
Post-Coronavirus Disease 2019 Pandemic Antimicrobial Resistance

 ,
,  ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Results and Discussion
2.1. Antimicrobial Resistance and Germs during the Pandemic
2.1.1. The Concept of Antimicrobial Resistance
2.1.2. Antibiotics Resistance and Germs: Gram-Negative Bacteria
2.1.3. Gram-Positive Bacteria
2.1.4. Fungi

{kind=link}
| Type and Number of Patients | Germs’ Resistance | Main Antibiotic Resistance | Reference |
|---|---|---|---|
| 340 outpatients/inpatients | E. coli, Klebsiella, S. aureus (MSSA), S. aureus (MRSA), P. aeruginosa., and Enterobacter species | Cotrimoxazole, piperacillin, ceftazidime, and cefepime | [38] |
| 102 ICU patients | A. baumannii, K. pneumoniae, and S. maltophilia | Carbapenem and methicillin | [39] |
| 190 ICU patients | K. pneumoniae, A. baumannii, S. maltophilia, C. albicans, and Pseudomonas spp. | Carbapenem | [40] |
| 750 ICU patients | A. baumannii, and K. pneumonia | MDR, carbapenem | [41] |
| 611 ICU patients | Acinetobacter spp. | Imipenem, meropenem, and ciprofloxacin | [42] |
| 197 ICU patients | K. pneumoniae and A. baumannii | (PDR)K. pneumoniae and (MDR) A. baumannii | [43] |
