
Validity and Reliability of a Questionnaire on Attitudes, Knowledge, and Perceptions of Pharmacy Students Regarding the Training Received on Antibiotics and Antimicrobial Resistance during Their University Studies
 and
and 
Abstract
1. Introduction
2. Results
2.1. Demographic Characteristics of Participants
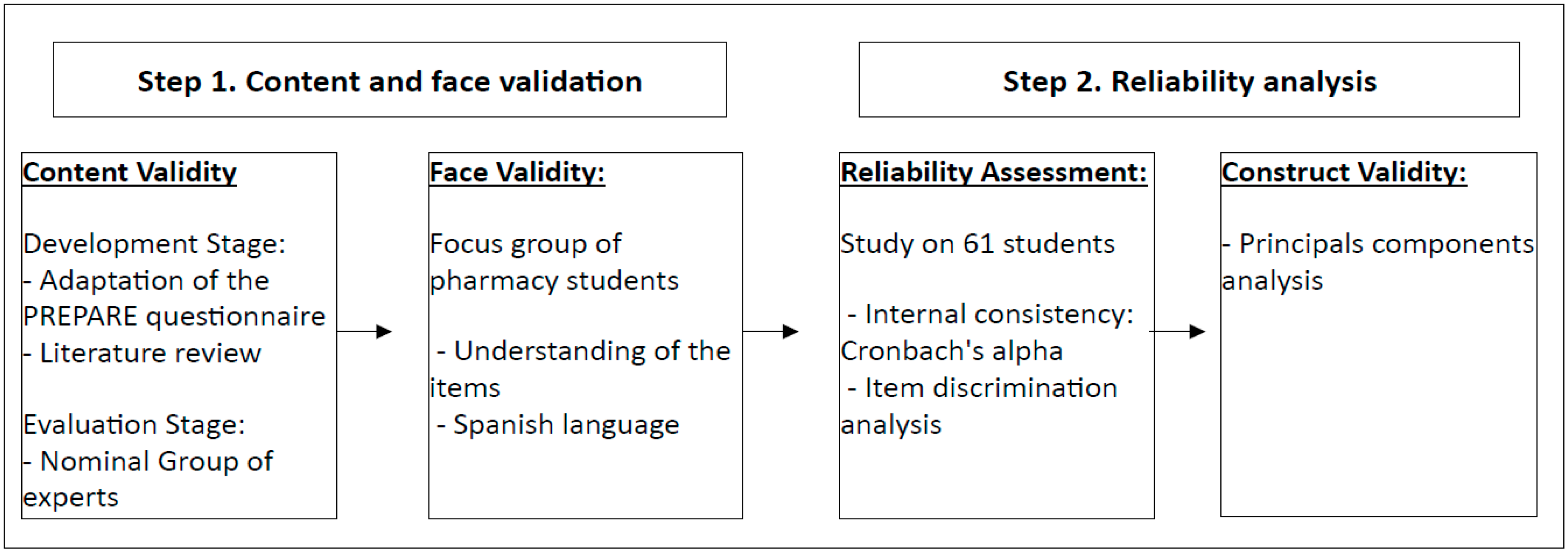
2.2. Validation and Reliability of the Questionnaire
2.3. Exploratory Results of Questionnaire Responses
3. Discussion
Questionnaire Development
4. Materials and Methods
4.1. Study Design, Population, and Sample
4.2. Sample Selection
4.3. Questionnaire Design and Validation Method
4.4. Questionnaire Dissemination
4.5. Statistical Analysis
4.6. Ethical and Legal Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Machowska, A.; Stålsby Lundborg, C. Drivers of Irrational Use of Antibiotics in Europe. Int. J. Environ. Res. Public. Health 2018, 16, 27. [Google Scholar] [CrossRef]
- Lubwama, M.; Onyuka, J.; Ayazika, K.T.; Ssetaba, L.J.; Siboko, J.; Daniel, O.; Mushi, M.F. Knowledge, attitudes, and perceptions about antibiotic use and antimicrobial resistance among final year undergraduate medical and pharmacy students at three universities in East Africa. PLoS ONE 2021, 16, e0251301. [Google Scholar] [CrossRef]
- Yuste, J.R.; Matteo, A.B.; Gruber, F. Impact of Infectious Diseases training in the perception of antibiotic resistance and rational use of antibiotics among Spanish medical students—A cross-sectional study. BMC Med. Educ. 2022, 22, 550. [Google Scholar] [CrossRef]
- Dopelt, K.; Amar, A.; Yonatan, N.; Davidovitch, N. Knowledge, Attitudes, and Practices Regarding Antibiotic Use and Resistance: A Cross-Sectional Study among Students in Israel. Antibiotics 2023, 12, 1028. [Google Scholar] [CrossRef]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- IHME Pathogen Core Group. Global burden associated with 85 pathogens in 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Infect. Dis. 2024, 24, 868–895. [Google Scholar] [CrossRef] [PubMed]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef]
- Pan American Health Organization PAHO/WHO Collaborating Centers. In Proceedings of the 59th Directing Council, 73rd Session of the Regional Committee of WHO for the Americas, Virtual, 20–24 July 2021; Document CD59/INF/6. PAHO: Washington, DC, USA, 2021. Available online: https://www.paho.org/en/governing-bodies/directing-council/59th-directing-council (accessed on 13 June 2024).
