

Deciphering the Intricate Interplay in the Framework of Antibiotic-Drug Interactions: A Narrative Review

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Methodology of Research
3. Overview of Antibiotics
4. Antibiotic-Drug Interactions
Antibiotic-Drug Interactions in the Geriatric Population
5. Online Tools in Antibiotic-Drug Interactions
Antibiotic-Antibiotic Combinations Targeting ESKAPE Pathogens
6. Future Perspectives in Antibiotic-Drug Interactions
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Halawa, E.M.; Fadel, M.; Al-Rabia, M.W.; Behairy, A.; Nouh, N.A.; Abdo, M.; Olga, R.; Fericean, L.; Atwa, A.M.; El-Nablaway, M.; et al. Antibiotic Action and Resistance: Updated Review of Mechanisms, Spread, Influencing Factors, and Alternative Approaches for Combating Resistance. Front. Pharmacol. 2023, 14, 1305294. [Google Scholar] [CrossRef] [PubMed]
- Bacanlı, M.G. The Two Faces of Antibiotics: An Overview of the Effects of Antibiotic Residues in Foodstuffs. Arch. Toxicol. 2024, 98, 1717–1725. [Google Scholar] [CrossRef]
- Aminov, R.I. A Brief History of the Antibiotic Era: Lessons Learned and Challenges for the Future. Front. Microbiol. 2010, 1, 134. [Google Scholar] [CrossRef] [PubMed]
- Browne, A.J.; Chipeta, M.G.; Haines-Woodhouse, G.; Kumaran, E.P.A.; Hamadani, B.H.K.; Zaraa, S.; Henry, N.J.; Deshpande, A.; Reiner, R.C.J.; Day, N.P.J.; et al. Global Antibiotic Consumption and Usage in Humans, 2000–2018: A Spatial Modelling Study. Lancet Planet. Health 2021, 5, e893–e904. [Google Scholar] [CrossRef]
- Chin, K.W.; Michelle Tiong, H.L.; Luang-In, V.; Ma, N.L. An Overview of Antibiotic and Antibiotic Resistance. Environ. Adv. 2023, 11, 100331. [Google Scholar] [CrossRef]
- Emblaveo®, a New Antibiotic to Fight Infections Caused by Multidrug-Resistant Bacteria Approved by the European Medicines Agency. Available online: https://www.ema.europa.eu/en/news/new-antibiotic-fight-infections-caused-multidrug-resistant-bacteria (accessed on 5 August 2024).
- Zevtera®, a New Antibiotic for Three Different Uses Approved by the United States Food and Drug Administration. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-new-antibiotic-three-different-uses (accessed on 5 August 2024).
- Singh, S.B.; Young, K.; Silver, L.L. What Is an “Ideal” Antibiotic? Discovery Challenges and Path Forward. Biochem. Pharmacol. 2017, 133, 63–73. [Google Scholar] [CrossRef]
- Gajdács, M. The Concept of an Ideal Antibiotic: Implications for Drug Design. Molecules 2019, 24, 892. [Google Scholar] [CrossRef] [PubMed]
- Zaha, D.C.; Bungau, S.; Aleya, S.; Tit, D.M.; Vesa, C.M.; Popa, A.R.; Pantis, C.; Maghiar, O.A.; Bratu, O.G.; Furau, C.; et al. What Antibiotics for What Pathogens? The Sensitivity Spectrum of Isolated Strains in an Intensive Care Unit. Sci. Total Environ. 2019, 687, 118–127. [Google Scholar] [CrossRef]
- Christaki, E.; Marcou, M.; Tofarides, A. Antimicrobial Resistance in Bacteria: Mechanisms, Evolution, and Persistence. J. Mol. Evol. 2020, 88, 26–40. [Google Scholar] [CrossRef]
- Pulingam, T.; Parumasivam, T.; Gazzali, A.M.; Sulaiman, A.M.; Chee, J.Y.; Lakshmanan, M.; Chin, C.F.; Sudesh, K. Antimicrobial Resistance: Prevalence, Economic Burden, Mechanisms of Resistance and Strategies to Overcome. Eur. J. Pharm. Sci. 2022, 170, 106103. [Google Scholar] [CrossRef]
- de la Fuente-Nunez, C.; Cesaro, A.; Hancock, R.E.W. Antibiotic Failure: Beyond Antimicrobial Resistance. Drug Resist. Updat. 2023, 71, 101012. [Google Scholar] [CrossRef] [PubMed]
- Fishbein, S.R.S.; Mahmud, B.; Dantas, G. Antibiotic Perturbations to the Gut Microbiome. Nat. Rev. Microbiol. 2023, 21, 772–788. [Google Scholar] [CrossRef] [PubMed]
- Kuehl, R.; Morata, L.; Meylan, S.; Mensa, J.; Soriano, A. When Antibiotics Fail: A Clinical and Microbiological Perspective on Antibiotic Tolerance and Persistence of Staphylococcus Aureus. J. Antimicrob. Chemother. 2020, 75, 1071–1086. [Google Scholar] [CrossRef] [PubMed]
- Hodel, M.; Genné, D. Antibiotics: Drug and food interactions. Rev. Med. Suisse 2009, 5, 1979–1984. [Google Scholar]
- Cattaneo, D.; Gervasoni, C.; Corona, A. The Issue of Pharmacokinetic-Driven Drug-Drug Interactions of Antibiotics: A Narrative Review. Antibiotics 2022, 11, 1410. [Google Scholar] [CrossRef] [PubMed]
- Hakkola, J.; Hukkanen, J.; Turpeinen, M.; Pelkonen, O. Inhibition and Induction of CYP Enzymes in Humans: An Update. Arch. Toxicol. 2020, 94, 3671–3722. [Google Scholar] [CrossRef]
- Khatib, R.; Sabir, F.R.N.; Omari, C.; Pepper, C.; Tayebjee, M.H. Managing Drug-Induced QT Prolongation in Clinical Practice. Postgrad. Med. J. 2021, 97, 452–458. [Google Scholar] [CrossRef]
- Wiggins, B.S.; Saseen, J.J.; Page, R.L., 2nd; Reed, B.N.; Sneed, K.; Kostis, J.B.; Lanfear, D.; Virani, S.; Morris, P.B. Recommendations for Management of Clinically Significant Drug-Drug Interactions with Statins and Select Agents Used in Patients With Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e468–e495. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration. Preventable Adverse Drug Reactions: A Focus on Drug Interactions. Available online: https://www.fda.gov/drugs/drug-interactions-labeling/preventable-adverse-drug-reactions-focus-drug-interactions (accessed on 9 August 2024).
- Bhattacharjee, M.K. Chemistry of Antibiotics and Related Drugs; Springer: Cham, Switzerland, 2022; ISBN 978-3-031-07582-7. [Google Scholar]
- Villa Zapata, L.; Hansten, P.D.; Horn, J.R.; Boyce, R.D.; Gephart, S.; Subbian, V.; Romero, A.; Malone, D.C. Evidence of Clinically Meaningful Drug-Drug Interaction with Concomitant Use of Colchicine and Clarithromycin. Drug Saf. 2020, 43, 661–668. [Google Scholar] [CrossRef]
- Laatikainen, O.; Sneck, S.; Turpeinen, M. Medication-Related Adverse Events in Health Care-What Have We Learned? A Narrative Overview of the Current Knowledge. Eur. J. Clin. Pharmacol. 2022, 78, 159–170. [Google Scholar] [CrossRef]
- Obreli-Neto, P.R.; Nobili, A.; de Oliveira Baldoni, A.; Guidoni, C.M.; de Lyra Júnior, D.P.; Pilger, D.; Duzanski, J.; Tettamanti, M.; Cruciol-Souza, J.M.; Gaeti, W.P.; et al. Adverse Drug Reactions Caused by Drug-Drug Interactions in Elderly Outpatients: A Prospective Cohort Study. Eur. J. Clin. Pharmacol. 2012, 68, 1667–1676. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Yin, J.; Zhang, L.; Zhang, Y.; Chen, X. Drug-Drug Interaction Prediction: Databases, Web Servers and Computational Models. Brief. Bioinform. 2023, 25, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Katz, L.; Baltz, R.H. Natural Product Discovery: Past, Present, and Future. J. Ind. Microbiol. Biotechnol. 2016, 43, 155–176. [Google Scholar] [CrossRef] [PubMed]
- Darby, E.M.; Trampari, E.; Siasat, P.; Gaya, M.S.; Alav, I.; Webber, M.A.; Blair, J.M.A. Molecular Mechanisms of Antibiotic Resistance Revisited. Nat. Rev. Microbiol. 2023, 21, 280–295. [Google Scholar] [CrossRef] [PubMed]
- Abbas, A.; Barkhouse, A.; Hackenberger, D.; Wright, G.D. Antibiotic Resistance: A Key Microbial Survival Mechanism That Threatens Public Health. Cell Host Microbe 2024, 32, 837–851. [Google Scholar] [CrossRef]
- Kapoor, G.; Saigal, S.; Elongavan, A. Action and Resistance Mechanisms of Antibiotics: A Guide for Clinicians. J. Anaesthesiol. Clin. Pharmacol. 2017, 33, 300–305. [Google Scholar] [CrossRef]
- Sahu, U.; Khare, P. Antibiotics: Action Mechanism and Modern Challenges. In Developments in Applied Microbiology and Biotechnology; Chandra Pandey, S., Pande, V., Sati, D., Samant, M., Eds.; Academic Press: Cambridge, MA, USA, 2023; pp. 281–292. ISBN 978-0-323-91643-1. [Google Scholar]
- Upmanyu, N.; Malviya, V.N. Antibiotics: Mechanisms of Action and Modern Challenges. In Microorganisms for Sustainable Environment and Health; Chowdhary, P., Raj, A., Verma, D., Akhter, Y., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 367–382. ISBN 978-0-12-819001-2. [Google Scholar]
