
Improving Clostridioides difficile Infectious Disease Treatment Response via Adherence to Clinical Practice Guidelines

 ,
,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
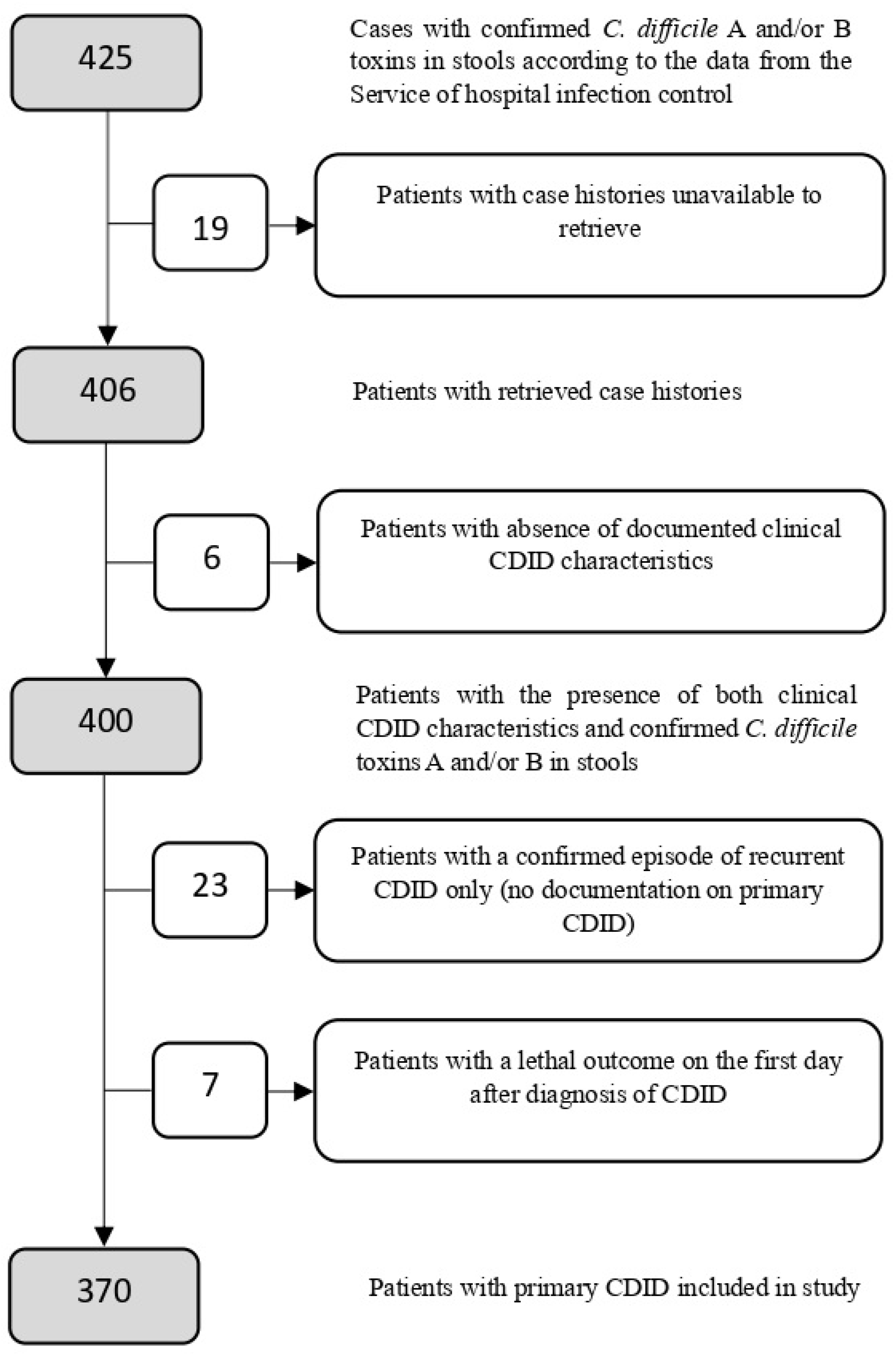
3. Results
3.1. General Characteristics
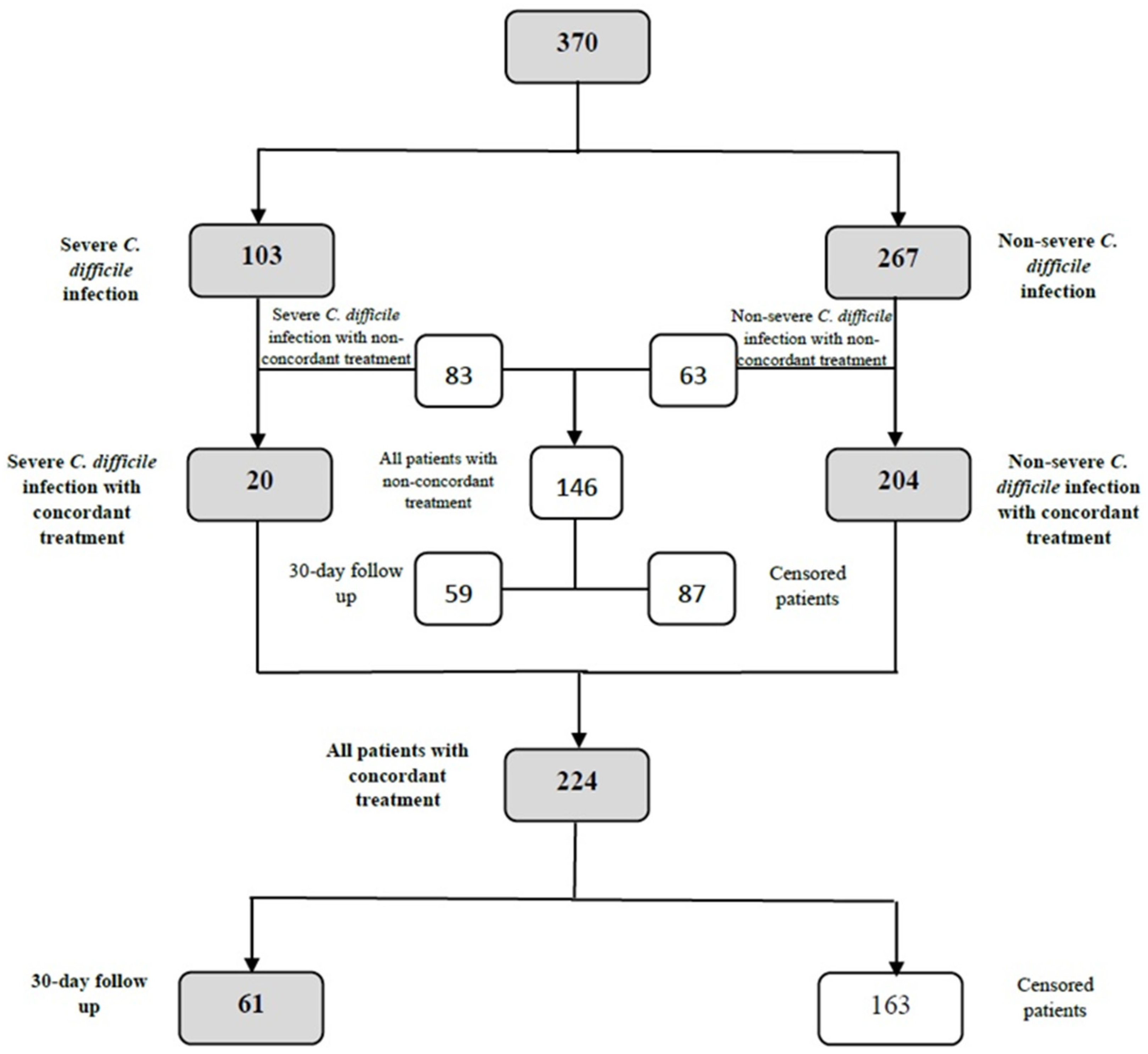
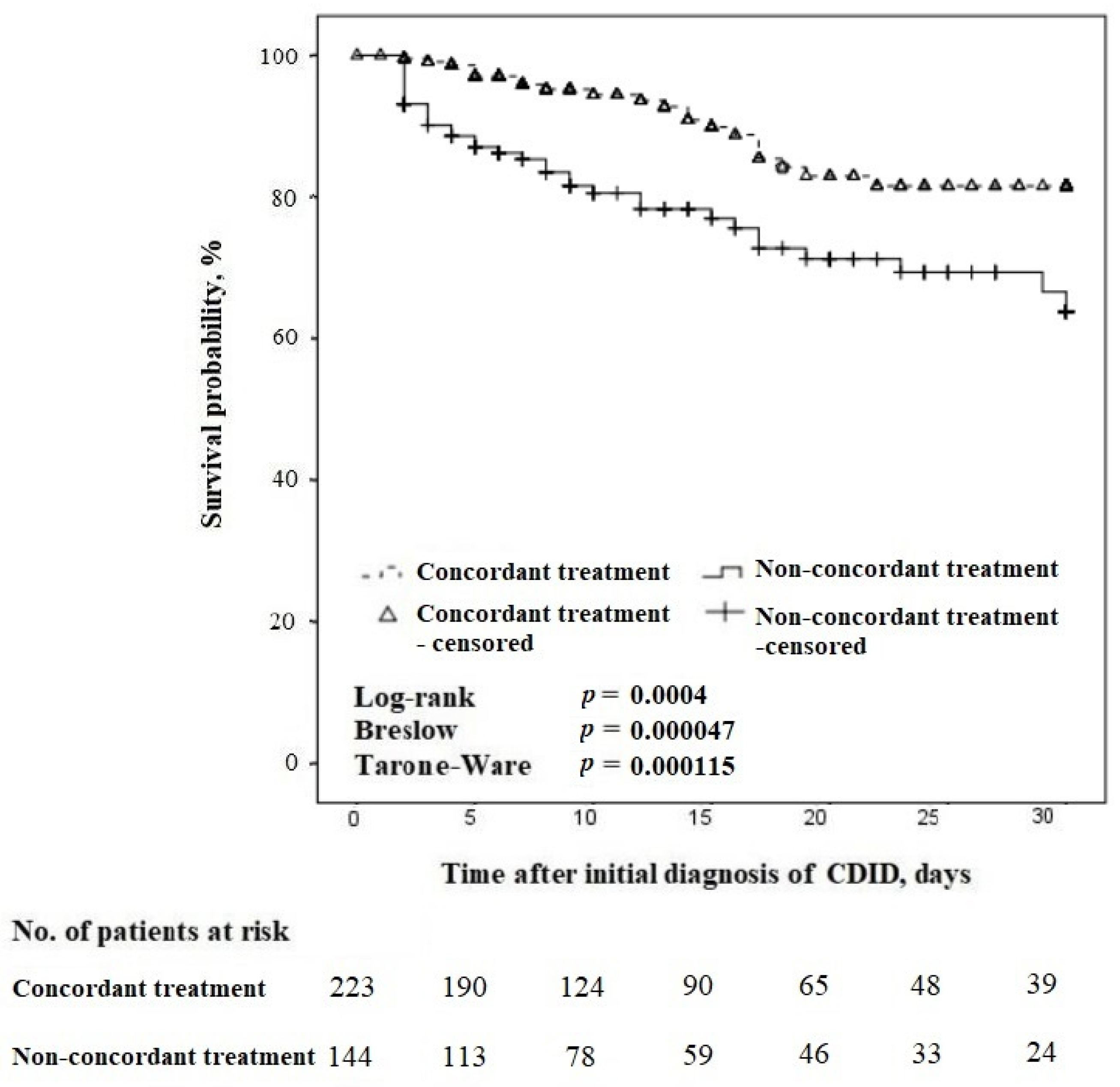
3.2. All Cases of CDID
3.3. Cases of Non-Severe CDID
3.4. Cases of Severe CDID
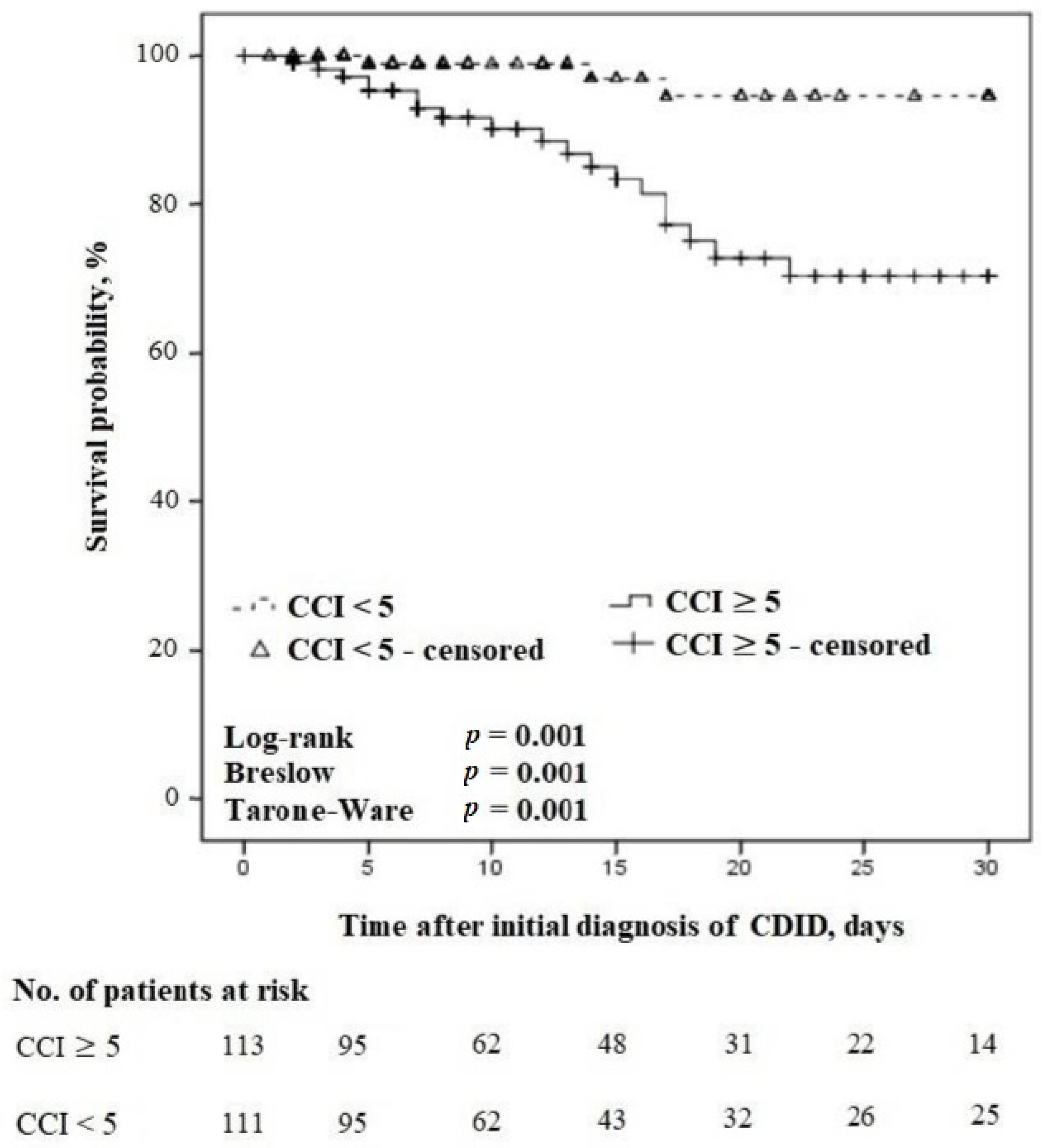
3.5. All CDID Cases with Concordant Treatment
3.6. CDID Cases before (Group 1) and after (Group 2) Integrating the 2017 Guidelines
4. Discussion
Study Novelties and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aktories, K.; Schwan, C.; Jank, T. Clostridium difficile Toxin Biology. Annu. Rev. Microbiol. 2017, 71, 281–307. [Google Scholar] [CrossRef] [PubMed]
- Jeffrey, M.; Denny, K.J.; Lipman, J.; Conway Morris, A. Differentiating infection, colonisation, and sterile inflammation in critical illness: The emerging role of host-response profiling. Intensive Care Med. 2023, 49, 760–771. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Flaster, N.; Casanello, A.L.; Curcio, D. Assessing risk factors, mortality, and healthcare utilization associated with Clostridioides difficile infection in four Latin American countries. Braz. J. Infect. Dis. 2021, 25, 101040. [Google Scholar] [CrossRef] [PubMed]
- Thibault, A.; Miller, M.A.; Gaese, C. Risk Factors for the Development of Clostridium difficile-Associated Diarrhea During a Hospital Outbreak. Infect. Control Hosp. Epidemiol. 1991, 12, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Kelly, C.P.; LaMont, J.T. Clostridium difficile—More Difficult Than Ever. N. Engl. J. Med. 2008, 359, 1932–1940. [Google Scholar] [CrossRef] [PubMed]
- Boland, E.; Thompson, J.S. Fulminant Clostridium difficile Enteritis after Proctocolectomy and Ileal Pouch-Anal Anastamosis. Gastroenterol. Res. Pract. 2008, 2008, 985658. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, L.E.; Yang, S.S.; Bank, S. Clostridium difficile-associated Small Bowel Enteritis After Total Proctocolectomy in a Crohn’s Disease Patient. J. Clin. Gastroenterol. 2010, 44, 76–77. [Google Scholar] [CrossRef]
- Abid, H.; Bischof, E. An Unusual Presentation of Severe Sepsis Due to Clostridium difficile Enteritis. Cureus 2019, 11, e4162. [Google Scholar] [CrossRef]
- Nunes, B.P.; Soares, M.U.; Wachs, L.S.; Volz, P.M.; de Oliveira Saes, M.; Duro, S.M.S.; Thumé, E.; Facchini, L.A. Hospitalization in older adults: Association with multimorbidity, primary health care and private health plan. Rev. Saude Publica 2017, 51, 43. [Google Scholar] [CrossRef]
- Karanika, S.; Paudel, S.; Zervou, F.N.; Grigoras, C.; Zacharioudakis, I.M.; Mylonakis, E. Prevalence and Clinical Outcomes of Clostridium difficile Infection in the Intensive Care Unit: A Systematic Review and Meta-Analysis. Open Forum Infect. Dis. 2015, 3, 186. [Google Scholar] [CrossRef]
- Lofgren, E.T.; Cole, S.R.; Weber, D.J.; Anderson, D.J.; Moehring, R.W. Hospital-Acquired Clostridium difficile Infections. Epidemiology 2014, 25, 570–575. [Google Scholar] [CrossRef]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. 2018, 66, e1–e48. [Google Scholar] [CrossRef] [PubMed]
