
Updated Review on Clinically-Relevant Properties of Delafloxacin



Abstract
1. Introduction
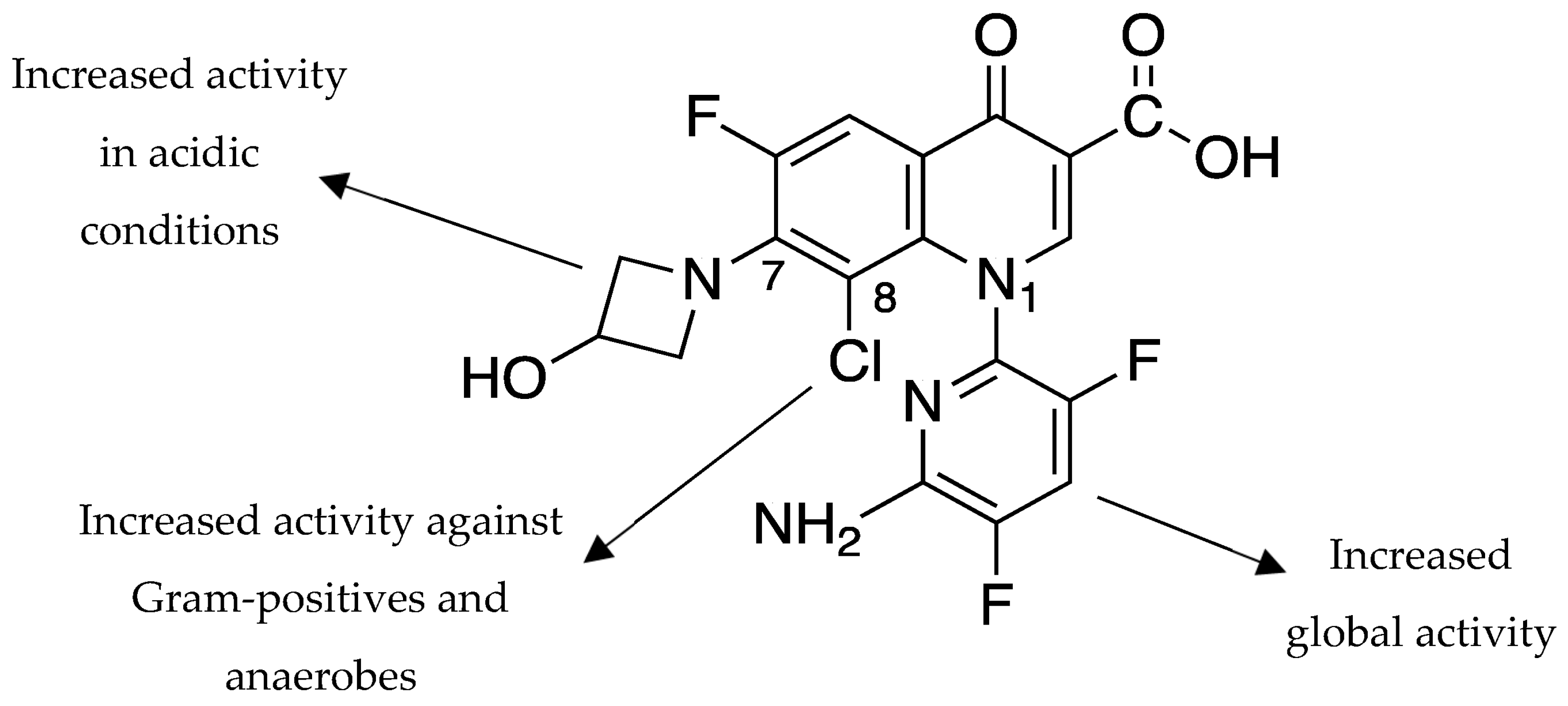
2. Structure-Activity Relationships and Mechanism of Action
3. Pharmacokinetics and Pharmacodynamics
4. In Vitro Activity
4.1. Activity against Gram-Positive Bacteria
4.2. Activity against Gram-Negative Bacteria
4.3. Activity against Other Bacteria
5. Mechanisms of Resistance to Delafloxacin
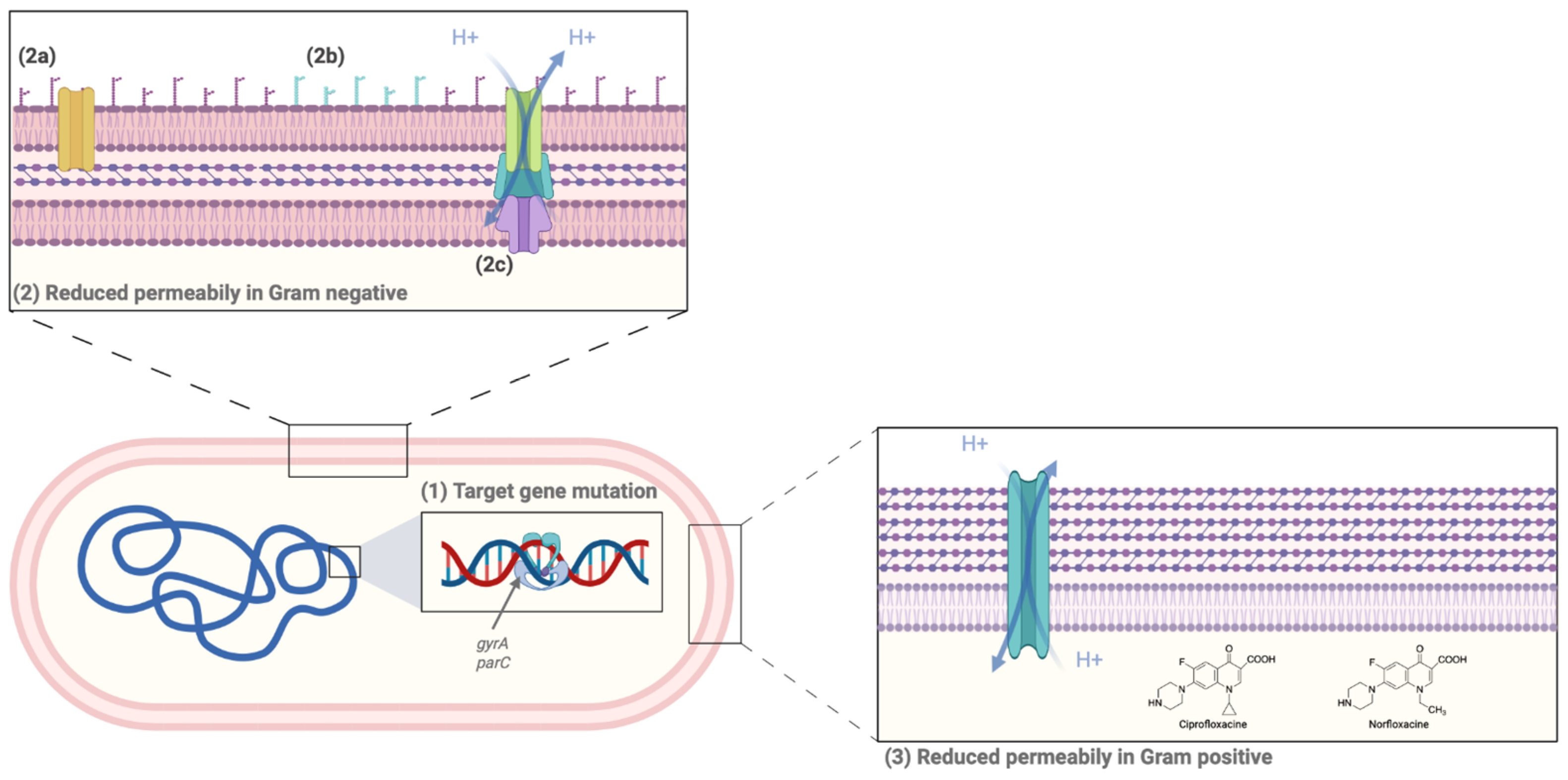
5.1. Main Mechanisms of FQ Resistance
5.1.1. Target Gene Mutation
5.1.2. Decrease in Intracellular Drug Concentration
5.1.3. Plasmid-Mediated Quinolone Resistance (PMQR)
5.2. Resistance to DLX
6. In Vivo Efficacy
6.1. Animal Models
6.2. Phase II Clinical Trials
6.3. Phase III Clinical Trials
6.3.1. ABSSSI Phase III Clinical Trials
6.3.2. CABP Phase III Trial
6.3.3. Uncomplicated Gonorrhea Phase III Trials
7. Safety
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lesher, G.; Froelich, E.; Gruett, M.; Bailey, J.; Brundage, R. 1,8-Naphthyridine Derivatives. A New Class Of Chemotherapeutic Agents. J. Med. Pharm. Chem. 1962, 91, 1063–1065. [Google Scholar] [CrossRef] [PubMed]
- Pullman, J.; Gardovskis, J.; Farley, B.; Sun, E.; Quintas, M.; Lawrence, L.; Ling, R.; Cammarata, S.; PROCEED Study Group. Efficacy and Safety of Delafloxacin Compared with Vancomycin plus Aztreonam for Acute Bacterial Skin and Skin Structure Infections: A Phase 3, Double-Blind, Randomized Study. J. Antimicrob. Chemother. 2017, 72, 3471–3480. [Google Scholar] [CrossRef] [PubMed]
- O’Riordan, W.; McManus, A.; Teras, J.; Poromanski, I.; Cruz-Saldariagga, M.; Quintas, M.; Lawrence, L.; Liang, S.; Cammarata, S.; PROCEED Study Group; et al. A Comparison of the Efficacy and Safety of Intravenous Followed by Oral Delafloxacin With Vancomycin Plus Aztreonam for the Treatment of Acute Bacterial Skin and Skin Structure Infections: A Phase 3, Multinational, Double-Blind, Randomized Study. Clin. Infect. Dis. 2018, 67, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Hook, E.W.; Golden, M.R.; Taylor, S.N.; Henry, E.; Tseng, C.; Workowski, K.A.; Swerdlow, J.; Nenninger, A.; Cammarata, S. Efficacy and Safety of Single-Dose Oral Delafloxacin Compared With Intramuscular Ceftriaxone for Uncomplicated Gonorrhea Treatment: An Open-Label, Noninferiority, Phase 3, Multicenter, Randomized Study. Sex. Trans. Dis. 2019, 46, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Horcajada, J.P.; Salata, R.A.; Álvarez-Sala, R.; Nitu, F.M.; Lawrence, L.; Quintas, M.; Cheng, C.-Y.; Cammarata, S.; DEFINE-CABP Study Group. A Phase 3 Study to Compare Delafloxacin With Moxifloxacin for the Treatment of Adults With Community-Acquired Bacterial Pneumonia (DEFINE-CABP). Open Forum Infect. Dis. 2020, 7, ofz514. [Google Scholar] [CrossRef]
- Panholzer, J.; Neuboeck, M.; Shao, G.; Heldt, S.; Winkler, M.; Greiner, P.; Fritsch, N.; Lamprecht, B.; Salzer, H. Ciprofloxacin-Resistant Pseudomonas Aeruginosa Lung Abscess Complicating COVID-19 Treated with the Novel Oral Fluoroquinolone Delafloxacin. Case Rep. Pulmonol. 2022, 2022, 1008330. [Google Scholar] [CrossRef]
- Bouchand, C.; Navas, D.; Corvec, S.; Pattier, S.; Roussel, J.-C.; Lepoivre, T.; Bonsergent, M.; Boutoille, D.; Bémer, P.; Lecomte, R. Postoperative Linezolid-Resistant Methicillin-Resistant Staphylococcus epidermidis Mediastinitis in a Heart Transplant Patient: First Case of Therapeutic Success with Delafloxacin. J. Glob. Antimicrob. Resist. 2023, 32, 72–73. [Google Scholar] [CrossRef]
- Hornak, J.P.; Reynoso, D. Early Clinical Experience with Delafloxacin: A Case Series. Am. J. Med. Sci. 2022, 363, 359–363. [Google Scholar] [CrossRef]
- Iregui, A.; Khan, Z.; Malik, S.; Landman, D.; Quale, J. Emergence of Delafloxacin-Resistant Staphylococcus aureus in Brooklyn, New York. Clin. Infect. Dis. 2020, 70, 1758–1760. [Google Scholar] [CrossRef]