- Etebu, E.; Arikekpar, I. Antibiotics: Classification and Mechanisms of Action with Emphasis on Molecular Perspectives. Int. J. Appl. Microbiol. Biotechnol. Res. 2016, 4, 90–101. [Google Scholar]
- Eyler, R.F.; Shvets, K. Clinical Pharmacology of Antibiotics. Clin. J. Am. Soc. Nephrol. 2019, 14, 1080–1090. [Google Scholar] [CrossRef]
- Lewis, K.; Lee, R.E.; Brötz-Oesterhelt, H.; Hiller, S.; Rodnina, M.V.; Schneider, T.; Weingarth, M.; Wohlgemuth, I. Sophisticated Natural Products as Antibiotics. Nature 2024, 632, 39–49. [Google Scholar] [CrossRef]
- Quinn, G.A.; Banat, A.M.; Abdelhameed, A.M.; Banat, I.M. Streptomyces from Traditional Medicine: Sources of New Innovations in Antibiotic Discovery. J. Med. Microbiol. 2020, 69, 1040–1048. [Google Scholar] [CrossRef]
- Abdallah, E.M.; Alhatlani, B.Y.; de Paula Menezes, R.; Martins, C.H.G. Back to Nature: Medicinal Plants as Promising Sources for Antibacterial Drugs in the Post-Antibiotic Era. Plants 2023, 12, 3077. [Google Scholar] [CrossRef] [PubMed]
- Pancu, D.F.; Scurtu, A.; Macasoi, I.G.; Marti, D.; Mioc, M.; Soica, C.; Coricovac, D.; Horhat, D.; Poenaru, M.; Dehelean, C. Antibiotics: Conventional Therapy and Natural Compounds with Antibacterial Activity-A Pharmaco-Toxicological Screening. Antibiotics 2021, 10, 401. [Google Scholar] [CrossRef] [PubMed]
- Bernatová, S.; Samek, O.; Pilát, Z.; Serý, M.; Ježek, J.; Jákl, P.; Siler, M.; Krzyžánek, V.; Zemánek, P.; Holá, V.; et al. Following the Mechanisms of Bacteriostatic versus Bactericidal Action Using Raman Spectroscopy. Molecules 2013, 18, 13188–13199. [Google Scholar] [CrossRef]
- Hutchings, M.I.; Truman, A.W.; Wilkinson, B. Antibiotics: Past, Present and Future. Curr. Opin. Microbiol. 2019, 51, 72–80. [Google Scholar] [CrossRef]
- Pai, M.; Kiser, J.J.; Gubbins, P.O.; Rodvold, K.A. Drug Interactions in Infectious Diseases: Antimicrobial Drug Interactions, 4th ed.; Humana: Cham, Switzerland, 2018; ISBN 978-3-319-72416-4. [Google Scholar]
- Wald-Dickler, N.; Holtom, P.; Spellberg, B. Busting the Myth of “Static vs Cidal”: A Systemic Literature Review. Clin. Infect. Dis. 2018, 66, 1470–1474. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Zhang, J.; Tian, L.; Xin, L.; Liang, C.; Ren, X.; Li, M. A Comprehensive Overview of the Antibiotics Approved in the Last Two Decades: Retrospects and Prospects. Molecules 2023, 28, 1762. [Google Scholar] [CrossRef]
- Li, B.; Liu, Y.; Luo, J.; Cai, Y.; Chen, M.; Wang, T. Contezolid, a Novel Oxazolidinone Antibiotic, May Improve Drug-Related Thrombocytopenia in Clinical Antibacterial Treatment. Front. Pharmacol. 2023, 14, 1157437. [Google Scholar] [CrossRef]
- Wang, Y.-T.; Yang, P.-C.; Zhang, Y.-F.; Sun, J.-F. Synthesis and Clinical Application of New Drugs Approved by FDA in 2023. Eur. J. Med. Chem. 2024, 265, 116124. [Google Scholar] [CrossRef]
- Lupia, T.; Pallotto, C.; Corcione, S.; Boglione, L.; De Rosa, F.G. Ceftobiprole Perspective: Current and Potential Future Indications. Antibiotics 2021, 10, 170. [Google Scholar] [CrossRef]
- FDA Novel Drug Therapy Approvals for 2024. Available online: https://www.fda.gov/drugs/novel-drug-approvals-fda/novel-drug-approvals-2024 (accessed on 6 August 2024).
- Pereira, J.M.; Paiva, J.A. Antimicrobial Drug Interactions in the Critically Ill Patients. Curr. Clin. Pharmacol. 2013, 8, 25–38. [Google Scholar]
- Radkowski, P.; Derkaczew, M.; Mazuchowski, M.; Moussa, A.; Podhorodecka, K.; Dawidowska-Fidrych, J.; Braczkowska-Skibińska, M.; Synia, D.; Śliwa, K.; Wiszpolska, M.; et al. Antibiotic–Drug Interactions in the Intensive Care Unit: A Literature Review. Antibiotics 2024, 13, 503. [Google Scholar] [CrossRef] [PubMed]
- Le Louët, H.; Pitts, P.J. Twenty-First Century Global ADR Management: A Need for Clarification, Redesign, and Coordinated Action. Ther. Innov. Regul. Sci. 2023, 57, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Lin, Y.; Ren, W.; Fang, Z.; Liu, Y.; Tan, X.; Lv, X.; Zhang, N. Adverse Drug Reactions and Correlations with Drug-Drug Interactions: A Retrospective Study of Reports from 2011 to 2020. Front. Pharmacol. 2022, 13, 923939. [Google Scholar] [CrossRef] [PubMed]
- Sultana, J.; Cutroneo, P.; Trifirò, G. Clinical and Economic Burden of Adverse Drug Reactions. J. Pharmacol. Pharmacother. 2013, 4, S73–S77. [Google Scholar] [CrossRef]
- Durand, M.; Castelli, C.; Roux-Marson, C.; Kinowski, J.-M.; Leguelinel-Blache, G. Evaluating the Costs of Adverse Drug Events in Hospitalized Patients: A Systematic Review. Health Econ. Rev. 2024, 14, 11. [Google Scholar] [CrossRef]
- Slight, S.P.; Seger, D.L.; Franz, C.; Wong, A.; Bates, D.W. The National Cost of Adverse Drug Events Resulting from Inappropriate Medication-Related Alert Overrides in the United States. J. Am. Med. Inform. Assoc. 2018, 25, 1183–1188. [Google Scholar] [CrossRef]
- Kovačević, M.; Vezmar Kovačević, S.; Radovanović, S.; Stevanović, P.; Miljković, B. Adverse Drug Reactions Caused by Drug-Drug Interactions in Cardiovascular Disease Patients: Introduction of a Simple Prediction Tool Using Electronic Screening Database Items. Curr. Med. Res. Opin. 2019, 35, 1873–1883. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.Y.; Richardson, L.C.; Li, L.; Day, R.O.; Westbrook, J.I.; Baysari, M.T. Drug-Drug Interactions and Their Harmful Effects in Hospitalised Patients: A Systematic Review and Meta-Analysis. Eur. J. Clin. Pharmacol. 2018, 74, 15–27. [Google Scholar] [CrossRef]
- Wang, Y.; Yang, Z.; Yao, Q. Accurate and Interpretable Drug-Drug Interaction Prediction Enabled by Knowledge Subgraph Learning. Commun. Med. 2024, 4, 59. [Google Scholar] [CrossRef] [PubMed]
- Pai, M.; Kiser, J.J.; Gubbins, P.O.; Rodvold, K.A. Drug Interactions in Infectious Diseases: Mechanisms and Models of Drug Interactions, 4th ed.; Humana: Cham, Switzerland, 2018; ISBN 978-3-319-72422-5. [Google Scholar]
- Baniasadi, S.; Farzanegan, B.; Alehashem, M. Important Drug Classes Associated with Potential Drug-Drug Interactions in Critically Ill Patients: Highlights for Cardiothoracic Intensivists. Ann. Intensive Care 2015, 5, 44. [Google Scholar] [CrossRef]
- Shetty, V.; Chowta, M.N.; Chowta, K.N.; Shenoy, A.; Kamath, A.; Kamath, P. Evaluation of Potential Drug-Drug Interactions with Medications Prescribed to Geriatric Patients in a Tertiary Care Hospital. J. Aging Res. 2018, 2018, 5728957. [Google Scholar] [CrossRef] [PubMed]
- Min, J.S.; Bae, S.K. Prediction of Drug-Drug Interaction Potential Using Physiologically Based Pharmacokinetic Modeling. Arch. Pharm. Res. 2017, 40, 1356–1379. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Hisaka, A.; Ito, K.; Ohno, Y.; Ishiguro, A.; Sato, R.; Nagai, N. Classification of Drugs for Evaluating Drug Interaction in Drug Development and Clinical Management. Drug Metab. Pharmacokinet. 2021, 41, 100414. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, T.; Gomes, T.; Mamdani, M.M.; Juurlink, D.N. Ciprofloxacin-Induced Theophylline Toxicity: A Population-Based Study. Eur. J. Clin. Pharmacol. 2011, 67, 521–526. [Google Scholar] [CrossRef]
- Ferner, R.E. Adverse Drug Interactions: A Handbook for Prescribers; Hodder Education Group: London, UK, 2011; Volume 71, ISBN 9780340927694. [Google Scholar]
- McCance-Katz, E.F.; Sullivan, L.E.; Nallani, S. Drug Interactions of Clinical Importance among the Opioids, Methadone and Buprenorphine, and Other Frequently Prescribed Medications: A Review. Am. J. Addict. 2010, 19, 4–16. [Google Scholar] [CrossRef]
- Federico, S.; Carrano, R.; Capone, D.; Gentile, A.; Palmiero, G.; Basile, V. Pharmacokinetic Interaction between Levofloxacin and Ciclosporin or Tacrolimus in Kidney Transplant Recipients: Ciclosporin, Tacrolimus and Levofloxacin in Renal Transplantation. Clin. Pharmacokinet. 2006, 45, 169–175. [Google Scholar] [CrossRef]
