Abstract
Background: Ceftazidime–avibactam (CAZ-AVI) is recommended as first-line treatment for Oxacillinase-48 (OXA-48) β-Lactamase-producing carbapenem-resistant Enterobacterales (CRE) infections, while polymyxin-based combination therapies (PBCTs) are used as a last resort when CAZ-AVI is unavailable. Research comparing the effectiveness of CAZ-AVI and PBCT in CRE blood stream infections (CRE-BSIs) is limited, mostly focusing on Klebsiella pneumoniae carbapenemase (KPC)-producing isolates. In Turkey, OXA-48 is endemic and OXA-48-Like is common. Therefore, our study aimed to compare the impact of these treatments on 30-day mortality in patients with CRE-BSIs in endemic regions. Methods: Retrospective data from January 2019 to May 2023 were collected from four tertiary healthcare centers in Istanbul. Demographic, clinical, and outcome data of ICU patients treated with CAZ-AVI monotherapy or PBCT for CRE-BSIs were analyzed. The effect on 30-day survival was evaluated using Cox regression analysis post propensity score matching (PSM). Results: Out of 151 patients, 44.4% (n: 67) received CAZ-AVI and 55.6% (n: 84) received PBCT. All-cause mortality rates were 20% (n: 13) with CAZ-AVI and 36.9% (n: 31) with PBCT. Cox regression analysis post PSM indicated CAZ-AVI monotherapy significantly reduced the mortality risk compared to PBCT (HR: 0.16, 95%CI: 0.07–0.37, p < 0.001), while age increased the risk (HR: 1.02 per year, 95% CI 1.0–1.04, p: 0.01). Conclusions: In OXA-48-predominant areas, CAZ-AVI demonstrated significantly lower mortality in patients with CRE-BSIs compared to PBCT. The results were attributed to the pharmacokinetic and pharmacodynamic disadvantages of polymyxins compared to CAZ-AVI, and the impact of age-related physical conditions. Therefore, CAZ-AVI should be the preferred treatment for CRE-BSIs in OXA-48-endemic regions.
1. Introduction
Carbapenem-resistant Enterobacterales (CRE) infections remain a global health problem due to their increasing incidence, high mortality rates, and negative impact on health economics [1]. The Centers for Disease Control and Prevention (CDC) reported that the proportion of healthcare-associated CRE infections and related healthcare expenditures have increased over the years [2,3]. Also, in Turkey, carbapenem resistance rates for Escherichia coli and Klebsiella pneumoniae isolates showed a significant increase from 2017 to 2021 [4].
The Infectious Diseases Society of America (IDSA) 2024 guideline recommends novel beta-lactams for the treatment of CRE. Previously recommended polymyxin-based combination therapies (PBCTs) have been associated with increased mortality and should be avoided [5].
In Turkey, where Oxacillinase-48 (OXA-48) carbapenemase-producing strains are predominant [6], ceftazidime–avibactam (CAZ-AVI) is used as first-line treatment. Nevertheless, in cases where CAZ-AVI is not available due to economic or logistical reasons, or resistance to CAZ-AVI is detected, last-resort treatment options, especially PBCTs, are to be used [7].
CAZ-AVI has been approved by the United States Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for various indications [8,9,10]. Its use in CRE bloodstream infections (CRE-BSIs) is based on limited literature data supporting it. The literature comparing the efficacy of CAZ-AVI and PBCT in CRE-BSIs with real-life data is also limited, and most is on Klebsiella pneumoniae carbapenemase (KPC)-producing isolates [11]. In this study, we aimed to compare the effects of the two treatment options on 30-day mortality in patients with CRE-BSIs in Turkey, an endemic area for OXA-48 [12,13], with real-life data. We also investigated the effects of sociodemographic, clinical, and microbiological factors on mortality in patients with CRE-BSIs receiving these treatments.
2. Results
Among the 151 patients with CRE-BSIs, 60% (n: 91) were male, with a mean age of 62 years (IQR 48–74). Targeted therapy was administered to 44.4% (n: 67) of patients with CAZ-AVI and to 55.6% (n: 84) of patients with PBCT.
The 30-day mortality rates were 20% (n: 13) for CAZ-AVI and 36.9% (n: 31) for PBCT. Microbiological eradication rates among patients (n: 120) who had follow-up blood cultures after targeted treatment were 100% (n: 57) for CAZ-AVI and 53.9% (n: 34) for PBCT (p < 0.001). Adequate source control was achieved in all patients. No relapse or development of resistance to targeted therapy during the course of treatment was detected in any of the patients.