- de la Rosa, J.M.O.; Fernández, M.A.; Rodríguez-Villodres, Á.; Casimiro-Soriguer, C.S.; Cisneros, J.M.; Lepe, J.A. High-Level Delafloxacin Resistance through the Combination of Two Different Mechanisms in Staphylococcus aureus. Int. J. Antimicrob. Agents 2023, 61, 106795. [Google Scholar] [CrossRef]
- Remy, J.M.; Tow-Keogh, C.A.; McConnell, T.S.; Dalton, J.M.; Devito, J.A. Activity of Delafloxacin against Methicillin-Resistant Staphylococcus aureus: Resistance Selection and Characterization. J. Antimicrob. Chemother. 2012, 67, 2814–2820. [Google Scholar] [CrossRef] [PubMed]
- Soge, O.O.; Salipante, S.J.; No, D.; Duffy, E.; Roberts, M.C. In Vitro Activity of Delafloxacin against Clinical Neisseria Gonorrhoeae Isolates and Selection of Gonococcal Delafloxacin Resistance. Antimicrob. Agents Chemother. 2016, 60, 3106–3111. [Google Scholar] [CrossRef]
- Byrd, B.A.; Zenick, B.; Rocha-Granados, M.C.; Englander, H.E.; Hare, P.J.; LaGree, T.J.; DeMarco, A.M.; Mok, W.W.K. The AcrAB-TolC Efflux Pump Impacts Persistence and Resistance Development in Stationary-Phase Escherichia Coli Following Delafloxacin Treatment. Antimicrob. Agents Chemother. 2021, 65, e0028121. [Google Scholar] [CrossRef] [PubMed]
- Gulyás, D.; Kamotsay, K.; Szabó, D.; Kocsis, B. Investigation of Delafloxacin Resistance in Multidrug-Resistant Escherichia Coli Strains and the Detection of E. Coli ST43 International High-Risk Clone. Microorganisms 2023, 11, 1602. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.D.M.; Ziora, Z.M.; Blaskovich, M.A.T. Quinolone Antibiotics. Med. Chem. Commun. 2019, 10, 1719–1739. [Google Scholar] [CrossRef]
- Tulkens, P.M.; Van Bambeke, F.; Zinner, S.H. Profile of a Novel Anionic Fluoroquinolone-Delafloxacin. Clin. Infect. Dis. 2019, 68, S213–S222. [Google Scholar] [CrossRef]
- Kocsis, B.; Domokos, J.; Szabo, D. Chemical Structure and Pharmacokinetics of Novel Quinolone Agents Represented by Avarofloxacin, Delafloxacin, Finafloxacin, Zabofloxacin and Nemonoxacin. Ann. Clin. Microbiol. Antimicrob. 2016, 15, 34. [Google Scholar] [CrossRef]
- Kocsis, B.; Gulyás, D.; Szabó, D. Delafloxacin, Finafloxacin, and Zabofloxacin: Novel Fluoroquinolones in the Antibiotic Pipeline. Antibiotics 2021, 10, 1506. [Google Scholar] [CrossRef]
- Kuramoto, Y.; Ohshita, Y.; Yoshida, J.; Yazaki, A.; Shiro, M.; Koike, T. A Novel Antibacterial 8-Chloroquinolone with a Distorted Orientation of the N1-(5-Amino-2,4-Difluorophenyl) Group. J. Med. Chem. 2003, 46, 1905–1917. [Google Scholar] [CrossRef]
- Van Bambeke, F. Delafloxacin, a Non-Zwitterionic Fluoroquinolone in Phase III of Clinical Development: Evaluation of Its Pharmacology, Pharmacokinetics, Pharmacodynamics and Clinical Efficacy. Future Microbiol. 2015, 10, 1111–1123. [Google Scholar] [CrossRef]
- Lemaire, S.; Tulkens, P.M.; Van Bambeke, F. Contrasting Effects of Acidic PH on the Extracellular and Intracellular Activities of the Anti-Gram-Positive Fluoroquinolones Moxifloxacin and Delafloxacin against Staphylococcus aureus. Antimicrob. Agents Chemother. 2011, 55, 649–658. [Google Scholar] [CrossRef]
- So, W.; Crandon, J.L.; Nicolau, D.P. Effects of Urine Matrix and PH on the Potency of Delafloxacin and Ciprofloxacin against Urogenic Escherichia Coli and Klebsiella Pneumoniae. J. Urol. 2015, 194, 563–570. [Google Scholar] [CrossRef]
- Bassetti, M.; Della Siega, P.; Pecori, D.; Scarparo, C.; Righi, E. Delafloxacin for the Treatment of Respiratory and Skin Infections. Expert Opin. Investig. Drugs 2015, 24, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Vialichka, A.; Biagi, M.; Meyer, K.; Wu, T.; Shajee, A.; Tan, X.; Wenzler, E. Activity of Delafloxacin and Levofloxacin against Stenotrophomonas Maltophilia at Simulated Plasma and Intrapulmonary PH Values. Microbiol. Spectr. 2022, 10, e0270521. [Google Scholar] [CrossRef] [PubMed]
