


A Low Rate of Periprosthetic Infections after Aseptic Knee Prosthesis Revision Using Dual-Antibiotic-Impregnated Bone Cement

Abstract
:1. Introduction
2. Results
3. Discussion
- 1.
- 2.
- With respect to the elution of the individual antibiotics, both G and C are eluted more efficiently in the combination in dual ALBC than when alone in the cement. The molecules of both antibiotics are small and hydrophilic and have very good diffusion properties [22].
- 3.
- Due to the higher local release of the antibiotics, the otherwise bacteriostatic antibiotic clindamycin reaches local concentrations that make it bactericidal [22].
- 4.
- The mode of action or target of the antibiotics in bacteria is also synergistic in that gentamycin targets the 30 s ribosome on the mRNA while clindamycin has a different site of action, namely the 50 s ribosome. This means that the bacteria are attacked at two different sites at the same time, providing a synergy in the prevention of bacterial resistance development [22].
4. Materials and Methods
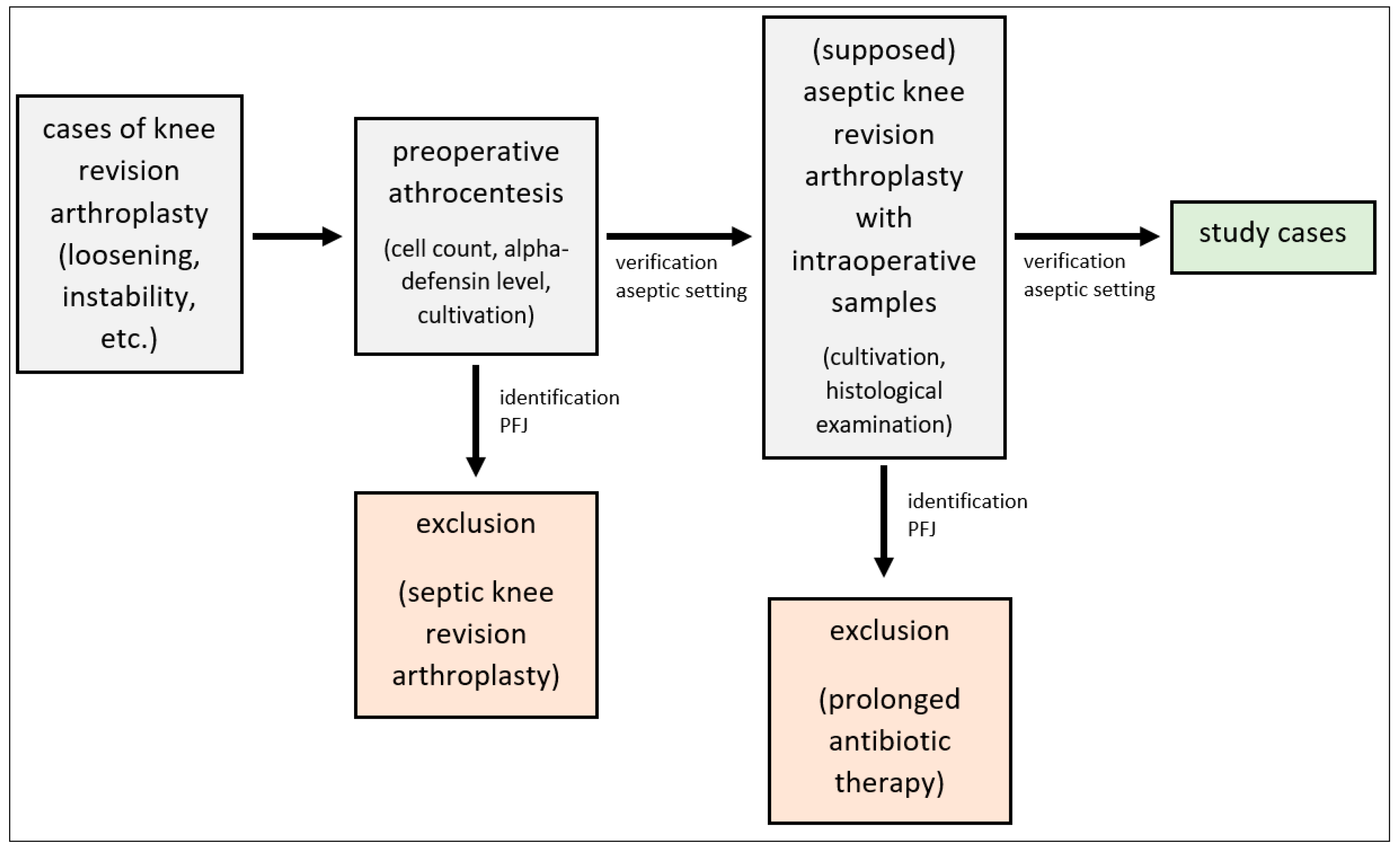
- 1.