- Herpers, B.L.; Vlaminckx, B.; Burkhardt, O.; Blom, H.; Biemond-Moeniralam, H.S.; Hornef, M.; Welte, T.; Kuijper, E.J. Intravenous Tigecycline as Adjunctive or Alternative Therapy for Severe Refractory Clostridium difficile Infection. Clin. Infect. Dis. 2009, 48, 1732–1735. [Google Scholar] [CrossRef]
- Garey, K.W.; Sethi, S.; Yadav, Y.; DuPont, H.L. Meta-analysis to assess risk factors for recurrent Clostridium difficile infection. J. Hosp. Infect. 2008, 70, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.; Pasupuleti, V.; Thota, P.; Pant, C.; Rolston, D.D.K.; Hernandez, A.V.; Donskey, C.J.; Fraser, T.G. Risk Factors for Recurrent Clostridium difficile Infection: A Systematic Review and Meta-Analysis. Infect. Control Hosp. Epidemiol. 2015, 36, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.J.; Seo, K.H.; Wi, Y.M. The effect of concomitant use of systemic antibiotics in patients with Clostridium difficile infection receiving metronidazole therapy. Epidemiol. Infect. 2018, 146, 558–664. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Louie, T.J.; Gerding, D.N.; Cornely, O.A.; Chasan-Taber, S.; Fitts, D.; Gelone, S.P.; Broom, C.; Davidson, D.M. Vancomycin, Metronidazole, or Tolevamer for Clostridium difficile Infection: Results From Two Multinational, Randomized, Controlled Trials. Clin. Infect. Dis. 2014, 59, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Zar, F.A.; Bakkanagari, S.R.; Moorthi, K.M.L.S.T.; Davis, M.B. A Comparison of Vancomycin and Metronidazole for the Treatment of Clostridium difficile-Associated Diarrhea, Stratified by Disease Severity. Clin. Infect. Dis. 2007, 45, 302–307. [Google Scholar] [CrossRef]
- Zhang, K.; Beckett, P.; Abouanaser, S.; Smieja, M. Initial vancomycin versus metronidazole for the treatment of first-episode non-severe Clostridioides difficile infection. Antimicrob. Steward. Healthc. Epidemiol. 2021, 1, e27. [Google Scholar] [CrossRef]
- Stevens, V.W.; Nelson, R.E.; Schwab-Daugherty, E.M.; Khader, K.; Jones, M.M.; Brown, K.A.; Greene, T.; Croft, L.D.; Neuhauser, M.; Glassman, P.; et al. Comparative Effectiveness of Vancomycin and Metronidazole for the Prevention of Recurrence and Death in Patients With Clostridium difficile Infection. JAMA Intern. Med. 2017, 177, 546. [Google Scholar] [CrossRef]
- Barbut, F. Prevalence and Pathogenicity of Clostridium difficile in Hospitalized Patients. Arch. Intern. Med. 1996, 156, 1449. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Q.; Gou, R.; Diao, Y.S.; Yin, Q.H.; Fan, W.X.; Liang, Y.P.; Chen, Y.; Wu, M.; Zang, L.; Li, L.; et al. Charlson comorbidity index helps predict the risk of mortality for patients with type 2 diabetic nephropathy. J. Zhejiang Univ. Sci. B 2014, 15, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Hsiao, H.L.; Chia, C.Y.; Cheng, C.W.; Tsai, T.C.; Deng, S.T.; Chen, C.L.; Chiu, C.H. Risk factors and outcomes of Clostridium difficile infection in hospitalized patients. Biomed. J. 2019, 42, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Feuerstadt, P.; Tillotson, G.; Archbald-Pannone, L.; Johnson, S.; Ng, S.; Ando, M.; Harvey, A. Efficacy and Safety of RBX2660 in Patients with Recurrent Clostridioides difficile Infection Grouped by Age and Underlying Comorbidities. Am. J. Gastroenterol. 2022, 117, e114–e115. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Hensgens, M.P.M.; Goorhuis, A.; Dekkers, O.M.; Kuijper, E.J. Time interval of increased risk for Clostridium difficile infection after exposure to antibiotics. J. Antimicrob. Chemother. 2011, 67, 742–748. [Google Scholar] [CrossRef]