- World Health Organization. 118th Session, 11 May 2006, Provisional Agenda Item 5.3, Rational Use of Medicines: Progress in Implementing the WHO Medicines Strategy; WHO: Geneva, Switzerland, 2006; Available online: https://apps.who.int/gb/ebwha/pdf_files/EB118/B118_6-en.pdf (accessed on 13 June 2024).
- World Health Organization. Global Action Plan on Antimicrobial Resistance; WHO: Geneva, Switzerland, 2015; Available online: https://www.who.int/publications/i/item/9789241509763 (accessed on 13 June 2024).
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.; Wertheim, H.F.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic resistance-the need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef]
- World Health Organization. Global Antimicrobial Resistance Surveillance System (GLASS) Report: Early Implementation 2021; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240062702 (accessed on 14 June 2024).
- Vazquez-Lago, J.; Gonzalez-Gonzalez, C.; Zapata-Cachafeiro, M.; Lopez-Vazquez, P.; Taracido, M.; López, A.; Figueiras, A. Knowledge, attitudes, perceptions and habits towards antibiotics dispensed without medical prescription: A qualitative study of Spanish pharmacists. BMJ Open 2017, 7, e015674. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Fabra, D.; Dyar, O.J.; Del Pozo, J.L.; Amiguet, J.A.; Colmenero, J.D.; Fariñas, M.D.C.; López-Medrano, F.; Portilla, J.; Praena, J.; Torre-Cisneros, J.; et al. Perspective of Spanish medical students regarding undergraduate education in infectious diseases, bacterial resistance and antibiotic use. Enferm. Infecc. Microbiol. Clin. 2019, 37, 25–30. [Google Scholar] [CrossRef]
- De Vries, E.; Johnson, Y.; Willems, B.; Bedeker, W.; Ras, T.; Coetzee, R.; Tembo, Y.; Brink, A. Improving primary care antimicrobial stewardship by implementing a peer audit and feedback intervention in Cape Town community healthcare centres. S. Afr. Med. J. 2022, 112, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Lambert, M.; Smit, C.C.H.; De Vos, S.; Benko, R.; Llor, C.; Paget, W.J.; Briant, K.; Pont, L.; Van Dijk, L.; Taxis, K. A systematic literature review and meta-analysis of community pharmacist-led interventions to optimise the use of antibiotics. Br. J. Clin. Pharmacol. 2022, 88, 2617–2641. [Google Scholar] [CrossRef] [PubMed]
- Azechi, T.; Sasano, H.; Sato, K.; Arakawa, R.; Suzuki, K. Evaluation of Knowledge Regarding the Use of Antibiotics among Pharmacy Undergraduates in Japan. J. Microbiol. Biol. Educ. 2022, 23, e00146-22. [Google Scholar] [CrossRef] [PubMed]
- Hayat, K.; Jamshed, S.; Rosenthal, M.; Haq, N.U.; Chang, J.; Rasool, M.F.; Malik, U.R.; Rehman, A.U.; Khan, K.M.; Fang, Y. Understanding of Pharmacy Students towards Antibiotic Use, Antibiotic Resistance and Antibiotic Stewardship Programs: A Cross-Sectional Study from Punjab, Pakistan. Antibiotics 2021, 10, 66. [Google Scholar] [CrossRef]
- Boletín Oficial del Estado. Resolución de 17 de Febrero de 2011, de la Universidad de Santiago de Compostela, por la que se Publica el PLAN de Estudios de Graduado en Farmacia; Boletín Oficial del Estado: Madrid, Spain, 2011; pp. 24400–24403. Available online: https://www.boe.es/diario_boe/txt.php?id=BOE-A-2011-4076 (accessed on 18 July 2024).
- Sociedad Española de Farmacéuticos de Atención Primaria. Cartera de Servicios del Farmacéutico de Atención Primaria; SEFAP: Madrid, Spain, 2017; 34p, Available online: https://www.sefap.org/wp-content/uploads/2018/01/Cartera-Servicios-FAP-Final.pdf (accessed on 18 July 2024).
- Beier, M.E.; Ackerman, P.L. Determinants of Health Knowledge: An Investigation of Age, Gender, Abilities, Personality, and Interests. J. Pers. Soc. Psychol. 2003, 84, 439–448. [Google Scholar] [CrossRef]
- Cheng, C.; Elsworth, G.; Osborne, R.H. Validity Evidence Based on Relations to Other Variables of the eHealth Literacy Questionnaire (eHLQ): Bayesian Approach to Test for Known-Groups Validity. J. Med. Internet Res. 2021, 23, e30243. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net)—Annual Epidemiological Report 2022; ECDC: Stockholm, Sweden, 2023; 27p, Available online: https://www.ecdc.europa.eu/sites/default/files/documents/AER-antimicrobial-consumption.pdf (accessed on 18 July 2024).