- Bush, N.G.; Evans-Roberts, K.; Maxwell, A. DNA Topoisomerases. EcoSal Plus 2015, 6. [Google Scholar] [CrossRef]
- Wang, J.C. Cellular Roles of DNA Topoisomerases: A Molecular Perspective. Nat. Rev. Mol. Cell Biol. 2002, 3, 430–440. [Google Scholar] [CrossRef]
- Deweese, J.E.; Osheroff, M.A.; Osheroff, N. DNA Topology and Topoisomerases: Teaching a “Knotty” Subject. Biochem. Mol. Biol. Educ. 2009, 37, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Nilius, A.M.; Shen, L.L.; Hensey-Rudloff, D.; Almer, L.S.; Beyer, J.M.; Balli, D.J.; Cai, Y.; Flamm, R.K. In Vitro Antibacterial Potency and Spectrum of ABT-492, a New Fluoroquinolone. Antimicrob Agents Chemother 2003, 47, 3260–3269. [Google Scholar] [CrossRef]
- Drlica, K.; Zhao, X. DNA Gyrase, Topoisomerase IV, and the 4-Quinolones. Microbiol. Mol. Biol. Rev. 1997, 61, 16. [Google Scholar]
- Fournier, B.; Zhao, X.; Lu, T.; Drlica, K.; Hooper, D.C. Selective Targeting of Topoisomerase IV and DNA Gyrase in Staphylococcus aureus: Different Patterns of Quinolone- Induced Inhibition of DNA Synthesis. Antimicrob. Agents Chemother. 2000, 44, 2160–2165. [Google Scholar] [CrossRef] [PubMed]
- Scott, L.J. Delafloxacin: A Review in Acute Bacterial Skin and Skin Structure Infections. Drugs 2020, 80, 1247–1258. [Google Scholar] [CrossRef] [PubMed]
- Kakoullis, L.; Papachristodoulou, E.; Chra, P.; Panos, G. Mechanisms of Antibiotic Resistance in Important Gram-Positive and Gram-Negative Pathogens and Novel Antibiotic Solutions. Antibiotics 2021, 10, 415. [Google Scholar] [CrossRef]
- Lodise, T.; Corey, R.; Hooper, D.; Cammarata, S. Safety of Delafloxacin: Focus on Adverse Events of Special Interest. Open Forum Infect. Dis. 2018, 5, ofy220. [Google Scholar] [CrossRef] [PubMed]
- Alam, P.; Iqbal, M.; Ezzeldin, E.; Khalil, N.Y.; Foudah, A.I.; Alqarni, M.H.; Shakeel, F. Simple and Accurate HPTLC-Densitometric Method for Quantification of Delafloxacin (A Novel Fluoroquinolone Antibiotic) in Plasma Samples: Application to Pharmacokinetic Study in Rats. Antibiotics 2020, 9, 134. [Google Scholar] [CrossRef] [PubMed]
- Hernandis, V.; Escudero, E.; Marín, P. A Novel Liquid Chromatography-Fluorescence Method for the Determination of Delafloxacin in Human Plasma. J. Sep. Sci. 2021, 45, 706–716. [Google Scholar] [CrossRef]
- Hoover, R.; Hunt, T.; Benedict, M.; Paulson, S.K.; Lawrence, L.; Cammarata, S.; Sun, E. Safety, Tolerability, and Pharmacokinetic Properties of Intravenous Delafloxacin After Single and Multiple Doses in Healthy Volunteers. Clin. Ther. 2016, 38, 53–65. [Google Scholar] [CrossRef]
- Mogle, B.T.; Steele, J.M.; Thomas, S.J.; Bohan, K.H.; Kufel, W.D. Clinical Review of Delafloxacin: A Novel Anionic Fluoroquinolone. J. Antimicrob. Chemother. 2018, 73, 1439–1451. [Google Scholar] [CrossRef]
- Hoover, R.; Hunt, T.; Benedict, M.; Paulson, S.K.; Lawrence, L.; Cammarata, S.; Sun, E. Single and Multiple Ascending-Dose Studies of Oral Delafloxacin: Effects of Food, Sex, and Age. Clin. Ther. 2016, 38, 39–52. [Google Scholar] [CrossRef]
- Shiu, J.; Ting, G.; Kiang, T.K. Clinical Pharmacokinetics and Pharmacodynamics of Delafloxacin. Eur. J. Drug Metab. Pharmacokinet. 2019, 44, 305–317. [Google Scholar] [CrossRef]
- McEwen, A.; Lawrence, L.; Hoover, R.; Stevens, L.; Mair, S.; Ford, G.; Williams, D.; Wood, S. Disposition, Metabolism and Mass Balance of Delafloxacin in Healthy Human Volunteers Following Intravenous Administration. Xenobiotica 2015, 45, 1054–1062. [Google Scholar] [CrossRef]
- European Medicines Agency. Quofenix (Delafloxacin): Summary of Product Characteristics; European Medicines Agency: Amsterdam, The Netherlands, 2019.