- Stevens, V.W.; Thurm, C.; Schwab, E.M.; Kronman, M.P.; Gerber, J.S.; Shah, S.S.; Newland, J.G.; Courter, J.; Parker, S.; Brogan, T.V.; et al. Use of Concomitant Antibiotics During Treatment for Clostridium difficile Infection (CDI) in Pediatric Inpatients: An Observational Cohort Study. Infect. Dis. Ther. 2016, 5, 45–51. [Google Scholar] [CrossRef]
- van Prehn, J.; Reigadas, E.; Vogelzang, E.H.; Bouza, E.; Hristea, A.; Guery, B.; Krutova, M.; Norén, T.; Allerberger, F.; Coia, J.E.; et al. European Society of Clinical Microbiology and Infectious Diseases: 2021 update on the treatment guidance document for Clostridioides difficile infection in adults. Clin. Microbiol. Infect. 2021, 27, S1–S21. [Google Scholar] [CrossRef]
- Miller, R.; Morillas, J.A.; Brizendine, K.D.; Fraser, T.G. Predictors of Clostridioides difficile Infection-Related Complications and Treatment Patterns among Nucleic Acid Amplification Test-Positive/Toxin Enzyme Immunoassay-Negative Patients. J. Clin. Microbiol. 2020, 58, e01764-19. [Google Scholar] [CrossRef]
- Hota, S.S.; Achonu, C.; Crowcroft, N.S.; Harvey, B.J.; Lauwers, A.; Gardam, M.A. Determining Mortality Rates Attributable to Clostridium difficile Infection. Emerg. Infect. Dis. 2012, 18, 305–307. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, 31. [Google Scholar] [CrossRef] [PubMed]
- Patel, I.; Wungjiranirun, M.; Theethira, T.; Villafuerte-Galvez, J.; Castillo, N.; Akbari, M.; Alonso, C.D.; Leffler, D.A.; Kelly, C.P. Lack of adherence to SHEA-IDSA treatment guidelines for Clostridium difficile infection is associated with increased mortality. J. Antimicrob. Chemother. 2016, 72, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.T.; Seifert, C.F. Effect of Treatment Variation on Outcomes in Patients with Clostridium difficile. Am. J. Med. 2014, 127, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Ebben, R.H.A.; Siqeca, F.; Madsen, U.R.; Vloet, L.C.M.; van Achterberg, T. Effectiveness of implementation strategies for the improvement of guideline and protocol adherence in emergency care: A systematic review. BMJ Open 2017, 8, e017572. [Google Scholar] [CrossRef] [PubMed]
- Runnacles, J.; Roueché, A.; Lachman, P. The right care, every time: Improving adherence to evidence-based guidelines. Arch. Dis. Child. 2017, 103, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Tay, H.L.; Chow, A.; Ng, T.M.; Lye, D.C. Risk factors and treatment outcomes of severe Clostridioides difficile infection in Singapore. Sci. Rep. 2019, 9, 13440. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.P.; Hensgens, M.P.M.; Miller, M.A.; Gerding, D.N.; Wilcox, M.H.; Dale, A.P.; Fawley, W.N.; Kuijper, E.J.; Gorbach, S.L. Renal Failure and Leukocytosis Are Predictors of a Complicated Course of Clostridium difficile Infection if Measured on Day of Diagnosis. Clin. Infect. Dis. 2012, 55, 149–153. [Google Scholar] [CrossRef]