- European Centre for Disease Prevention and Control. Antimicrobial Resistance Surveillance in Europe 2023—2021 Data; ECDC: Stockholm, Sweden; WHO: Geneva, Switzerland, 2023; 186p, Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Antimicrobial%20resistance%20surveillance%20in%20Europe%202023%20-%202021%20data.pdf (accessed on 18 July 2024).
- Carretero-Dios, H.; Pérez, C. Normas para el desarrollo y revisión de estudios instrumentales: Consideraciones sobre la selección de tests en la investigación psicológica. Int. Clin. Health Psychol. 2007, 7, 863–882. [Google Scholar]
- Taborda, J.C.M.; Guzmán, J.C.M.; Higuita-Gutiérrez, L.F. Understanding antibiotic knowledge, attitudes, and practices: A cross-sectional study in physicians from a Colombian region, 2023. BMC Med. Educ. 2024, 24, 380. [Google Scholar] [CrossRef]
- Ogoina, D.; Iliyasu, G.; Kwaghe, V.; Otu, A.; Akase, I.E.; Adekanmbi, O.; Mahmood, D.; Iroezindu, M.; Aliyu, S.; Oyeyemi, A.S.; et al. Predictors of antibiotic prescriptions: A knowledge, attitude and practice survey among physicians in tertiary hospitals in Nigeria. Antimicrob. Resist. Infect. Control 2021, 10, 73. [Google Scholar] [CrossRef]
- Ashiru-Oredope, D.; Casale, E.; Harvey, E.; Umoh, E.; Vasandani, S.; Reilly, J.; Hopkins, S. Knowledge and Attitudes about Antibiotics and Antibiotic Resistance of 2404 UK Healthcare Workers. Antibiotics 2022, 11, 1133. [Google Scholar] [CrossRef]
- Lin, L.; Sun, R.; Yao, T.; Zhou, X.; Harbarth, S. Factors influencing inappropriate use of antibiotics in outpatient and community settings in China: A mixed-methods systematic review. BMJ Glob. Health 2020, 5, e003599. [Google Scholar] [CrossRef]
- Teixeira Rodrigues, A.; Ferreira, M.; Roque, F.; Falcão, A.; Ramalheira, E.; Figueiras, A.; Herdeiro, M.T. Physicians’ attitudes and knowledge concerning antibiotic prescription and resistance: Questionnaire development and reliability. BMC Infect. Dis. 2016, 16, 7. [Google Scholar] [CrossRef] [PubMed]
- Baddal, B.; Lajunen, T.J.; Sullman, M.J.M. Knowledge, attitudes and behaviours regarding antibiotics use among Cypriot university students: A multi-disciplinary survey. BMC Med. Educ. 2022, 22, 847. [Google Scholar] [CrossRef]
- Al-Taani, G.M.; Karasneh, R.A.; Al-Azzam, S.; Bin Shaman, M.; Jirjees, F.; Al-Obaidi, H.; Conway, B.R.; Aldeyab, M.A. Knowledge, Attitude, and Behavior about Antimicrobial Use and Resistance among Medical, Nursing and Pharmacy Students in Jordan: A Cross Sectional Study. Antibiotics 2022, 11, 1559. [Google Scholar] [CrossRef] [PubMed]
- Al-Qerem, W.; Hammad, A.; Jarab, A.; MSaleh, M.; Amawi, H.A.; Ling, J.; Alasmari, F. Knowledge, attitudes, and practice with respect to antibiotic use among pharmacy students: A cross-sectional study. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 3408–3418. [Google Scholar] [CrossRef] [PubMed]
- Sakeena, M.H.F.; Bennett, A.A.; Carter, S.J.; McLachlan, A.J. A comparative study regarding antibiotic consumption and knowledge of antimicrobial resistance among pharmacy students in Australia and Sri Lanka. PLoS ONE 2019, 14, e0213520. [Google Scholar] [CrossRef]
- Rusic, D.; Bozic, J.; Vilovic, M.; Bukic, J.; Zivkovic, P.M.; Leskur, D.; Seselja Perisin, A.; Tomic, S.; Modun, D. Attitudes and Knowledge Regarding Antimicrobial Use and Resistance Among Pharmacy and Medical Students at the University of Split, Croatia. Microb. Drug Resist. 2018, 24, 1521–1528. [Google Scholar] [CrossRef]
- Sakeena, M.H.F.; Bennett, A.A.; Jamshed, S.; Mohamed, F.; Herath, D.R.; Gawarammana, I.; McLachlan, A.J. Investigating knowledge regarding antibiotics and antimicrobial resistance among pharmacy students in Sri Lankan universities. BMC Infect. Dis. 2018, 18, 209. [Google Scholar] [CrossRef]
- Ahmad, A.; Khan, M.U.; Patel, I.; Maharaj, S.; Pandey, S.; Dhingra, S. Knowledge, attitude and practice of B.Sc. Pharmacy students about antibiotics in Trinidad and Tobago. J. Res. Pharm. Pract. 2015, 4, 37–41. [Google Scholar] [CrossRef]
- Epstein, J.; Santo, M.R.; Guillemin, F. Cross-cultural adaptation of questionnaires: Review of concepts and current guidelines. J. Clin. Epidemiol. 2015, 68, 435–441. [Google Scholar] [CrossRef]