- Identification of at least two synovial membrane samples with bacterial growth showing the same pathogen.
- 2.
- Identification of at least one synovial membrane sample with bacterial growth in combination with a histological examination showing at least five neutrophilic polymorph leukocytes in five high power fields (×400) and an increased CPR-value (>10 mg/L), as described in the MSIS-criteria [42] and in the ICM-2018-Definition [36], as well as in accordance with Feldman et al. [44].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blom, A.W.; Brown, J.; Taylor, A.H.; Pattison, G.; Whitehouse, S.; Bannister, G.C. Infection after total knee arthroplasty. J. Bone Jt. Surg. Br. 2004, 86-B, 688–691. [Google Scholar] [CrossRef] [PubMed]
- Bohl, D.D.; Sershon, R.A.; Fillingham, Y.A.; Della Valle, C.J. Incidence, risk factors, and sources of sepsis following total joint arthroplasty. J. Arthroplast. 2016, 31, 2875–2879. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Lau, E.; Watson, J.; Schmier, J.K.; Parvizi, J. Economic burden of periprosthetic joint infection in the United States. J. Arthroplast. 2012, 27, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Pulido, L.; Ghanem, E.; Joshi, A.; Purtill, J.J.; Parvizi, J. Periprosthetic join infection: The incidence, timing, and predisposing factors. Clin. Orthop. Relat. Res. 2008, 466, 1710–1715. [Google Scholar] [CrossRef] [PubMed]
- Zingg, M.; Kheir, M.M.; Ziemba-Davis, M.; Menethini, R.M. Reduced infection rate after aseptic revision total knee arthroplasty with extended oral antibiotic protocol. J. Arthroplast. 2022, 37, 905–909. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, N.D.; Werner, B.C.; Brown, T.E.; Browne, J.A. Risk of prosthetic joint infection increases following early aseptic revision surgery of total hip and knee arthroplasty. J. Arthroplast. 2020, 35, 3661–3667. [Google Scholar] [CrossRef]
- Tande, A.J.; Patel, R. Prosthetic Joint Infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef]
- Lemaignen, A.; Bernard, L.; Marmor, S.; Ferry, T.; Grammatico-Guillon, L.; Astagneau, P.; Scientific Committee for Complex Bone and Joint Infections Reference Centers (CRIOAc), on behalf of the CRIOAc network. Epidemiology of Complex Bone and Joint Infections in France Using a National Registry: The CRIOAc Network. J. Infect. 2021, 82, 199–206. [Google Scholar]