Demographic and comorbidity characteristics are detailed in Table 1, where older age, higher Charlson Comorbidity Index (CCI) scores, and presence of hematological malignancy were associated with higher mortality rates.

Table 1.
The effect of demographic data and case backgrounds on the outcome.
Table 2 presents the clinical and microbiological profiles, treatment regimens, and their outcomes. Mortality was more prevalent among patients with central venous and percutaneous enterogastrostomy (PEG) catheters, septic shock, inotropic agent use, and higher Pittsburgh Bacteremia Index (PBI) scores. The incidence of sepsis alone did not differ significantly between the treatment arms.
Table 2.
The effect of clinical and microbiological features and treatments on the outcome.
K. pneumoniae was identified in 98% (n: 148) and E. coli in 2% (n: 3) of the blood cultures. Microbiological eradication was achieved in 60.3% (n: 91) of cases. Eradication rates were significantly higher in survivors, though the impact of eradication time on outcomes was not conclusive.
Empirical treatment regimens included piperacillin–tazobactam in 71% (n: 60), third- or fourth-generation cephalosporins in 16% (n: 14), carbapenems in 80% (n: 68), aminoglycosides in 13% (n: 11), fluoroquinolones in 12% (n: 10), tigecycline in 15% (n: 13), and fosfomycin in 6% (n: 5) of patients. The mean duration of empirical therapy was 4 days (IQR: 3–5). In survivors, the duration of empirical therapy, as the time between blood culture collection and initiation of targeted therapy, was significantly shorter than in those with a fatal outcome (p < 0.001). Additionally, CAZ-AVI as targeted therapy was associated with a significantly lower mortality rate (p < 0.001).