- Althaqafi, A.; Ali, M.; Alzahrani, Y.; Ming, L.C.; Hussain, Z. How Safe Are Fluoroquinolones for Diabetic Patients? A Systematic Review of Dysglycemic and Neuropathic Effects of Fluoroquinolones. Ther. Clin. Risk Manag. 2021, 17, 1083–1090. [Google Scholar] [CrossRef]
- Vega, A.J.; Smith, C.; Matejowsky, H.G.; Thornhill, K.J.; Borne, G.E.; Mosieri, C.N.; Shekoohi, S.; Cornett, E.M.; Kaye, A.D. Warfarin and Antibiotics: Drug Interactions and Clinical Considerations. Life 2023, 13, 1661. [Google Scholar] [CrossRef]
- Patocka, J.; Nepovimova, E.; Wu, W.; Kuca, K. Digoxin: Pharmacology and Toxicology—A Review. Environ. Toxicol. Pharmacol. 2020, 79, 103400. [Google Scholar] [CrossRef] [PubMed]
- Al-Quteimat, O.; Laila, A. Valproate Interaction With Carbapenems: Review and Recommendations. Hosp. Pharm. 2020, 55, 181–187. [Google Scholar] [CrossRef]
- Huang, C.-R.; Lin, C.-H.; Hsiao, S.-C.; Chen, N.-C.; Tsai, W.-C.; Chen, S.-D.; Lu, Y.-T.; Chuang, Y.-C. Drug Interaction between Valproic Acid and Carbapenems in Patients with Epileptic Seizures. Kaohsiung J. Med. Sci. 2017, 33, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Terkeltaub, R.A.; Furst, D.E.; Digiacinto, J.L.; Kook, K.A.; Davis, M.W. Novel Evidence-Based Colchicine Dose-Reduction Algorithm to Predict and Prevent Colchicine Toxicity in the Presence of Cytochrome P450 3A4/P-Glycoprotein Inhibitors. Arthritis Rheum. 2011, 63, 2226–2237. [Google Scholar] [CrossRef] [PubMed]
- Bolhuis, M.S.; Panday, P.N.; Pranger, A.D.; Kosterink, J.G.W.; Alffenaar, J.-W.C. Pharmacokinetic Drug Interactions of Antimicrobial Drugs: A Systematic Review on Oxazolidinones, Rifamycines, Macrolides, Fluoroquinolones, and Beta-Lactams. Pharmaceutics 2011, 3, 865–913. [Google Scholar] [CrossRef]
- Lonks, J.R.; Goldmann, D.A.; Saravolatz, L.D. Telithromycin: A Ketolide Antibiotic for Treatment of Respiratory Tract Infections. Clin. Infect. Dis. 2005, 40, 1657–1664. [Google Scholar] [CrossRef]
- Oude Munnink, T.H.; Demmer, A.; Slenter, R.H.J.; Movig, K.L.L. Amiodarone Rifampicin Drug-Drug Interaction Management With Therapeutic Drug Monitoring. Ther. Drug Monit. 2018, 40, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Srinivas, N.R. Pharmacokinetic Interaction of Rifampicin with Oral Versus Intravenous Anticancer Drugs: Challenges, Dilemmas and Paradoxical Effects Due to Multiple Mechanisms. Drugs R D 2016, 16, 141–148. [Google Scholar] [CrossRef]
- Hebenstreit, D.; Pichler, R.; Heidegger, I. Drug-Drug Interactions in Prostate Cancer Treatment. Clin. Genitourin. Cancer 2020, 18, e71–e82. [Google Scholar] [CrossRef] [PubMed]
- Nakou, E.S.; Marketou, M.E.; Vardas, P.E.; Parthenakis, F.I. The Clinical Relevance of Drug–Drug Interaction between Co-Trimoxazole and Sacubitril/Valsartan Treatment in a Heart Failure Patient: A Case Report and Overview of Mechanisms and Management in Clinical Practice. Clin. Res. Cardiol. 2018, 107, 524–526. [Google Scholar] [CrossRef]
- Nutescu, E.; Chuatrisorn, I.; Hellenbart, E. Drug and Dietary Interactions of Warfarin and Novel Oral Anticoagulants: An Update. J. Thromb. Thrombolysis 2011, 31, 326–343. [Google Scholar] [CrossRef]
- Bezabeh, S.; Mackey, A.C.; Kluetz, P.; Jappar, D.; Korvick, J. Accumulating Evidence for a Drug-Drug Interaction between Methotrexate and Proton Pump Inhibitors. Oncologist 2012, 17, 550–554. [Google Scholar] [CrossRef]
- May, M.; Schindler, C. Clinically and Pharmacologically Relevant Interactions of Antidiabetic Drugs. Ther. Adv. Endocrinol. Metab. 2016, 7, 69–83. [Google Scholar] [CrossRef] [PubMed]
- Corsini Campioli, C.; Barth, D.; Esquer Garrigos, Z.; Abu Saleh, O.; Sohail, R.M.; Sia, I.G. Linezolid and Fentanyl: An Underrecognized Drug-to-Drug Interaction. J. Clin. Pharm. Ther. 2020, 45, 825–827. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.H. Interpretation of Drug Interaction Using Systemic and Local Tissue Exposure Changes. Pharmaceutics 2020, 12, 417. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Cheng, Z.; Xie, F. Evaluation of Pharmacokinetic Drug-Drug Interactions: A Review of the Mechanisms, In Vitro and In Silico Approaches. Metabolites 2021, 11, 75. [Google Scholar] [CrossRef] [PubMed]
- Micheli, L.; Sbrilli, M.; Nencini, C. Severe Hypoglycemia Associated with Levofloxacin in Type 2 Diabetic Patients Receiving Polytherapy: Two Case Reports. Int. J. Clin. Pharmacol. Ther. 2012, 50, 302–306. [Google Scholar] [CrossRef]
- Steyger, P.S. Mechanisms of Ototoxicity and Otoprotection. Otolaryngol. Clin. N. Am. 2021, 54, 1101–1115. [Google Scholar] [CrossRef]
- Rivetti, S.; Romano, A.; Mastrangelo, S.; Attinà, G.; Maurizi, P.; Ruggiero, A. Aminoglycosides-Related Ototoxicity: Mechanisms, Risk Factors, and Prevention in Pediatric Patients. Pharmaceuticals 2023, 16, 1353. [Google Scholar] [CrossRef]
- Davis, M.T.; Eaton, M.P. Physiology of Skeletal Muscle and the Neuromuscular Junction. In Pediatric Critical Care: Text and Study Guide; Lucking, S.E., Maffei, F.A., Tamburro, R.F., Zaritsky, A., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 677–688. ISBN 978-3-030-53363-2. [Google Scholar]
- Wu, Y.; Bi, W.-T.; Qu, L.-P.; Fan, J.; Kong, X.-J.; Ji, C.-C.; Chen, X.-M.; Yao, F.-J.; Liu, L.-J.; Cheng, Y.-J.; et al. Administration of Macrolide Antibiotics Increases Cardiovascular Risk. Front. Cardiovasc. Med. 2023, 10, 1117254. [Google Scholar] [CrossRef]
- Sharma, S.K.; Sharma, A.; Kadhiravan, T.; Tharyan, P. Rifamycins (Rifampicin, Rifabutin and Rifapentine) Compared to Isoniazid for Preventing Tuberculosis in HIV-Negative People at Risk of Active TB. Cochrane Database Syst. Rev. 2013, 2013, CD007545. [Google Scholar] [CrossRef]
- Asaumi, R.; Menzel, K.; Lee, W.; Nunoya, K.-I.; Imawaka, H.; Kusuhara, H.; Sugiyama, Y. Expanded Physiologically-Based Pharmacokinetic Model of Rifampicin for Predicting Interactions With Drugs and an Endogenous Biomarker via Complex Mechanisms Including Organic Anion Transporting Polypeptide 1B Induction. CPT Pharmacomet. Syst. Pharmacol. 2019, 8, 845–857. [Google Scholar] [CrossRef]
- Niemi, M.; Backman, J.T.; Fromm, M.F.; Neuvonen, P.J.; Kivistö, K.T. Pharmacokinetic Interactions with Rifampicin: Clinical Relevance. Clin. Pharmacokinet. 2003, 42, 819–850. [Google Scholar] [CrossRef] [PubMed]
- Rabi, R.; Enaya, A.; Sweileh, M.W.; Aiesh, B.M.; Namrouti, A.; Hamdan, Z.I.; Abugaber, D.; Nazzal, Z. Comprehensive Assessment of Colistin Induced Nephrotoxicity: Incidence, Risk Factors and Time Course. Infect. Drug Resist. 2023, 16, 3007–3017. [Google Scholar] [CrossRef]
- Kwiatkowska, E.; Domański, L.; Dziedziejko, V.; Kajdy, A.; Stefańska, K.; Kwiatkowski, S. The Mechanism of Drug Nephrotoxicity and the Methods for Preventing Kidney Damage. Int. J. Mol. Sci. 2021, 22, 6109. [Google Scholar] [CrossRef]
- Lane, M.A.; Zeringue, A.; McDonald, J.R. Serious Bleeding Events Due to Warfarin and Antibiotic Co-Prescription in a Cohort of Veterans. Am. J. Med. 2014, 127, 657–663.e2. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.T.; Gentry, C.A.; Furrh, R.Z. A Comparison of Adverse Drug Reactions between High- and Standard-Dose Trimethoprim-Sulfamethoxazole in the Ambulatory Setting. Curr. Drug Saf. 2013, 8, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Gentry, C.A.; Nguyen, A.T. An Evaluation of Hyperkalemia and Serum Creatinine Elevation Associated with Different Dosage Levels of Outpatient Trimethoprim-Sulfamethoxazole with and without Concomitant Medications. Ann. Pharmacother. 2013, 47, 1618–1626. [Google Scholar] [CrossRef]
- Rodvold, K.A.; McConeghy, K.W. Methicillin-Resistant Staphylococcus Aureus Therapy: Past, Present, and Future. Clin. Infect. Dis. 2014, 58, 20–27. [Google Scholar] [CrossRef]