| 856 ICU patients | E. coli and K. pneumonia | Ciprofloxacin and ampicillin (E. coli); ampicillin and amoxycillin (K. pneumoniae) | [44] |
| 255 outpatients/inpatients | S. aureus and P. aeruginosa | Oxacillin, vancomycin, carbapenems, colistin, third- and fourth-generation cephalosporins | [45] |
| 7309 ICU patients | A. baumannii and E. coli | MDR | [46] |
| 3532 outpatients/inpatients | E. coli, K. pneumoniae, and P. aeruginosa | ESBL producing Enterobacterales MDR | [47] |
| 553 ICU patients | K. pneumonia and A. baumannii | Carbapenem resistant | [48] |
2.1.5. Virus and Protozoa
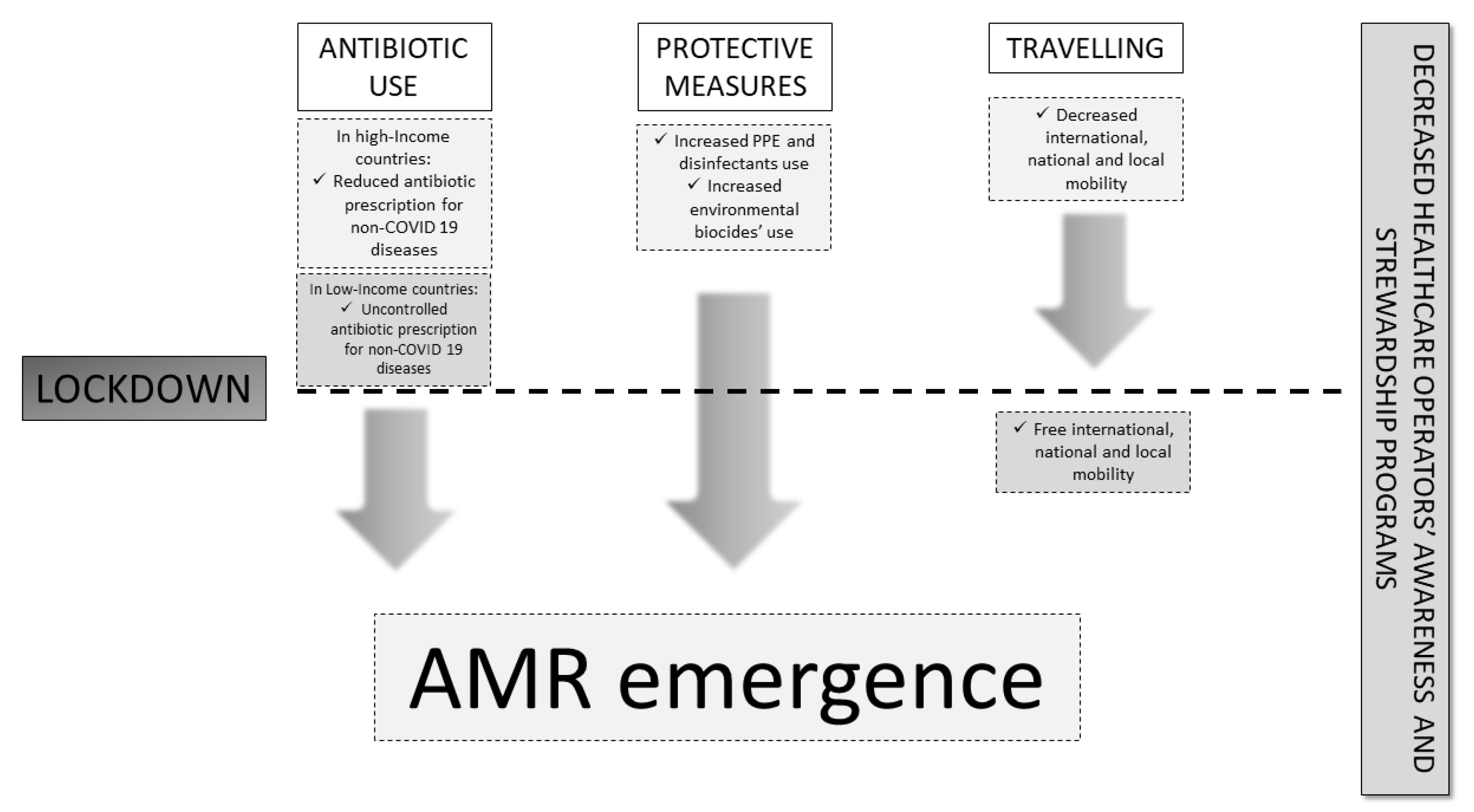
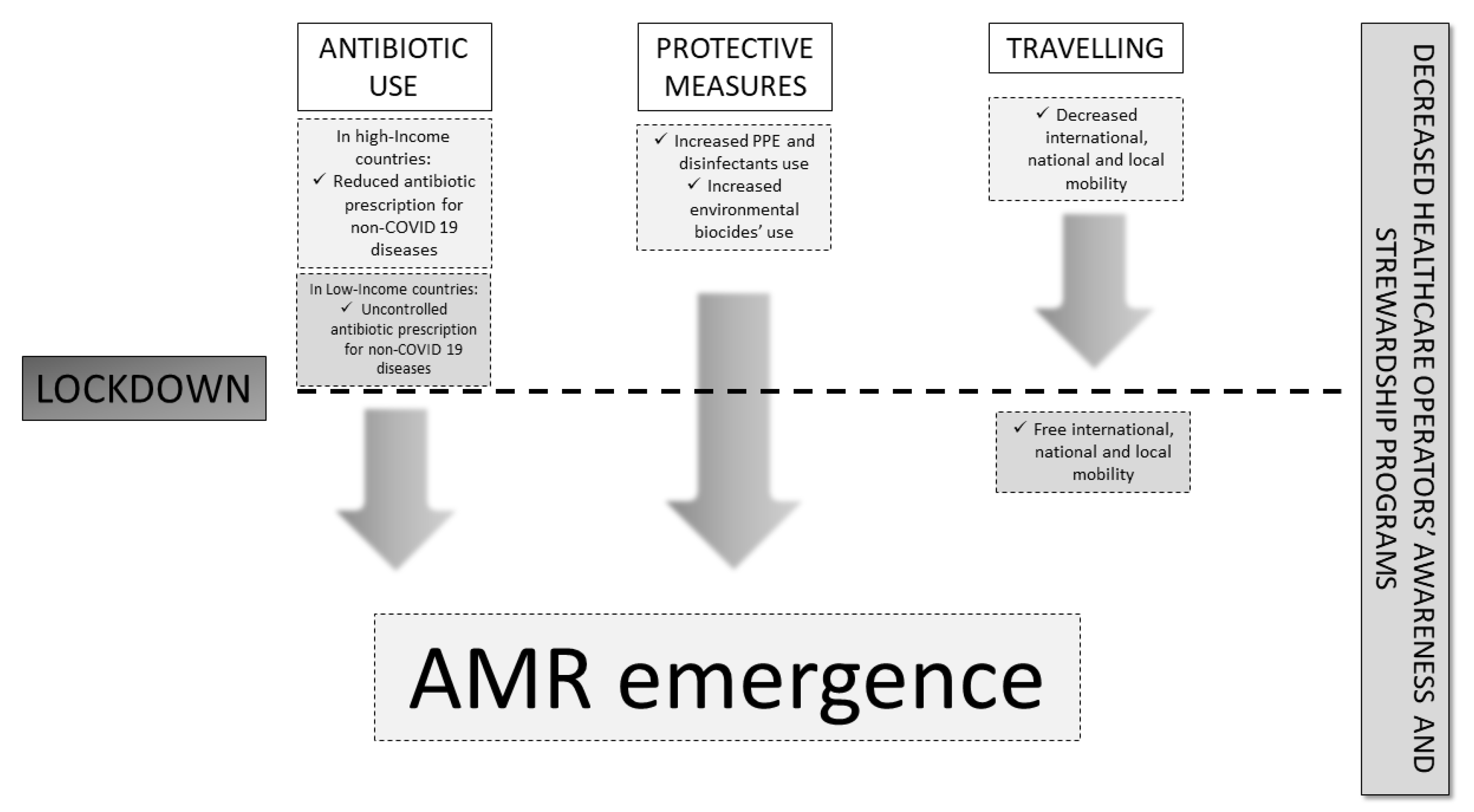
2.2. Factors Involved in AMR Development during COVID-19
2.2.1. Hospital Use of Antibiotics during the Pandemic
2.2.2. Preventive Measures: PPE and Disinfectants
2.2.3. Travel Restrictions and Re-Opening
3. Materials and Methods
4. Conclusions and Future Perspectives
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spotlight on Antimicrobial Resistance: The Slow Pandemic. Royal Society of Medicine Website. Available online: https://www.rsm.ac.uk/events/rsm-studios/2021-22/ceq03/ (accessed on 3 February 2022).
