
Antimicrobial Susceptibility of Canine and Feline Urinary Tract Infection Pathogens Isolated from Animals with Clinical Signs in European Veterinary Practices during the Period 2013–2018

 ,
,
Abstract
1. Introduction
2. Results
2.1. Isolated Bacteria
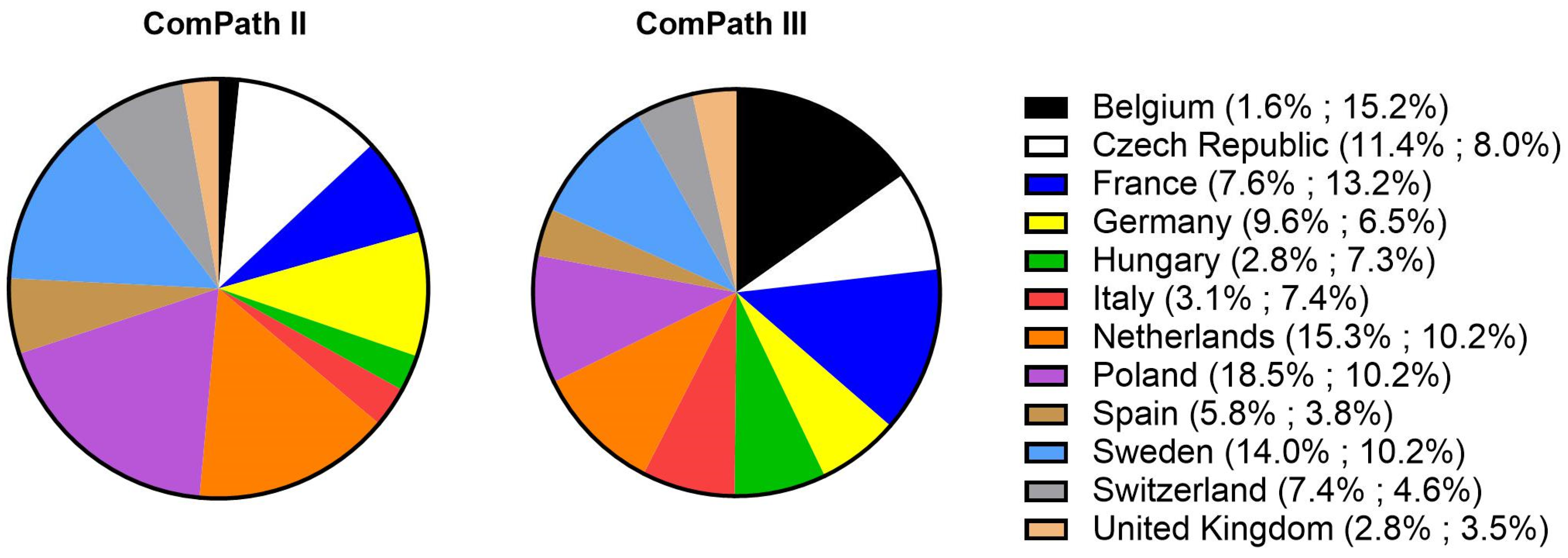
2.1.1. General
2.1.2. Dogs—ComPath II
2.1.3. Cats—ComPath II
2.1.4. Dogs—ComPath III
2.1.5. Cats—ComPath III
2.2. Antimicrobial Susceptibility
2.2.1. Antimicrobial Susceptibility of Gram-Negative Pathogens
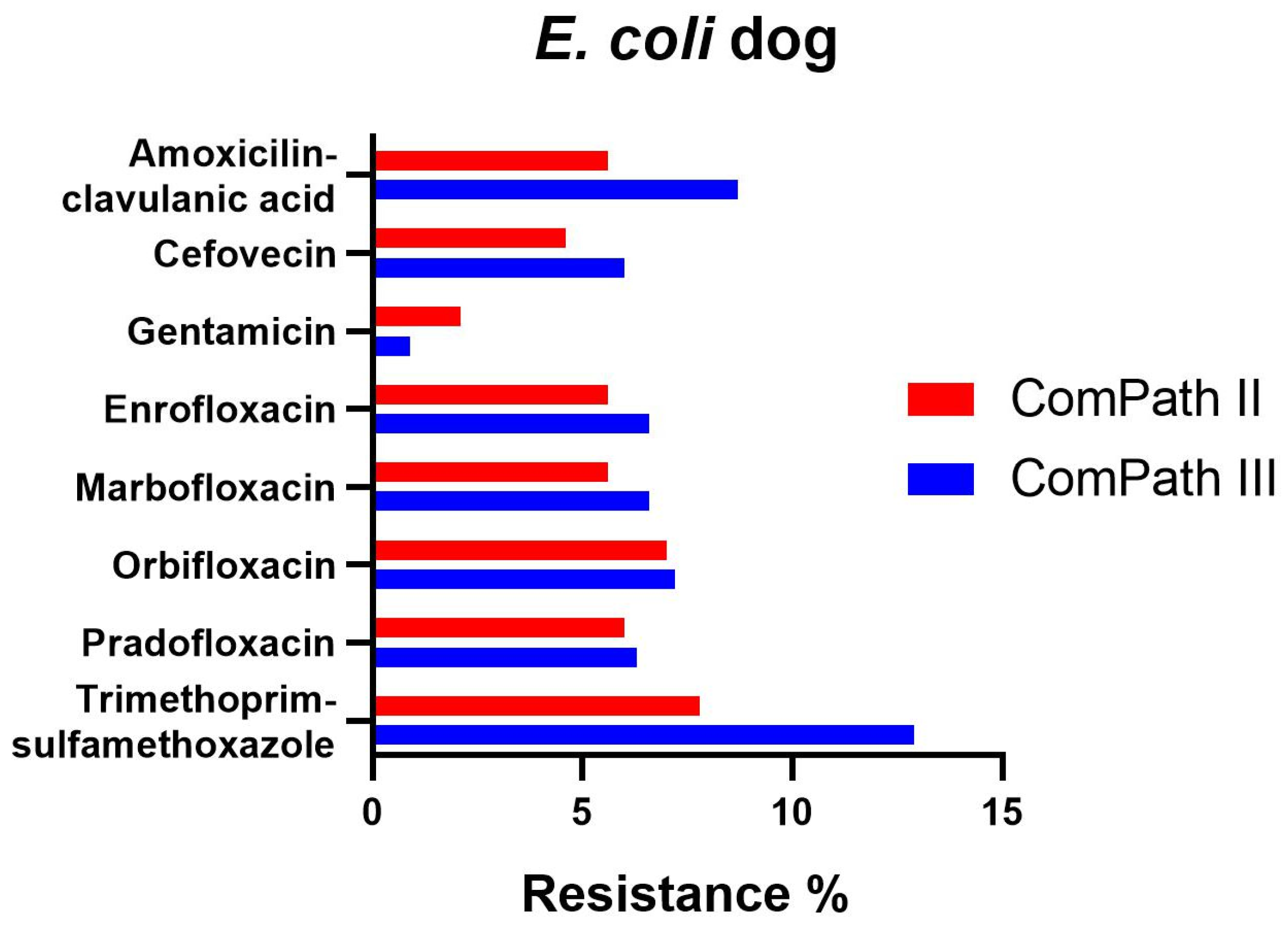
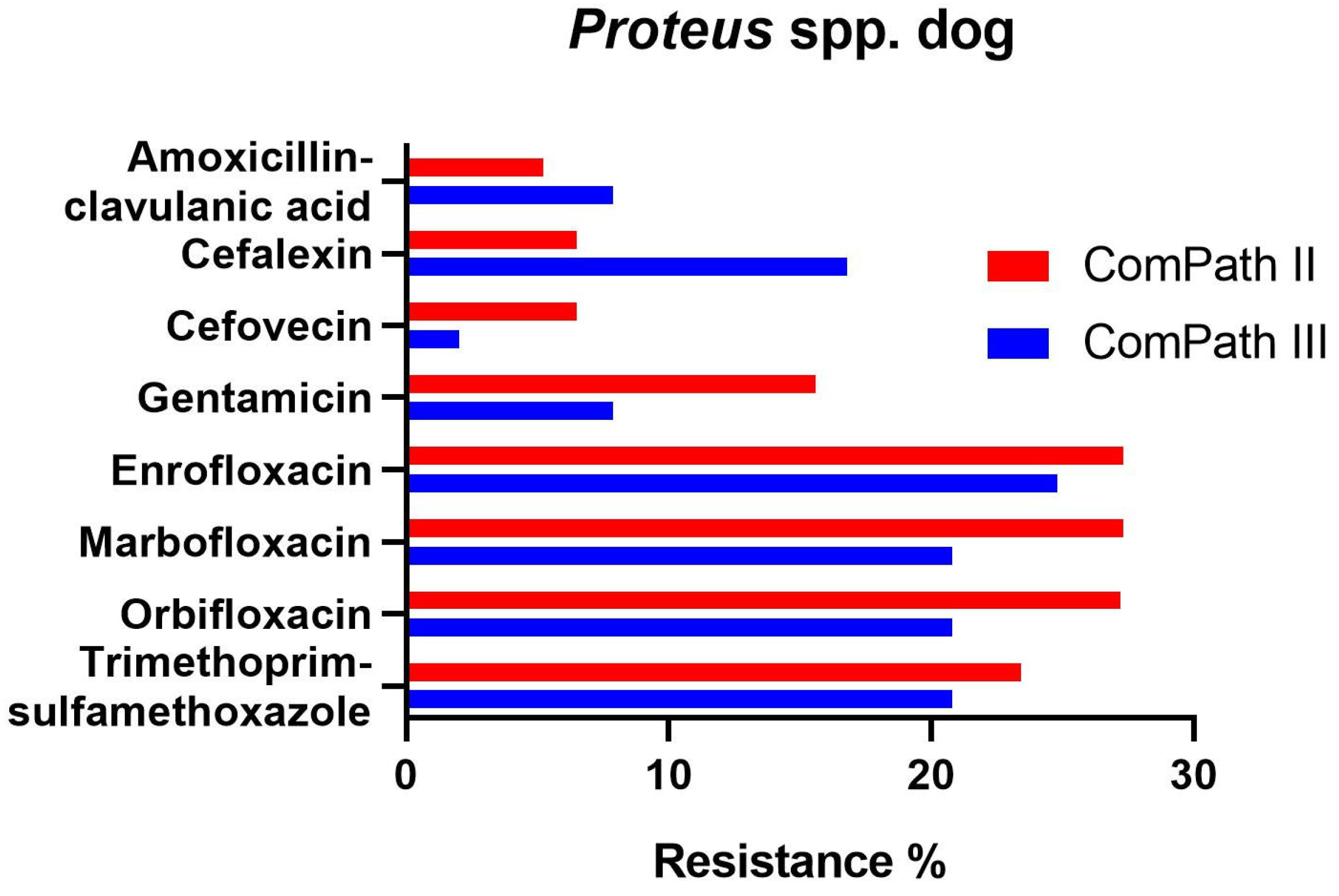
Canine Isolates
Feline Isolates
2.2.2. Antimicrobial Susceptibility of Gram-Positive Pathogens
Canine Isolates
Feline Isolates
2.3. Methicillin-Resistant Staphylococci
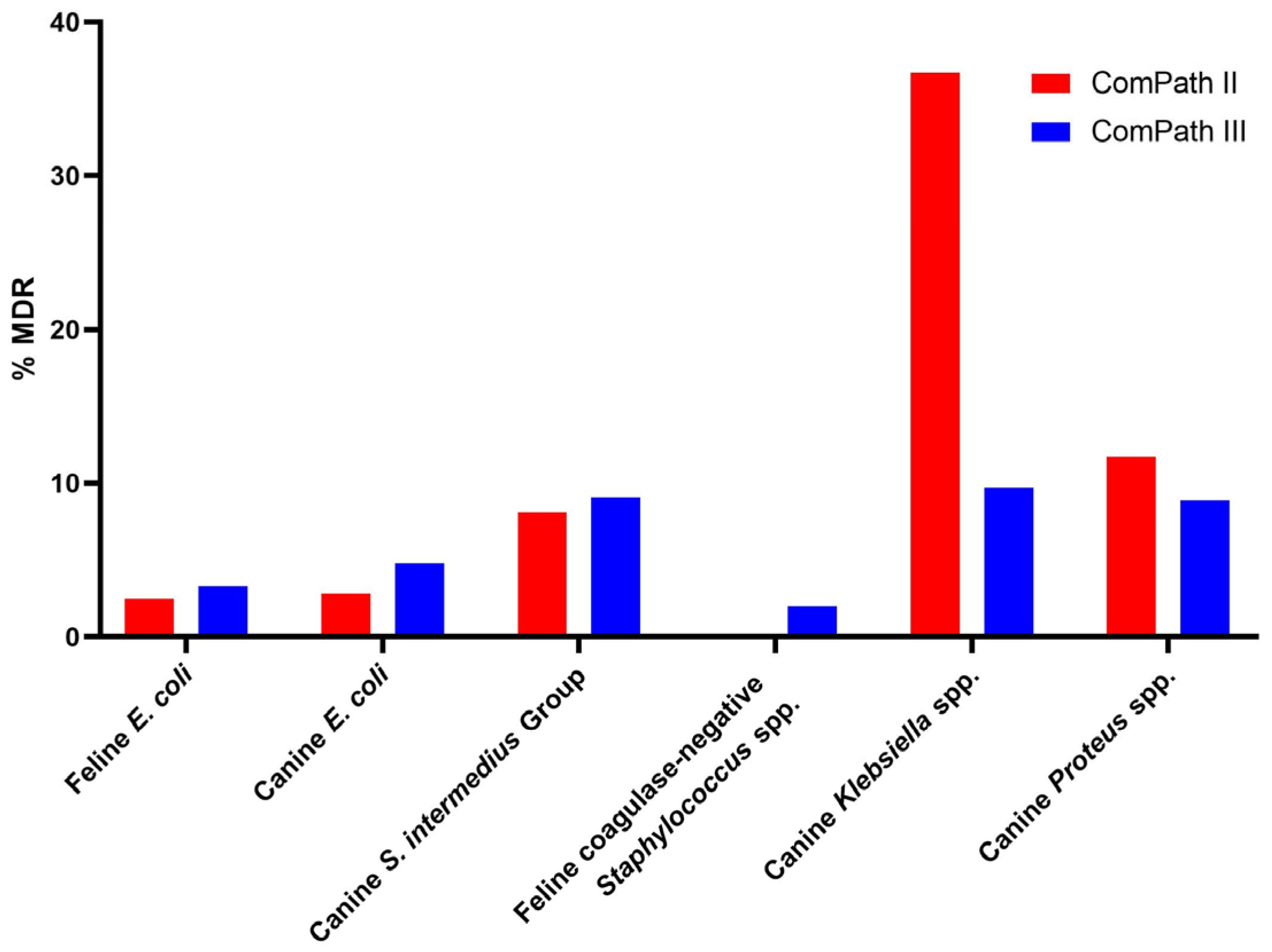
2.4. Multidrug Resistance
3. Discussion
4. Materials and Methods
4.1. Bacterial Collection
4.2. Antimicrobial Susceptibility Testing
4.3. MecA Detection in Staphylococcus spp.
4.4. Data Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnstone, T. A clinical approach to multidrug-resistant urinary tract infection and subclinical bacteriuria in dogs and cats. N. Z. Vet. J. 2020, 68, 69–83. [Google Scholar] [CrossRef] [PubMed]
- Byron, J.K. Urinary Tract Infection. Vet. Clin. Small Anim. Pract. 2019, 49, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Vapalahti, K.; Virtala, A.M.; Joensuu, T.A.; Tiira, K.; Tähtinen, J.; Lohi, H. Health and Behavioral Survey of over 8000 Finnish Cats. Front. Vet. Sci. 2016, 3, 70. [Google Scholar] [CrossRef] [PubMed]
- Weese, J.S.; Blondeau, J.; Boothe, D.; Guardabassi, L.G.; Gumley, N.; Papich, M.; Jessen, L.R.; Lappin, M.; Rankin, S.; Westropp, J.L.; et al. International Society for Companion Animal Infectious Diseases (ISCAID) guidelines for the diagnosis and management of bacterial urinary tract infections in dogs and cats. Vet. J. 2019, 247, 8–25. [Google Scholar] [CrossRef] [PubMed]
- De Briyne, N.; Atkinson, J.; Pokludova, L.; Borriello, S.P.; Price, S. Factors influencing antibiotic prescribing habits and use of sensitivity testing amongst veterinarians in Europe. Vet. Rec. 2013, 173, 475. [Google Scholar] [CrossRef]
- Guardabassi, L.; Schwarz, S.; Lloyd, D.H. Pet animals as reservoirs of antimicrobial-resistant bacteria. J. Antimicrob. Chemother. 2004, 54, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Aslam, B.; Wang, W.; Arshad, M.I.; Khurshid, M.; Muzammil, S.; Rasool, M.H.; Nisar, M.A.; Alvi, R.F.; Aslam, M.A.; Qamar, M.U.; et al. Antibiotic resistance: A rundown of a global crisis. Infect. Drug Resist. 2018, 11, 1645–1658. [Google Scholar] [CrossRef]