- Kim, J.Y.; Yee, J.; Yoon, H.Y.; Han, J.M.; Gwak, H.S. Risk Factors for Vancomycin-Associated Acute Kidney Injury: A Systematic Review and Meta-Analysis. Br. J. Clin. Pharmacol. 2022, 88, 3977–3989. [Google Scholar] [CrossRef]
- Guerra, W.; Silva-Caldeira, P.P.; Terenzi, H.; Pereira-Maia, E.C. Impact of Metal Coordination on the Antibiotic and Non-Antibiotic Activities of Tetracycline-Based Drugs. Coord. Chem. Rev. 2016, 327–328, 188–199. [Google Scholar] [CrossRef]
- Arslan, A.; Zain, M.A.; Mukhtar, M.; Ullah, W.; Roomi, S. Methotrexate and Doxycycline Interaction: A Rare Cause of Pancytopenia. BMJ Case Rep. 2019, 12, e229296. [Google Scholar] [CrossRef]
- Ramsey, T.D.; Lau, T.T.; Ensom, M.H. Serotonergic and Adrenergic Drug Interactions Associated with Linezolid: A Critical Review and Practical Management Approach. Ann. Pharmacother. 2013, 47, 543–560. [Google Scholar] [CrossRef]
- Douros, A.; Grabowski, K.; Stahlmann, R. Drug-Drug Interactions and Safety of Linezolid, Tedizolid, and Other Oxazolidinones. Expert Opin. Drug Metab. Toxicol. 2015, 11, 1849–1859. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, R.A.; Vandenberg, A.M.; Canepa, E.A. Serotonergic Antidepressants and Linezolid: A Retrospective Chart Review and Presentation of Cases. Int. J. Psychiatry Med. 2008, 38, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Occhineri, S.; Matucci, T.; Rindi, L.; Tiseo, G.; Falcone, M.; Riccardi, N.; Besozzi, G. Pretomanid for Tuberculosis Treatment: An Update for Clinical Purposes. Curr. Res. Pharmacol. Drug Discov. 2022, 3, 100128. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.-X.-Z.; Liu, T.-T.; Ren, A.-X.; Liang, W.-X.; Yin, H.; Cai, Y. Advances in Contezolid: Novel Oxazolidinone Antibacterial in Gram-Positive Treatment. Infection 2024, 52, 787–800. [Google Scholar] [CrossRef] [PubMed]
- Hammar, T.; Hamqvist, S.; Zetterholm, M.; Jokela, P.; Ferati, M. Current Knowledge about Providing Drug-Drug Interaction Services for Patients—A Scoping Review. Pharmacy 2021, 9, 69. [Google Scholar] [CrossRef] [PubMed]
- Dahri, K.; Araujo, L.; Chen, S.; Bagri, H.; Walia, K.; Lau, L.; Legal, M. Community Pharmacist Perceptions of Drug-Drug Interactions. Can. Pharm. J. 2023, 156, 42–47. [Google Scholar] [CrossRef]
- Hamadouk, R.M.; Albashair, E.D.; Mohammed, F.M.; Yousef, B.A. The Practice of the Community Pharmacists in Managing Potential Drug-Drug Interactions: A Simulated Patient Visits. Integr. Pharm. Res. Pract. 2022, 11, 71–84. [Google Scholar] [CrossRef]
- Ansari, J. Drug Interaction and Pharmacist. J. Young Pharm. 2010, 2, 326–331. [Google Scholar] [CrossRef]
- Soraci, L.; Cherubini, A.; Paoletti, L.; Filippelli, G.; Luciani, F.; Laganà, P.; Gambuzza, M.E.; Filicetti, E.; Corsonello, A.; Lattanzio, F. Safety and Tolerability of Antimicrobial Agents in the Older Patient. Drugs Aging 2023, 40, 499–526. [Google Scholar] [CrossRef]
- Giarratano, A.; Green, S.E.; Nicolau, D.P. Review of Antimicrobial Use and Considerations in the Elderly Population. Clin. Interv. Aging 2018, 13, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Kurczewska-Michalak, M.; Lewek, P.; Jankowska-Polańska, B.; Giardini, A.; Granata, N.; Maffoni, M.; Costa, E.; Midão, L.; Kardas, P. Polypharmacy Management in the Older Adults: A Scoping Review of Available Interventions. Front. Pharmacol. 2021, 12, 734045. [Google Scholar] [CrossRef] [PubMed]
- Scondotto, G.; Pojero, F.; Pollina Addario, S.; Ferrante, M.; Pastorello, M.; Visconti, M.; Scondotto, S.; Casuccio, A. The Impact of Polypharmacy and Drug Interactions among the Elderly Population in Western Sicily, Italy. Aging Clin. Exp. Res. 2018, 30, 81–87. [Google Scholar] [CrossRef]
- Błeszyńska, E.; Wierucki, Ł.; Zdrojewski, T.; Renke, M. Pharmacological Interactions in the Elderly. Medicina 2020, 56, 320. [Google Scholar] [CrossRef]
- Levison, M.E.; Levison, J.H. Pharmacokinetics and Pharmacodynamics of Antibacterial Agents. Infect. Dis. Clin. N. Am. 2009, 23, 791–815. [Google Scholar] [CrossRef]
- Epps, P.V.; Canaday, D.H. (Eds.) Infections in Older Adults, An Issue of Infectious Disease Clinics of North America, 1st ed.; Elsevier: Amsterdam, The Netherlands, 2023; ISBN 9780443182242. [Google Scholar]
- Faulkner, C.M.; Cox, H.L.; Williamson, J.C. Unique Aspects of Antimicrobial Use in Older Adults. Clin. Infect. Dis. 2005, 40, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, C.M.; Kim, M.C.; Winston, J.A. Therapy Insight: How Changes in Renal Function with Increasing Age Affect Cardiovascular Drug Prescribing. Nat. Clin. Pract. Cardiovasc. Med. 2006, 3, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Thürmann, P.A. Pharmacodynamics and Pharmacokinetics in Older Adults. Curr. Opin. Anaesthesiol. 2020, 33, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Polaka, S.; Tella, J.D.; Tekade, M.; Sharma, M.C.; Tekade, R.K. Impact of Ageing on the Pharmacokinetics and Pharmacodynamics of the Drugs. In Pharmacokinetcs and Toxicokinetic Consideration. Advances in Pharmaceutical Product Development and Research; Tekade, R.K., Ed.; Academic Press: Cambridge, MA, USA, 2022; Volume 2, pp. 241–261. ISBN 978-0-323-98367-9. [Google Scholar]
- Bowie, M.W.; Slattum, P.W. Pharmacodynamics in Older Adults: A Review. Am. J. Geriatr. Pharmacother. 2007, 5, 263–303. [Google Scholar] [CrossRef]
- Noreddin, A.M.; El-Khatib, W.; Haynes, V. Optimal Dosing Design for Antibiotic Therapy in the Elderly: A Pharmacokinetic and Pharmacodynamic Perspective. Recent Pat. Antiinfect. Drug Discov. 2008, 3, 45–52. [Google Scholar] [CrossRef]
- Wilson, R.C.; Arkell, P.; Riezk, A.; Gilchrist, M.; Wheeler, G.; Hope, W.; Holmes, A.H.; Rawson, T.M. Addition of Probenecid to Oral β-Lactam Antibiotics: A Systematic Review and Meta-Analysis. J. Antimicrob. Chemother. 2022, 77, 2364–2372. [Google Scholar] [CrossRef] [PubMed]
- Moj, D.; Hanke, N.; Britz, H.; Frechen, S.; Kanacher, T.; Wendl, T.; Haefeli, W.E.; Lehr, T. Clarithromycin, Midazolam, and Digoxin: Application of PBPK Modeling to Gain New Insights into Drug-Drug Interactions and Co-Medication Regimens. AAPS J. 2017, 19, 298–312. [Google Scholar] [CrossRef] [PubMed]
- Fralick, M.; Macdonald, E.M.; Gomes, T.; Antoniou, T.; Hollands, S.; Mamdani, M.M.; Juurlink, D.N. Co-Trimoxazole and Sudden Death in Patients Receiving Inhibitors of Renin-Angiotensin System: Population Based Study. BMJ 2014, 349, g6196. [Google Scholar] [CrossRef]
- Fischer, H.D.; Juurlink, D.N.; Mamdani, M.M.; Kopp, A.; Laupacis, A. Hemorrhage during Warfarin Therapy Associated with Cotrimoxazole and Other Urinary Tract Anti-Infective Agents: A Population-Based Study. Arch. Intern. Med. 2010, 170, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Juurlink, D.N.; Mamdani, M.; Kopp, A.; Laupacis, A.; Redelmeier, D.A. Drug-Drug Interactions among Elderly Patients Hospitalized for Drug Toxicity. JAMA 2003, 289, 1652–1658. [Google Scholar] [CrossRef]
- Paulson, S.K.; Wood-Horrall, R.N.; Hoover, R.; Quintas, M.; Lawrence, L.E.; Cammarata, S.K. The Pharmacokinetics of the CYP3A Substrate Midazolam After Steady-State Dosing of Delafloxacin. Clin. Ther. 2017, 39, 1182–1190. [Google Scholar] [CrossRef]
- Henneman, A.; Thornby, K.-A. Risk of Hypotension with Concomitant Use of Calcium-Channel Blockers and Macrolide Antibiotics. Am. J. Health Pharm. 2012, 69, 1038–1043. [Google Scholar] [CrossRef]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global Increase and Geographic Convergence in Antibiotic Consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef]
- Outpatient Antibiotic Prescriptions—United States. 2022. Available online: https://archive.cdc.gov/www_cdc_gov/antibiotic-use/data/report-2022.html (accessed on 9 August 2024).