- O’Neil, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations—The Review on Antimicrobial Resistance Chaired by Wellcome Website. Available online: https://wellcomecollection.org/works/rdpck35v (accessed on 3 February 2022).
- Available online: https://www.epicentro.iss.it/antibiotico-resistenza/impatto-europa-mondo (accessed on 11 November 2023).
- COVID Live Update: 252,253,520 Cases and 5,091,111 Deaths from the Coronavirus. Worldometer Website. Available online: https://www.worldometers.info/coronavirus/ (accessed on 3 February 2021).
- While, A. Antimicrobial resistance post-COVID-19 pandemic. Br. J. Community Nurs. 2023, 28, 422–423. [Google Scholar] [CrossRef] [PubMed]
- Kondilis, E.; Tarantilis, F.; Benos, A. Essential public healthcare services utilization and excess non–COVID-19 mortality in Greece. Public Health 2021, 198, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Roy, C.M.; Bollman, E.B.; Carson, L.M.; Northrop, A.J.; Jackson, E.F.; Moresky, R.T. Assessing the indirect effects of COVID-19 on healthcare delivery, utilization and health outcomes: A scoping review. Eur. J. Public Health 2021, 31, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Tomczyk, S.; Taylor, A.; Brown, A.; de Kraker, M.E.A.; El-Saed, A.; Alshamrani, M.; Hendriksen, R.S.; Jacob, M.; Löfmark, S.; Perovic, O.; et al. Impact of the COVID-19 pandemic on the surveillance, prevention and control of antimicrobial resistance: A global survey. J. Antimicrob. Chemother. 2021, 76, 3045–3058. [Google Scholar] [CrossRef]
- Nowbuth, A.A.; Asombang, A.W.; Alaboud, K.; Souque, C.; Dahu, B.M.; Pather, K.; Mwanza, M.M.; Lotfi, S.; Parmar, V.S. Gamification as an educational tool to address antimicrobial resistance: A systematic review. JAC Antimicrob. Resist. 2023, 5, dlad130. [Google Scholar] [CrossRef] [PubMed]
- Blair, J.M.A.; Webber, M.A.; Baylay, A.J.; Ogbolu, D.O.; Piddock, L.J.V. Molecular mechanisms of antibiotic resistance. Nat. Rev. Microbiol. 2015, 13, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Loh, B.; Chen, J.; Manohar, P.; Yu, Y.; Hua, X.; Leptihn, S. A biological inventory of prophages in A. baumannii genomes reveal distinct distributions in classes, length, and genomic positions. Front. Microbiol. 2020, 11, 579802. [Google Scholar] [CrossRef] [PubMed]
- Blair, J.M.A.; Richmond, G.E.; Piddock, L.J.V. Multidrug efflux pumps in Gram-negative bacteria and their role in antibiotic resistance. Future Microbiol. 2014, 9, 1165–1177. [Google Scholar] [CrossRef]
- Chancey, S.T.; Zähner, D.; Stephens, D.S. Acquired inducible antimicrobial resistance in Gram-positive bacteria. Future Microbiol. 2012, 7, 959–978. [Google Scholar] [CrossRef]
- Abushaheen, M.A.; Muzaheed; Fatani, A.J.; Alosaimi, M.; Mansy, W.; George, M.; Acharya, S.; Rathod, S.; Divakar, D.D.; Jhugroo, C.; et al. Antimicrobial resistance, mechanisms and its clinical significance. Dis. Mon. 2020, 66, 100971. [Google Scholar] [CrossRef]
- Yang, B.; Mallett, S.; Takwoingi, Y.; Davenport, C.F.; Hyde, C.J.; Whiting, P.F.; Deeks, J.J.; Leeflang, M.M.G.; QUADAS-C Group; Bossuyt, P.M.M.; et al. QUADAS-C: A Tool for Assessing Risk of Bias in Comparative Diagnostic Accuracy Studies. Ann. Intern. Med. 2021, 174, 1592–1599. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, J.; Yang, Y.; Cai, P.; Cao, J.; Cai, X.; Zhang, Y. Etiology and antimicrobial resistance of secondary bacterial infections in patients hospitalized with COVID-19 in Wuhan, China: A retrospective analysis. Antimicrob. Resist. Infect. Control. 2020, 9, 153. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.epicentro.iss.it/antibiotico-resistenza/ar-iss/RIS-1_2021.pdf (accessed on 3 February 2023).