- WHO. Global Action Plan on Antimicrobial Resistance; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/bitstream/handle/10665/193736/9789241509763_eng.pdf?sequence=1 (accessed on 27 December 2023).
- Weese, J.S.; Blondeau, J.M.; Boothe, D.; Breitschwerdt, E.B.; Guardabassi, L.; Hillier, A.; Lloyd, D.H.; Papich, M.G.; Rankin, S.C.; Turnidge, J.D.; et al. Antimicrobial Use Guidelines for Treatment of Urinary Tract Disease in Dogs and Cats: Antimicrobial Guidelines Working Group of the International Society for Companion Animal Infectious Diseases. Vet. Med. Int. 2011, 2011, 263768. [Google Scholar] [CrossRef]
- de Jong, A.; Thomas, V.; Klein, U.; Marion, H.; Moyaert, H.; Simjee, S.; Valle, M. Pan-European resistance monitoring programmes encompassing food-borne bacteria and target pathogens of food-producing and companion animals. Int. J. Antimicrob. Agents 2013, 41, 403–409. [Google Scholar] [CrossRef]
- de Jong, A.; Youala, M.; El Garch, F.; Simjee, S.; Rose, M.; Morrissey, I.; Moyaert, H. Antimicrobial susceptibility monitoring of canine and feline skin and ear pathogens isolated from European veterinary clinics: Results of the ComPath Surveillance programme. Vet. Dermatol. 2020, 31, 431. [Google Scholar] [CrossRef]
- Moyaert, H.; Morrissey, I.; de Jong, A.; El Garch, F.; Klein, U.; Ludwig, C.; Thiry, J.; Youala, M. Antimicrobial Susceptibility Monitoring of Bacterial Pathogens Isolated from Urinary Tract Infections in Dogs and Cats Across Europe: ComPath Results. Microb. Drug Resist. 2017, 23, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Mouton, J.W.; Muller, A.E.; Canton, R.; Giske, C.G.; Kahlmeter, G.; Turnidge, J. MIC-based dose adjustment: Facts and fables. J. Antimicrob. Chemother. 2018, 73, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Mader, R.; Damborg, P.; Amat, J.-P.; Bengtsson, B.; Bourély, C.; Broens, E.M.; Busani, L.; Crespo-Robledo, P.; Filippitzi, M.-E.; Fitzgerald, W.; et al. Building the European Antimicrobial Resistance Surveillance network in veterinary medicine (EARS-Vet). Eurosurveillance 2021, 26, 2001359. [Google Scholar] [CrossRef]
- Madhaiyan, M.; Wirth, J.S.; Saravanan, V.S. Phylogenomic analyses of the Staphylococcaceae family suggest the reclassification of five species within the genus Staphylococcus as heterotypic synonyms, the promotion of five subspecies to novel species, the taxonomic reassignment of five Staphylococcus species to Mammaliicoccus gen. nov., and the formal assignment of Nosocomiicoccus to the family Staphylococcaceae. Int. J. Syst. Evol. Microbiol. 2020, 70, 5926–5936. [Google Scholar] [CrossRef] [PubMed]