Univariate regression analysis identified age as a significant predictor of mortality. Chronic liver disease and a history of hematopoietic stem cell transplantation (HSCT) were also positively correlated with mortality. Higher PBI and CCI scores were associated with increased mortality risk. While sepsis alone did not significantly impact outcomes, septic shock was positively correlated with mortality. Microbiological eradication significantly improved survival outcomes (Table 3).
Table 3.
Investigation of the effect of demographic data and history of the cases on the outcome.
In multivariate regression analysis following propensity score matching to control for confounding factors, age and the use of CAZ-AVI as targeted therapy emerged as significant predictors of mortality. Each additional year of age increased the risk of mortality 1.03-fold (HR: 1.02, 95% CI 1.0 to 1.04, p: 0.01), while the use of CAZ-AVI instead of PBCT statistically reduced mortality risk (HR: 0.16, 95% CI 0.07 to 0.37, p < 0.001). No other factors showed a significant impact (Table 3).
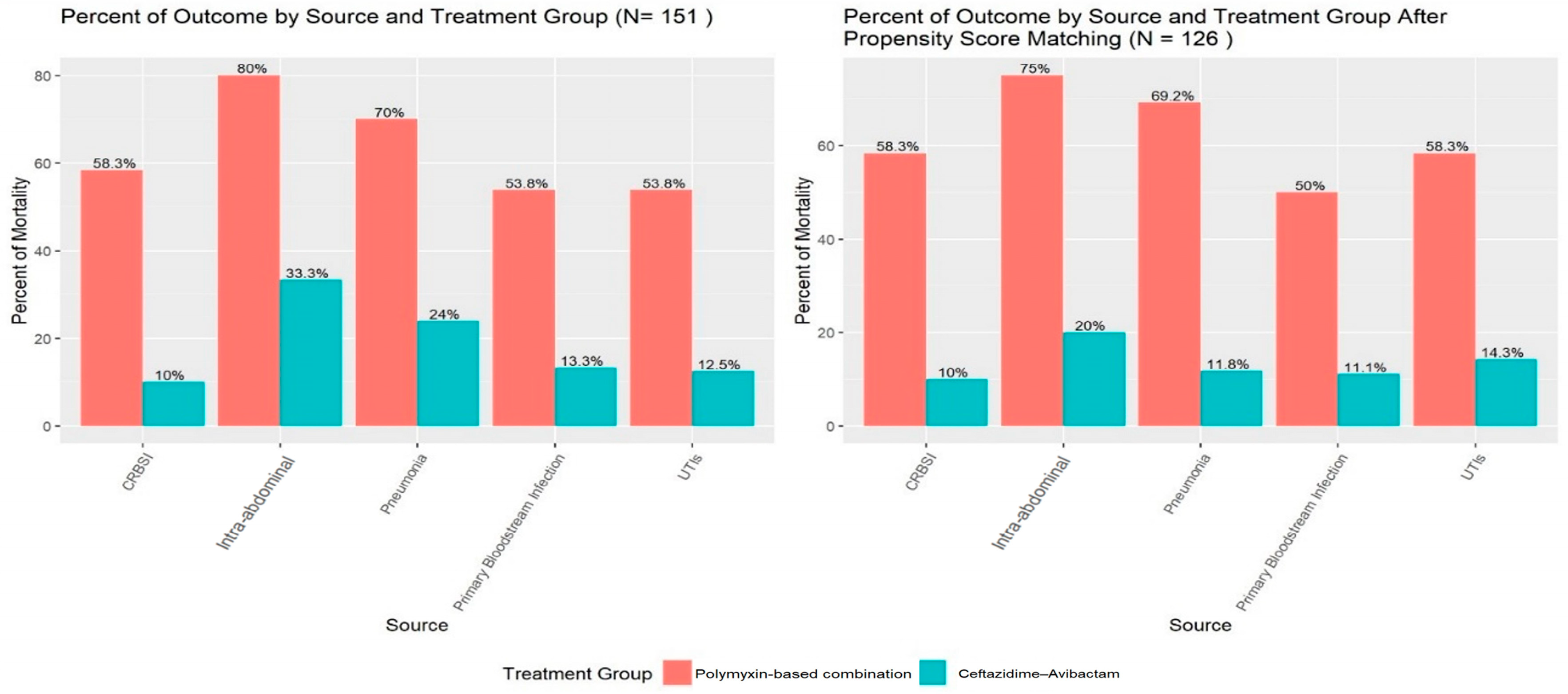
The impact of targeted therapies on outcomes was further analyzed by the source of infection, revealing that CAZ-AVI was associated with lower mortality compared to PBCT across the total cohort and in the propensity score-matched group (Figure 1).
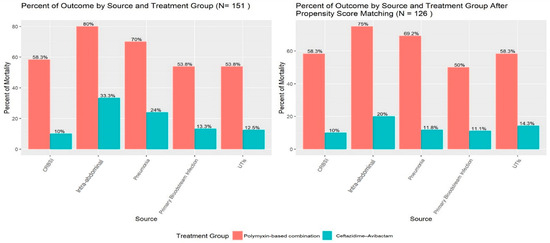
Figure 1.
Effect of targeted therapies on outcomes, according to source of infection in total cohort and propensity score-matched groups.
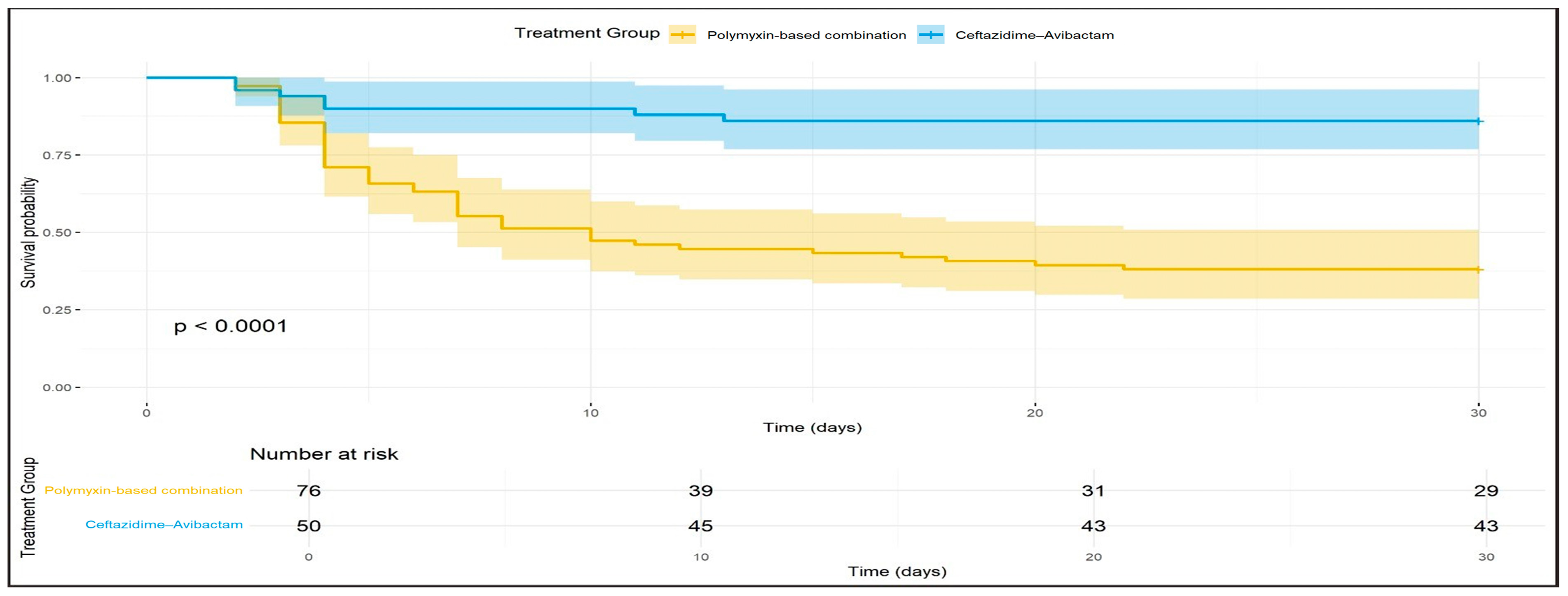
Kaplan–Meier survival analysis demonstrated that the survival probability at 30 days was significantly higher for patients receiving CAZ-AVI as targeted therapy compared to those receiving PBCT (p < 0.0001) (Figure 2).