- Escoffery, C.; Lebow-Skelley, E.; Haardoerfer, R.; Boing, E.; Udelson, H.; Wood, R.; Hartman, M.; Fernandez, M.E.; Mullen, P.D. A systematic review of adaptations of evidence-based public health interventions globally. Implementation Sci. 2018, 13, 125. [Google Scholar] [CrossRef]
- Moore, G.; Campbell, M.; Copeland, L.; Craig, P.; Movsisyan, A.; Hoddinott, P.; Littlecott, H.; O’Cathain, A.; Pfadenhauer, L.; Rehfuess, E. Adapting interventions to new contexts—The ADAPT guidance. BMJ 2021, 374, n1679. [Google Scholar] [CrossRef]
- Bernal, G.; Adames, C. Cultural Adaptations: Conceptual, Ethical, Contextual, and Methodological Issues for Working with Ethnocultural and Majority-World Populations. Prev. Sci. 2017, 18, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.J.; Bowden, S.C.; Byrne, L.K.; Joshua, N.R.; Marx, W.; Weiss, L.G. The cross-cultural generalizability of cognitive ability measures: A systematic literature review. Intelligence 2023, 98, 101751. [Google Scholar] [CrossRef]
- Chen, E.K.; Reid, M.C.; Parker, S.J.; Pillemer, P.K. Tailoring Evidence-Based Interventions for New Populations: A Method for Program Adaptation Through Community Engagement. Eval Health Prof. 2013, 36, 73–92. [Google Scholar] [CrossRef] [PubMed]
- van Alphen, A.; Halfens, R.; Hasman, A.; Imbos, T. Likert or Rasch? Nothing is more applicable than good theory. J. Adv. Nurs. 1994, 20, 196–201. [Google Scholar] [CrossRef]
- Derrick, B.; White, P. Comparing Two Samples from an Individual Likert Question. Int. J. Math. Stat. 2017, 18, 1–13. [Google Scholar]
- Norman, G. Likert scales, levels of measurement and the “laws” of statistics. Adv. Health Sci. Educ. Theory Pract. 2010, 15, 625–632. [Google Scholar] [CrossRef]
- De Von, H.A.; Block, M.E.; Moyle-Wright, P.; Ernst, D.M.; Hayden, S.J.; Lazzara, D.J.; Savoy, S.M.; Kostas-Polston, E. A psychometric toolbox for testing validity and reliability. J. Nurs. Scholarsh. 2007, 39, 155–164. [Google Scholar] [CrossRef]
- Aljefree, N.M.; Almoraie, N.M.; Althaiban, M.A.; Hanbazaza, M.A.; Wazzan, H.A.; Shatwan, I.M. Gender differences in knowledge, attitudes, and practices with respect to type 1 diabetes among Saudi public-school teachers. BMC Public Health 2023, 23, 118. [Google Scholar] [CrossRef]
- Yaghmaie, F. Content validity and its estimation. J. Med. Educ. 2003, 3, 25–27. [Google Scholar]
- Shen, T.; Teo, T.Y.; Yap, J.J.L.; Yeo, K.K. Gender Differences in Knowledge, Attitudes and Practices towards Cardiovascular Disease and its Treatment among Asian Patients. Annals 2017, 46, 20–28. [Google Scholar] [CrossRef]
- Laitner, M.; Erickson, L.; Ortman, E. Understanding the Impact of Sex and Gender in Osteoarthritis: Assessing Research Gaps and Unmet Needs. J. Women’s Health 2020, 30, 634–641. [Google Scholar] [CrossRef]
- Roco Videla, A.; Hernández Orellana, M.; Silva González, O. ¿Cuál es el tamaño muestral adecuado para validar un cuestionario? Nutr. Hosp. 2021, 38, 877–878. [Google Scholar] [CrossRef] [PubMed]
- Johanson, G.A.; Brooks, G.P. Initial Scale Development: Sample Size for Pilot Studies. Educ. Psychol. Meas. 2009, 70, 394–400. [Google Scholar] [CrossRef]
- Alabi, A.T.; Jelili, M.O. Clarifying likert scale misconceptions for improved application in urban studies. Qual. Quant. 2023, 57, 1337–1350. [Google Scholar] [CrossRef]
- Celenza, A.; Rogers, I.R. Comparison of visual analogue and Likert scales in evaluation of an emergency department bedside teaching programme. Emerg. Med. Australas. 2011, 23, 68–75. [Google Scholar] [CrossRef]
- Foley, D.K. Development of a visual analogue scale to measure curriculum outcomes. J. Nurs. Educ. 2008, 47, 209–213. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Guilford, J.P. Psychometric Methods, 2nd ed.; McGraw-Hill: New York, NY, USA, 1954. [Google Scholar]
- Zijlmans, E.A.O.; Tijmstra, J.; van der Ark, L.A.; Sijtsma, K. Item-score reliability in empirical-data sets and its relationship with other item indices. Educ. Psychol. Meas. 2018, 78, 998–1020. [Google Scholar] [CrossRef]
- García de Yébenes Prous, M.J.; Rodríguez Salvanés, F.; Carmona Ortells, L. Validation of questionnaires. Reumatol. Clin. 2009, 5, 171–177. [Google Scholar] [CrossRef]
- University of Santiago de Compostela. Santiago de Compostela: University of Santiago de Compostela. Degree in Pharmacy. Available online: https://www.usc.gal/en/studies/degrees/health-sciences/pharmacy-degree (accessed on 14 June 2024).