- Nelson, R.L.; Suda, K.J.; Evans, C.T. Antibiotic treatment for Clostridium difficile-associated diarrhoea in adults. Cochrane Database Syst. Rev. 2017, 3, 004610. [Google Scholar] [CrossRef]
- Bolton, R.P.; Culshaw, M.A. Faecal metronidazole concentrations during oral and intravenous therapy for antibiotic associated colitis due to Clostridium difficile. Gut 1986, 27, 1169–1172. [Google Scholar] [CrossRef]
- Napolitano, L.M.; Edmiston, C.E., Jr. Clostridium difficile disease: Diagnosis, pathogenesis, and treatment update. Surgery 2017, 162, 325–348. [Google Scholar] [CrossRef]
- Chilton, C.H.; Crowther, G.S.; Ashwin, H.; Longshaw, C.M.; Wilcox, M.H. Association of Fidaxomicin with C. difficile Spores: Effects of Persistence on Subsequent Spore Recovery, Outgrowth and Toxin Production. PLoS ONE 2016, 11, e0161200. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, M.; Pepin, J.; Frost, E.H.; Carrier, J.C.; Sirard, S.; Fortier, L.C.; Valiquette, L. Faecal pharmacokinetics of orally administered vancomycin in patients with suspected Clostridium difficile infection. BMC Infect. Dis. 2010, 10, 363. [Google Scholar] [CrossRef] [PubMed]
- Matzke, G.R.; Zhanel, G.G.; Guay, D.R.P. Clinical Pharmacokinetics of Vancomycin. Clin. Pharmacokinet. 1986, 11, 257–282. [Google Scholar] [CrossRef]
- Johnson, S.; Lavergne, V.; Skinner, A.M.; Gonzales-Luna, A.J.; Garey, K.W.; Kelly, C.P.; Wilcox, M.H. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 Focused Update Guidelines on Management of Clostridioides difficile Infection in Adults. Clin. Infect. Dis. 2021, 73, 1029–1044. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J.C.; Reilly, J.P.; Navalkele, B.; Downham, G.; Haynes, K.; Trivedi, M. Clinical and Economic Benefits of Fidaxomicin Compared to Vancomycin for Clostridium difficile Infection. Antimicrob. Agents Chemother. 2015, 59, 7007–7010. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, S.M.; Umscheid, C.A.; Fishman, N.; Lee, B.Y. Is Fidaxomicin Worth the Cost? An Economic Analysis. Clin. Infect. Dis. 2013, 57, 555–561. [Google Scholar] [CrossRef]
- Nathwani, D.; Cornely, O.A.; Van Engen, A.K.; Odufowora-Sita, O.; Retsa, P.; Odeyemi, I.A.O. Cost-effectiveness analysis of fidaxomicin versus vancomycin in Clostridium difficile infection. J. Antimicrob. Chemother. 2014, 69, 2901–2912. [Google Scholar] [CrossRef]
- Watt, M.; McCrea, C.; Johal, S.; Posnett, J.; Nazir, J. A cost-effectiveness and budget impact analysis of first-line fidaxomicin for patients with Clostridium difficile infection (CDI) in Germany. Infection 2016, 44, 599–606. [Google Scholar] [CrossRef]
- Swart, N.; Sinha, A.M.; Bentley, A.; Smethurst, H.; Spencer, G.; Ceder, S.; Wilcox, M.H. A cost-utility analysis of two Clostridioides difficile infection guideline treatment pathways. Clin. Microbiol. Infect. 2023, 29, 1291–1297. [Google Scholar] [CrossRef]
- Venugopal, A.A.; Johnson, S. Fidaxomicin: A Novel Macrocyclic Antibiotic Approved for Treatment of Clostridium difficile Infection. Clin. Infect. Dis. 2011, 54, 568–574. [Google Scholar] [CrossRef]