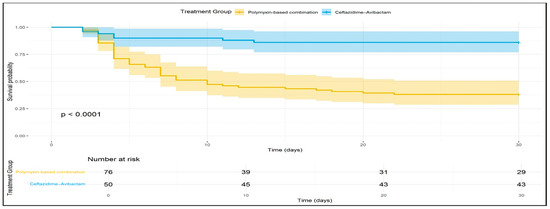
Figure 2.
Kaplan–Meier survival analysis for patients receiving Ceftazidime-Avibactam and Polymyxin-based combination therapy for 30 days after treatment initiation.
3. Discussion
Our study demonstrates that in Turkey, an OXA-48-endemic region [12,13], CAZ-AVI monotherapy significantly reduces mortality in CRE-BSIs compared to PBCT. It has been reported that there are limited studies in the literature on this issue especially in OXA-48-endemic regions [11]. Hakeam et al. reported lower mortality with CAZ-AVI compared to colistin in 61 patients with CRE-BSIs, most of which were OXA-48 producers, but the difference was not statistically significant [14]. Similarly, Lima et al. found that CAZ-AVI was associated with lower mortality compared to other last-resort therapies in 76 patients with OXA-48-producing CRKP-BSIs, yet the difference lacked statistical significance [15].
Consistent with these two studies, our study observed higher survival rates in patients treated with CAZ-AVI. In contrast, it demonstrated a statistically significant association between CAZ-AVI use and survival. This may be attributed to the multicenter design of our study, a larger cohort, and the use of PSM to control for confounding factors such as age, severity of infection, and comorbidities.
PBCT, which is a last-resort treatment option that was frequently used in the pre-novel antibiotics era in Turkey [16], was associated with an increased mortality risk compared with CAZ-AVI in our study. This is likely due to the pharmacokinetic and pharmacodynamic (PK/PD) differences between CAZ-AVI and polymyxins [17]. Polymyxins have disadvantages, including concentration-dependent activity, a narrow therapeutic window, risk of resistance development during therapy, and insufficient distribution in tissues and body fluids. In contrast, CAZ-AVI offers advantages such as low plasma protein binding, stable volume of distribution, and rapid attainment of bactericidal concentrations [18].
The high prevalence of OXA-48 in Turkey [6] underscores the efficacy of CAZ-AVI in the treatment of CRE-BSIs in this setting. Its broad-spectrum activity against OXA-48-producing strains [5] and its favorable PK/PD properties in treating CRE-BSIs [18] likely contribute to improved survival by providing faster and more effective microbiological clearance. The higher microbiological eradication rate observed with CAZ-AVI and the association of microbiological clearance with survival in univariate analysis further support this argument.
Our study identified older age as another determinant factor for mortality in CRE-BSIs. This finding is consistent with other studies [19,20] in the literature showing age as a risk factor for CRE-BSIs. This may be due to the lower physical and immunological performance of geriatric patients compared to younger populations, coupled with higher rates of hospitalization, ICU admission, and invasive device use.
Univariate regression analysis identified liver disease, history of HSCT, high PBI and CCI scores, and septic shock as mortality-associated factors. These conditions, which exacerbate BSI severity due to compromised immune responses and increased vulnerability to infection, align with those identified in findings from other studies [19,20,21]. This underscores the critical role of utilizing CAZ-AVI as a first-line therapy in high-risk groups. Integrating CAZ-AVI into clinical management strategies for CRE-BSIs may enhance survival outcomes in these susceptible populations.