- Esteba-Castillo, S.; Torrents-Rodas, D.; García-Alba, J.; Ribas-Vidal, N.; Novell-Alsina, R. Translation and validation of the Spanish version of the Health of the Nation Outcome Scales for People with Learning Disabilities (HoNOS-LD). Rev. Psiquiatr. Salud Ment. 2018, 11, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Efthymiou, P.; Gkentzi, D.; Dimitriou, G. Knowledge, Attitudes and Perceptions of Medical Students on Antimicrobial Stewardship. Antibiotics 2020, 9, 821. [Google Scholar] [CrossRef] [PubMed]
- DeVellis, R.F. Scale Development: Theory and Applications, 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Alumran, A.; Hou, X.Y.; Hurst, C. Validity and reliability of instruments designed to measure factors influencing the overuse of antibiotics. J. Infect. Public Health 2012, 5, 221–232. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Year of Study | n | M | SD | Min | Max |
|---|---|---|---|---|---|
| Second year | 6 | 18.83 | 0.41 | 18 | 19 |
| Third year | 9 | 19.56 | 0.53 | 19 | 20 |
| Fourth year | 16 | 20.88 | 0.5 | 20 | 22 |
| Fifth year | 30 | 23.6 | 4.76 | 21 | 46 |
| Total | 61 | 21.82 | 3.81 | 18 | 46 |
| Item (Variable) | Cronbach’s Alpha If Item Deleted | Homogeneity Index |
|---|---|---|
| Item 7: I feel capable of understanding the motivation for the use of antibiotics in the clinical setting | 0.778 | 0.539 |
| Item 8: I feel capable of working within the multidisciplinary team dedicated to antibiotic management in hospitals | 0.78 | 0.505 |
| Item 9: I feel capable of communicating to patients the needs or limitations of antibiotic use in the clinical setting | 0.772 | 0.611 |
| Item 10: I feel capable of effectively communicating within the multidisciplinary team dedicated to antibiotic management in hospitals | 0.791 | 0.393 |
| Item 11: I feel capable of using knowledge about common antibiotic resistance mechanisms in pathogens | 0.772 | 0.608 |
| Item 12: I feel capable of using knowledge about the epidemiology of bacterial resistance, including local/regional variations | 0.781 | 0.495 |
| Item 13: I feel capable of practicing effective infection control and hygiene (to prevent the spread of bacteria) | 0.784 | 0.453 |
| Item 14: I feel capable of using knowledge about the negative consequences of antibiotic use (bacterial resistance, toxic or adverse effects, cost, Clostridium difficile infections) | 0.779 | 0.528 |
| Item 15: Faculty methodology: lectures with fewer than 15 people | 0.799 | 0.211 |
| Item 16: Faculty methodology: small group teaching | 0.797 | 0.24 |
| Item 17: Faculty methodology: discussion of clinical cases and vignettes | 0.795 | 0.284 |
| Item 18: Faculty methodology: active learning tasks | 0.795 | 0.295 |
| Item 20: Faculty methodology: role playing | 0.801 | 0.171 |
| Item 21: Faculty methodology: rotation in infectious disease units | 0.794 | 0.303 |
| Item 22: Faculty methodology: rotation in microbiology units | 0.802 | 0.186 |
| Item 23: Faculty methodology: tutored or semi-tutored teaching | 0.794 | 0.301 |
| Item 24: In general, do you think you have received sufficient training in the pharmacy faculty on the use of antibiotics? | 0.791 | 0.49 |
| Item 25: Have any of the pharmacy faculty exams included questions about antibiotic treatment? | 0.798 | 0.245 |
| Item (Variable) | Correlation Coefficient | p-Value |
|---|---|---|
| Item 7: I feel capable of understanding the motivation for the use of antibiotics in the clinical setting | 0.628 | <0.01 |
| Item 8: I feel capable of working within the multidisciplinary team dedicated to antibiotic management in hospitals | 0.622 | <0.01 |
| Item 9: I feel capable of communicating to patients the needs or limitations of antibiotic use in the clinical setting | 0.695 | <0.01 |
| Item 10: I feel capable of effectively communicating within the multidisciplinary team dedicated to antibiotic management in hospitals | 0.525 | <0.01 |
| Item 11: I feel capable of using knowledge about common antibiotic resistance mechanisms in pathogens | 0.698 | <0.01 |
| Item 12: I feel capable of using knowledge about the epidemiology of bacterial resistance, including local/regional variations | 0.604 | <0.01 |