- Marques, C.; Belas, A.; Franco, A.; Aboim, C.; Gama, L.T.; Pomba, C. Increase in antimicrobial resistance and emergence of major international high-risk clonal lineages in dogs and cats with urinary tract infection: 16 year retrospective study. J. Antimicrob. Chemother. 2018, 73, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Garcês, A.; Lopes, R.; Silva, A.; Sampaio, F.; Duque, D.; Brilhante-Simões, P. Bacterial Isolates from Urinary Tract Infection in Dogs and Cats in Portugal, and Their Antibiotic Susceptibility Pattern: A Retrospective Study of 5 Years (2017–2021). Antibiotics 2022, 11, 1520. [Google Scholar] [CrossRef] [PubMed]
- Smoglica, C.; Evangelisti, G.; Fani, C.; Marsilio, F.; Trotta, M.; Messina, F.; Di Francesco, C.E. Antimicrobial Resistance Profile of Bacterial Isolates from Urinary Tract Infections in Companion Animals in Central Italy. Antibiotics 2022, 11, 1363. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Wang, Y.; Chen, Y.; Huang, M.; Wang, Y.; Shen, Z.; Xia, Z.; Li, G. Antimicrobial resistance of bacterial pathogens isolated from canine urinary tract infections. Vet. Microbiol. 2020, 241, 8540. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.; Epstein, S.E.; Westropp, J.L. Antimicrobial Susceptibility Patterns in Urinary Tract Infections in Dogs (2010–2013). J. Vet. Intern. Med. 2015, 29, 1045–1052. [Google Scholar] [CrossRef]
- Yudhanto, S.; Hung, C.C.; Maddox, C.W.; Varga, C. Antimicrobial Resistance in Bacteria Isolated from Canine Urine Samples Submitted to a Veterinary Diagnostic Laboratory, Illinois, United States. Front. Vet. Sci. 2022, 9, 867784. [Google Scholar] [CrossRef]
- Roberts, M.; White, J.; Lam, A. Prevalence of bacteria and changes in trends in antimicrobial resistance of Escherichia coli isolated from positive canine urinary samples from an Australian referral hospital over a 5-year period (2013–2017). Vet. Rec. Open 2019, 6, e000345. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, J.D.; Mavrides, D.E.; Graham, P.A.; McHugh, T.D. Results of urinary bacterial cultures and antibiotic susceptibility testing of dogs and cats in the UK. J. Small Anim. Pract. 2021, 62, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Darwich, L.; Seminati, C.; Burballa, A.; Nieto, A.; Duran, I.; Tarradas, N.; Molina-Lopez, R.A. Antimicrobial susceptibility of bacterial isolates from urinary tract infections in companion animals in Spain. Vet. Rec. 2021, 188, e60. [Google Scholar] [CrossRef] [PubMed]