- Prunier, A.L.; Malbruny, B.; Tandé, D.; Picard, B.; Leclercq, R. Clinical Isolates of Staphylococcus aureus with Ribosomal Mutations Conferring Resistance to Macrolides. Antimicrob. Agents Chemother. 2002, 46, 3054–3056. [Google Scholar] [CrossRef] [PubMed]
- Fyfe, C.; Grossman, T.H.; Kerstein, K.; Sutcliffe, J. Resistance to Macrolide Antibiotics in Public Health Pathogens. Cold Spring Harb. Perspect. Med. 2016, 6, 025395. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, C.M.; McDermott, L.A.; Tran, M.K.; Chang, J.; Jenkins, S.G.; Goldstein, E.J.C.; Patel, R.; Forbes, B.A.; Johnson, S.; Gerding, D.N.; et al. U.S.-Based National Surveillance for Fidaxomicin Susceptibility of Clostridioides difficile-Associated Diarrheal Isolates from 2013 to 2016. Antimicrob. Agents Chemother. 2019, 63, e00391-19. [Google Scholar] [CrossRef]
- Sholeh, M.; Krutova, M.; Forouzesh, M.; Mironov, S.; Sadeghifard, N.; Molaeipour, L.; Maleki, A.; Kouhsari, E. Antimicrobial resistance in Clostridioides (Clostridium) difficile derived from humans: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control 2020, 9, 158. [Google Scholar] [CrossRef]
- Carlson, T.J.; Gonzales-Luna, A.J.; Nebo, K.; Chan, H.Y.; Tran, N.L.T.; Antony, S.; Lancaster, C.; Alam, M.J.; Begum, K.; Garey, K.W. Assessment of Kidney Injury as a Severity Criteria for Clostridioides Difficile Infection. Open Forum Infect. Dis. 2020, 7, 476. [Google Scholar] [CrossRef]
- Musher, D.M.; Aslam, S.; Logan, N.; Nallacheru, S.; Bhaila, I.; Borchert, F.; Hamill, R.J. Relatively Poor Outcome after Treatment of Clostridium difficile Colitis with Metronidazole. Clin. Infect. Dis. 2005, 40, 1586–1590. [Google Scholar] [CrossRef]
- Haubitz, S.; Bartlom, N.; Bucheli Laffer, E.; Spelters, C.; Fankhauser, H.; Fux, C.A. Outcome of Clostridioides difficile infections treated in a Swiss tertiary care hospital: An observational study. Swiss Med. Wkly. 2020, 150, 0102. [Google Scholar] [CrossRef]
- Lee, J.C.; Lee, C.C.; Chiu, C.W.; Tsai, P.J.; Hsueh, P.R.; Lee, Y.T.; Hung, Y.P.; Ko, W.C. Reappraisal of the clinical role of metronidazole therapy for Clostridioides difficile infection in Taiwan: A multicenter prospective study. J. Formos. Med. Assoc. 2022, 121, 2608–2616. [Google Scholar] [CrossRef]
- Adukauskienė, D.; Čyžiūtė, J.; Mickus, R.; Dambrauskienė, A. Dėmesio: Clostridium difficile infekcija. Sveik. Moksl. 2019, 29, 28–34. [Google Scholar] [CrossRef]
- Weinke, T.; Beier, D.; Brestrich, G.; von Eiff, C.; Häckl, D.; Heinrich, K.; Moïsi, J.; Schley, K. Epidemiology and Risk Factors of Clostridioides difficile Infections in Germany: A Health Claims Data Analysis. Infect. Dis. Ther. 2023, 12, 1299–1317. [Google Scholar] [CrossRef]
- Eze, P.; Balsells, E.; Kyaw, M.H.; Nair, H. Risk factors for Clostridium difficile infections—An overview of the evidence base and challenges in data synthesis. J. Glob. Health 2017, 7, 010417. [Google Scholar] [CrossRef] [PubMed]
- Abou Chakra, C.N.; Pepin, J.; Sirard, S.; Valiquette, L. Risk Factors for Recurrence, Complications and Mortality in Clostridium difficile Infection: A Systematic Review. PLoS ONE 2014, 9, 98400. [Google Scholar] [CrossRef]