- Rodríguez-Pardo, D.; Pigrau, C.; Lora-Tamayo, J.; Soriano, A.; del Toro, M.D.; Cobo, J.; Palomino, J.; Euba, G.; Riera, M.; Sánchez-Somolinos, M.; et al. Gram-negative Prosthetic Joint Infection: Outcome of a Debridement, Antibiotics and Implant Retention Approach. A Large Multicentre Study. Clin. Microbiol. Infect. 2014, 20, 911–919. [Google Scholar] [CrossRef]
- Hsieh, P.H.; Lee, M.S.; Hsu, K.Y.; Chang, Y.H.; Shih, H.N.; Ueng, S.W. Gram-negative Prosthetic Joint Infections: Risk Factors and Outcome of Treatment. Clin. Infect. Dis. 2009, 49, 1036–1043. [Google Scholar] [CrossRef]
- Zmistowski, B.; Fedorka, C.J.; Sheehan, E.; Deirmengian, G.; Austin, M.S.; Parvizi, J. Prosthetic Joint Infection Caused by Gram-negative Organisms. J. Arthroplast. 2011, 26, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Berberich, C.E.; Josse, J.; Laurent, F.; Ferry, T. Dual antibiotic loaded bone cement in patients at high infection risks in arthroplasty: Rationale of use for prophylaxis and scientific evidence. World J. Orthop. 2021, 12, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Hickson, C.J.; Metcalfe, D.; Elgohari, S.; Oswald, T.; Masters, J.P.; Rymaszewska, M.; Reed, M.R.; Sprowson, A.P. Prophylactic antibiotics in elective hip and knee arthroplasty: An analysis of organisms reported to cause infections and National survey of clinical practice. Bone Jt. Res. 2015, 4, 181–189. [Google Scholar] [CrossRef]
- Nodzo, S.R.; Boyle, K.K.; Frisch, N.B. Nationwide Organism Susceptibility Patterns to Common Preoperative Prophylactic Antibiotics: What Are We Covering? J. Arthroplast. 2019, 34, 302–306. [Google Scholar] [CrossRef] [PubMed]
- Anagnostakos, K.; Kelm, J.; Regitz, T.; Schmitt, E.; Jung, W. In vitro evaluation of antibiotic release from and bacteria growth inhibition by antibiotic-loaded acrylic bone cement spacers. J. Biomed. Mater. Res. B Appl. Biomater. 2005, 72, 373–378. [Google Scholar] [CrossRef]
- Baleani, M.; Persson, C.; Zolezzi, C.; Andollina, A.; Borrelli, A.M.; Tigani, D. Biological and biomechanical effects of vancomycin and meropenem in acrylic bone cement. J. Arthroplast. 2008, 23, 1232–1238. [Google Scholar] [CrossRef]