Compared to the limited literature on the efficacy of CAZ-AVI and PBCT in CRE-BSIs, our study, conducted with a larger cohort, provides statistically significant results in terms of 30-day mortality. This is one of the strengths of the study. Moreover, the use of real-world data increases the clinical applicability of our findings. The retrospective nature of the study and the inability to determine the carbapenemase type are, however, limitations that should be considered when generalizing the results. Nevertheless, these findings highlight the efficacy of CAZ-AVI in high-risk CRE-BSIs in OXA-48-endemic areas and support its prioritization over PBCT in treatment strategies. Future prospective studies that include carbapenemase typing will provide valuable contributions to the literature.
4. Material and Methods
4.1. Study Design and Setting
This multicenter, observational, retrospective study involved the analysis of intensive care unit (ICU) patients from four tertiary hospitals in Istanbul who developed CRE-BSIs between 1 January 2019 and 30 May 2023. The study protocol, including case definitions, inclusion, and exclusion criteria, was shared with the participating centers. Data on the cases were collected via Microsoft Forms.
Inclusion Criteria:
- Patients aged 18 years or older;
- Admitted to an ICU;
- Blood cultures taken at least 48 h after hospital admission;
- Growth of an Enterobacterales species resistant to at least carbapenem antibiotics in blood cultures;
- Treated with either CAZ-AVI or PBCT for CRE-BSIs.
Exclusion Criteria:
- Polymicrobial growth in blood cultures;
- Mortality within the first 24 h of CRE treatment or less than 24 h of treatment;
- Patients with a concurrent focus of infection other than CRE-BSIs;
- Concurrent use of polymyxins and CAZ-AVI;
- Use of CAZ-AVI in combination therapy;
- Targeted treatment with an agent to which the pathogen was resistant;
- Patients have incomplete or inaccessible data;
- CRE-BSIs that are resistant to only ertapenem among carbapenem-group drugs (since these two regimens are not recommended primarily in their treatment) [5].
Patient data, including sociodemographic characteristics (age and gender), comorbidities, number of days in hospital before diagnosis of bloodstream infection, Charlson Comorbidity Index score [22], Pitt Bacteremia Score [23], presence of sepsis or septic shock, invasive devices used and their types, the focus of infection according to CDC definitions [24], the type of Enterobacterales species, antimicrobial susceptibility patterns, microbiological eradication within the first seven days of targeted treatments, empirical antibiotics used until blood culture results were available, targeted treatments and their duration, and presence of 30-day mortality were collected retrospectively. The study focused on the impact of ceftazidime–avibactam monotherapy and polymyxin-based combination therapy on 30-day mortality.
4.2. Ethical Approval
Ethical approval was obtained from the Istanbul Medipol University Clinical Research Ethics Committee (date and decision number: 17 July 2023/E-10840098–772.02–4257). The study was conducted in accordance with the 1964 Helsinki Declaration and Good Clinical Practice guidelines. As this was a retrospective observational study, informed consent from patients or their relatives was waived.
4.3. Microbiological Analysis
Blood culture samples were processed using a BacT/ALERT 3D system (bioMérieux, Craponne, France). Positive growth signals were examined via Gram staining and cultured on sheep blood agar, MacConkey agar, and chocolate agar (all from bioMérieux, France). Plates were incubated at 37 °C for 24–48 h. Isolates were identified using a MALDI-TOF MS system (bioMérieux, France). In vitro, antibiotic susceptibility was determined using a VITEK® 2 system (bioMérieux, France) or Phonenix® system (Becton Dickinson, Franklin Lakes, NJ, USA), according to each center’s protocols and based on European Committee on Antimicrobial Susceptibility Testing (EUCAST) criteria [25]. Isolates intermediate or resistant to one or more carbapenem antibiotics were included in the study. Colistin susceptibility was assessed using an MIC-COL kit (Diagnostics, Inc., Galanta, Slovakia). CAZ-AVI susceptibility was determined using the Kirby–Bauer disk diffusion method with ceftazidime–avibactam disks (10/4 microgram) (Oxoid, Basingstoke, UK). Susceptibility thresholds were ≥13 mm for CAZ-AVI and ≤2 µg/mL for colistin.
4.4. Treatment Protocol
CAZ-AVI was administered intravenously as a 2 h infusion at a standard dose of 2/0.5 g every 8 h, while colistin and polymyxin B were administered according to the protocol recommendations, which were based dosage on patients’ body mass index [5]. Doses were adjusted for patients with renal impairment during treatments [26,27].