- George, B.; Seals, S.; Aban, I. Survival analysis and regression models. J. Nucl. Cardiol. 2014, 21, 686–694. [Google Scholar] [CrossRef]
- Filippidis, P.; Kampouri, E.; Woelfle, M.; Badinski, T.; Croxatto, A.; Galperine, T.; Papadimitriou-Olivgeris, M.; Grandbastien, B.; Achermann, Y.; Guery, B. Treatment and Outcomes of Clostridioides difficile Infection in Switzerland: A Two-Center Retrospective Cohort Study. J. Clin. Med. 2022, 11, 3805. [Google Scholar] [CrossRef] [PubMed]
- Boeriu, A.; Roman, A.; Dobru, D.; Stoian, M.; Voidăzan, S.; Fofiu, C. The Impact of Clostridioides Difficile Infection in Hospitalized Patients: What Changed during the Pandemic? Diagnostics 2022, 12, 3196. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, R.C.; Salmanton-García, J.; Carney, J.; Böll, B.; Kochanek, M.; Jazmati, N.; Cornely, O.A.; Vehreschild, M.J.G.T. Clostridioides difficile infections in the intensive care unit: A monocentric cohort study. Infection 2020, 48, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.; Dean, B.; Nathanson, B.; Haidar, T.; Strauss, M.; Thomas, S. Length of stay and hospital costs among high-risk patients with hospital-origin Clostridium difficile-associated diarrhea. J. Med. Econ. 2013, 16, 440–448. [Google Scholar] [CrossRef]
- Mullane, K.M.; Miller, M.A.; Weiss, K.; Lentnek, A.; Golan, Y.; Sears, P.S.; Shue, Y.K.; Louie, T.J.; Gorbach, S.L. Efficacy of Fidaxomicin Versus Vancomycin as Therapy for Clostridium difficile Infection in Individuals Taking Concomitant Antibiotics for Other Concurrent Infections. Clin. Infect. Dis. 2011, 53, 440–447. [Google Scholar] [CrossRef]
- Chang, V.T.; Nelson, K. The Role of Physical Proximity in Nosocomial Diarrhea. Clin. Infect. Dis. 2000, 31, 717–722. [Google Scholar] [CrossRef]
- Hung, Y.P.; Lee, J.C.; Tsai, B.Y.; Wu, J.L.; Liu, H.C.; Liu, H.C.; Lin, H.J.; Tsai, P.J.; Ko, W.C. Risk factors of Clostridium difficile-associated diarrhea in hospitalized adults: Vary by hospitalized duration. J. Microbiol. Immunol. Infect. 2021, 54, 276–283. [Google Scholar] [CrossRef]
- Deshpande, A.; Pasupuleti, V.; Thota, P.; Pant, C.; Rolston, D.D.K.; Sferra, T.J.; Hernandez, A.V.; Donskey, C.J. Community-associated Clostridium difficile infection and antibiotics: A meta-analysis. J. Antimicrob. Chemother. 2013, 68, 1951–1961. [Google Scholar] [CrossRef]
- Slimings, C.; Riley, T.V. Antibiotics and hospital-acquired Clostridium difficile infection: Update of systematic review and meta-analysis. J. Antimicrob. Chemother. 2013, 69, 881–891. [Google Scholar] [CrossRef] [PubMed]
- Loo, V.G.; Poirier, L.; Miller, M.A.; Oughton, M.; Libman, M.D.; Michaud, S.; Bourgault, A.M.; Nguyen, T.; Frenette, C.; Kelly, M.; et al. A Predominantly Clonal Multi-Institutional Outbreak of Clostridium difficile–Associated Diarrhea with High Morbidity and Mortality. N. Engl. J. Med. 2005, 353, 2442–2449. [Google Scholar] [CrossRef] [PubMed]