- Ensing, G.T.; van Horn, J.R.; van der Mei, H.C.; Busscher, H.J.; Neut, D. Copal bone cement is more effective in preventing biofilm formation than Palacos R-G. Clin. Orthop. Relat. Res. 2008, 466, 1492–1498. [Google Scholar] [CrossRef]
- Penner, M.J.; Masri, B.A.; Duncan, C.P. Elution characteristics of vancomycin and tobramycin combined in acrylic bone-cement. J. Arthroplast. 1996, 11, 939–944. [Google Scholar] [CrossRef]
- Simpson, P.M.; Dall, G.F.; Breusch, S.J.; Heisel, C. In vitro elution and mechanical properties of antibiotic-loaded SmartSet HV and Palacos R acrylic bone cements. Orthopäde 2005, 34, 1255–1262. [Google Scholar] [CrossRef]
- Cara, A.; Ferry, T.; Laurent, F.; Josse, J. Prophylacitc antibiofilm activity on antibiotic-loaded bone cements against Gram-negative bacteria. Antibiotics 2022, 11, 137. [Google Scholar] [CrossRef]
- Sanz-Ruiz, P.; Matas-Diez, J.A.; Villanueva-Martínez, M.; Santos-Vaquinha Blanco, A.D.; Vaquero, J. Is Dual Antibiotic-Loaded Bone Cement More Effective and Cost-Efficient Than a Single Antibiotic-Loaded Bone Cement to Reduce the Risk of Prosthetic Joint Infection in Aseptic Revision Knee Arthroplasty? J. Arthroplast. 2020, 35, 3724–3729. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, A.; Lieb, E.; Berberich, C.; Kühn, K.D. PMMA cements in revision surgery. In Management of Periprosthetic Joint Infection; Kühn, K.D., Ed.; Springer: Berlin, Germany, 2018; pp. 243–255. [Google Scholar]
- Sprowson, A.P.; Jensen, C.; Chambers, S.; Parsons, N.R.; Aradhyula, N.M.; Carluke, I.; Inman, D.; Reed, M.R. The use of high-dose dual-impregnated antibiotic-laden cement with hemiarthroplasty for the treatment of a fracture of the hip: The Fractured Hip Infection trial. Bone Jt. J. 2016, 98-B, 1534–1541. [Google Scholar] [CrossRef] [PubMed]
- Tyas, B.; Marsh, M.; Oswald, T.; Refaie, R.; Molyneux, C.; Reed, M. Antibiotic resistance profiles of deep surgical site infections in hip hemiarthroplasty; comparing low dose single antibiotic vs high dose dual antibiotic impregnated cement. J. Bone Jt. Infect. 2018, 3, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Savage, P.; McCormick, M.; Al-Dadah, O. Arthroplasty infection rates in fractured neck of femur: Single vs dual antibiotic cement. Ann. R. Coll. Surg. Engl. 2019, 101, 514–518. [Google Scholar] [CrossRef] [PubMed]