- Perez, S. Increase in hospital-acquired carbapenem-resistant Acinetobacter baumannii infection and colonization in an acute care hospital during a surge in COVID-19 admissions—New Jersey, February–July 2020. Morb. Mortal. Wkly Rep. 2020, 69, 1827–1831. [Google Scholar] [CrossRef] [PubMed]
- US Centers for Disease Control and Prevention. COVID-19: U.S. Impact on Antimicrobial Resistance, Special Report 2022 [Internet]. National Center for Emerging and Zoonotic Infectious Diseases. 2022. Available online: https://stacks.cdc.gov/view/cdc/117915 (accessed on 9 August 2022).
- Langford, B.J.; Soucy, J.R.; Leung, V.; So, M.; Kwan, A.T.H.; Portnoff, J.S.; Bertagnolio, S.; Raybardhan, S.; MacFadden, D.R.; Daneman, N. Antibiotic resistance associated with the COVID-19 pandemic: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2023, 29, 302–309. [Google Scholar] [CrossRef]
- Chamieh, A.; Zgheib, R.; El-Sawalhi, S.; Yammine, L.; El-Hajj, G.; Zmerli, O.; Afif, C.; Rolain, J.M.; Azar, E. Trends of Multidrug-Resistant Pathogens, Difficult to Treat Bloodstream Infections, and Antimicrobial Consumption at a Tertiary Care Center in Lebanon from 2015-2020: COVID-19 Aftermath. Antibiotic 2021, 10, 1016. [Google Scholar] [CrossRef] [PubMed]
- Lemenand, O.; Coeffic, T.; Thibaut, S.; Colomb Cotinat, M.; Caillon, J.; Birgand, G. Decreasing proportion of extended-spectrum beta-lactamase among, E. coli infections during the COVID-19 pandemic in France. J. Infect. 2021, 83, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Wardoyo, E.H.; Suardana, I.W.; Yasa, I.W.P.S.; Sukrama, I.D.M. Antibiotics susceptibility of Escherichia coli isolates from clinical specimens before and during COVID-19 pandemic. Iran. J. Microbiol. 2021, 13, 156. [Google Scholar]
- Porto, A.P.M.; Borges, I.C.; Buss, L.; Machado, A.; Bassetti, B.R.; Cocentino, B.; Bicalho, C.S.; Carrilho, C.M.D.M.; Rodrigues, C.; Neto, E.A.S.; et al. Healthcare-associated infections on the intensive care unit in 21 Brazilian hospitals during the early months of the coronavirus disease 2019 (COVID-19) pandemic: An ecological study. Infect. Control. Hosp. Epidemiol. 2023, 44, 284–290. [Google Scholar] [CrossRef]
- Evans, M.E.; Simbartl, L.A.; Kralovic, S.M.; Clifton, M.; DeRoos, K.; McCauley, B.P.; Gauldin, N.; Flarida, L.K.; Gamage, S.D.; Jones, M.M.; et al. Healthcare-associated infections in Veterans Affairs acute-care and long-term healthcare facilities during the coronavirus disease 2019 (COVID-19) pandemic. Infect. Control. Hosp. Epidemiol. 2023, 44, 420–426. [Google Scholar] [CrossRef]
- Bentivegna, E.; Luciani, M.; Arcari, L.; Santino, I.; Simmaco, M.; Martelletti, P. Reduction of multidrug-resistant (MDR) bacterial infections during the COVID-19 Pandemic: A retrospective study. Int. J. Environ. Res. Public Health 2021, 18, 1003. [Google Scholar] [CrossRef]
- McNeil, J.C.; Flores, A.R.; Kaplan, S.L.; Hulten, K.G. The indirect impact of the SARSCoV-2 pandemic on invasive group a Streptococcus, Streptococcus Pneumoniae and Staphylococcus Aureus infections in Houston area children. Pediatr. Infect. Dis. J. 2021, 40, e313e6. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Simeonova, M.; Leung, V.; Lo, J.; Kan, T.; Raybardhan, S.; Sapin, M.E.; Mponponsuo, K.; Farrell, A.; et al. Antimicrobial resistance in patients with COVID-19: A systematic review and meta-analysis. Lancet Microbe 2023, 4, e179–e191. [Google Scholar] [CrossRef] [PubMed]
- Gisselø, K.L.; Rubin, I.M.C.; Knudsen, M.S.; From-Hansen, M.; Stangerup, M.; Kavalaris, C.P.; Pinholt, M.; Mollerup, S.; Westh, H.; Bartels, M.D.; et al. Substantial Decrease in Vancomycin-Resistant Enterococcus faecium Outbreak Duration and Number of Patients During the Danish COVID-19 Lockdown: A Prospective Observational Study. Microb. Drug Resist. 2022, 28, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Song, G.; Liang, G.; Liu, W. Fungal co-infections associated with global COVID-19 pandemic: A clinical and diagnostic perspective from China. Mycopathologia 2020, 185, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Vinh, D.C. The molecular immunology of human susceptibility to fungal diseases: Lessons from single gene defects of immunity. Expert Rev. Clin. Immunol. 2019, 15, 461–486. [Google Scholar] [CrossRef]