- Litster, A.; Moss, S.M.; Honnery, M.; Rees, B.; Trott, D.J. Prevalence of bacterial species in cats with clinical signs of lower urinary tract disease: Recognition of Staphylococcus felis as a possible feline urinary tract pathogen. Vet. Microbiol. 2007, 121, 182–188. [Google Scholar] [CrossRef] [PubMed]
- BVL. GERM-VET: Bericht zur Resistenzmonitoringstudie 2021-Resistenzsituation bei Klinisch Wichtigen Tierpathogenen Bakterien. Germany. 2021. Available online: https://www.bvl.bund.de/DE/Arbeitsbereiche/09_Untersuchungen/01_Aufgaben/03_Nationales-Resistenz-Monitoring/untersuchungen_NatResistenzmonitoring_node.html (accessed on 16 January 2024).
- Swedres-Svarm. Sales of Antibiotics and Occurrence of Antibiotic Resistance in Sweden. 2022. Solna/Uppsala ISSN2001-7901. Available online: https://www.folkhalsomyndigheten.se/publikationer-och-material/publikationsarkiv/s/swedres-svarm-2022/ (accessed on 16 January 2024).
- Anses. Resapath-French Surveillance Network for Antimicrobial Resistance in Bacteria from Diseased Animals. 2022 Annual Report. Lyon et Ploufragan-Plouzané-Niort, France, November 2023, Report, 53. Available online: https://anses.fr/en/content/anses-request-based-opinions-and-reports (accessed on 16 January 2024).
- KuKanich, K.; Lubbers, B.; Salgado, B. Amoxicillin and amoxicillin-clavulanate resistance in urinary Escherichia coli antibiograms of cats and dogs from the Midwestern United States. J. Vet. Intern. Med. 2020, 34, 227–231. [Google Scholar] [CrossRef] [PubMed]
- KuKanich, K.; Woodruff, K.; Bieberly, Z.; Papich, M.G.; KuKanich, B. Evaluation of urine concentrations of amoxicillin and clavulanate in cats. J. Vet. Intern. Med. 2021, 35, 456–461. [Google Scholar] [CrossRef]
- Meletis, G.; Bagkeri, M. Pseudomonas aeruginosa: Multi-Drug-Resistance Development and Treatment Options. In Infection Control; IntechOpen: London, UK, 2013. [Google Scholar] [CrossRef]
- Pang, Z.; Raudonis, R.; Glick, B.R.; Lin, T.-J.; Cheng, Z. Antibiotic resistance in Pseudomonas aeruginosa: Mechanisms and alternative therapeutic strategies. Biotechnol. Adv. 2019, 37, 177–192. [Google Scholar] [CrossRef] [PubMed]
- Köhler, T.; Kok, M.; Michea-Hamzehpour, M.; Plesiat, P.; Gotoh, N.; Nishino, T.; Curty, L.K.; Pechere, J.C. Multidrug efflux in intrinsic resistance to trimethoprim and sulfamethoxazole in Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 1996, 40, 2288–2290. [Google Scholar] [CrossRef]
- NORM/NORM-VET. Usage of Antimicrobial Agents and Occurrence of Antimicrobial Resistance in Norway—2021. 2022. Available online: https://www.fhi.no/en/publ/2022/norm-og-norm-vet-usage-of-antimicrobial-agents-and-occurrence-of-antimicrob/ (accessed on 16 January 2024).