| Item 13: I feel capable of practicing effective infection control and hygiene (to prevent the spread of bacteria) | 0.56 | <0.01 |
| Item 14: I feel capable of using knowledge about the negative consequences of antibiotic use (bacterial resistance, toxic or adverse effects, cost, Clostridium difficile infections) | 0.617 | <0.01 |
| Item 15: Faculty methodology: lectures with fewer than 15 people | 0.311 | 0.02 |
| Item 16: Faculty methodology: small group teaching | 0.24 | <0.01 |
| Item 17: Faculty methodology: discussion of clinical cases and vignettes | 0.369 | <0.01 |
| Item 18: Faculty methodology: active learning tasks | 0.356 | <0.01 |
| Item 20: Faculty methodology: role playing | 0.266 | 0.04 |
| Item 21: Faculty methodology: rotation in infectious disease units | 0.4 | <0.01 |
| Item 22: Faculty methodology: rotation in microbiology units | 0.304 | 0.02 |
| Item 23: Faculty methodology: tutored or semi-tutored teaching | 0.38 | <0.01 |
| Item 24: In general, do you think you have received sufficient training in the pharmacy faculty on the use of antibiotics? | 0.525 | <0.01 |
| Item 25: Have any of the pharmacy faculty exams included questions about antibiotic treatment? | 0.284 | 0.03 |
| Item (Variable) | Component | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| Item 21: Faculty methodology: rotation in infectious disease units | 0.73 | 0.55 | |||
| Item 22: Faculty methodology: rotation in microbiology units | 0.79 | ||||
| Item 23: Faculty methodology: tutored or semi-tutored teaching | 0.46 | 0.63 | |||
| Item 15: Faculty methodology: lectures with fewer than 15 people | 0.84 | ||||
| Item 16: Faculty methodology: small group teaching | 0.82 | ||||
| Item 9: I feel capable of communicating to patients the needs or limitations of antibiotic use in the clinical setting | 0.87 | ||||
| Item 13: I feel capable of practicing effective infection control and hygiene (to prevent the spread of bacteria) | 0.83 | ||||
| Item 11: I feel capable of using knowledge about common antibiotic resistance mechanisms in pathogens | 0.84 | ||||
| Item 7: I feel capable of understanding the motivation for the use of antibiotics in the clinical setting | 0.79 | ||||
| Item 14: I feel capable of using knowledge about the negative consequences of antibiotic use (bacterial resistance, toxic or adverse effects, cost, Clostridium difficile infections) | 0.78 | ||||
| Item 8: I feel capable of working within the multidisciplinary team dedicated to antibiotic management in hospitals | 0.82 | ||||
| Item 24: In general, do you think you have received sufficient training in the pharmacy faculty on the use of antibiotics? | −0.67 | ||||
| Item 12: I feel capable of using knowledge about the epidemiology of bacterial resistance, including local/regional variations | 0.73 | ||||
| Item 25: Have any of the pharmacy faculty exams included questions about antibiotic treatment? | −0.68 | ||||
| Item 18: Faculty methodology: active learning tasks | 0.83 | ||||
| Item 10: I feel capable of effectively communicating within the multidisciplinary team dedicated to antibiotic management in hospitals | 0.69 | 0.55 | |||
| Item 17: Faculty methodology: discussion of clinical cases and vignettes | 0.8 | ||||
| Item 20: Faculty methodology: role playing | 0.83 | ||||
| Cronbach’s Alpha | 0.8 | 0.73 | 0.86 | 0.82 | 0.3 |
| Cronbach’s Alpha of the total scale | 0.8 | ||||
| Item (Variable) | M | SD | Agreement (%) | Neutral (%) | Disagreement (%) |
|---|---|---|---|---|---|
| Item 7: I feel capable of understanding the motivation for the use of antibiotics in the clinical setting | 6.3 | 2.3 | 53.3 | 41.7 | 5 |
| Item 8: I feel capable of working within the multidisciplinary team dedicated to antibiotic management in hospitals | 5 | 2.4 | 27.7 | 55.3 | 17 |
| Item 9: I feel capable of communicating to patients the needs or limitations of antibiotic use in the clinical setting | 5.3 | 2.6 | 59.6 | 33.3 | 7 |
| Item 10: I feel capable of effectively communicating within the multidisciplinary team dedicated to antibiotic management in hospitals | 6.6 | 2.2 | 36 | 46 | 18 |