- Bassetti, M.; Pecori, D.; Cojutti, P.; Righi, E.; Pea, F. Clinical and Pharmacokinetic Drug Evaluation of Delafloxacin for the Treatment of Acute Bacterial Skin and Skin Structure Infections. Expert Opin. Drug Metab. Toxicol. 2017, 13, 1193–1200. [Google Scholar] [CrossRef][Green Version]
- Hoover, R.; Marbury, T.C.; Preston, R.A.; Quintas, M.; Lawrence, L.E.; Paulson, S.K.; Luke, D.R.; Cammarata, S.K. Clinical Pharmacology of Delafloxacin in Patients With Hepatic Impairment. J. Clin. Pharmacol. 2017, 57, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Righi, E.; Pecori, D.; Tillotson, G. Delafloxacin: An Improved Fluoroquinolone Developed through Advanced Molecular Engineering. Future Microbiol. 2018, 13, 1081–1094. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Sader, H.S.; Rhomberg, P.R.; Flamm, R.K. In Vitro Activity of Delafloxacin against Contemporary Bacterial Pathogens from the United States and Europe, 2014. Antimicrob. Agents Chemother. 2017, 61, e02609-16. [Google Scholar] [CrossRef] [PubMed]
- McCurdy, S.; Keedy, K.; Lawrence, L.; Nenninger, A.; Sheets, A.; Quintas, M.; Cammarata, S. Efficacy of Delafloxacin versus Moxifloxacin against Bacterial Respiratory Pathogens in Adults with Community-Acquired Bacterial Pneumonia (CABP): Microbiology Results from the Delafloxacin Phase 3 CABP Trial. Antimicrob. Agents Chemother. 2020, 64, e01949-19. [Google Scholar] [CrossRef]
- Flamm, R.K.; Rhomberg, P.R.; Huband, M.D.; Farrell, D.J. In Vitro Activity of Delafloxacin Tested against Isolates of Streptococcus Pneumoniae, Haemophilus Influenzae, and Moraxella Catarrhalis. Antimicrob. Agents Chemother. 2016, 60, 6381–6385. [Google Scholar] [CrossRef] [PubMed][Green Version]
- McCurdy, S.; Lawrence, L.; Quintas, M.; Woosley, L.; Flamm, R.; Tseng, C.; Cammarata, S. In Vitro Activity of Delafloxacin and Microbiological Response against Fluoroquinolone-Susceptible and Nonsusceptible Staphylococcus aureus Isolates from Two Phase 3 Studies of Acute Bacterial Skin and Skin Structure Infections. Antimicrob. Agents Chemother. 2017, 61, e00772-17. [Google Scholar] [CrossRef] [PubMed]
- Shortridge, D.; Pfaller, M.A.; Streit, J.M.; Flamm, R.K. Update on the Activity of Delafloxacin against Acute Bacterial Skin and Skin-Structure Infection Isolates from European Hospitals (2014–2019). J. Glob. Antimicrob. Resist. 2020, 23, 278–283. [Google Scholar] [CrossRef]
- Boyanova, L.; Yordanov, D.; Ouzounova-Raykova, V.; Markovska, R.; Marteva-Proevska, Y.; Mitov, I. Activity of Delafloxacin versus That of Levofloxacin against Anaerobic and Microaerophilic Isolates. Anaerobe 2020, 62, 102150. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Lamb, Y.N.; Shirley, M. Delafloxacin: A Review in Community-Acquired Pneumonia. Drugs 2022, 82, 913–923. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Flamm, R.K.; McCurdy, S.P.; Pillar, C.M.; Shortridge, D.; Jones, R.N. Delafloxacin In Vitro Broth Microdilution and Disk Diffusion Antimicrobial Susceptibility Testing Guidelines: Susceptibility Breakpoint Criteria and Quality Control Ranges for an Expanded-Spectrum Anionic Fluoroquinolone. J. Clin. Microbiol. 2018, 56, e00339-18. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Palatnick, L.; Nichol, K.A.; Bellyou, T.; Low, D.E.; Hoban, D.J. Antimicrobial Resistance in Respiratory Tract Streptococcus Pneumoniae Isolates: Results of the Canadian Respiratory Organism Susceptibility Study, 1997 to 2002. Antimicrob. Agents Chemother. 2003, 47, 1867–1874. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Zorrilla, S.; Sendra, E.; Horcajada, J.P. A Profile of Delafloxacin in the Treatment of Adults with Community-Acquired Bacterial Pneumonia. Expert Rev. Clin. Pharmacol. 2022, 15, 671–688. [Google Scholar] [CrossRef] [PubMed]
- Almer, L.S.; Hoffrage, J.B.; Keller, E.L.; Flamm, R.K.; Shortridge, V.D. In Vitro and Bactericidal Activities of ABT-492, a Novel Fluoroquinolone, against Gram-Positive and Gram-Negative Organisms. Antimicrob. Agents Chemother. 2004, 48, 2771–2777. [Google Scholar] [CrossRef]
- Saravolatz, L.D.; Pawlak, J.M.; Wegner, C. Delafloxacin Activity against Staphylococcus aureus with Reduced Susceptibility or Resistance to Methicillin, Vancomycin, Daptomycin or Linezolid. J. Antimicrob. Chemother. 2020, 75, 2605–2608. [Google Scholar] [CrossRef] [PubMed]
- Coustillères, F.; Renault, V.; Corvec, S.; Dupieux, C.; Simões, P.M.; Lartigue, M.F.; Plouzeau-Jayle, C.; Tande, D.; Lamoureux, C.; Lemarié, C.; et al. Clinical, Bacteriological, and Genetic Characterization of Bone and Joint Infections Involving Linezolid-Resistant Staphylococcus epidermidis: A Retrospective Multicenter Study in French Reference Centers. Microbiol. Spectr. 2023, 11, e0419022. [Google Scholar] [CrossRef]
- Siala, W.; Mingeot-Leclercq, M.-P.; Tulkens, P.M.; Hallin, M.; Denis, O.; Van Bambeke, F. Comparison of the Antibiotic Activities of Daptomycin, Vancomycin, and the Investigational Fluoroquinolone Delafloxacin against Biofilms from Staphylococcus aureus Clinical Isolates. Antimicrob. Agents Chemother. 2014, 58, 6385–6397. [Google Scholar] [CrossRef]
- Bauer, J.; Siala, W.; Tulkens, P.M.; Van Bambeke, F. A Combined Pharmacodynamic Quantitative and Qualitative Model Reveals the Potent Activity of Daptomycin and Delafloxacin against Staphylococcus aureus Biofilms. Antimicrob. Agents Chemother. 2013, 57, 2726–2737. [Google Scholar] [CrossRef]