- Pepin-Puget, L.; El Garch, F.; Bertrand, X.; Valot, B.; Hocquet, D. Genome analysis of enterobacteriaceae with non-wild type susceptibility to third-generation cephalosporins recovered from diseased dogs and cats in Europe. Vet. Microbiol. 2020, 242, 108601. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Disk and Dilution Susceptibility Tests for Bacteria Isolated from Animals, 7th ed.; CLSI Supplement VET01S; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2024. [Google Scholar]
- Papich, M.G.; Gunnett, L.A.; Lubbers, B.V. Revision of fluoroquinolone breakpoints used for interpretation of antimicrobial susceptibility testing of canine bacterial isolates. Am. J. Vet. Res. 2023, 84, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Turnidge, J.; Paterson, D.L. Setting and Revising Antibacterial Susceptibility Breakpoints. Clin. Microbiol. Rev. 2007, 20, 391–408. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Development of Quality Control Ranges, Breakpoints, and Interpretive Categories for Antimicrobial Agents Used in Veterinary Medicine, 4th ed.; CLSI guideline VET02; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2021. [Google Scholar]
- Toutain, P.L.; Bousquet-Melou, A.; Damborg, P.; Ferran, A.A.; Mevius, D.; Pelligand, L.; Veldman, K.T.; Lees, P. En Route towards European Clinical Breakpoints for Veterinary Antimicrobial Susceptibility Testing: A Position Paper Explaining the VetCAST Approach. Front. Microbiol. 2017, 8, 2344. [Google Scholar] [CrossRef] [PubMed]
- Pelligand, L.; Lees, P.; Sidhu, P.K.; Toutain, P.-L. Semi-Mechanistic Modeling of Florfenicol Time-Kill Curves and in silico Dose Fractionation for Calf Respiratory Pathogens. Front. Microbiol. 2019, 10, 1237. [Google Scholar] [CrossRef]
- EUCAST. New Definitions of S, I and R from 2019. Available online: https://www.eucast.org/newsiandr (accessed on 31 January 2023).
- Hollenbeck, B.L.; Rice, L.B. Intrinsic and acquired resistance mechanisms in enterococcus. Virulence 2012, 3, 421–433. [Google Scholar] [CrossRef] [PubMed]
- Zervos, M.J.; Schaberg, D.R. Reversal of the in vitro susceptibility of enterococci to trimethoprim-sulfamethoxazole by folinic acid. Antimicrob. Agents Chemother. 1985, 28, 446–448. [Google Scholar] [CrossRef] [PubMed]
- Grayson, M.L.; Thauvin-Eliopoulos, C.; Eliopoulos, G.M.; Yao, J.D.; Deangelis, D.V.; Walton, L.; Woolley, J.L.; Moellering, R.C. Failure of trimethoprim-sulfamethoxazole therapy in experimental enterococcal endocarditis. Antimicrob. Agents Chemother. 1990, 34, 1792–1794. [Google Scholar] [CrossRef]
- Chew, D.J. Diagnosis and Treatment of Simple and Recurrent Urinary Tract Infections. In Proceedings of the WSAVA/FECAVA/BSAVA World Congress 2012, Birmingham, UK, 11–15 April 2012. [Google Scholar]
- Kraszewska, Z.; Skowron, K.; Kwiecińska-Piróg, J.; Grudlewska-Buda, K.; Przekwas, J.; Wiktorczyk-Kapischke, N.; Wałecka-Zacharska, E.; Gospodarek-Komkowska, E. Antibiotic Resistance of Enterococcus spp. Isolated from the Urine of Patients Hospitalized in the University Hospital in North-Central Poland, 2016–2021. Antibiotics 2022, 11, 1749. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.T.; Lubbers, B.V.; Schwarz, S.; Watts, J.L. Applying definitions for multidrug resistance, extensive drug resistance and pandrug resistance to clinically significant livestock and companion animal bacterial pathogens. J. Antimicrob. Chemother. 2018, 73, 1460–1463. [Google Scholar] [CrossRef]
- Toutain, P.L.; Sidhu, P.K.; Lees, P.; Rassouli, A.; Pelligand, L. VetCAST Method for Determination of the Pharmacokinetic-Pharmacodynamic Cut-Off Values of a Long-Acting Formulation of Florfenicol to Support Clinical Breakpoints for Florfenicol Antimicrobial Susceptibility Testing in Cattle. Front. Microbiol. 2019, 10, 1310. [Google Scholar] [CrossRef]
- Lallemand, E.A.; Bousquet-Mélou, A.; Chapuis, L.; Davis, J.; Ferran, A.A.; Kukanich, B.; Kuroda, T.; Lacroix, M.Z.; Minamijima, Y.; Olsén, L.; et al. Pharmacokinetic–pharmacodynamic cutoff values for benzylpenicillin in horses to support the establishment of clinical breakpoints for benzylpenicillin antimicrobial susceptibility testing in horses. Front. Microbiol. 2023, 14, 1282949. [Google Scholar] [CrossRef] [PubMed]