4.5. Definitions
CRE-BSIs were diagnosed by the isolation of at least one carbapenem-resistant or increased-exposure-susceptible Enterobacterales strain from blood cultures. However, CRE-BSIs caused by isolates with only ertapenem resistance were excluded from the study since the two treatment options were not the priority treatment [5]. Charlson Comorbidity Index [22] and Pitt Bacteremia Score [23] were calculated on the day of blood culture collection. BSIs were categorized as primary or secondary according to CDC/NHSN surveillance definitions [24].
The presence of sepsis or septic shock on the day of diagnosis was determined using the Sequential Organ Failure Assessment (SOFA) score based on Surviving Sepsis Campaign 2021 criteria [28]. Antibiotic regimens administered during the period from blood culture collection to result confirmation were classified as empirical therapy, while treatments directed against CRE were defined as targeted therapy.
The absence of bacterial growth in blood cultures within the first 7 days of targeted therapy was defined as microbiological eradication. Mortality occurring within 30 days from the start of targeted therapy was considered the outcome. A recurrence of BSI with the same bacterium within 30 days of treatment initiation was defined as a relapse. Clinical improvement was defined as the resolution of all clinical and laboratory findings within 30 days after completing the treatment.
Adequate source control was defined as catheter removal within 48 h of blood culture or drainage via surgical or radiological methods in cases of abscesses or fluid collections.
4.6. Statistical Analysis
Data were analyzed using R 4.3.3. [29] and Rstudio [30]. Descriptive statistics were presented as count, percentage, mean, standard deviation, Median, minimum, and maximum values. Statistical hypothesis testing was employed to determine significance based on data type and normality assumptions. Categorical variables were analyzed using Chi-squared or Fisher’s exact tests, while continuous variables were evaluated using either Student’s t-test or the Mann–Whitney U test, depending on the distribution. The study was designed to achieve a statistical power of 80% and a significance level of 0.05.
To mitigate potential selection bias arising from baseline differences between the treatment groups (“PBCT” and “CAZ-AVI”), we employed propensity score matching (PSM) with the “MatchIt” package [31]. The propensity score, which estimates the probability of receiving a specific treatment based on observed covariates, was calculated using logistic regression with a probit link function. The matching process utilized a nearest-neighbor algorithm with a caliper, aiming to pair individuals from the two groups with similar propensity scores. The effectiveness of the matching was assessed by examining the standardized mean differences in covariates before and after matching. Details of the propensity score matching study are provided in the Supplementary Material (Supplement Text S1).
Following successful propensity score matching, we conducted survival analyses to investigate the association between the treatment type and the outcome of interest (30-day mortality). Both univariable and multivariable Cox proportional hazards regression models were employed. The univariable analyses assessed the individual effects of each predictor variable on the outcome, while the multivariable model incorporated multiple predictors simultaneously to evaluate their independent contributions, adjusting for potential confounding effects. The proportional hazards assumption was verified to ensure the validity of the Cox models. The hazard ratios (HRs) and their corresponding 95% confidence intervals were reported to quantify the risk associated with each predictor.
5. Conclusions
In conclusion, our study shows that in an OXA-48-endemic region, CAZ-AVI monotherapy significantly reduces 30-day mortality in CRE-BSIs compared to PBCT. We believe that prioritizing CAZ-AVI over last-resort therapies in this specific context and improving its availability is crucial, especially in regions where access to novel antibiotics is limited.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/antibiotics13100990/s1. Figure S1: Balance of Covariates Before and After Propensity Score Matching. Figure S2: Distribution of Propensity Scores Before and After Matching. Figure S3: Histograms of Propensity Scores for Treated and Control Groups Before and After Matching. Supplement Text S1: Detailed statistical information about probability score matching analysis.
Author Contributions
Conceptualization, R.D., M.Ş., O.D., F.Ş., S.G., A.S.K. and A.M.; Data curation, R.D., Ö.G., S.B., R.Z., Ç.A., F.Ş., S.G. and A.S.K.; Formal analysis, R.D. and O.D.; Investigation, R.D. and A.M.; Methodology, R.D., M.Ş., O.D., Ç.A., F.Ş., S.G., A.S.K. and A.M.; Project administration, R.D.; Resources, R.D.; Software, R.D., M.Ş. and O.D.; Supervision, R.D.; Validation, R.D., O.D. and A.M.; Visualization, R.D.; Writing—original draft, R.D., O.D. and Ç.A.; Writing—review and editing, R.D., M.Ş., Ç.A., and A.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical approval was obtained from the Istanbul Medipol University Clinical Research Ethics Committee (date and decision number: 17 July 2023/E-10840098–772.02–4257). The study was conducted in accordance with the 1964 Helsinki Declaration and Good Clinical Practice guidelines. All study centers obtained managerial approval for the research.