| Item 11: I feel capable of using knowledge about common antibiotic resistance mechanisms in pathogens | 6.1 | 2.4 | 55.2 | 32.8 | 12.1 |
| Item 12: I feel capable of using knowledge about the epidemiology of bacterial resistance, including local/regional variations | 5.2 | 2.4 | 34.5 | 49.1 | 16.4 |
| Item 13: I feel capable of practicing effective infection control and hygiene (to prevent the spread of bacteria) | 6.5 | 2.4 | 58.6 | 31 | 10.3 |
| Item 14: I feel capable of using knowledge about the negative consequences of antibiotic use (bacterial resistance, toxic or adverse effects, cost, Clostridium difficile infections) | 6.6 | 2.2 | 63.2 | 33.3 | 3.5 |
| Item (Variable) | M | SD | Agreement (%) | Neutral (%) | Disagreement (%) |
|---|---|---|---|---|---|
| Item 15: Faculty methodology: lectures with fewer than 15 people | 0.6 | 0.83 | 21.8 | 16.4 | 61.8 |
| Item 16: Faculty methodology: small group teaching | 0.96 | 0.68 | 20.4 | 55.1 | 24.5 |
| Item 17: Faculty methodology: discussion of clinical cases and vignettes | 0.91 | 0.83 | 29.6 | 31.5 | 38.9 |
| Item 18: Faculty methodology: active learning tasks | 1 | 0.67 | 22.2 | 55.6 | 22.2 |
| Item 20: Faculty methodology: role playing | 0.5 | 0.72 | 13 | 24.1 | 63 |
| Item 21: Faculty methodology: rotation in infectious disease units | 0.32 | 0.68 | 11.9 | 8.5 | 79.7 |
| Item 22: Faculty methodology: rotation in microbiology units | 0.54 | 0.73 | 14 | 26.3 | 59.6 |
| Item 23: Faculty methodology: tutored or semi-tutored teaching | 0.37 | 0.7 | 12.3 | 12.3 | 75.4 |
| Item 24: In general, do you think you have received sufficient training in the pharmacy faculty on the use of antibiotics? | 0.55 | 0.89 | 26.7 | 1.7 | 71.7 |
| Item 25: Have any of the pharmacy faculty exams included questions about antibiotic treatment? | 1.5 | 0.87 | 75 | 0 | 25 |
| Item (Variable) | Woman (M ± SD) | Man (M ± SD) | p-Value |
|---|---|---|---|
| Item 7: I feel capable of understanding the motivation for the use of antibiotics in the clinical setting | 6.30 ± 2.15 | 6.35 ± 2.68 | 0.94 |
| Item 8: I feel capable of working within the multidisciplinary team dedicated to antibiotic management in hospitals | 5.07 ± 2.46 | 4.76 ± 2.44 | 0.69 |
| Item 9: I feel capable of communicating to patients the needs or limitations of antibiotic use in the clinical setting | 6.57 ± 2.52 | 6.35 ± 2.37 | 0.75 |
| Item 10: I feel capable of effectively communicating within the multidisciplinary team dedicated to antibiotic management in hospitals | 5.16 ± 2.58 | 5.58 ± 2.59 | 0.58 |
| Item 11: I feel capable of using knowledge about common antibiotic resistance mechanisms in pathogens | 6.11 ± 2.27 | 5.95 ± 2.56 | 0.81 |
| Item 12: I feel capable of using knowledge about the epidemiology of bacterial resistance, including local/regional variations | 5.17 ± 2.35 | 5.32 ± 2.50 | 0.83 |
| Item 13: I feel capable of practicing effective infection control and hygiene (to prevent the spread of bacteria) | 6.53 ± 2.53 | 6.44 ± 2.28 | 0.91 |
| Item 14: I feel capable of using knowledge about the negative consequences of antibiotic use (bacterial resistance, toxic or adverse effects, cost, Clostridium difficile infections) | 6.63 ± 2.24 | 6.63 ± 2.27 | 1 |
| Item 15: Faculty methodology: lectures with fewer than 15 people | 0.42 ± 0.76 | 1.00 ± 0.87 | 0.02 |
| Item 16: Faculty methodology: small group teaching | 0.84 ± 0.72 | 1.18 ± 0.53 | 0.1 |
| Item 17: Faculty methodology: discussion of clinical cases and vignettes | 0.80 ± 0.80 | 0.84 ± 0.72 | 0.2 |
| Item 18: Faculty methodology: active learning tasks | 0.87 ± 0.62 | 1.29 ± 0.73 | 0.05 |
| Item 20: Faculty methodology: role playing | 0.38 ± 0.68 | 0.76 ± 0.75 | 0.07 |
| Item 21: Faculty methodology: rotation in infectious disease units | 0.10 ± 0.44 | 0.79 ± 0.86 | <0.01 |
| Item 22: Faculty methodology: rotation in microbiology units | 0.38 ± 0.60 | 0.89 ± 0.90 | 0.04 |
| Item 23: Faculty methodology: tutored or semi-tutored teaching | 0.20 ± 0.52 | 0.76 ± 0.90 | 0.02 |