- Mader, R.; Eu, J.; Bourely, C.; Amat, J.P.; Broens, E.M.; Busani, L.; Callens, B.; Crespo-Robledo, P.; Damborg, P.; Filippitzi, M.E.; et al. Defining the scope of the European Antimicrobial Resistance Surveillance network in Veterinary medicine (EARS-Vet): A bottom-up and One Health approach. J. Antimicrob. Chemother. 2022, 77, 816–826. [Google Scholar] [CrossRef] [PubMed]
- Kahlmeter, G.; Brown, D.F.J.; Goldstein, F.W.; MacGowan, A.P.; Mouton, J.W.; Osterlund, A.; Rodloff, A.; Steinbakk, M.; Urbaskova, P.; Vaopoulos, A. European harmonization of MIC breakpoints for antimicrobial susceptibility testing of bacteria. J. Antimicrob. Chemother. 2003, 52, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Kahlmeter, G.; Turnidge, J. How to: ECOFFs-the why, the how, and the don’ts of EUCAST epidemiological cutoff values. Clin. Microbiol. Infect. 2022, 28, 952–954. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Performance Standards for Antimicrobial Disk and Dilution Susceptibility Tests for Bacteria Isolated from Animals, 5th ed.; CLSI Standard VET01; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- Zhang, K.; McClure, J.A.; Conly, J.M. Enhanced multiplex PCR assay for typing of staphylococcal cassette chromosome mec types I to V in methicillin-resistant Staphylococcus aureus. Mol. Cell. Probes 2012, 26, 218–221. [Google Scholar] [CrossRef] [PubMed]
- EFSA; ECDC. The European Union Summary Report on Antimicrobial Resistance in zoonotic and indicator bacteria from humans, animals and food in 2018/2019. EFSA J. 2021, 19, e06490. [Google Scholar] [CrossRef]
- De Jong, A.; Youala, M.; Klein, U.; El Garch, F.; Simjee, S.; Moyaert, H.; Rose, M.; Gautier-Bouchardon, A.V.; Catania, S.; Ganapathy, K.; et al. Minimal inhibitory concentration of seven antimicrobials to Mycoplasma gallisepticum and Mycoplasma synoviae isolates from six European countries. Avian Pathol. 2021, 50, 161–173. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Escherichia coli (Dog, n = 284/Cat, n = 161) | Proteus spp. (Dog, n = 77) | Pseudomonas spp. (Dog, n = 18) | Klebsiella spp. (Dog, n = 30) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial Agent | S (%) | I (%) | R (%) | MIC50 | MIC90 | S (%) | I (%) | R (%) | MIC50 | MIC90 | S (%) | I (%) | R (%) | MIC50 | MIC90 | S (%) | I (%) | R (%) | MIC50 | MIC90 |
| Amoxicillin | 4/4 | >64/>64 | 2 | >64 | >64 | >64 | >64 | >64 | ||||||||||||
| Amoxicillin- clavulanic acid (2:1) | 94.4/94.4 | 0/0 | 5.6/5.6 | 4/4 | 8/8 | 94.8 | 0 | 5.2 | 2 | 4 | >32 | >32 | 90.0 | 0 | 10.0 | 2 | 8 | |||
| Cefadroxil | 8/8 | 16/16 | 16 | 16 | >32 | >32 | 8 | >32 | ||||||||||||
| Cefalexin | 94.7/94.4 | 0/0 | 5.3/5.6 | 8/8 | 8/8 | 93.5 | 0 | 6.5 | 16 | 16 | >32 | >32 | 60.0 | 0 | 40.0 | 8 | >32 | |||
| Cefovecin | 92.6/93.2 | 2.8/2.5 | 4.6/4.3 | 1/1 | 2/1 | 93.5 | 0 | 6.5 | 0.5 | 0.5 | >32 | >32 | 1 | >32 | ||||||
| Cephalothin | 8/8 | 16/16 | 4 | 8 | >64 | >64 | 4 | >64 | ||||||||||||
| Gentamicin (* for cats) | 97.5/98.8 | 0.4/0 | 2.1/1.2 | 1/1 | 1/1 | 81.8 | 2.6 | 15.6 | 0.5 | 8 | 88.9 | 11.1 | 0.0 | 2 | 4 | 70.0 | 0 | 30.0 | 0.5 | >32 |
| Neomycin | 2/2 | 2/2 | 2 | 16 | 8 | 32 | 1 | 16 | ||||||||||||
| Enrofloxacin | 88.0 | 2.8 | 9.2 | 0.03/0.03 | 0.25/0.5 | 1.3 | 71.4 | 27.3 | 0.25 | >8 | 0 | 0 | 100 | 1 | >8 | 53.3 | 0 | 46.7 | 0.06 | >8 |
| Marbofloxacin | 89.4 | 1.4 | 9.2 | 0.03/0.03 | 0.25/0.5 | 71.4 | 1.3 | 27.3 | 0.12 | 4 | 0 | 22.2 | 77.8 | 0.5 | 2 | 53.3 | 0 | 46.7 | 0.06 | >8 |
| Orbifloxacin | 91.2 | 1.8 | 7.0 | 0.12/0.12 | 0.5/2 | 42.9 | 29.9 | 27.2 | 2 | >16 | 4 | 8 | 53.3 | 3.3 | 43.4 | 0.25 | >16 | |||
| Pradofloxacin | 93.3 | 0.7 | 6.0 | 0.03/0.03 | 0.12/0.25 | 0.25 | 8 | 0.5 | 2 | 0.06 | 4 | |||||||||
| Trimethoprim- sulfamethoxazole (1:19) * | 92.3/87.0 | 0/0 | 7.8/13.0 | 0.25/0.12 | 2/>8 | 76.6 | 0 | 23.4 | 0.25 | >8 | 8 | >8 | 66.7 | 0 | 33.3 | 0.5 | >8 | |||
| Escherichia coli (Dog, n = 333/Cat, n = 183) | Proteus spp. (Dog, n = 101/Cat, n = 20) | Pseudomonas spp. (Dog, n = 22/Cat, n = 16) | Klebsiella spp. (Dog, n = 31) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial Agent | S (%) | I (%) | R (%) | MIC50 | MIC90 | S (%) | I (%) | R (%) | MIC50 | MIC90 | S (%) | I (%) | R (%) | MIC50 | MIC90 | S (%) | I (%) | R (%) | MIC50 | MIC90 |
| Amoxicillin | 4/4 | >64/>64 | 1/2 | >64/>64 | >64/>64 | >64/>64 | >64 | >64 | ||||||||||||
| Amoxicillin- clavulanic acid (2:1) | 91.3/90.7 | 0/0 | 8.7/9.3 | 4/4 | 8/8 | 92.1/85.0 | 0/0 | 7.9/15.0 | 1/1 | 8/>32 | >32/>32 | >32/>32 | 93.5 | 0 | 6.5 | 2 | 8 | |||
| Cefadroxil | 8/8 | 16/16 | 16/16 | 32/>32 | >32/>32 | >32/>32 | 8 | 16 | ||||||||||||