- Houfani, F.; Mainard, D.; Rubens-Duval, B.; Papin, P.E.; Pasquier, G.; Ehlinger, M.; French Society for Orthopaedic, Trauma Surgery (SoFCOT). Rotating-hinge prosthesis for aseptic revision knee arthroplasty: A multicentre retrospective study of 127 cases with a mean follow-up of five years. Orthop. Traumatol. Surg. Res. 2021, 107, 102855. [Google Scholar] [CrossRef]
- Clement, N.D.; Avery, P.; Mason, J.; Baker, P.N.; Deehan, D.J. First-time revision knee arthroplasty using a hinged prosthesis: Temporal trends, indications, and risk factors associated with re-revision using data from the National Joint Registry for 3855 patients. Bone Jt. J. 2023, 105-B, 47–55. [Google Scholar] [CrossRef]
- Coventry, M.B. Treatment of infections occurring in total hip surgery. Orthop. Clin. N. Am. 1975, 6, 991–1003. [Google Scholar] [CrossRef]
- Della Valle, C.J.; Zuckerman, J.D.; Di Cesare, P.E. Periprosthetic sepsis. Clin. Orthop. Relat. Res. 2004, 420, 26–31. [Google Scholar] [CrossRef]
- Lehner, B.; Witte, V.; Suda, A.J.; Weiss, S. Revision strategy for periprosthetic infection. Orthopade 2009, 38, 681–688. [Google Scholar] [CrossRef]
- Haleem, A.A.; Berry, D.J.; Hanssen, A.D. Mid-term to long-term followup of two-stage reimplantation for infected total knee arthroplasty. Clin. Orthop. Relat. Res. 2004, 428, 35–39. [Google Scholar] [CrossRef]
- Kurd, M.F.; Ghanem, E.; Steinbrecher, J.; Parvizi, J. Two-stage exchange knee arthroplasty. Does resistance of the infecting organism influence the outcome? Clin. Orthop. Relat. Res. 2010, 468, 2060–2066. [Google Scholar] [CrossRef] [PubMed]
- Teves, J.; Holc, F.; Castro Lalín, A.; García-Mansilla, A.; Vildoza, S.; Brandariz, R.; Carbó, L.; Costantini, J. Are frailty scores superior to the ASA score in predicting complications, hospital stay, and readmissions in total knee replacement? A comparative study between octogenarian and septuagenarian patients. Rev. Esp. Cir. Ortop. Traumatol. 2023, 30, S1888-4415(23)00123-6. [Google Scholar] [CrossRef]
- Quach, L.H.; Jayamaha, S.; Whitehouse, S.L.; Crawford, R.; Pulle, C.R.; Bell, J.J. Comparison of the Charlson Comorbidity Index with the ASA score for predicting 12-month mortality in acute hip fracture. Injury 2020, 51, 1004–1010. [Google Scholar] [CrossRef]