Informed Consent Statement
Patient consent was waived since the study was conducted retrospectively and relied on hospital registry data. All information was handled anonymously.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to administrative reasons but are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- CDC. Healthcare-Associated Infections (HAIs), Carbapenem-Resistant Enterobacterales. Available online: https://www.cdc.gov/cre/about/index.html (accessed on 26 August 2024).
- 2022 Special Report: COVID-19 U.S. Impact on Antimicrobial Resistance. Available online: https://stacks.cdc.gov/view/cdc/119025 (accessed on 26 August 2024).
- Centers for Disease Control and Prevention (CDC). Antibiotic Resistance Threats in the United States, 2019. Available online: https://stacks.cdc.gov/view/cdc/82532 (accessed on 26 August 2024).
- Central Asian and European Surveillance of Antimicrobial Resistance: Annual Report 2023–2021 Data. Available online: https://www.who.int/europe/publications/i/item/9789289058537 (accessed on 19 July 2024).
- Tamma, P.D.; Heil, E.L.; Justo, J.A.; Mathers, A.J.; Satlin, M.J.; Bonomo, R.A. Infectious Diseases Society of America Antimicrobial-Resistant Treatment Guidance: Gram-Negative Bacterial Infections. Infectious Diseases Society of America 2024, Version 4.0. Available online: https://www.idsociety.org/practice-guideline/amr-guidance/ (accessed on 20 August 2024).
- Isler, B.; Özer, B.; Çınar, G.; Aslan, A.T.; Vatansever, C.; Falconer, C.; Dolapçı, İ.; Şimşek, F.; Tülek, N.; Demirkaya, H.; et al. Characteristics and outcomes of carbapenemase harbouring carbapenem-resistant Klebsiella spp. bloodstream infections: A multicentre prospective cohort study in an OXA-48 endemic setting. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Isler, B.; Aslan, A.T.; Akova, M.; Harris, P.; Paterson, D.L. Treatment strategies for OXA-48-like and NDM producing Klebsiella pneumoniae infections. Expert Rev. Anti-Infect. Ther. 2022, 20, 1389–1400. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. NDA Multi-Disciplinary Review and Evaluation—NDA 206494 Supplements 005 and 006 AVYCAZ (Ceftazidime/Avibactam) for Injection. Available online: https://www.fda.gov/media/124307/download (accessed on 20 August 2024).
- European Medicines Agency (EMA). European Public Assessment Report (EPAR) for Zavicefta. Available online: https://www.ema.europa.eu/en/documents/assessment-report/zavicefta-epar-public-assessment-report_en.pdf (accessed on 20 August 2024).
- U.S. Department of Health and Human Services, U.S. Food and Drug Administration, Center for Drug Evaluation and Research (CDER). Guidance for Industry. Hospital-Acquired Bacterial Pneumonia and Ventilator-associated Bacterial Pneumonia: Developing Drugs for Treatment. Available online: https://www.fda.gov/downloads/drugs/guidances/ucm234907.pdf (accessed on 20 August 2024).
- Chen, Y.; Huang, H.; Peng, J.; Weng, L.; Du, B. Efficacy and Safety of Ceftazidime-Avibactam for the Treatment of Carbapenem-Resistant Enterobacterales Bloodstream Infection: A Systematic Review and Meta-Analysis. Microbiol. Spectr. 2022, 10, e02603-21. [Google Scholar] [CrossRef]
- Suay-García, B.; Pérez-Gracia, M.T. Present and Future of Carbapenem-resistant Enterobacteriaceae (CRE) Infections. Antibiotics 2019, 8, 122. [Google Scholar] [CrossRef] [PubMed]
- Taggar, G.; Rehman, M.A.; Boerlin, P.; Diarra, M.S. Molecular Epidemiology of Carbapenemases in Enterobacteriales from Humans, Animals, Food, and the Environment. Antibiotics 2020, 9, 693. [Google Scholar] [CrossRef] [PubMed]