- Cercenado, E.; Loras, C.; Cobos, A.; Sanz, J.C. In Vitro Activity of Delafloxacin against Highly Levofloxacin-Resistant Invasive Isolates of Streptococcus pneumoniae. Enfermedades Infecc. Microbiol. Clínica 2022, 40, 131–133. [Google Scholar] [CrossRef]
- Gerges, B.; Rolston, K.; Shelburne, S.A.; Rosenblatt, J.; Prince, R.; Raad, I. The in Vitro Activity of Delafloxacin and Comparator Agents against Bacterial Pathogens Isolated from Patients with Cancer. JAC Antimicrob. Resist. 2023, 5, dlad034. [Google Scholar] [CrossRef]
- Millar, B.C.; McCaughan, J.; Rendall, J.C.; Moore, J.E. Delafloxacin—A Novel Fluoroquinolone for the Treatment of Ciprofloxacin-resistant Pseudomonas Aeruginosa in Patients with Cystic Fibrosis. Clin. Respir. J. 2021, 15, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Farfour, E.; d’Epenoux, L.R.; Muggeo, A.; Alauzet, C.; Crémet, L.; Moussalih, S.; Roux, A.; de Verdière, S.C.; Bosphore, A.; Corvec, S.; et al. In Vitro Susceptibility of Nonfermenting Gram-Negative Rods to Meropenem-Vaborbactam and Delafloxacin. Future Microbiol. 2023, 18, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Brown Elliott, B.A.; Wallace, R.J. Comparison of In Vitro Susceptibility of Delafloxacin with Ciprofloxacin, Moxifloxacin, and Other Comparator Antimicrobials against Isolates of Nontuberculous Mycobacteria. Antimicrob. Agents Chemother. 2021, 65, e0007921. [Google Scholar] [CrossRef]
- Chew, K.L.; Octavia, S.; Go, J.; Yeoh, S.F.; Teo, J. MIC Distributions of Routinely Tested Antimicrobials and of Rifabutin, Eravacycline, Delafloxacin, Clofazimine, and Bedaquiline for Mycobacterium Fortuitum. Antimicrob. Agents Chemother. 2021, 65, e0059321. [Google Scholar] [CrossRef]
- McCurdy, S.; Halasohoris, S.A.; Babyak, A.L.; Lembirik, S.; Hoover, R.; Hickman, M.; Scarff, J.; Klimko, C.P.; Cote, C.K.; Meinig, J.M. Efficacy of Delafloxacin against the Biothreat Pathogen Bacillus Anthracis. J. Antimicrob. Chemother. 2023, 78, 810–816. [Google Scholar] [CrossRef]
- Waites, K.B.; Crabb, D.M.; Duffy, L.B. Comparative In Vitro Susceptibilities and Bactericidal Activities of Investigational Fluoroquinolone ABT-492 and Other Antimicrobial Agents against Human Mycoplasmas and Ureaplasmas. Antimicrob. Agents Chemother. 2003, 47, 3973–3975. [Google Scholar] [CrossRef]
- Harnett, S.J.; Fraise, A.P.; Andrews, J.M.; Jevons, G.; Brenwald, N.P.; Wise, R. Comparative Study of the in Vitro Activity of a New Fluoroquinolone, ABT-492. J. Antimicrob. Chemother. 2004, 53, 783–792. [Google Scholar] [CrossRef]
- Righi, E.; Carnelutti, A.; Vena, A.; Bassetti, M. Emerging Treatment Options for Acute Bacterial Skin and Skin Structure Infections: Focus on Intravenous Delafloxacin. Infect. Drug Resist. 2018, 11, 479–488. [Google Scholar] [CrossRef]
- Kong, Y.; Li, C.; Li, G.; Yang, T.; Draz, M.S.; Xie, X.; Zhang, J.; Ruan, Z. In Vitro Activity of Delafloxacin and Finafloxacin against Mycoplasma Hominis and Ureaplasma Species. Microbiol. Spectr. 2022, 10, e00099-22. [Google Scholar] [CrossRef] [PubMed]
- Dejoies, L.; Cattoir, V. Fluoroquinolones: Classification, activités antibactériennes, résistances et indications thérapeutiques. EMC-Mal. Infect. 2020, 37, 1–13. [Google Scholar]
- Penven, M.; Cattoir, V. Résistance bactérienne aux antibiotiques: Définitions, mécanismes et évolution. EMC-Mal. Infect. 2022, 0, 1–17. [Google Scholar]
- Aldred, K.J.; Kerns, R.J.; Osheroff, N. Mechanism of Quinolone Action and Resistance. Biochemistry 2014, 53, 1565–1574. [Google Scholar] [CrossRef] [PubMed]
- Bush, N.G.; Diez-Santos, I.; Abbott, L.R.; Maxwell, A. Quinolones: Mechanism, Lethality and Their Contributions to Antibiotic Resistance. Molecules 2020, 25, 5662. [Google Scholar] [CrossRef] [PubMed]
- Correia, S.; Poeta, P.; Hébraud, M.; Capelo, J.L.; Igrejas, G. Mechanisms of Quinolone Action and Resistance: Where Do We Stand? J. Med. Microbiol. 2017, 66, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Hooper, D.C.; Jacoby, G.A. Topoisomerase Inhibitors: Fluoroquinolone Mechanisms of Action and Resistance. Cold Spring Harb. Perspect. Med. 2016, 6, a025320. [Google Scholar] [CrossRef]
- Arsène, S.; Leclercq, R. Role of a Qnr-like Gene in the Intrinsic Resistance of Enterococcus Faecalis to Fluoroquinolones. Antimicrob. Agents Chemother. 2007, 51, 3254–3258. [Google Scholar] [CrossRef]
- Hooper, D.C. Mechanisms of Action of Antimicrobials: Focus on Fluoroquinolones. Clin. Infect. Dis. 2001, 32 (Suppl. S1), S9–S15. [Google Scholar] [CrossRef]
- Okumura, R.; Hirata, T.; Onodera, Y.; Hoshino, K.; Otani, T.; Yamamoto, T. Dual-Targeting Properties of the 3-Aminopyrrolidyl Quinolones, DC-159a and Sitafloxacin, against DNA Gyrase and Topoisomerase IV: Contribution to Reducing in Vitro Emergence of Quinolone-Resistant Streptococcus Pneumoniae. J. Antimicrob. Chemother. 2008, 62, 98–104. [Google Scholar] [CrossRef]
- Strahilevitz, J.; Hooper, D.C. Dual Targeting of Topoisomerase IV and Gyrase To Reduce Mutant Selection: Direct Testing of the Paradigm by Using WCK-1734, a New Fluoroquinolone, and Ciprofloxacin. Antimicrob. Agents Chemother. 2005, 49, 1949–1956. [Google Scholar] [CrossRef]
- Tow-Keogh, C.; McConnell, T.; Remy, J.; Dalton, J.; DeVito, J.A. Anti-MRSA Properties of Delafloxacin: Mutant Analysis and Characterization. Available online: www.melintamedicalinformation.com/Media/Publications/BAXDELA/ICAAC%202009/Rib-X_Delafloxacin_ICAAC-2009_C1-1363.pdf (accessed on 8 December 2021).