- Adriaenssens, N.; Bruyndonckx, R.; Versporten, A.; Hens, N.; Monnet, D.L.; Molenberghs, G.; Goossens, H.; Weist, K.; Coenen, S. Consumption of Quinolones in the Community, European Union/European Economic Area, 1997–2017. J. Antimicrob. Chemother. 2021, 76, ii37–ii44. [Google Scholar] [CrossRef]
- Gupta, N.; Singarapu, S.; Ahmed, M.I.; Pasupuleti, H.; Fatima, S. An Ambispective Observational Study on Antibiotics in Pulmonology Department in a Tertiary Care Hospital. Int. J. Community Med. Public Health 2024, 11, 1608–1611. [Google Scholar] [CrossRef]
- Syed, A.; Mosaddek, M. Prescribing Practice of Antibiotics for Outpatients in Bangladesh: Rationality Analysis. Am. J. Pharmacol. 2018, 1, 1008. [Google Scholar]
- Antimicrobial Consumption in the EU/EEA (ESAC-Net)—Annual Epidemiological Report for 2022. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-consumption-europe-2022 (accessed on 9 August 2024).
- Lv, J.; Liu, G.; Dong, W.; Ju, Y.; Sun, Y. ACDB: An Antibiotic Combination DataBase. Front. Pharmacol. 2022, 13, 869983. [Google Scholar] [CrossRef] [PubMed]
- Xiong, G.; Yang, Z.; Yi, J.; Wang, N.; Wang, L.; Zhu, H.; Wu, C.; Lu, A.; Chen, X.; Liu, S.; et al. DDInter: An Online Drug-Drug Interaction Database towards Improving Clinical Decision-Making and Patient Safety. Nucleic Acids Res. 2022, 50, D1200–D1207. [Google Scholar] [CrossRef] [PubMed]
- Shariff, A.; Belagodu Sridhar, S.; Abdullah Basha, N.F.; Bin Taleth Alshemeil, S.S.H.; Ahmed Aljallaf Alzaabi, N.A. 4th Assessing Consistency of Drug-Drug Interaction-Related Information Across Various Drug Information Resources. Cureus 2021, 13, e13766. [Google Scholar]
- Abbas, K.; Ahmed, M.; Babar, Z.-U.-D. Trends in Prescribing Antibiotics Between 2012 and 2022: High-Income Versus Low-Middle-Income Countries. In Encyclopedia of Evidence in Pharmaceutical Public Health and Health Services Research in Pharmacy; Springer: Cham, Switzerland, 2023; ISBN 978-3-030-50247-8. [Google Scholar]
- Durkin, M.J.; Jafarzadeh, S.R.; Hsueh, K.; Sallah, Y.H.; Munshi, K.D.; Henderson, R.R.; Fraser, V.J. Outpatient Antibiotic Prescription Trends in the United States: A National Cohort Study. Infect. Control Hosp. Epidemiol. 2018, 39, 584–589. [Google Scholar] [CrossRef]
- Drug Interaction Checker in Drugs.Com. Available online: https://www.drugs.com/drug_interactions.html (accessed on 10 August 2024).
- Drug Interaction Checker in Medscape. Available online: https://reference.medscape.com/drug-interactionchecker (accessed on 10 August 2024).
- Drug Interaction Checker in WebMD. Available online: https://www.webmd.com/interaction-checker/default.htm (accessed on 10 August 2024).
- Drug Interaction Checker in DrugBank. Available online: https://go.drugbank.com/drug-interaction-checker (accessed on 10 August 2024).
- Drug Interaction Checker in DDInter. Available online: http://ddinter.scbdd.com/inter-checker/ (accessed on 10 August 2024).
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Mulani, M.S.; Kamble, E.E.; Kumkar, S.N.; Tawre, M.S.; Pardesi, K.R. Emerging Strategies to Combat ESKAPE Pathogens in the Era of Antimicrobial Resistance: A Review. Front. Microbiol. 2019, 10, 539. [Google Scholar] [CrossRef]
- Zaha, D.C.; Bungau, S.; Uivarosan, D.; Tit, D.M.; Maghiar, T.A.; Maghiar, O.; Pantis, C.; Fratila, O.; Rus, M.; Vesa, C.M. Antibiotic Consumption and Microbiological Epidemiology in Surgery Departments: Results from a Single Study Center. Antibiotics 2020, 9, 81. [Google Scholar] [CrossRef]
- Tyers, M.; Wright, G.D. Drug Combinations: A Strategy to Extend the Life of Antibiotics in the 21st Century. Nat. Rev. Microbiol. 2019, 17, 141–155. [Google Scholar] [CrossRef]
- ACDB. A Comprehensive Database of Antibiotic Combinations. Available online: http://www.acdb.plus (accessed on 11 August 2024).