- Pepin, J.; Saheb, N.; Coulombe, M.A.; Alary, M.E.; Corriveau, M.P.; Authier, S.; Leblanc, M.; Rivard, G.; Bettez, M.; Primeau, V.; et al. Emergence of Fluoroquinolones as the Predominant Risk Factor for Clostridium difficile-Associated Diarrhea: A Cohort Study during an Epidemic in Quebec. Clin. Infect. Dis. 2005, 41, 1254–1260. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.A.; Khanafer, N.; Daneman, N.; Fisman, D.N. Meta-Analysis of Antibiotics and the Risk of Community-Associated Clostridium difficile Infection. Antimicrob. Agents Chemother. 2013, 57, 2326–2332. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Laslop, N.; Mankin, A.S. How Macrolide Antibiotics Work. Trends Biochem. Sci. 2018, 43, 668–684. [Google Scholar] [CrossRef] [PubMed]
- Dubourg, G.; Lagier, J.C.; Robert, C.; Armougom, F.; Hugon, P.; Metidji, S.; Dione, N.; Dangui, N.P.M.; Pfleiderer, A.; Abrahao, J.; et al. Culturomics and pyrosequencing evidence of the reduction in gut microbiota diversity in patients with broad-spectrum antibiotics. Int. J. Antimicrob. Agents. 2014, 44, 117–124. [Google Scholar] [CrossRef]
- Patangia, D.V.; Anthony Ryan, C.; Dempsey, E.; Paul Ross, R.; Stanton, C. Impact of antibiotics on the human microbiome and consequences for host health. MicrobiologyOpen 2022, 11, e1260. [Google Scholar] [CrossRef]
- Williams, D.J.; Hall, M.; Shah, S.S.; Parikh, K.; Tyler, A.; Neuman, M.I.; Hersh, A.L.; Brogan, T.V.; Blaschke, A.J.; Grijalva, C.G. Narrow Vs Broad-spectrum Antimicrobial Therapy for Children Hospitalized with Pneumonia. Pediatrics 2013, 132, e1141–e1148. [Google Scholar] [CrossRef]
- Theriot, C.M.; Bowman, A.A.; Young, V.B. Antibiotic-Induced Alterations of the Gut Microbiota Alter Secondary Bile Acid Production and Allow for Clostridium difficile Spore Germination and Outgrowth in the Large Intestine. mSphere 2016, 1, e00045-15. [Google Scholar] [CrossRef]
- Rea, M.C.; Dobson, A.; O’Sullivan, O.; Crispie, F.; Fouhy, F.; Cotter, P.D.; Shanahan, F.; Kiely, B.; Hill, C.; Ross, R.P. Effect of broad- and narrow-spectrum antimicrobials on Clostridium difficile and microbial diversity in a model of the distal colon. Proc. Natl. Acad. Sci. USA 2010, 108, 4639–4644. [Google Scholar] [CrossRef] [PubMed]
- Teng, C.; Reveles, K.R.; Obodozie-Ofoegbu, O.O.; Frei, C.R. Clostridium difficile Infection Risk with Important Antibiotic Classes: An Analysis of the FDA Adverse Event Reporting System. Int. J. Med. Sci. 2019, 16, 630–635. [Google Scholar] [CrossRef]
- Panda, S. Medicine: Science or Art? Mens Sana Monogr. 2006, 4, 127. [Google Scholar] [CrossRef] [PubMed]
- Reller, M.E.; Lema, C.A.; Perl, T.M.; Cai, M.; Ross, T.L.; Speck, K.A.; Carroll, K.C. Yield of Stool Culture with Isolate Toxin Testing versus a Two-Step Algorithm Including Stool Toxin Testing for Detection of Toxigenic Clostridium difficile. J. Clin. Microbiol. 2007, 45, 3601–3605. [Google Scholar] [CrossRef] [PubMed]
- Mawer, D.P.C.; Eyre, D.W.; Griffiths, D.; Fawley, W.N.; Martin, J.S.H.; Quan, T.P.; Peto, T.E.A.; Crook, D.W.; Walker, A.S.; Wilcox, M.H. Contribution to Clostridium Difficile Transmission of Symptomatic Patients with Toxigenic Strains Who Are Fecal Toxin Negative. Clin. Infect. Dis. 2017, 64, 1163–1170. [Google Scholar] [CrossRef]