- Posteraro, B.; Torelli, R.; Vella, A.; Leone, P.M.; De Angelis, G.; De Carolis, E.; Ventura, G.; Sanguinetti, M.; Fantoni, M. Pan-Echinocandin-Resistant Candida glabrataBloodstream Infection Complicating COVID-19: A Fatal Case Report. J. Fungi 2020, 6, 163. [Google Scholar] [CrossRef]
- Srivastava, V.K.; Suneetha, K.J.; Kaur, R. A systematic analysis reveals an essential role for high-affinity iron uptake system, haemolysin and CFEM domain-containing protein in iron homoeostasis and virulence in Candida glabrata. Biochem. J. 2014, 463, 103–114. [Google Scholar] [CrossRef]
- Chowdhary, A.; Tarai, B.; Singh, A.; Sharma, A. Multidrug-resistant candida auris infections in critically Ill Coronavirus disease patients, India, April–July 2020. Emerg. Infect Dis. 2020, 26, 2694–2696. [Google Scholar] [CrossRef]
- Mohamed, A.; Hassan, T.; Trzos-Grzybowska, M.; Thomas, J.; Quinn, A.; O’Sullivan, M.; Griffin, A.; Rogers, T.R.; Talento, A.F. Multi-triazole-resistant Aspergillus fumigatus and SARS-CoV 2 co-infection: A lethal combination. Med. Mycol. Case Rep. 2021, 31, 11–14. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Denning, D.W.; Park, S.; Lass-Florl, C.; Fraczek, M.G.; Kirwan, M.; Gore, R.; Smith, J.; Bueid, A.; Moore, C.B.; Bowyer, P.; et al. High-frequency triazole resistance found In nonculturable Aspergillus fumigatus from lungs of patients with chronic fungal disease. Clin. Infect. Dis. 2011, 52, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, H. Bacterial co-infections and antibiotic resistance in patients with COVID-19. GMS Hyg. Infect. Control. 2020, 15, Doc35. [Google Scholar]
- Obeidat, H.; El-Nasser, Z.; Amarin, Z.; Qablan, A.; Gharaibeh, F. The impact of COVID-19 pandemic on healthcare associated infections: A teaching hospital experience. Medicine 2023, 102, e33488. [Google Scholar] [CrossRef] [PubMed]
- Sang, L.; Xi, Y.; Lin, Z.; Pan, Y.; Song, B.; Li, C.A.; Zheng, X.; Zhong, M.; Jiang, L.; Pan, C.; et al. Secondary infection in severe and critical COVID-19 patients in China: A multicenter retrospective study. Ann. Palliat. Med. 2021, 10, 8557–8570. [Google Scholar] [CrossRef] [PubMed]
- Palanisamy, N.; Vihari, N.; Meena, D.S.; Kumar, D.; Midha, N.; Tak, V.; Sharma, A.; Bohra, G.K.; Kothari, N.; Dutt, N.; et al. Clinical profile of bloodstream infections in COVID-19 patients: A retrospective cohort study. BMC Infect. Dis. 2021, 21, 933. [Google Scholar] [CrossRef] [PubMed]
- Despotovic, A.; Milosevic, B.; Cirkovic, A.; Vujovic, A.; Cucanic, K.; Cucanic, T.; Stevanovic, G. The Impact of COVID-19 on the Profile of Hospital-Acquired Infections in Adult Intensive Care Units. Antibiotics 2021, 10, 1146. [Google Scholar] [CrossRef] [PubMed]
- Meawed, T.E.; Ahmed, S.M.; Mowafy, S.M.S.; Samir, G.M.; Anis, R.H. Bacterial and fungal ventilator associated pneumonia in critically ill COVID-19 patients during the second wave. J. Infect. Public Health 2021, 14, 1375–1380. [Google Scholar] [CrossRef]
- Zeshan, B.; Karobari, M.I.; Afzal, N.; Siddiq, A.; Basha, S.; Basheer, S.N.; Peeran, S.W.; Mustafa, M.; Daud, N.H.A.; Ahmed, N.; et al. The Usage of Antibiotics by COVID-19 Patients with Comorbidities: The Risk of Increased Antimicrobial Resistance. Antibiotics 2021, 11, 35. [Google Scholar] [CrossRef]
- Caruso, P.; Maiorino, M.I.; Macera, M.; Signoriello, G.; Castellano, L.; Scappaticcio, L.; Longo, M.; Gicchino, M.; Campitiello, F.; Bellastella, G.; et al. Antibiotic resistance in diabetic foot infection: How it changed with COVID-19 pandemic in a tertiary care center. Diabetes Res. Clin. Pract. 2021, 175, 108797. [Google Scholar] [CrossRef]