- Hermsen, E.D.; Hovde, L.B.; Konstantinides, G.N.; Rotschafer, J.C. Mutant Prevention Concentrations of ABT-492, Levofloxacin, Moxifloxacin, and Gatifloxacin against Three Common Respiratory Pathogens. Antimicrob. Agents Chemother. 2005, 49, 1633–1635. [Google Scholar] [CrossRef]
- Remy, J.M.; Marra, A.; Duffy, E. Bactericidal Activity of Delafloxacin against Recent Isolates of Staphylococcus aureus. In Proceedings of the ASM Microbe 2016, Boston, MA, USA, 16–20 June 2016. [Google Scholar]
- McCurdy, S.P.; Somprasong, N.; Schweizer, H.P. Evaluation of Delafloxacin against a Burkholderia Pseudomallei Efflux Mutant Panel. Microbiol. Spectr. 2022, 10, e0090322. [Google Scholar] [CrossRef] [PubMed]
- Thabit, A.K.; Crandon, J.L.; Nicolau, D.P. Pharmacodynamic and Pharmacokinetic Profiling of Delafloxacin in a Murine Lung Model against Community-Acquired Respiratory Tract Pathogens. Int. J. Antimicrob. Agents 2016, 48, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Lepak, A.J.; Andes, D.R. In Vivo Pharmacodynamic Target Assessment of Delafloxacin against Staphylococcus aureus, Streptococcus pneumoniae, and Klebsiella pneumoniae in a Murine Lung Infection Model. Antimicrob. Agents Chemother. 2016, 60, 4764–4769. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Lepak, A.J.; Marchillo, K.; Andes, D.R. In Vivo Pharmacodynamic Target Determination for Delafloxacin against Klebsiella Pneumoniae and Pseudomonas Aeruginosa in the Neutropenic Murine Pneumonia Model. Antimicrob. Agents Chemother. 2019, 63, e01131-19. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y. Treatment of Renal Abscesses Caused by Staphylococcus aureus MW2, Using Delafloxacin and Moxifloxacin. In Proceedings of the 21th European Congress of Clinical Microbiology and Infectious Diseases, Milan, Italy, 7–10 May 2011. [Google Scholar]
- O’Riordan, W.; Mehra, P.; Manos, P.; Kingsley, J.; Lawrence, L.; Cammarata, S. A Randomized Phase 2 Study Comparing Two Doses of Delafloxacin with Tigecycline in Adults with Complicated Skin and Skin-Structure Infections. Int. J. Infect. Dis. 2015, 30, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Kingsley, J.; Mehra, P.; Lawrence, L.E.; Henry, E.; Duffy, E.; Cammarata, S.K.; Pullman, J. A Randomized, Double-Blind, Phase 2 Study to Evaluate Subjective and Objective Outcomes in Patients with Acute Bacterial Skin and Skin Structure Infections Treated with Delafloxacin, Linezolid or Vancomycin. J. Antimicrob. Chemother. 2016, 71, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Giordano, P.A.; Pogue, J.M.; Cammarata, S. Analysis of Pooled Phase III Efficacy Data for Delafloxacin in Acute Bacterial Skin and Skin Structure Infections. Clin. Infect. Dis. 2019, 68, S223–S232. [Google Scholar] [CrossRef]
- Rusu, A.; Munteanu, A.-C.; Arbănași, E.-M.; Uivarosi, V. Overview of Side-Effects of Antibacterial Fluoroquinolones: New Drugs versus Old Drugs, a Step Forward in the Safety Profile? Pharmaceutics 2023, 15, 804. [Google Scholar] [CrossRef]
- Bassetti, M.; Hooper, D.; Tillotson, G. Analysis of Pooled Phase 3 Safety Data for Delafloxacin in Acute Bacterial Skin and Skin Structure Infections. Clin. Infect. Dis. 2019, 68, S233–S240. [Google Scholar] [CrossRef]
- Litwin, J.S.; Benedict, M.S.; Thorn, M.D.; Lawrence, L.E.; Cammarata, S.K.; Sun, E. A Thorough QT Study To Evaluate the Effects of Therapeutic and Supratherapeutic Doses of Delafloxacin on Cardiac Repolarization. Antimicrob. Agents Chemother. 2015, 59, 3469–3473. [Google Scholar] [CrossRef] [PubMed]
- Thabit, A.K.; Fatani, D.F.; Bamakhrama, M.S.; Barnawi, O.A.; Basudan, L.O.; Alhejaili, S.F. Antibiotic Penetration into Bone and Joints: An Updated Review. Int. J. Infect. Dis. 2019, 81, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Metallidis, S.; Topsis, D.; Nikolaidis, J.; Alexiadou, E.; Lazaraki, G.; Grovaris, L.; Theodoridou, A.; Nikolaidis, P. Penetration of Moxifloxacin and Levofloxacin into Cancellous and Cortical Bone in Patients Undergoing Total Hip Arthroplasty. J. Chemother. 2007, 19, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Naber, K.G.; Sorgel, F. Antibiotic Therapy—Rationale and Evidence for Optimal Drug Concentrations in Prostatic and Seminal Fluid and in Prostatic Tissue. Andrologia 2003, 35, 331–335. [Google Scholar] [CrossRef]
- Xiong, S.; Liu, X.; Deng, W.; Zhou, Z.; Li, Y.; Tu, Y.; Chen, L.; Wang, G.; Fu, B. Pharmacological Interventions for Bacterial Prostatitis. Front. Pharmacol. 2020, 11, 504. [Google Scholar] [CrossRef]