| Item 24: In general, do you think you have received sufficient training in the pharmacy faculty on the use of antibiotics? | 0.46 ± 0.84 | 0.74 ± 0.99 | 0.31 |
| Item 25: Have any of the pharmacy faculty exams included questions about antibiotic treatment? | 1.46 ± 0.90 | 1.58 ± 0.84 | 0.64 |
| Item (Variable) | Age Group in Years | Difference of Means | Standard Error | p-Value | |
|---|---|---|---|---|---|
| Item 15: Faculty methodology: lectures with fewer than 15 people | ≤20 | 21–23 | −0.35 | 0.26 | 0.54 |
| >23 | −0.63 | 0.3 | 0.12 | ||
| 21–23 | ≤20 | 0.35 | 0.26 | 0.54 | |
| >23 | −0.28 | 0.28 | 0.94 | ||
| >23 | ≤20 | 0.63 | 0.3 | 0.12 | |
| 21–23 | 0.28 | 0.28 | 0.94 | ||
| Item 16: Faculty methodology: small group teaching | ≤20 | 21–23 | 0.2 | 0.25 | 1 |
| >23 | 0.09 | 0.29 | 1 | ||
| 21–23 | ≤20 | −0.2 | 0.25 | 1 | |
| >23 | −0.11 | 0.25 | 1 | ||
| >23 | ≤20 | −0.09 | 0.29 | 1 | |
| 21–23 | 0.11 | 0.25 | 1 | ||
| Item 17: Faculty methodology: discussion of clinical cases and vignettes | ≤20 | 21–23 | −0.35 | 0.24 | 0.45 |
| >23 | −1.08 | 0.28 | <0.01 | ||
| 21–23 | ≤20 | 0.35 | 0.24 | 0.45 | |
| >23 | −0.74 | 0.26 | 0.02 | ||
| >23 | ≤20 | 1.08 | 0.28 | <0.01 | |
| 21–23 | 0.74 | 0.26 | 0.02 | ||
| Item 18: Faculty methodology: active learning tasks | ≤20 | 21–23 | −0.23 | 0.25 | 1 |
| >23 | −0.26 | 0.28 | 1 | ||
| 21–23 | ≤20 | 0.23 | 0.25 | 1 | |
| >23 | −0.03 | 0.24 | 1 | ||
| >23 | ≤20 | 0.26 | 0.28 | 1 | |
| 21–23 | 0.03 | 0.24 | 1 | ||
| Item 20: Faculty methodology: role playing | ≤20 | 21–23 | −0.14 | 0.21 | 1 |
| >23 | −0.83 | 0.25 | 0.01 | ||
| 21–23 | ≤20 | 0.14 | 0.21 | 1 | |
| >23 | −0.7 | 0.23 | 0.01 | ||
| >23 | ≤20 | 0.83 | 0.25 | 0.01 | |
| 21–23 | 0.7 | 0.23 | 0.01 | ||
| Item 21: Faculty methodology: rotation in infectious disease units | ≤20 | 21–23 | −0.16 | 0.2 | 1 |
| >23 | −0.58 | 0.24 | 0.06 | ||
| 21–23 | ≤20 | 0.16 | 0.2 | 1 | |
| >23 | −0.42 | 0.22 | 0.19 | ||
| >23 | ≤20 | 0.58 | 0.24 | 0.06 | |
| 21–23 | 0.42 | 0.22 | 0.19 | ||
| Item 22: Faculty methodology: rotation in microbiology units | ≤20 | 21–23 | 0.13 | 0.23 | 1 |
| >23 | −0.21 | 0.27 | 1 | ||
| 21–23 | ≤20 | −0.13 | 0.23 | 1 | |
| >23 | −0.34 | 0.25 | 0.52 | ||
| >23 | ≤20 | 0.21 | 0.27 | 1 | |
| 21–23 | 0.34 | 0.25 | 0.52 | ||
| Item 23: Faculty methodology: tutored or semi-tutored teaching | ≤20 | 21–23 | −0.41 | 0.21 | 0.17 |
| >23 | −0.53 | 0.26 | 0.14 | ||
| 21–23 | ≤20 | 0.41 | 0.21 | 0.17 | |
| >23 | −0.12 | 0.23 | 1 | ||
| >23 | ≤20 | 0.53 | 0.26 | 0.14 | |
| 21–23 | 0.12 | 0.23 | 1 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otero-Batán, P.; Lens-Perol, G.; Vázquez-Cancela, O.; Salgado-Barreira, A.; Vazquez-Lago, J.M. Validity and Reliability of a Questionnaire on Attitudes, Knowledge, and Perceptions of Pharmacy Students Regarding the Training Received on Antibiotics and Antimicrobial Resistance during Their University Studies. Antibiotics 2024, 13, 811. https://doi.org/10.3390/antibiotics13090811
Otero-Batán P, Lens-Perol G, Vázquez-Cancela O, Salgado-Barreira A, Vazquez-Lago JM. Validity and Reliability of a Questionnaire on Attitudes, Knowledge, and Perceptions of Pharmacy Students Regarding the Training Received on Antibiotics and Antimicrobial Resistance during Their University Studies. Antibiotics. 2024; 13(9):811. https://doi.org/10.3390/antibiotics13090811
Chicago/Turabian StyleOtero-Batán, Patricia, Guillermo Lens-Perol, Olalla Vázquez-Cancela, Angel Salgado-Barreira, and Juan Manuel Vazquez-Lago. 2024. "Validity and Reliability of a Questionnaire on Attitudes, Knowledge, and Perceptions of Pharmacy Students Regarding the Training Received on Antibiotics and Antimicrobial Resistance during Their University Studies" Antibiotics 13, no. 9: 811. https://doi.org/10.3390/antibiotics13090811
APA StyleOtero-Batán, P., Lens-Perol, G., Vázquez-Cancela, O., Salgado-Barreira, A., & Vazquez-Lago, J. M. (2024). Validity and Reliability of a Questionnaire on Attitudes, Knowledge, and Perceptions of Pharmacy Students Regarding the Training Received on Antibiotics and Antimicrobial Resistance during Their University Studies. Antibiotics, 13(9), 811. https://doi.org/10.3390/antibiotics13090811