- Saini, V.; Jain, C.; Singh, N.P.; Alsulimani, A.; Gupta, C.; Dar, S.A.; Haque, S.; Das, S. Paradigm Shift in Antimicrobial Resistance Pattern of Bacterial Isolates during the COVID-19 Pandemic. Antibiotics 2021, 10, 954. [Google Scholar] [CrossRef]
- Karatas, M.; Yasar-Duman, M.; Tünger, A.; Çilli, F.; Aydemir, S.; Özenci, V. Secondary bacterial infections and antimicrobial resistance in COVID-19: Comparative evaluation of pre-pandemic and pandemic-era, a retrospective single center study. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 51. [Google Scholar] [CrossRef] [PubMed]
- Pourajam, S.; Kalantari, E.; Talebzadeh, H.; Mellali, H.; Sami, R.; Soltaninejad, F.; Amra, B.; Sajadi, M.; Alenaseri, M.; Kalantari, F.; et al. Secondary Bacterial Infection and Clinical Characteristics in Patients With COVID-19 Admitted to Two Intensive Care Units of an Academic Hospital in Iran During the First Wave of the Pandemic. Front. Cell. Infect. Microbiol. 2022, 12, 784130. [Google Scholar] [CrossRef] [PubMed]
- Towns, A.M.; Mengue Eyi, S.; van Andel, T. Traditional medicine and childcare in Western Africa: Mothers’ knowledge, folk illnesses, and patterns of healthcare-seeking behavior. PLoS ONE 2014, 9, e105972. [Google Scholar] [CrossRef]
- Ataba, E.; Dorkenoo, A.M.; Nguepou, C.T.; Bakai, T.; Tchadjobo, T.; Kadzahlo, K.D.; Yakpa, K.; Atcha-Oubou, T. Potential Emergence of Plasmodium Resistance to Artemisinin Induced by the Use of Artemisia annua for Malaria and COVID-19 Prevention in Sub-African Region. Acta Parasitol. 2022, 67, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Welz, A.N.; Emberger-Klein, A.; Menrad, K. Why people use herbal medicine: Insights from a focus-group study in Germany. BMC Complement. Altern. Med. 2018, 18, 92. [Google Scholar] [CrossRef] [PubMed]
- Septembre-Malaterre, A.; Lalarizo Rakoto, M.; Marodon, C.; Bedoui, Y.; Nakab, J.; Simon, E.; Hoarau, L.; Savriama, S.; Strasberg, D.; Guiraud, P.; et al. Artemisia annua, a traditional plant brought to light. Int. J. Mol. Sci. 2020, 21, 4986. [Google Scholar] [CrossRef]
- Balikagala, B.; Fukuda, N.; Ikeda, M.; Katuro, O.T.; Tachibana, S.I.; Yamauchi, M.; Opio, W.; Emoto, S.; Anywar, D.A.; Kimura, E.; et al. Evidence of Artemisinin-Resistant Malaria in Africa. N. Engl. J. Med. 2021, 385, 1163–1171. [Google Scholar] [CrossRef]
- Schüz, M.L.; Dallmeyer, L.; Fragkou, P.C.; Omony, J.; Krumbein, H.; Hünerbein, B.L.; Skevaki, C. Global prevalence of respiratory virus infections in adults and adolescents during the COVID-19 pandemic: A systematic review and meta-analysis. Int. J. Infect. Dis. 2023, 137, 16–24. [Google Scholar] [CrossRef]
- Gandhi, S.; Klein, J.; Robertson, A.J.; Peña-Hernández, M.A.; Lin, M.J.; Roychoudhury, P.; Lu, P.; Fournier, J.; Ferguson, D.; Mohamed Bakhash, S.A.K.; et al. De novo emergence of a remdesivir resistance mutation during treatment of persistent SARS-CoV-2 infection in an immunocompromised patient: A case report. Nat. Commun. 2022, 13, 1547. [Google Scholar] [CrossRef]
- Donovan-Banfield, I.; Penrice-Randal, R.; Goldswain, H.; Rzeszutek, A.M.; Pilgrim, J.; Bullock, K.; Saunders, G.; Northey, J.; Dong, X.; Ryan, Y.; et al. Characterisation of SARS-CoV-2 genomic variation in response to molnupiravir treatment in the AGILE Phase Iia clinical trial. Nat. Commun. 2022, 13, 7284. [Google Scholar] [CrossRef]
- Rehman, S. A parallel and silent emerging pandemic: Antimicrobial resistance (AMR) amid COVID-19 pandemic. J. Infect. Public Health. 2023, 16, 611–617. [Google Scholar] [CrossRef]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaëlo, M.; Longuet Flandre, P.; Dubert, M.; Cally, R.; Logre, E.; Fraissé, M.; Mentec, H.; et al. Bacterial and viral co-infections in patients with severe SARS-CoV 2 pneumonia admitted to a French ICU. Ann. Intensive Care 2020, 10, 119. [Google Scholar] [CrossRef] [PubMed]
