batteri Gram Negativi Resistenti a Multipli Antibiotici. Available online: https://www.aifa.gov.it/documents/20142/1787183/AIFA-OPERA_Raccomandazioni_pazienti_ospedalizzati.pdf (accessed on 24 May 2024).
- Gandra, S.; Mojica, N.; Klein, E.Y.; Ashok, A.; Nerurkar, V.; Kumari, M.; Ramesh, U.; Dey, S.; Vadwai, V.; Das, B.R.; et al. Trends in antibiotic resistance among major bacterial pathogens isolated from blood cultures tested at a large private laboratory network in India, 2008–2014. Int. J. Infect. Dis. 2016, 50, 75–82. [Google Scholar] [CrossRef]
- Gebremeskel, L.; Teklu, T.; Kasahun, G.G.; Tuem, K.B. Antimicrobial resistance pattern of Klebsiella isolated from various clinical samples in Ethiopia: A systematic review and meta-analysis. BMC Infect. Dis. 2023, 23, 643. [Google Scholar] [CrossRef]
- Zhen, X.; Stalsby Lundborg, C.; Sun, X.; Hu, X.; Dong, H. Clinical and Economic Impact of Third-Generation Cephalosporin-Resistant Infection or Colonization Caused by Escherichia coli and Klebsiella pneumoniae: A Multicenter Study in China. Int. J. Environ. Res. Public Health 2020, 17, 9285. [Google Scholar] [CrossRef] [PubMed]
- Petrakis, V.; Panopoulou, M.; Rafailidis, P.; Lemonakis, N.; Lazaridis, G.; Terzi, I.; Papazoglou, D.; Panagopoulos, P. The Impact of the COVID-19 Pandemic on Antimicrobial Resistance and Management of Bloodstream Infections. Pathogens 2023, 12, 780. [Google Scholar] [CrossRef] [PubMed]
- Istituto Superiore di Sianità. Rapporto AR-ISS—I Dati 2022. Available online: https://www.epicentro.iss.it/antibiotico-resistenza/ar-iss-rapporto-klebsiella-pneumoniae (accessed on 10 July 2024).
- Tabah, A.; Koulenti, D.; Laupland, K.; Misset, B.; Valles, J.; Bruzzi de Carvalho, F.; Paiva, J.A.; Cakar, N.; Ma, X.; Eggimann, P.; et al. Characteristics and determinants of outcome of hospital-acquired bloodstream infections in intensive care units: The EUROBACT International Cohort Study. Intensive Care Med. 2012, 38, 1930–1945. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Bassetti, M.; Ceccarelli, G.; Carannante, N.; Losito, A.R.; Bartoletti, M.; Corcione, S.; Granata, G.; Santoro, A.; Giacobbe, D.R.; et al. Bloodstream infections caused by carbapenem-resistant Acinetobacter baumannii: Clinical features, therapy and outcome from a multicenter study. J. Infect. 2019, 79, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Bizimungu, O.; Crook, P.; Babane, J.F.; Bitunguhari, L. The prevalence and clinical context of antimicrobial resistance amongst medical inpatients at a referral hospital in Rwanda: A cohort study. Antimicrob. Resist. Infect. Control 2024, 13, 22. [Google Scholar] [CrossRef]
- AIFA, Agenzia Italiana Del Farmaco. AIFA Publishes Recommendations on Targeted Therapy of Resistant Infections. Available online: https://www.aifa.gov.it/en/-/aifa-pubblica-le-raccomandazioni-sulla-terapia-mirata-delle-infezioni-resistenti (accessed on 24 May 2024).
- Serretiello, E.; Manente, R.; Dell’Annunziata, F.; Folliero, V.; Iervolino, D.; Casolaro, V.; Perrella, A.; Santoro, E.; Galdiero, M.; Capunzo, M.; et al. Antimicrobial Resistance in Pseudomonas aeruginosa before and during the COVID-19 Pandemic. Microorganisms 2023, 11, 1918. [Google Scholar] [CrossRef]
- Xia, J.; Lu, L.; Zhao, K.L.; Zeng, Q.L. Resistance Transition of Pseudomonas aeruginosa in SARS-CoV-2-Uninfected Hospitalized Patients in the Pandemic. Infect. Drug Resist. 2023, 16, 6717–6724. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).