- Wagenlehner, F.M.E.; Kees, F.; Weidner, W.; Wagenlehner, C.; Naber, K.G. Concentrations of Moxifloxacin in Plasma and Urine, and Penetration into Prostatic Fluid and Ejaculate, Following Single Oral Administration of 400mg to Healthy Volunteers. Int. J. Antimicrob. Agents 2008, 31, 21–26. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Principal Pharmacokinetic Parameters of DLX | ||
|---|---|---|
| Tmax | 1 h (IV) | |
| 1–2.5 h (PO) | ||
| Vd | 35 L | |
| Oral bioavailability | 59% | |
| Protein binding | 84% | |
| Half-life | IV | PO |
| 10 h | 14 h | |
| Elimination | 66% (urines) | 50% (urines) |
| 28% (feces) | 48% (feces) | |
| Organism/Antimicrobial Agent | MIC50 (mg/L) | MIC90 (mg/L) | MIC Range (mg/L) |
|---|---|---|---|
| Staphylococcus aureus | |||
| Delafloxacin | ≤0.004 | 0.25 | ≤0.004–8 |
| Levofloxacin | 0.25 | >4 | ≤0.12–>4 |
| Moxifloxacin | ≤0.06 | 2 | ≤0.06–>4 |
| Ciprofloxacin | 64 | >128 | 64–>128 |
| MSSA | |||
| Delafloxacin | ≤0.004 | 0.008 | ≤0.004–4 |
| Levofloxacin | 0.25 | 0.25 | ≤0.12–>4 |
| Moxifloxacin | ≤0.06 | ≤0.06 | ≤0.06–>4 |
| Ciprofloxacin | >128 | >128 | >128 |
| MRSA | |||
| Delafloxacin | 0.06–0.25 | 0.25–1 | |
| Levofloxacin | 4 | >4 | |
| Moxifloxacin | 2 | >4 | |
| Levofloxacin-susceptible S. aureus | |||
| Delafloxacin | 0.008 | 0.008 | 0.002–0.12 |
| Levofloxacin-resistant S. aureus | |||
| Delafloxacin | 0.25 | 0.25–1 | 0.004–4 |
| Moxifloxacin | 2 | 8 | |
| CoNS | |||
| Delafloxacin | ≤0.004 | 0.06 | ≤0.004–1 |
| Levofloxacin | 0.25 | 4 | ≤0.12–> 4 |
| MR-CoNS | |||
| Delafloxacin | 0.06 | 0.5 | ≤0.004–2 |
| Levofloxacin | 4 | >4 | ≤0.12–>4 |
| Levofloxacin-susceptible CoNS | |||
| Delafloxacin | ≤0.004 | 0.06 | ≤0.004–1 |
| Levofloxacin | 0.25 | 4 | ≤0.12–> 4 |
| Levofloxacin-resistant CoNS | |||
| Delafloxacin | 0.06 | 0.5 | ≤0.004–2 |
| Levofloxacin | 4 | >4 | ≤0.12–>4 |
| Streptococcus spp. | |||
| Delafloxacin | 0.016 | 0.03 | |
| Levofloxacin | 0.5 | 1 | |
| Moxifloxacin | ≤0.012 | 0.25 | |
| Viridans group streptococci | |||
| Delafloxacin | 0.016 | 0.03 | ≤0.004–2 |
| Levofloxacin | 1 | 2 | ≤0.12–>4 |
| Moxifloxacin | ≤0.012 | 0.25 | ≤0.12–>4 |
| Streptococcus pyogenes | |||
| Delafloxacin | 0.008 | 0.03 | ≤0.004–0.06 |
| Levofloxacin | 0.5 | 1 | 0.12–4 |
| Moxifloxacin | ≤0.012 | 0.25 | ≤0.012–2 |
| Streptococcus agalactiae | |||
| Delafloxacin | 0.008–0.016 | 0.016–0.03 | 0.004–1 |
| Levofloxacin | 0.5 | 1 | 0.5–>4 |
| Moxifloxacin | ≤0.012 | 0.25 | ≤0.012–4 |
| Streptococcus dysgalactiae | |||
| Delafloxacin | 0.008 | 0.016 | ≤0.004–0.12 |
| Levofloxacin | 0.5 | 1 | 0.12–>4 |
| Moxifloxacin | ≤0.012 | 0.25 | ≤0.012–2 |
| Streptococcus pneumoniae | |||
| Delafloxacin | 0.008 | 0.016 | ≤0.004–0.5 |
| Levofloxacin | 1 | 1 | 0.5–>4 |
| Moxifloxacin | ≤0.012 | 0.25 | ≤0.12–>4 |
| Levofloxacin-resistant S. pneumoniae | |||
| Delafloxacin | 0.12 | 0.5 | 0.016–1 |
| Levofloxacin | >4 | >4 | >4 |
| Moxifloxacin | 2 | 4 | 0.25–>4 |
| Enterococcus faecalis | |||
| Delafloxacin | 0.06–0.12 | 1 | ≤0.004–2 |
| Levofloxacin | 1 | >4 | 0.25–>4 |
| Levofloxacin-resistant E. faecalis | |||
| Delafloxacin | 1 | 2 | 0.06–2 |
| Enterococcus faecium | |||
| Delafloxacin | >4 | >4 | 0.008–>4 |
| Levofloxacin | >4 | >4 | 0.5–4 |
| Organism/Antimicrobial Agent | MIC50 (mg/L) | MIC90 (mg/L) | MIC Range (mg/L) |
|---|---|---|---|
| Enterobacterales | |||
| Delafloxacin | 0.06 | 4 | ≤0.004–>4 |
| Levofloxacin | ≤0.12 | >4 | ≤0.12–>4 |
| Ciprofloxacin | ≤0.03 | >4 | ≤0.03–>4 |
| Escherichia coli | |||
| Delafloxacin | 0.03 | 4 | ≤0.004–>4 |
| Levofloxacin | ≤0.12 | >4 | ≤0.12–>4 |
| Ciprofloxacin | ≤0.03 | >4 | ≤0.25–>4 |
| Moxifloxacin | ≤0.25 | >4 | ≤0.03–>4 |
| ESBL-producing E. coli | |||
| Delafloxacin | 2 | >4 | 0.008–>4 |
| Levofloxacin | >4 | >4 | ≤0.12–>4 |
| Ciprofloxacin | >4 | >4 | ≤0.03–>4 |
| Klebsiella pneumoniae | |||
| Delafloxacin | 0.06 | >4 | 0.016–>4 |
| Levofloxacin | ≤0.12 | >4 | ≤0.12–>4 |
| Ciprofloxacin | ≤0.03 | >4 | |
| ESBL-producing K. pneumonia | |||
| Delafloxacin | 4 | >4 | 0.06–>4 |
| Levofloxacin | >4 | >4 | ≤0.12–>4 |
| Ciprofloxacin | >4 | >4 | ≤0.03–>4 |
| Klebsiella oxytoca | |||
| Delafloxacin | 0.06 | 0.12 | 0.03–1 |
| Levofloxacin | ≤0.12 | ≤0.12 | ≤0.12–1 |
| Ciprofloxacin | ≤0.03 | 0.06 | ≤0.03–4 |
| Proteus mirabilis | |||
| Delafloxacin | 0.06 | 2 | 0.016–>4 |
| Levofloxacin | ≤0.12 | >4 | ≤0.12–>4 |
| Ciprofloxacin | ≤0.03 | >4 | ≤0.03–>4 |
| Enterobacter spp. | |||
| Delafloxacin | 0.06 | 1 | ≤0.004–>4 |
| Levofloxacin | ≤0.12 | 0.5 | ≤0.12–>4 |
| Ciprofloxacin | ≤0.03 | 0.25 | ≤0.03–>4 |
| Citrobacter spp. | |||