- Glasheen, W.P.; Cordier, T.; Gumpina, R.; Haugh, G.; Davis, J.; Renda, A. Charlson Comorbidity Index: ICD-9 Update and ICD-10 Translation. Am. Health Drug Benefits 2019, 12, 188–197. [Google Scholar] [PubMed]
- Schäfer, P.; Fink, B.; Sandow, D.; Margull, A.; Berger, I.; Frommelt, L. Prolonged bacterial culture to identify late periprosthetic joint infection: A promising strategy. Clin. Infect. Dis. 2008, 47, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of periprosthetic hip and knee infection: An evidence-based and validated criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef]
- Steinbrink, K.; Frommelt, L. Treatment of periprosthetic infection of the hip using one-stage exchange surgery. Orthopäde 1995, 24, 335–343. [Google Scholar]
- Atkins, B.L.; Athanasou, N.; Deeks, J.J.; Crook, D.W.; Simpson, H.; Peto, T.E.; McLardy-Smith, P.; Berendt, A.R. Prospective evaluation of criteria for microbiological diagnosis of prosthetic-joint infection at revision arthroplasty. J. Clin. Microbiol. 1998, 36, 2932–2939. [Google Scholar] [CrossRef]
- Virolainen, P.; Lahteenmaki, H.; Hiltunen, A.; Sipola, E.; Meurman, O.; Nelimarkka, O. The reliability of diagnosis of infection during revision arthroplasties. Scand. J. Surg. 2002, 91, 178–181. [Google Scholar] [CrossRef]
- Ince, A.; Rupp, J.; Frommelt, L.; Katzer, A.; Gille, J.; Löhr, J.F. Is “aseptic” loosening of the prosthetic cup after total hip replacement due to nonculturable bacterial pathogens in patients with low-grade infection? Clin. Inf. Dis. 2004, 39, 1599–1603. [Google Scholar] [CrossRef]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New definition for periprosthetc joint infection: From the Workgroup of the Musculoskeletal Infection Society. Clin. Orthop. Relat. Res. 2011, 469, 2992–2994. [Google Scholar] [CrossRef] [PubMed]
- Pandey, R.; Drakouilakis, E.; Athanasou, N.A. An assessment of the histological criteria used to diagnose infection in hip revision arthroplasty tissues. J. Clin. Pathol. 1999, 52, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.S.; Lonner, J.H.; Desai, P.; Zuckerman, J.D. The role of intraoperative frozen sections in revision total joint arthroplasty. J. Bone Jt. Surg. Am. 1995, 77-A, 1807–1813. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Periprosthetic Joint Infection | Aseptic Loosening | Hematoma | Low Range of Motion | Dislocation of Insert | Periprosthetic Fracture | Superficial Wound Healing Problems without Infection | ||