- Noel, D.J.; Keevil, C.W.; Wilks, S.A. Synergism versus Additivity: Defining the Interactions between Common Disinfectants. MBio 2021, 12, e0228121. [Google Scholar] [CrossRef]
- Lagatolla, C.; Milic, J.; Imperi, F.; Cervoni, M.; Bressan, R.; Luzzati, R.; Di Bella, S. Synergistic Activity of Fosfomycin and Chloramphenicol against Vancomycin-Resistant Enterococcus Faecium (VREfm) Isolates from Bloodstream Infections. Diagn. Microbiol. Infect. Dis. 2021, 99, 115241. [Google Scholar] [CrossRef] [PubMed]
- Boudrioua, A.; Li, Y.; Hartke, A.; Giraud, C. Opposite Effect of Vancomycin and D-Cycloserine Combination in Both Vancomycin Resistant Staphylococcus Aureus and Enterococci. FEMS Microbiol. Lett. 2020, 367, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Aktas, G.; Derbentli, S. In Vitro Activity of Daptomycin Combinations with Rifampicin, Gentamicin, Fosfomycin and Fusidic Acid against MRSA Strains. J. Glob. Antimicrob. Resist. 2017, 10, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Kussmann, M.; Obermueller, M.; Karer, M.; Kriz, R.; Chen, R.-Y.; Hohl, L.; Schneider, L.; Burgmann, H.; Traby, L.; Vossen, M.G. Synergistic Effect of Cefazolin Plus Fosfomycin Against Staphylococcus Aureus in Vitro and in Vivo in an Experimental Galleria Mellonella Model. Front. Pharmacol. 2021, 12, 685807. [Google Scholar] [CrossRef]
- Huang, L.; Wang, M.; Sun, L. Synergy Testing by E-Test and Microdilution Checkerboard for Fosfomycin Combined with Tigecycline against KPC-Producing Klebsiella Pneumoniae. Clin. Lab. 2019, 65, 1. [Google Scholar] [CrossRef]
- Patil, S.V.; Hajare, A.L.; Patankar, M.; Krishnaprasad, K. In Vitro Fractional Inhibitory Concentration (FIC) Study of Cefixime and Azithromycin Fixed Dose Combination (FDC) Against Respiratory Clinical Isolates. J. Clin. Diagn. Res. 2015, 9, DC13–DC15. [Google Scholar] [CrossRef]
- Maryam, L.; Khalid, S.; Ali, A.; Khan, A.U. Synergistic Effect of Doripenem in Combination with Cefoxitin and Tetracycline in Inhibiting NDM-1 Producing Bacteria. Future Microbiol. 2019, 14, 671–689. [Google Scholar] [CrossRef]
- Gunalan, A.; Sarumathi, D.; Sastry, A.S.; Ramanathan, V.; Rajaa, S.; Sistla, S. Effect of Combined Colistin and Meropenem against Meropenem Resistant Acinetobacter Baumannii and Pseudomonas Aeruginosa by Checkerboard Method: A Cross Sectional Analytical Study. Indian J. Pharmacol. 2021, 53, 207–212. [Google Scholar]
- Lin, F.; Yu, B.; Wang, Q.; Yuan, M.; Ling, B. Combination Inhibition Activity of Chlorhexidine and Antibiotics on Multidrug-Resistant Acinetobacter Baumannii in Vitro. BMC Infect. Dis. 2021, 21, 266. [Google Scholar] [CrossRef]
- Yang, H.; Lv, N.; Hu, L.; Liu, Y.; Cheng, J.; Ye, Y.; Li, J. In Vivo Activity of Vancomycin Combined with Colistin against Multidrug-Resistant Strains of Acinetobacter Baumannii in a Galleria Mellonella Model. Infect. Dis. 2016, 48, 189–194. [Google Scholar] [CrossRef]
- Ozbek, B.; Otuk, G. Post-Antibiotic Effect of Levofloxacin and Tobramycin Alone or in Combination with Cefepime against Pseudomonas Aeruginosa. Chemotherapy 2009, 55, 446–450. [Google Scholar] [CrossRef] [PubMed]
- Brochado, A.R.; Telzerow, A.; Bobonis, J.; Banzhaf, M.; Mateus, A.; Selkrig, J.; Huth, E.; Bassler, S.; Zamarreño Beas, J.; Zietek, M.; et al. Species-Specific Activity of Antibacterial Drug Combinations. Nature 2018, 559, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Maryam, L.; Khan, A.U. Combination of Aztreonam and Cefotaxime against CTX-M-15 Type β-Lactamases: A Mechanism Based Effective Therapeutic Approach. Int. J. Biol. Macromol. 2018, 116, 1186–1195. [Google Scholar] [CrossRef] [PubMed]
- Hagiya, H.; Aoki, K.; Akeda, Y.; Yamamoto, N.; Shanmugakani, R.K.; Ishii, Y.; Tomono, K. In Vitro Effectiveness of Meropenem and Cefmetazole Combination Treatment Against KPC-2-Producing Enterobacteriaceae. Microb. Drug Resist. 2019, 25, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Tohamy, S.T.; Aboshanab, K.M.; El-Mahallawy, H.A.; El-Ansary, M.R.; Afifi, S.S. Prevalence of Multidrug-Resistant Gram-Negative Pathogens Isolated from Febrile Neutropenic Cancer Patients with Bloodstream Infections in Egypt and New Synergistic Antibiotic Combinations. Infect. Drug Resist. 2018, 11, 791–803. [Google Scholar] [CrossRef]
- Subramanian, A. Emerging Roles of Bacteriophage-Based Therapeutics in Combating Antibiotic Resistance. Front. Microbiol. 2024, 15, 1384164. [Google Scholar] [CrossRef]
- Tiwari, P.; Srivastava, Y.; Sharma, A.; Vinayagam, R. Antimicrobial Peptides: The Production of Novel Peptide-Based Therapeutics in Plant Systems. Life 2023, 13, 1875. [Google Scholar] [CrossRef]
- Zou, W.; McAdorey, A.; Yan, H.; Chen, W. Nanomedicine to Overcome Antimicrobial Resistance: Challenges and Prospects. Nanomedicine 2023, 18, 471–484. [Google Scholar] [CrossRef]
- Mayorga-Ramos, A.; Zúñiga-Miranda, J.; Carrera-Pacheco, S.E.; Barba-Ostria, C.; Guamán, L.P. CRISPR-Cas-Based Antimicrobials: Design, Challenges, and Bacterial Mechanisms of Resistance. ACS Infect. Dis. 2023, 9, 1283–1302. [Google Scholar] [CrossRef]
- Zhu, M.; Tse, M.W.; Weller, J.; Chen, J.; Blainey, P.C. The Future of Antibiotics Begins with Discovering New Combinations. Ann. N. Y. Acad. Sci. 2021, 1496, 82–96. [Google Scholar] [CrossRef]
- Butler, M.S.; Henderson, I.R.; Capon, R.J.; Blaskovich, M.A.T. Antibiotics in the Clinical Pipeline as of December 2022. J. Antibiot. 2023, 76, 431–473. [Google Scholar] [CrossRef] [PubMed]
- Ru, X.; Ye, X.; Sakurai, T.; Zou, Q.; Xu, L.; Lin, C. Current Status and Future Prospects of Drug-Target Interaction Prediction. Brief. Funct. Genom. 2021, 20, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xiong, Z.; Zhang, W.; Liu, S. Deep Learning for Drug-Drug Interaction Prediction: A Comprehensive Review. Quant. Biol. 2024, 12, 30–52. [Google Scholar] [CrossRef]
- ClinicalTrials.Gov. National Library of Medicine. Available online: https://clinicaltrials.gov/ (accessed on 11 August 2024).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Perpetrator Drug (Class) | Victim Drug | Effect and Mechanisms | Clinical Implications/ Recommendations | Ref. |
|---|---|---|---|---|
| Ciprofloxacin (quinolones) | Theophylline | effects of theophylline are increased by ciprofloxacin through the inhibition of CYP2D6-mediated metabolism of theophylline | ciprofloxacin-induced theophylline toxicity/decrease dosage and closely observe for signs of theophylline toxicity | [59,63] |
| Erythromycin | additive effect with a prolongation of the QT interval | risk for torsades de pointes/avoid combination | [59,64] | |
| Voriconazole | ||||
| Formoterol | ||||
| Methadone | effects of methadone are increased by ciprofloxacin through the inhibition of CYP1A2-, CYP3A4-, CYP2D6-mediated metabolism of methadone | possible increased opioid effects/avoid opioid premedication when antibiotics are used for prophylaxis | [65] | |
| Levofloxacin (quinolones) | Ciclosporin | increased concentrations of ciclosporin through the inhibition of CYP3A4-mediated metabolism of ciclosporin | risk for renal toxicity and neurotoxicity/monitor the function of the kidneys and the plasma concentrations | [66] |
| Insulin | modified insulin needs | hypoglycemia or hyperglycemia/frequent monitoring of blood sugar levels | [67] | |
| Warfarin | increased concentrations of warfarin through the inhibition of CYP2C9-mediated metabolism of warfarin | possible increases of the INR values/INR monitoring | [68] | |
| Neomycin (aminoglycosides) | Methotrexate | decreases the gastrointestinal absorption of oral methotrexate by half | lack of effect/2-4 h interval between administration | [64] |
| Digoxin | decreases the gastrointestinal absorption of digoxin | lack of effect/2-4 h interval between administration | [69] | |
| Meropenem Ertapenem Imipenem Doripenem (carbapenems, β-lactam) | Valproic acid | decreases in the concentration of valproic acid through the inhibition of valproate glucuronide hydrolysis, induction of valproate hepatic glucuronidation, and increases of the renal clearance of valproate glucuronide | lack of effect/valproic acid levels monitoring | [70,71] |