- Sharifipour, E.; Shams, S.; Esmkhani, M.; Khodadadi, J.; Fotouhi-Ardakani, R.; Koohpaei, A.; Doosti, Z.; Ej Golzari, S. Evaluation of bacterial co-infections of the respiratory tract in COVID-19 patients admitted to ICU. BMC Infect. Dis. 2020, 20, 646. [Google Scholar] [CrossRef] [PubMed]
- Calderon, M.; Li, A.; Bazo-Alvarez, J.C.; Dennis, J.; Baker, K.F.; Schim van der Loeff, I.; Hanrath, A.T.; Capstick, R.; Payne, B.A.I.; Weiand, D.; et al. Evaluation of procalcitonin-guided antimicrobial stewardship in patients admitted to hospital with COVID-19 pneumonia. JAC Antimicrob. Resist. 2021, 3, dlab133. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, T.; Fedorowsky, R.; Yerushalmi, R.; Lellouche, J.; Nutman, A. An outbreak of carbapenem-resistant Acinetobacter baumannii in a COVID19 dedicated hospital. Infect. Prev. Pract. 2021, 3, 100113. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, D.R.; Dos Santos Saalfeld, S.M.; Martinez, H.V.; Altafini, D.D.; Costa, B.B.; Fedrigo, N.H.; Tognim, M.C.B. Outbreak of endemic carbapenem-resistant Acinetobacter baumannii in a coronavirus disease 2019 (COVID-19)-specific intensive care unit. Infect. Control. Hosp. Epidemiol. 2022, 43, 815–817. [Google Scholar] [CrossRef] [PubMed]
- Dieringer, T.D.; Furukawa, D.; Graber, C.J.; Stevens, V.W.; Jones, M.M.; Rubin, M.A.; Goetz, M.B. Inpatient antibiotic utilization in the Veterans’ Health Administration during the coronavirus disease 2019 (COVID-19) pandemic. Infect. Control. Hosp. Epidemiol. 2021, 42, 751–753. [Google Scholar] [CrossRef]
- UK Health Security Agency. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2020 to 2021. UK Government Website. Available online: https://www.gov.uk/government/publications/englishsurveillance-programme-antimicrobial-utilisation-and-resistance-espaurreport (accessed on 22 February 2023).
- Winders, H.R.; Bailey, P.; Kohn, J.; Faulkner-Fennell, C.M.; Utley, S.; Lantz, E.; Sarbacker, L.; Justo, J.A.; Bookstaver, P.B.; Weissman, S.; et al. Change in Antimicrobial Use during COVID-19 Pandemic in South Carolina Hospitals: A Multicenter Observational Cohort Study. Int. J. Antimicrob. Agents. 2021, 58, 106453. [Google Scholar] [CrossRef]
- Castro, M.G.; Ubiergo, L.; Vicino, M.; Cuevas, G.; Argarana, F. Rising incidence of carbapenem resistant isolates: An Argentinian hospital’s experience. More trouble in the aftermath of the COVID-19 pandemic. IberoAmerican J. Med. 2022, 4, 92–99. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Fujita, K.; Kashihara, E.; Kanai, O.; Hata, H.; Yasoda, A.; Odagaki, T.; Mio, T. Increasing Burden of Nursing Care on the Treatment of COVID-19 Patients in the Aging Society: Analyses During the First to the Third Wave of Pandemic in Kyoto City, Japan. Front. Med. 2021, 8, 767110. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.B. Active efflux, a common mechanism for biocide and antibiotic resistance. J. Appl. Microbiol. 2002, 92, 65S–71S. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Yang, L.; Liu, Z.; Han, J.; Zhao, Y.; Jin, Y.; Sheng, Y.; Zhu, L.; Hu, B. Excessive disinfection aggravated the environmental prevalence of antimicrobial resistance during COVID-19 pandemic. Sci. Total. Environ. 2023, 882, 163598. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.; Lu, H.; Zhua, L. Molecular mechanism of antibiotic resistance induced by mono- and twin-chained quaternary ammonium compounds. Sci. Total. Environ. 2022, 832, 155090. [Google Scholar] [CrossRef] [PubMed]
- Castanheira, M.; Griffin, M.A.; Deshpande, L.M.; Mendes, R.E.; Jones, R.N.; Flamm, R.K. Detection of mcr-1 among Escherichia coli clinical isolates collected worldwide as part of the SENTRY Antimicrobial Surveillance Program in 2014 and 2015. Antimicrob. Agents Chemother. 2016, 60, 5623–5624. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.Y.; Wang, Y.; Walsh, T.R.; Yi, L.X.; Zhang, R.; Spencer, J.; Doi, Y.; Tian, G.; Dong, B.; Huang, X.; et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: A microbiological and molecular biological study. Lancet Infect. Dis. 2016, 16, 161–168. [Google Scholar] [CrossRef]