- Hakeam, H.A.; Alsahli, H.; Albabtain, L.; Alassaf, S.; Al Duhailib, Z.; Althawadi, S. Effectiveness of Ceftazidime-Avibactam Versus Colistin in Treating Carbapenem-Resistant Enterobacteriaceae Bacteremia. Int. J. Infect. Dis. 2021, 109, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lima, O.; Sousa, A.; Longueira-Suárez, R.; Filgueira, A.; Taboada-Martínez, C.; Portela-Pino, C.; Nodar, A.; Vasallo-Vidal, F.; Martinez-Lamas, L.; Pérez-Landeiro, A.; et al. Ceftazidime-Avibactam Treatment in Bacteremia Caused by OXA-48 Carbapenemase-Producing Klebsiella pneumoniae. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Balkan, I.I.; Aygün, G.; Aydın, S.; Mutcalı, S.I.; Kara, Z.; Kuşkucu, M.; Midilli, K.; Şemen, V.; Aras, S.; Yemişen, M.; et al. Blood Stream Infections due to OXA-48-Like Carbapenemase-Producing Enterobacteriaceae: Treatment and Survival. Int. J. Infect. Dis. 2014, 26, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Dumlu, R.; Şahin, M.; Derin, O.; Gül, Ö.; Başgönül, S.; Zengin, R.; Arabacı, Ç.; Şimşek, F.; Gençer, S.; Kocagöz, S.; et al. Ceftazidime-Avibactam versus Polymyxin-Based Therapies: A Study on 30-Day Mortality in Carbapenem-Resistant Enterobacterales Bloodstream Infections in an OXA-48 Endemic Region. In Proceedings of the 33rd International Congress of Antimicrobial Chemotherapy (ICC 2024), Istanbul, Turkey, 3–6 November 2024. [Google Scholar]
- Chen, J.; Hu, Q.; Zhou, P.; Deng, S. Ceftazidime-Avibactam Versus Polymyxins in Treating Patients with Carbapenem-Resistant Enterobacteriaceae Infections: A Systematic Review and Meta-Analysis. Infection 2024, 52, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Tiseo, G.; Carbonara, S.; Marino, A.; Di Caprio, G.; Carretta, A.; Mularoni, A.; Mariani, M.F.; Maraolo, A.E.; Scotto, R.; et al. Mortality Attributable to Bloodstream Infections Caused by Different Carbapenem-Resistant Gram-Negative Bacilli: Results from a Nationwide Study in Italy (ALARICO Network). Clin. Infect. Dis. 2023, 76, 2059–2069. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Chen, Y.; Liu, P.; Guo, P.; Wu, Z.; Peng, Y.; Deng, J.; Kong, Y.; Cui, Y.; Liao, K.; et al. Risk Factors and Mortality for Elderly Patients with Bloodstream Infection of Carbapenem-Resistant Klebsiella pneumoniae: A 10-Year Longitudinal Study. BMC Geriatr. 2022, 22, 573. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Bassetti, M.; Tiseo, G.; Giordano, C.; Nencini, E.; Russo, A.; Graziano, E.; Tagliaferri, E.; Leonildi, A.; Barnini, S.; et al. Time to Appropriate Antibiotic Therapy Is a Predictor of Outcome in Patients with Bloodstream Infection Caused by KPC-Producing Klebsiella pneumoniae. Crit. Care 2020, 24, 29. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Al-Hasan, M.N.; Baddour, L.M. Resilience of the Pitt Bacteremia Score: 3 Decades and Counting. Clin. Infect. Dis. 2020, 70, 1834–1836. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. CDC/NHSN Surveillance Definitions for Specific Types of Infections. Available online: https://www.cdc.gov/nhsn/pdfs/pscmanual/17pscnosinfdef_current.pdf (accessed on 20 June 2024).
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 14.0. Available online: http://www.eucast.org (accessed on 20 June 2024).
- Forest Pharmaceuticals, Inc. Avycaz (Ceftazidime/Avibactam) Prescribing Information; Forest Pharmaceuticals, Inc.: Cincinnati, OH, USA, 2016; Available online: http://www.allergan.com/assets/pdf/avycaz_pi (accessed on 20 June 2023).
- Tsuji, B.T.; Pogue, J.M.; Zavascki, A.P.; Paul, M.; Daikos, G.L.; Forrest, A.; Giacobbe, D.R.; Viscoli, C.; Giamarellou, H.; Karaiskos, I.; et al. International Consensus Guidelines for the Optimal Use of the Polymyxins: Endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy 2019, 39, 10–39. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2024; Available online: https://www.R-project.org/ (accessed on 15 June 2024).
- Posit Team. RStudio: Integrated Development Environment for R; Posit Software, PBC: Boston, MA, USA, 2024; Available online: http://www.posit.co/ (accessed on 15 June 2024).
- Ho, D.; Imai, K.; King, G.; Stuart, E. MatchIt: Nonparametric Preprocessing for Parametric Causal Inference. J. Stat. Softw. 2011, 42, 1–28. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).