| Clarithromycin (macrolides) | Colchicine | increased concentrations of colchicine through the inhibition of P-glycoprotein and CYP3A4-mediated metabolism of colchicine | colchicine toxicity through gastrointestinal symptoms, multiple organ failure, and blood dyscrasias/use of another antibiotic | [72] |
| Venlafaxine | additive effect with a prolongation of the QT interval | risk for torsades de pointes/avoid combination | [64] | |
| Terfenadine | ||||
| Propafenone | ||||
| Telithromycin (macrolides) | Sotalol | additive effect with a prolongation of the QT interval | risk for torsades de pointes/avoid combination | [73] |
| Voriconazole | increased concentrations of voriconazole through the inhibition of CYP3A4-mediated metabolism of voriconazole | risk for toxic effects/monitor liver functionality | [64] | |
| Midazolam | increased concentrations of midazolam through the inhibition of CYP3A4-mediated metabolism of midazolam | risk for toxic effects/reduce the dose of midazolam by half | [74] | |
| Piperacillin (penicillins, β-lactam) | Depolarizing and non-depolarizing muscle relaxants | enhanced the effect of muscle relaxants through a neuromuscular blocking activity | risk for toxic effects/monitor the neuromuscular blockade | [64] |
| Rifampicin (rifamycins) | Amiodarone | decreased concentrations of amiodarone through the induction of CYP3A4-mediated metabolism of amiodarone | ineffective reaction to amiodarone/monitor the possible poor response, dose adjustments | [75] |
| Paracetamol | decreased paracetamol concentration through the increase of paracetamol glucuronidation | lack of effect/use an alternative analgesic | [64] | |
| Cabazitaxel | competitive antagonism for UGT | lack of effect/avoid combination | [76,77] | |
| Co-trimoxazole * (sulphonamides) | Sacubitril/Valsartan | additive effect on renal potassium regulation reducing aldosterone levels and potassium excretion | hyperkalemia/avoid combination | [78] |
| Warfarin | increased concentrations of warfarin through the inhibition of CYP-mediated metabolism of warfarin | increased risk of bleeding/avoid combination | [79] | |
| Vancomycin (glycopeptide) | Depolarizing and non-depolarizing muscle relaxants | enhanced the effect of muscle relaxants through a neuromuscular blocking activity | risk for toxic effects/monitor the neuromuscular blockade | [64] |
| Tetracycline (tetracyclines) | Methotrexate | increased concentration of methotrexate due to the disruption of the bacterial colonies involved in the metabolism of methotrexate | risk for toxic effects exerted by methotrexate/avoid combination | [80] |
| Chloramphenicol | Sulfonylureas as antidiabetic agents | increased concentrations of sulphonylureas through the inhibition of CYP2C9-mediated metabolism of sulphonylureas | elevated risk of hypoglycemia/monitor the blood sugar level | [81] |
| Vitamin B12 | decrease in the efficacy of vitamin B12 due to the inhibition of the bone marrow | risks related to the inhibition of bone marrow function/monitor the levels of vitamin B12 and the full blood count | [64] | |
| Quinupristin/dalfopristin (streptogramins) | Atomoxetine | additive effect with a prolongation of the QT interval | risk for torsades de pointes/avoid combination | [64] |
| Sotalol | ||||
| Disopyramide | ||||
| Amoxicillin (aminopenicillin, β-lactam) | Warfarin | probably through the reduction of intestinal bacteria that produce vitamin K, leading to a shortage of vitamin K | possible increases of the INR values/INR monitoring | [73] |
| Acenocumarol | ||||
| Linezolid | Fentanyl | uncertain, possibly due to the competitive inhibition of monoamine oxidase-A | risk for serotonin syndrome/avoid combination | [82] |
| Antibiotic | Drugs and Vaccines with Major Interaction Potential in Combination with the Antibiotic |
|---|---|
| Ciprofloxacin | Acalabrutinib, acetohexamide, adagrasib, aminolevulinic acid, aminophylline, amiodarone, amisulpride, anagrelide, anisindione, arsenic trioxide, avanafil, avapritinib, BCG vaccine, bedaquiline, bempedoic acid, bepridil, betamethasone, bosutinib, brexpiprazole, brigatinib, bromocriptine, bupropion, butorphanol, cabozantinib, capivasertib, ceritinib, chloroquine, chlorpropamide, cholera vaccine (live), cisapride, citalopram, clozapine, cobimetinib, colchicine, cortisone, crizotinib, deflazacort, dexamethasone, dicumarol, disopyramide, dofetilide, dolasetron, dronedarone, droperidol, duloxetine, efavirenz, elacestrant, eliglustat, entrectinib, eplerenone, escitalopram, etrasimod, fecal microbiota spores (live), fenfluramine, fexinidazole, fezolinetant, finerenone, fingolimod, flibanserin, fludrocortisone, gepirone, glimepiride, glipizide, glyburide, guanfacine, halofantrine, haloperidol, hydrocodone, hydrocortisone, hydroxychloroquine, ibrutinib, ibutilide, iloperidone, infigratinib, insulin, insulin aspart, insulin aspart protamine, insulin degludec, insulin detemir, insulin glargine, insulin glulisine, insulin inhalation (rapid-acting), insulin isophane, insulin lispro, insulin lispro protamine, insulin regular, insulin zinc, insulin zinc extended, iohexol, iomeprol, iopamidol, ivabradine, ivosidenib, lefamulin, lemborexant, levoketoconazole, levomethadylacetate, lomitapide, lonafarnib, lumateperone, lurbinectedin, mavacamten, mavorixafor, mesoridazine, methadone, methylprednisolone, metrizamide, mifepristone, mobocertinib, mycophenolate mofetil, mycophenolic acid, naloxegol, nateglinide, neratinib, nilotinib, nirogacestat, olanzapine, olaparib, oliceridine, oxtriphylline, oxycodone, ozanimod, pacritinib, palovarotene, panobinostat, papaverine, pasireotide, pemigatinib, pexidartinib, pimozide, pirfenidone, ponesimod, prednisolone, prednisone, procainamide, quinidine, quizartinib, rasagiline, repaglinide, repotrectinib, ribociclib, saquinavir, selpercatinib, selumetinib, siponimod, sirolimus protein-bound, sonidegib, sotalol, suvorexant, tasimelteon, tazemetostat, theophylline, thioridazine, tizanidine, tolazamide, tolbutamide, toremifene, tramadol, triamcinolone, typhoid vaccine (live), vamorolone, vandetanib, vemurafenib, venetoclax, voclosporin, warfarin, zanubrutinib, ziprasidone, zolpidem |
| Trimethoprim | Amiloride, azilsartan medoxomil, BCG vaccine, benazepril, candesartan, captopril, cholera vaccine (live), dofetilide, enalapril, enalaprilat, eplerenone, eprosartan, fecal microbiota spores (live), finerenone, fosinopril, fosphenytoin, irbesartan, leucovorin, levoleucovorin, lisinopril, losartan, lvp solution with potassium, methotrexate, moexipril, olmesartan, parenteral nutrition solution w/electrolytes, perindopril, phenytoin, potassium acetate, potassium acid phosphate, potassium bicarbonate, potassium chloride, potassium citrate, potassium gluconate, potassium iodide, potassium perchlorate, potassium phosphate, prilocaine, procaine penicillin, quinapril, ramipril, spironolactone, telmisartan, trandolapril, triamterene, typhoid vaccine (live), valsartan |
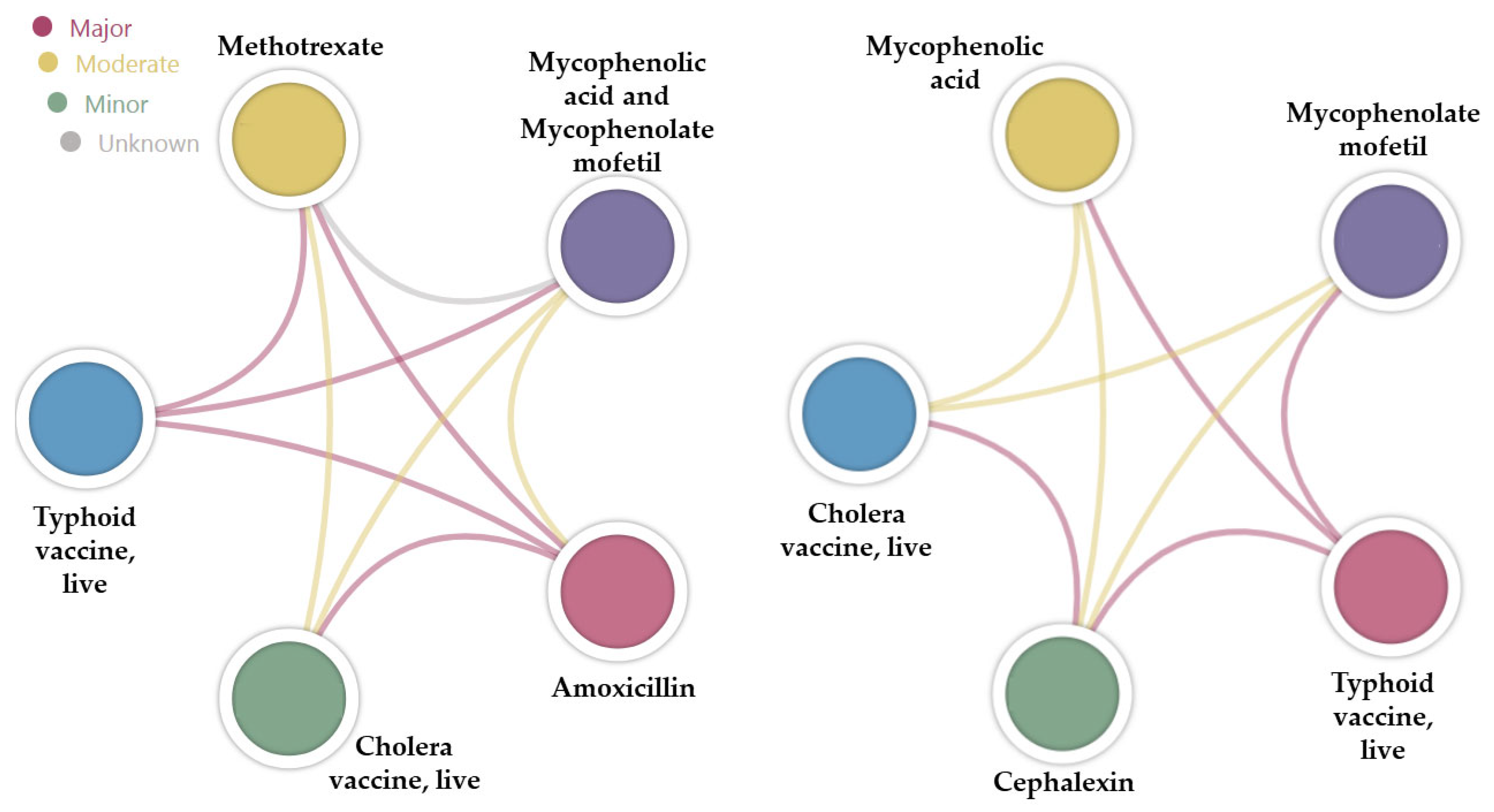
| Amoxicillin | BCG vaccine, cholera vaccine (live), fecal microbiota spores (live), methotrexate, mycophenolate mofetil, mycophenolic acid, typhoid vaccine (live) |
| Cephalexin | BCG vaccine, cholera vaccine (live), fecal microbiota spores (live), mycophenolate mofetil, mycophenolic acid, typhoid vaccine (live) |
| Azithromycin | Adagrasib, amiodarone, amisulpride, anagrelide, arsenic trioxide, BCG vaccine, bedaquiline, bepridil, berotralstat, betrixaban, cabozantinib, ceritinib, chloroquine, cholera vaccine (live), cisapride, citalopram, clozapine, colchicine, crizotinib, disopyramide, dofetilide, dolasetron, dronedarone, droperidol, edoxaban, efavirenz, escitalopram, etrasimod, fecal microbiota spores (live), fexinidazole, fingolimod, gatifloxacin, grepafloxacin, halofantrine, haloperidol, hydroxychloroquine, ibutilide, iloperidone, ivabradine, ivosidenib, lefamulin, leflunomide, levoketoconazole, levomethadyl acetate, lomitapide, mavorixafor, mesoridazine, methadone, mifepristone, mipomersen, mobocertinib, morphine, moxifloxacin, mycophenolate mofetil, mycophenolic acid, nilotinib, osimertinib, ozanimod, pacritinib, panobinostat, papaverine, pasireotide, pazopanib, pexidartinib, pimozide, ponesimod, procainamide, quinidine, quizartinib, relugolix, ribociclib, saquinavir, selpercatinib, siponimod, sotalol, sparfloxacin, teriflunomide, thioridazine, toremifene, typhoid vaccine (live), vandetanib, vemurafenib, ziprasidone |