| Cefalexin | 94.9/92.9 | 0/0 | 5.1/7.1 | 8/8 | 16/16 | 83.2/65.0 | 0/0 | 16.8/35.0 | 16/16 | 32/>32 | >32/>32 | >32/>32 | 90.3 | 0 | 9.7 | 4 | 16 | |||
| Cefovecin | 94.3/93.4 | 1.2/0.6 | 4.5/6.0 | 1/1 | 2/2 | 98.0/85.0 | 0/0 | 2.0/15.0 | 0.25/0.25 | 0.5/>32 | >32/>32 | >32/>32 | 0.5 | 2 | ||||||
| Cephalothin | 8/8 | 32/32 | 4/4 | 16/>64 | >64/>64 | >64/>64 | 4 | 16 | ||||||||||||
| Doxycycline (* for cats) | 0/86.9 | 1.2/3.8 | 98.8/9.3 | 2/1 | 16/8 | 0/10.0 | 0/0 | 100.0/90.0 | 64/32 | >64/64 | 16/16 | 64/32 | 0 | 0 | 100 | 2 | 2 | |||
| Gentamicin (* for cats) | 98.8/98.9 | 0.3/0 | 0.9/1.1 | 0.5/0.5 | 1/1 | 90.1/90.0 | 2.0/0 | 7.9/10.0 | 1/0.5 | 2/4 | 90.9 | 9.1 | 0 | 2/2 | 4/2 | 93.6 | 3.2 | 3.2 | 0.25 | 0.5 |
| Neomycin | 1/1 | 2/2 | 2/2 | 32/8 | 8/8 | 32/16 | 1 | 1 | ||||||||||||
| Enrofloxacin | 84.7 | 4.8 | 10.5 | 0.03/0.03 | 0.5/0.06 | 8.9 | 66.3 | 24.8 | 0.12/0.12 | 8/1 | 0 | 0 | 100 | 1/1 | 4/1 | 77.4 | 9.7 | 12.9 | 0.06 | 1 |
| Marbofloxacin | 86.8 | 1.8 | 11.4 | 0.03/0.03 | 0.5/0.06 | 79.2 | 0 | 20.8 | 0.06/0.03 | 2/0.25 | 0 | 18.2 | 81.8 | 0.5/0.5 | 2/1 | 87.1 | 0 | 12.9 | 0.03 | 1 |
| Orbifloxacin | 89.5 | 3.3 | 7.2 | 0.12/0.06 | 2/0.25 | 75.3 | 4.0 | 20.8 | 1/0.5 | >16/8 | 4/4 | 16/8 | 87.1 | 3.2 | 9.7 | 0.12 | 4 | |||
| Pradofloxacin | 92.5 | 1.2 | 6.3 | 0.015/0.015 | 0.12/0.03 | 0.12/0.12 | 4/1 | 0.5/0.5 | 4/1 | 0.03 | 0.25 | |||||||||
| Trimethoprim- sulfamethoxazole (1:19) * | 87.1/92.3 | 0/0 | 12.9/7.7 | 0.06/0.06 | >16/0.5 | 79.2/75.0 | 0/0 | 20.8/25.0 | 0.12/0.12 | >16/>16 | 8/8 | >16/16 | 90.3 | 0 | 9.7 | 0.12 | 2 | |||
| Staphylococcus intermedius Group (Dog, n = 86/Cat, n = 20) | Streptococcus spp. (Dog, n = 53) | Enterococcus spp. (Dog, n = 49)/Cat, n = 36) | Coagulase-Negative Staphylococci (Cat, n = 38) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial Agent | S (%) | I (%) | R (%) | MIC50 | MIC90 | S (%) | I (%) | R (%) | MIC50 | MIC90 | S (%) | I (%) | R (%) | MIC50 | MIC90 | S (%) | I (%) | R (%) | MIC50 | MIC90 |
| Amoxicillin | 0.25/0.12 | 0.25/2 | ≤0.015 | 0.03 | 1/1 | >64/1 | 0.12 | 0.5 | ||||||||||||
| Amoxicillin-clavulanic acid (2:1) | 91.9/85 | 2.3/5.0 | 5.8/10.0 | 0.12/0.12 | 0.12/0.5 | ≤0.015 | 0.03 | 85.7/100 | 0/0 | 14.3/0 | 1/1 | >32/1 | 89.5 | 10.5 | 0 | 0.12 | 0.5 | |||
| Cefadroxil | 1/1 | 2/4 | ≤0.25 | ≤0.25 | >32/>32 | >32/>32 | 1 | 4 | ||||||||||||
| Cefalexin | 1/1 | 2/4 | 0.25 | 0.25 | >32/>32 | >32/>32 | 2 | 8 | ||||||||||||
| Cefovecin | 0.25/0.12 | 0.25/1 | ≤0.03 | ≤0.03 | >32/>32 | >32/>32 | 0.25 | 2 | ||||||||||||
| Cephalothin | ≤0.06/0.06 | 0.12/0.25 | 0.25 | 0.25 | 32/32 | >64/64 | ≤0.06 | 0.25 | ||||||||||||
| Gentamicin * | 88.4/85.0 | 2.3/5.0 | 9.3/10.0 | 0.12/0.12 | 8/8 | 32 | 32 | 16/16 | >32/>32 | 97.4 | 0 | 2.6 | ≤0.06 | 0.25 | ||||||
| Neomycin | ≤0.25/8 | 16/16 | 128 | >128 | 64/64 | >128/>128 | ≤0.25 | ≤0.25 | ||||||||||||
| Enrofloxacin | 44.2 | 45.3 | 10.5 | 0.12/0.12 | 0.5/>8 | 43.4 | 56.6 | 0 | 1 | 1 | 1/1 | >8/>8 | 0.12 | 0.25 | ||||||
| Marbofloxacin | 20.9 | 67.5 | 11.6 | 0.25/0.25 | 0.5/>8 | 35.9 | 62.3 | 1.9 | 2 | 2 | 2/2 | >8/>8 | 0.25 | 0.5 | ||||||
| Orbifloxacin | 90.7 | 0 | 9.3 | 0.5/0.5 | 1/>16 | 0 | 100.0 | 0 | 4 | 4 | 2/4 | >16/>16 | 0.5 | 1 | ||||||
| Pradofloxacin | 90.7 | 1.2 | 8.1 | 0.03/0.03 | 0.06/2 | 0.12 | 0.12 | 0.5/0.5 | 2/2 | 0.06 | 0.25 | |||||||||
| Trimethoprim-sulfamethoxazole (1:19) * | 88.4/80.0 | 0/0 | 11.6/20.0 | 0.25/0.5 | 8/8 | 0.06 | 0.12 | 0.03/0.06 | >8/2 | 100 | 0 | 0 | 0.06 | 0.12 | ||||||
| Staphylococcus intermedius Group (Dog, n = 143/Cat, n = 15) | Streptococcus spp. (Dog, n = 64) | Enterococcus spp. (Dog, n = 62/Cat, n = 67) | Coagulase-Negative Staphylococci (Cat, n = 50) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial Agent | S (%) | I (%) | R (%) | MIC50 | MIC90 | S (%) | I (%) | R (%) | MIC50 | MIC90 | S (%) | I (%) | R (%) | MIC50 | MIC90 | S (%) | I (%) | R (%) | MIC50 | MIC90 |
| Amoxicillin | 0.5/0.5 | 16/64 | ≤0.015 | ≤0.015 | 1/1 | 4/2 | 0.12 | 4 | ||||||||||||
| Amoxicillin-clavulanic acid (2:1) | 89.5/73.3 | 1.4/0 | 9.1/26.7 | 0.12/0.12 | 0.5/32 | ≤0.015 | ≤0.015 | 90.3/92.5 | 0/0 | 9.7/7.5 | 1/1 | 4/2 | 86.0 | 4.0 | 10.0 | 0.12 | 0.5 | |||
| Cefadroxil | 2/2 | 4/>32 | 0.12 | 0.12 | >32/>32 | >32/>32 | 2 | 4 | ||||||||||||
| Cefalexin | 1/1 | 4/>32 | 0.25 | 0.25 | >32/>32 | >32/>32 | 1 | 8 | ||||||||||||