- van den Berg, R.J.; Vaessen, N.; Endtz, H.P.; Schülin, T.; van der Vorm, E.R.; Kuijper, E.J. Evaluation of real-time PCR and conventional diagnostic methods for the detection of Clostridium difficile-associated diarrhoea in a prospective multicentre study. J. Clin. Microbiol. 2007, 56, 36–42. [Google Scholar] [CrossRef]
- Deshpande, A.; Pasupuleti, V.; Rolston, D.D.K.; Jain, A.; Deshpande, N.; Pant, C.; Hernandez, A.V. Diagnostic Accuracy of Real-time Polymerase Chain Reaction in Detection of Clostridium difficile in the Stool Samples of Patients With Suspected Clostridium difficile Infection: A Meta-Analysis. Clin. Infect. Dis. 2011, 53, 81–90. [Google Scholar] [CrossRef]
- Lithuanian Institute of Hygiene. Report on Clostridioides Difficile Ribotypes and Antimicrobial Resistance 2019. Available online: https://www.hi.lt/uploads/pdf/tyrimai/2020/CDI_bandomojo_tyrimo_%20rezultatai.pdf (accessed on 25 October 2023).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| General Characteristics | |
|---|---|
| Age, years (Q1; Q3) | 67.0 (54.0; 77.0) |
| Immunocompromised patients, n (%) | 205 (55.4) |
| Serum creatinine, µmol/L (Q1; Q3) | 140.7 (76.0; 124.0) |
| Leucocytes, n × 109/L (Q1; Q3) | 10.1 (3.8; 13.5) |
| Hospital departments diagnosing CDID | |
| Medical, n (%) | 299 (80.8) |
| Surgical, n (%) | 56 (15.1) |
| Intensive Care Unit, n (%) | 15 (4.1) |
| Variable | OR for 30-Day All-Cause Mortality | 95% CI | p-Value |
|---|---|---|---|
| CCI score | 1.76 | 1.2–2.5 | 0.003 |
| Continuation of concomitant antibiotic | 3.2 | 1.02–10.4 | 0.047 |
| Leucocyte count, n × 109/L | 1.09 | 0.9–1.2 | 0.07 |
| Creatinine level, µmol/L | 1.003 | 0.9–1.03 | 0.7 |
| Presence of immunosuppression | 0.5 | 0.1–2.4 | 0.4 |
| Class of Antibiotic | Group 1 | Group 2 | p-Value |
|---|---|---|---|
| Second-generation cephalosporin, n (%) | 149 (75.6) | 102 (59.0) | 0.001 |
| Non-antipseudomonal third-generation cephalosporin, n (%) | 18 (9.1) | 4 (2.3) | 0.007 |
| Penicillin with beta-lactamase inhibitor, n (%) | 42 (21.3) | 59 (34.1) | 0.007 |
| Macrolide, n (%) | 4 (2.0) | 13 (7.5) | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adukauskienė, D.; Mickus, R.; Dambrauskienė, A.; Vanagas, T.; Adukauskaitė, A. Improving Clostridioides difficile Infectious Disease Treatment Response via Adherence to Clinical Practice Guidelines. Antibiotics 2024, 13, 51. https://doi.org/10.3390/antibiotics13010051
Adukauskienė D, Mickus R, Dambrauskienė A, Vanagas T, Adukauskaitė A. Improving Clostridioides difficile Infectious Disease Treatment Response via Adherence to Clinical Practice Guidelines. Antibiotics. 2024; 13(1):51. https://doi.org/10.3390/antibiotics13010051
Chicago/Turabian StyleAdukauskienė, Dalia, Rytis Mickus, Asta Dambrauskienė, Tomas Vanagas, and Agnė Adukauskaitė. 2024. "Improving Clostridioides difficile Infectious Disease Treatment Response via Adherence to Clinical Practice Guidelines" Antibiotics 13, no. 1: 51. https://doi.org/10.3390/antibiotics13010051
APA StyleAdukauskienė, D., Mickus, R., Dambrauskienė, A., Vanagas, T., & Adukauskaitė, A. (2024). Improving Clostridioides difficile Infectious Disease Treatment Response via Adherence to Clinical Practice Guidelines. Antibiotics, 13(1), 51. https://doi.org/10.3390/antibiotics13010051