| Antibiotic | Drug Pair | Results Displayed |
|---|---|---|
| Ciprofloxacin * | Acetohexamide, anisindione, bepridil, dicumarol, halofantrine, infigratinib, insulin, insulin lispro protamine, insulin zinc, insulin zinc extended, iohexol, iomeprol, iopamidol, levoketoconazole, levomethadyl acetate, mesoridazine, mycophenolate mofetil, mycophenolic acid, oxtriphylline, panobinostat | No results |
| Acalabrutinib, adagrasib, avanafil, bempedoic acid, betamethasone, brexpiprazole, brigatinib, bromocriptine, bupropion, butorphanol, cabozantinib, capivasertib, cisapride, deflazacort, elacestrant, eplerenone, fenfluramine, guanfacine, hydrocodone, hydrocortisone, insulin inhalation, insulin aspart protamine, insulin degludec, insulin detemir, insulin glargine, insulin glulisine, insulin isophane, ivabradine, lefamulin, lumateperone, lurbinectedin, mavacamten, metrizamide, naloxegol, neratinib, nirogacestat, oliceridine, oxycodone, pacritinib, palovarotene, papaverine, pemigatinib, pexidartinib, ponesimod, repotrectinib, selumetinib, sirolimus protein-bound, sonidegib, suvorexant, tasimelteon, tazemetostat, tramadol, triamcinolone, vamorolone, zanubrutinib | No Interactions Found | |
| Amiodarone, arsenic trioxide, avapritinib, bedaquiline, bosutinib, chloroquine, chlorpropamide, citalopram, colchicine, cortisone, crizotinib, dexamethasone, disopyramide, dolasetron, droperidol, duloxetine, efavirenz, escitalopram, etrasimod, finerenone, fingolimod, fludrocortisone, gepirone, glimepiride, glipizide, glyburide, haloperidol, ibutilide, iloperidone, insulin aspart, insulin lispro, insulin regular, lemborexant, lomitapide, mavorixafor, methadone, methylprednisolone, mifepristone, nateglinide, nilotinib, ozanimod, pasireotide, pimozide, prednisolone, prednisone, procainamide, quinidine, quizartinib, repaglinide, selpercatinib, sotalol, thioridazine, tolazamide, tolbutamide, voclosporin, warfarin, ziprasidone, zolpidem | Monitor closely (moderate) | |
| Azithromycin ** | Bepridil, grepafloxacin, halofantrine, levomethadyl acetate, mesoridazine, mycophenolate mofetil, mycophenolic acid, sparfloxacin | No results |
| Cabozantinib, etrasimod, gatifloxacin, ivabradine, ivosidenib, leflunomide, lomitapide, mipomersen, morphine, pacritinib, papaverine, pexidartinib, ponesimod, relugolix, teriflunomide | No Interactions Found | |
| Amiodarone, bedaquiline, berotralstat, betrixaban, chloroquine, citalopram, crizotinib, disopyramide, droperidol, edoxaban, haloperidol, ibutilide, levoketoconazole, mavorixafor, mifepristone, moxifloxacin, nilotinib, osimertinib, ozanimod, pasireotide, procainamide, quinidine, quizartinib, selpercatinib, sotalol, thioridazine, ziprasidone | Monitor closely (moderate) | |
| Dolasetron, iloperidone, methadone, pazopanib | Minor | |
| Trimethoprim *** | LVP solution with potassium, parenteral nutrition solution w/electrolytes, potassium perchlorate | No results |
| BCG vaccine, cholera vaccine, fecal microbiota spores, leucovorin, levoleucovorin, prilocaine, typhoid vaccine | No Interactions Found | |
| Azilsartan medoxomil, candesartan, eprosartan, finerenone, fosinopril, fosphenytoin, irbesartan, losartan, olmesartan, phenytoin, potassium acetate, potassium acid phosphate, potassium bicarbonate, potassium chloride, potassium citrate, potassium gluconate, potassium iodide, potassium phosphate, spironolactone, telmisartan, valsartan | Monitor closely (moderate) | |
| Amiloride, benazepril, captopril, enalapril, enalaprilat, eplerenone, lisinopril, moexipril, perindopril, procaine penicillin, quinapril, ramipril, trandolapril, triamterene | Minor |
| Database ID | Official Title | Description | Condition | Recruitment Status |
|---|---|---|---|---|
| NCT04840862 | Impact of Rifabutin on the Pharmacokinetics of Elexacaftor/Tezacaftor/Ivacaftor | A single-center, prospective, nonrandomized, open-label study was conducted in healthy adults to assess how Trikafta’s pharmacokinetics are affected by rifabutin | Drug-Drug Interaction | Completed |
| NCT04671589 | Antidote for Valproic Acid Toxicity: a New Indication for Meropenem Antibiotic. A Randomized Placebo-controlled Trial | Evaluation of an antidote for VPA by leveraging the well-documented drug-drug interaction between VPA and carbapenems, which significantly reduces VPA serum levels during concurrent administration | Drug toxicity | Unknown |
| NCT04140903 | Partial Oral Antibiotic Treatment for Bacterial Brain Abscess: An Open-label Randomized Non-inferiority Trial | Assessment of the clinical viability of oral antibiotics for the treatment of brain abscess | Brain abscess | Recruiting |
| NCT04551573 | A Study of the Pharmacokinetic and Pharmacodynamic Interactions Between Bictegravir, Tenofovir Alafenamide and Rifapentine in Healthy Adult Subjects | A single-center, open-label investigation that examines the pharmacokinetic interaction between bictegravir and tenofovir alafenamide when administered with rifapentine | Tuberculosis | Withdrawn |
| NCT05588492 | The Safety, Completion Rate and Prevention Effect by Rifamycin-containing Regimens for Latent Tuberculosis Infection in Patients With Kidney Transplantation: a Prospective Intervention Pilot Study | Evaluation of the co-administration of rifamycin and immunosuppressants in kidney transplant recipients | Pulmonology | Recruiting |
| NCT05046132 | A Randomized, Double-Blind, 3-arm, Parallel Group, Placebo- and Positive-controlled Study to Investigate the Effects of Setmelanotide on QTc Interval in Healthy Subjects | An assessment of the effects of various concentrations of setmelanotide on the QT interval in a study that employed a double-blind, randomized design with positive and placebo controls | Healthy | Completed with results |
| NCT06178627 | A Multi-center, Prospective, Randomized Trial of Amphotericin B in the Initial Antifungal Therapy for Non-HIV Cryptococcal Meningitis Patients | Comparative assessments to evaluate the safety and effectiveness of standard-dose amphotericin B (0.7 mg/kg/day) versus a lower dose (0.5 mg/kg/day) in the initial antifungal therapy for non-HIV patients with cryptococcal meningitis, since Asian patients may exhibit variations in drug metabolism and pharmacokinetics | Contraception Behavior | Enrolling by invitation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radu, A.-F.; Bungau, S.G.; Corb Aron, R.A.; Tarce, A.G.; Bodog, R.; Bodog, T.M.; Radu, A. Deciphering the Intricate Interplay in the Framework of Antibiotic-Drug Interactions: A Narrative Review. Antibiotics 2024, 13, 938. https://doi.org/10.3390/antibiotics13100938
Radu A-F, Bungau SG, Corb Aron RA, Tarce AG, Bodog R, Bodog TM, Radu A. Deciphering the Intricate Interplay in the Framework of Antibiotic-Drug Interactions: A Narrative Review. Antibiotics. 2024; 13(10):938. https://doi.org/10.3390/antibiotics13100938
Chicago/Turabian StyleRadu, Andrei-Flavius, Simona Gabriela Bungau, Raluca Anca Corb Aron, Alexandra Georgiana Tarce, Ruxandra Bodog, Teodora Maria Bodog, and Ada Radu. 2024. "Deciphering the Intricate Interplay in the Framework of Antibiotic-Drug Interactions: A Narrative Review" Antibiotics 13, no. 10: 938. https://doi.org/10.3390/antibiotics13100938
APA StyleRadu, A.-F., Bungau, S. G., Corb Aron, R. A., Tarce, A. G., Bodog, R., Bodog, T. M., & Radu, A. (2024). Deciphering the Intricate Interplay in the Framework of Antibiotic-Drug Interactions: A Narrative Review. Antibiotics, 13(10), 938. https://doi.org/10.3390/antibiotics13100938