- King, L.M.; Lovegrove, M.C.; Shehab, N.; Tsay, S.; Budnitz, D.S.; Geller, A.I.; Lind, J.N.; Roberts, R.M.; Hicks, L.A.; Kabbani, S. Trends in US Outpatient Antibiotic Prescriptions During the Coronavirus Disease 2019 Pandemic. Clin. Infect. Dis. 2021, 73, e652–e660. [Google Scholar] [CrossRef]
- Knight, B.D.; Shurgold, J.; Smith, G.; MacFadden, D.R.; Schwartz, K.L.; Daneman, N.; Gravel Tropper, D.; Brooks, J. The impact of COVID-19 on community antibiotic use in Canada: An ecological study. Clin. Microbiol. Infect. 2022, 28, 426–432. [Google Scholar] [CrossRef]
- Högberg, L.D.; Vlahovi´c-Palcevski, V.; Pereira, C.; Weist, K.; Monnet, D.L.; ESAC Net study group. Decrease in community antibiotic consumption during the COVID-19 pandemic, EU/EEA, 2020. Eurosurveillance 2021, 26, 2101020. [Google Scholar] [CrossRef]
- Seneghini, M.; Rüfenacht, S.; Babouee-Flury, B.; Flury, D.; Schlegel, M.; Kuster, S.P.; Kohler, P.P. It is complicated: Potential short- and long-term impact of coronavirus disease 2019 (COVID-19) on antimicrobial resistance-An expert review. Antimicrob. Steward Healthc. Epidemiol. 2022, 2, e27. [Google Scholar] [CrossRef]
- Seasonal Influenza—Annual Epidemiological Report for 2020–2021. European Centre for Disease Prevention and Control Website. Available online: https://www.ecdc.europa.eu/en/publications-data/seasonal-influenza-annualepidemiological-report-2020-2021 (accessed on 10 November 2023).
- Britton, P.N.; Hu, N.; Saravanos, G.; Shrapnel, J.; Davis, J.; Snelling, T.; Dalby-Payne, J.; Kesson, A.M.; Wood, N.; Macartney, K.; et al. COVID-19 public health measures and respiratory syncytial virus. Lancet Child Adolesc. Health 2020, 4, e42–e43. [Google Scholar] [CrossRef]
- Brueggemann, A.B.; Jansen van Rensburg, M.J.; Shaw, D.; McCarthy, N.D.; Jolley, K.A.; Maiden, M.C.J.; van der Linden, M.P.G.; Amin-Chowdhury, Z.; Bennett, D.E.; Borrow, R.; et al. Changes in the incidence of invasive disease due to Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis during the COVID-19 pandemic in 26 countries and territories in the Invasive Respiratory Infection Surveillance Initiative: A prospective analysis of surveillance data. Lancet Digit. Health 2021, 3, e360–e370. [Google Scholar]
- Belachew, S.A.; Hall, L.; Erku, D.A.; Selvey, L.A. No prescription? No problem: Drivers of nonprescribed sale of antibiotics among community drug retail outlets in low- and middle-income countries: A systematic review of qualitative studies. BMC Public Health 2021, 21, 1056. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boccabella, L.; Palma, E.G.; Abenavoli, L.; Scarlata, G.G.M.; Boni, M.; Ianiro, G.; Santori, P.; Tack, J.F.; Scarpellini, E. Post-Coronavirus Disease 2019 Pandemic Antimicrobial Resistance. Antibiotics 2024, 13, 233. https://doi.org/10.3390/antibiotics13030233
Boccabella L, Palma EG, Abenavoli L, Scarlata GGM, Boni M, Ianiro G, Santori P, Tack JF, Scarpellini E. Post-Coronavirus Disease 2019 Pandemic Antimicrobial Resistance. Antibiotics. 2024; 13(3):233. https://doi.org/10.3390/antibiotics13030233
Chicago/Turabian StyleBoccabella, Lucia, Elena Gialluca Palma, Ludovico Abenavoli, Giuseppe Guido Maria Scarlata, Mariavirginia Boni, Gianluca Ianiro, Pierangelo Santori, Jan F. Tack, and Emidio Scarpellini. 2024. "Post-Coronavirus Disease 2019 Pandemic Antimicrobial Resistance" Antibiotics 13, no. 3: 233. https://doi.org/10.3390/antibiotics13030233
APA StyleBoccabella, L., Palma, E. G., Abenavoli, L., Scarlata, G. G. M., Boni, M., Ianiro, G., Santori, P., Tack, J. F., & Scarpellini, E. (2024). Post-Coronavirus Disease 2019 Pandemic Antimicrobial Resistance. Antibiotics, 13(3), 233. https://doi.org/10.3390/antibiotics13030233