| Cefovecin | 0.12/0.25 | 1/32 | 0.03 | 0.06 | >32/>32 | >32/>32 | 0.25 | 4 | ||||||||||||
| Cephalothin | 0.06/0.06 | 0.25/64 | 0.12 | 0.12 | 32/32 | >64/64 | 0.12 | 1 | ||||||||||||
| Doxycycline * | 1/0.06 | 4/4 | 62.5 | 1.6 | 35.9 | 0.25 | 16 | 50.0/50.8 | 37.1/37.3 | 12.9/11.9 | 4/4 | 16/16 | 0.06 | 0.25 | ||||||
| Gentamicin * | 88.8/80.0 | 1.4/6.7 | 9.8/13.3 | 0.12/0.12 | 8/16 | 4 | 8 | 16/16 | >32/>32 | 94.0 | 0 | 6.0 | ≤0.03 | 0.12 | ||||||
| Neomycin | 0.25/0.25 | 32/16 | 32 | 64 | 128/128 | >128/>128 | 0.06 | 0.25 | ||||||||||||
| Enrofloxacin | 40.5 | 43.4 | 16.1 | 0.12/0.12 | 2/16 | 48.4 | 51.6 | 0.0 | 1 | 1 | 1/1 | >16/16 | 0.12 | 0.5 | ||||||
| Marbofloxacin | 18.2 | 62.2 | 19.6 | 0.25/0.25 | 4/16 | 78.1 | 20.3 | 1.6 | 1 | 2 | 2/2 | >16/16 | 0.25 | 1 | ||||||
| Orbifloxacin | 86.0 | 1.4 | 12.6 | 0.5/0.5 | 16/>16 | 3.1 | 95.3 | 1.6 | 2 | 4 | 4/4 | >16/>16 | 0.5 | 2 | ||||||
| Pradofloxacin | 89.5 | 3.5 | 7.0 | 0.03/0.03 | 0.5/2 | 0.12 | 0.12 | 0.25/0.25 | 8/2 | 0.03 | 0.25 | |||||||||
| Trimethoprim-sulfamethoxazole (1:19) * | 85.3/80.0 | 0/0 | 14.7/20.0 | 0.5/0.5 | 8/16 | 0.06 | 0.06 | 0.03/0.06 | 16/>16 | 98.0 | 0 | 2.0 | 0.06 | 0.12 | ||||||
| Breakpoints Ed6 | Breakpoints Ed7 | |||||
|---|---|---|---|---|---|---|
| S | I | R | S | SDD * | R | |
| ComPath II | ||||||
| Enrofloxacin | 90.7% | 0% | 9.3% | 44.2% | 45.3% | 10.5% |
| Marbofloxacin | 90.7% | 0% | 9.3% | 20.1% | 67.5% | 11.6% |
| ComPath III | ||||||
| Enrofloxacin | 86.0% | 4.9% | 9.1% | 40.5% | 43.4% | 16.1% |
| Marbofloxacin | 86.0% | 2.1% | 11.9% | 18.2% | 62.2% | 19.6% |
| Breakpoints in µg/mL [Susceptible (≤)/Resistant (≥)] a | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Penicillins | Cephalosporins | Tetra- Cyclines | Aminoglycosides | Fluoroquinolones | Sulpho-Namides | |||||||||
| Amoxi-Cillin | Amoxicillin-Clavulanic Acid (2:1) | Cefa-Droxil | Cefa-Lexin | Cefo-Vecin | Cepha-Lothin | Doxy-Cycline e | Genta-Micin | Neo-Mycin | Enro-Floxacin | Marbo-Floxacin | Orbi-Floxacin | Prado-Floxacin | Trimetho- Prim-Sulfa-Methoxazole (1:19) | |
| Staphylococcus spp. | - | 0.25/1 | - | - | - | - | - | (4/16) | - | 0.06/0.5 | 0.12/0.5 | 1/8 | 0.25/2 f | (2/4) |
| Streptococcus spp. | - | 0.25/1 | - | - | - | - | (2/8) g | - | - | 0.5/4 | 1/4 | 1/8 | - | - |
| Enterococcus spp. | - | 8/16 | - | - | - | - | (4/16) | - | - | - | - | - | - | - |
| E. coli | - | 8/- | - | 16/32; (16/32) | 2/8 | - | 0.12/0.5; (4/16) | 2/8; (2/8) | - | 0.06/0.5 | 0.12/0.5 | 1/8 | 0.25/2 | (2/4) |
| Klebsiella spp. | - | 8/- | - | 16/32; (16/32) c | - | - | 0.12/0.5; (4/16) | 2/8; (2/8) | - | 0.06/0.5 | 0.12/0.5 | 1/8 | - | (2/4) |
| Proteus spp. | - | 8/- | - | 16/32; (16/32) b | 2/8 b | - | 0.12/0.5; (4/16) | 2/8; (2/8) | - | 0.06/0.5 | 0.12/0.5 | 1/8 | - | (2/4) |
| P. aeruginosa d | - | - | - | - | - | - | 2/8 | - | 0.06/0.5 | 0.12/0.5 | - | - | - | |
| Pasteurella spp. | - | 0.25/1 | - | - | - | - | - | - | - | - | - | - | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Temmerman, R.; Berlamont, H.; El Garch, F.; Rose, M.; Simjee, S.; Meschi, S.; de Jong, A. Antimicrobial Susceptibility of Canine and Feline Urinary Tract Infection Pathogens Isolated from Animals with Clinical Signs in European Veterinary Practices during the Period 2013–2018. Antibiotics 2024, 13, 500. https://doi.org/10.3390/antibiotics13060500
Temmerman R, Berlamont H, El Garch F, Rose M, Simjee S, Meschi S, de Jong A. Antimicrobial Susceptibility of Canine and Feline Urinary Tract Infection Pathogens Isolated from Animals with Clinical Signs in European Veterinary Practices during the Period 2013–2018. Antibiotics. 2024; 13(6):500. https://doi.org/10.3390/antibiotics13060500
Chicago/Turabian StyleTemmerman, Robin, Helena Berlamont, Farid El Garch, Markus Rose, Shabbir Simjee, Sylvie Meschi, and Anno de Jong. 2024. "Antimicrobial Susceptibility of Canine and Feline Urinary Tract Infection Pathogens Isolated from Animals with Clinical Signs in European Veterinary Practices during the Period 2013–2018" Antibiotics 13, no. 6: 500. https://doi.org/10.3390/antibiotics13060500
APA StyleTemmerman, R., Berlamont, H., El Garch, F., Rose, M., Simjee, S., Meschi, S., & de Jong, A. (2024). Antimicrobial Susceptibility of Canine and Feline Urinary Tract Infection Pathogens Isolated from Animals with Clinical Signs in European Veterinary Practices during the Period 2013–2018. Antibiotics, 13(6), 500. https://doi.org/10.3390/antibiotics13060500