|---|---|---|---|---|---|---|---|---|---|
| medial uni- to bicondylar TKA | 120 | 2 | 1 | 1 | 1 | 5 | |||
| lateral uni- to bicondylar TKA | 8 | 1 | 1 | ||||||
| medial uni- to rotating hinge | 20 | 0 | |||||||
| bicondylar to rotating hinge | 188 | 2 | 6 | 1 | 1 | 2 | 3 | 15 | |
| rotating hinge to rotating hinge | 41 | 1 | 1 | 4 | 1 | 7 | |||
| exchange of only one component of bicondylar TKA | 26 | 1 | 2 | 1 | 4 | ||||
| 5 | 9 | 1 | 2 | 2 | 8 | 5 | 32 |
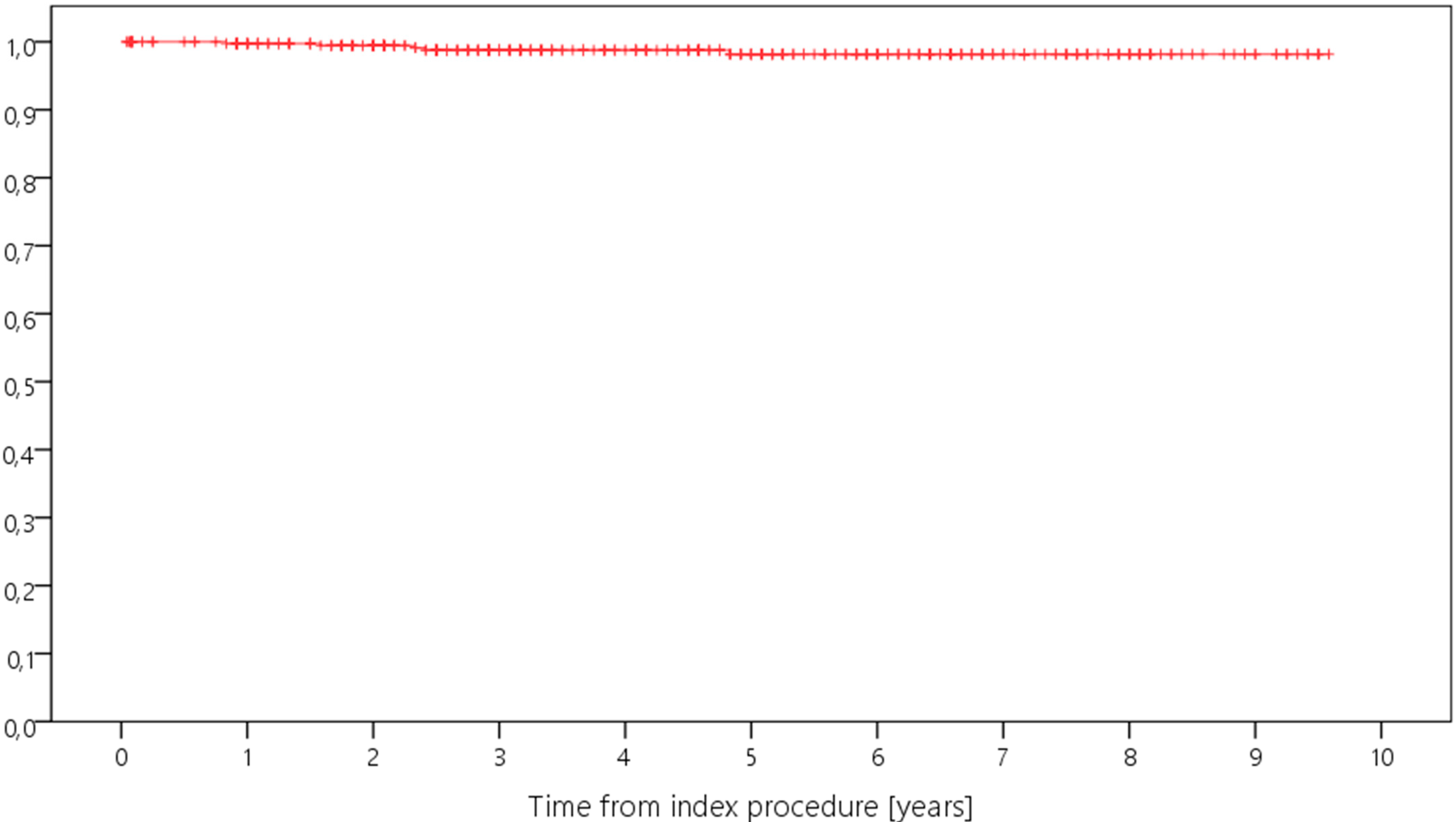
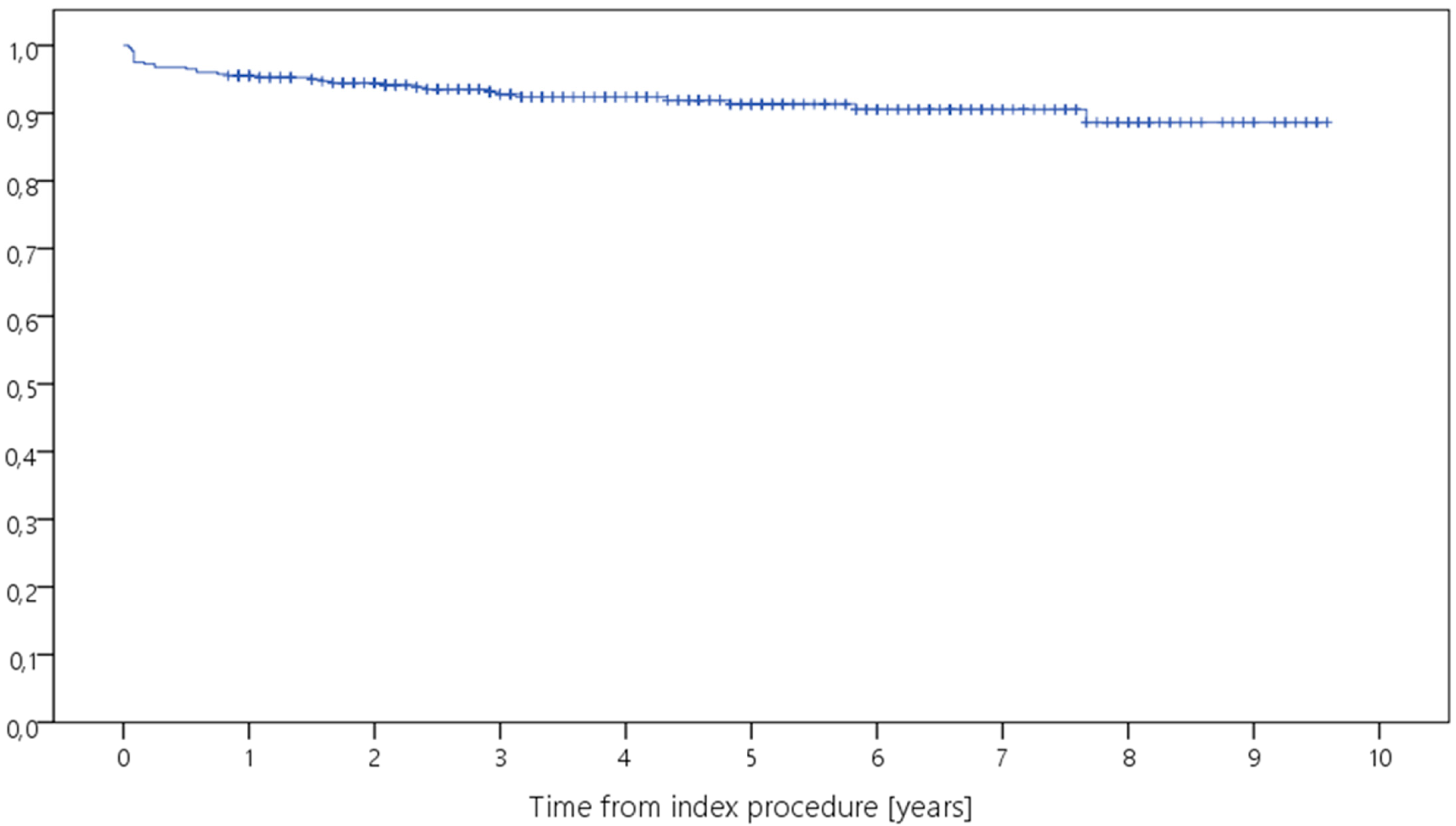
| Survival Cohort | Survival for Revision for Any Reason | Survival for Revision for PJI |
|---|---|---|
| whole study group | 91.3% [88.2–94.4%] | 98.2% [98.7–99.9%] |
| medial UKA to TKA | 95.0% [90.7–99.3%] | 98.1% [95.5–100.0%] |
| lateral UKA to TKA | 100.0% | 100.0% |
| medial UKA to hinged TKA | 100.0% | 100.0% |
| TKA to hinged TKA | 90.7% [85.8–95.6%] | 97.9% [95.0–100.0%] |
| hinged TKA to hinged TKA | 82.5% [70.7–94.3%] | 97.2% [91.9–100.0%] |
| change of femoral or tibial component | 84.6% [70.7–98.5%] | 100.0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blersch, B.P.; Barthels, M.; Schuster, P.; Fink, B. A Low Rate of Periprosthetic Infections after Aseptic Knee Prosthesis Revision Using Dual-Antibiotic-Impregnated Bone Cement. Antibiotics 2023, 12, 1368. https://doi.org/10.3390/antibiotics12091368
Blersch BP, Barthels M, Schuster P, Fink B. A Low Rate of Periprosthetic Infections after Aseptic Knee Prosthesis Revision Using Dual-Antibiotic-Impregnated Bone Cement. Antibiotics. 2023; 12(9):1368. https://doi.org/10.3390/antibiotics12091368
Chicago/Turabian StyleBlersch, Benedikt Paul, Michael Barthels, Philipp Schuster, and Bernd Fink. 2023. "A Low Rate of Periprosthetic Infections after Aseptic Knee Prosthesis Revision Using Dual-Antibiotic-Impregnated Bone Cement" Antibiotics 12, no. 9: 1368. https://doi.org/10.3390/antibiotics12091368
APA StyleBlersch, B. P., Barthels, M., Schuster, P., & Fink, B. (2023). A Low Rate of Periprosthetic Infections after Aseptic Knee Prosthesis Revision Using Dual-Antibiotic-Impregnated Bone Cement. Antibiotics, 12(9), 1368. https://doi.org/10.3390/antibiotics12091368