| Delafloxacin | 0.06 | 2 | 0.008–>4 |
| Levofloxacin | ≤0.12 | 0.5 | ≤0.12–>4 |
| Ciprofloxacin | ≤0.03 | 0.5 | ≤0.03–>4 |
| Proteus spp. | |||
| Delafloxacin | 0.12 | 4 | 0.008–>4 |
| Levofloxacin | ≤0.12 | >4 | ≤0.12–>4 |
| Ciprofloxacin | ≤0.03 | >4 | ≤0.03–>4 |
| Serratia spp. | |||
| Delafloxacin | 1 | 2 | 0.03–>4 |
| Levofloxacin | ≤0.12 | 1 | ≤0.12–>4 |
| Ciprofloxacin | 0.12 | 1 | ≤0.03–>4 |
| Pseudomonas aeruginosa | |||
| Delafloxacin | 0.25–0.5 | >4 | 0.016–>4 |
| Levofloxacin | 0.5 | >4 | ≤0.12–>4 |
| Ciprofloxacin | 0.25 | >4 | ≤0.03–>4 |
| Haemophilus influenzae | |||
| Delafloxacin | ≤0.001 | 0.004 | ≤0.001–0.25 |
| Levofloxacin | 0.016 | 0.016 | 0.004–>2 |
| Ciprofloxacin | 0.016 | 0.03 | 0.008–>2 |
| Moraxella catarrhalis | |||
| Delafloxacin | 0.008 | 0.008 | 0.004–0.016 |
| Levofloxacin | 0.06 | 0.06 | 0.03–0.12 |
| Ciprofloxacin | 0.03 | 0.06 | 0.016–0.06 |
| Acinetobacter baumannii | |||
| Delafloxacin | 2 | >4 | 0.015–>4 |
| Levofloxacin | >4 | >4 | ≤0.012–>4 |
| Ciprofloxacin | >4 | >4 | 0.06–>4 |
| Neisseria gonorrhoeae | |||
| Delafloxacin | 0.06 | 0.125 | ≤0.001–0.25 |
| Ciprofloxacin | 4 | 16 | 0.004–≥16 |
| Phase II Studies in ABSSIs | ||||||||
|---|---|---|---|---|---|---|---|---|
| Studies | Design | Population Size | Delafloxacin Group | Comparators Group | Duration | Monitoring | Evaluation Criteria | Results |
| O’Riordan et al., 2015 [89] | Multicenter, randomized (1:1:1), double-blind, non-inferiority | 150 | 300 mg (IV), 2/24 h or 450 mg (IV), 2/24 h | Tigecycline (IV) 100 mg on day 1, then 50 mg, 2/24 h | 5–14 days | 14–21 days after last dose (TOC) | Primary efficacy clinical endpoint: clinical response Microbiological endpoint of eradication: documented eradicated, presumed eradicated, documented persisted, presumed persisted, superinfection, new infection | Primary efficacy endpoint: rate of cure at TOC: DLX 300 mg (94.3%), DLX 450 mg (92.5%), and TGC (91.2%) No difference between the three groups Microbiological endpoint of eradication at FU: No difference between the three groups |
| Kingsley et al., 2016 [90] | Multicenter, randomized (1:1:1), double blind, non-inferiority | 256 | 300 mg (IV), 2/24 h | Vancomycin 15 mg/kg (IV), 2/24 h or Linezolid 600 mg (IV), 2/24 h | 5–14 days | 5 days after inclusion 14 days after inclusion(FU) | Primary efficacy clinical endpoint: investigator assessment of clinical response at FU defined patient as “cure”, “improved”, “failure”, or “indeterminate” Microbiological endpoint of eradication: documented eradicated, presumed eradicated, documented persisted, presumed persisted, superinfection, new infection | Primary efficacy endpoint: rate of cure at FU DLX (70.4%), LZD (64.9%) and VNC (54.1%) DLX significantly greater than VNC No difference between DLX and LZD Microbiological endpoint of eradication at FU: No difference between the three groups |
| Phase III Studies in ABSSIs | |||||||
|---|---|---|---|---|---|---|---|
| Studies | Design | Population Size | Delafloxacin Group | Comparators Group | Duration | Monitoring | Evaluation Criteria |
| Pullman et al., 2017 [2] | Multicenter, randomized (1:1), double-blind, non-inferiority | 660 | 300 mg (IV), 2/24 h | Vancomycin 15 mg/kg (IV), 2/24 h and aztreonam 1–2 g (stopped if no Gram-negatives found) | 5–14 days | 48–72 h after first dose Day 14 (FU) Days 21–28 (LFU) | Primary efficacy endpoint defined by FDA: objective response at 48–72 h Primary efficacy endpoint defined by EMA: investigator assessment of clinical response at the FU Secondary efficacy endpoint defined by EMA: investigator-assessed success at FU Microbiological endpoint of eradication at FU |
| O’Riordan et al., 2018 [3] | Multicenter, randomized (1:1), double-blind, non-inferiority | 850 | 300 mg (IV), 2/24 h with relay by 450 mg (PO) | Vancomycin 15 mg/kg (IV), 2/24 h and aztreonam 1–2 g (stopped if no Gram-negatives found) | 5–14 days | 48–72 h after first dose Day 14 (FU) Days 21–28 (LFU) | Primary efficacy endpoint defined by FDA: objective response at 48–72 h Primary efficacy endpoint defined by EMA: investigator assessment of clinical response at the FU Secondary efficacy endpoint defined by EMA: investigator-assessed success at FU Microbiological endpoint of eradication at FU |
| Phase III Studies in ABSSIs | ||||||
|---|---|---|---|---|---|---|
| Studies | Subgroup | DLX (Events/Total) | % | VNC + AZT (Events/Total) | % | Percentage Difference (CI 95%) |
| Pullman et al., 2017 [2] | ITT | |||||
| Objective response at 48–72 h a | 259/331 | 78.2 | 266/329 | 80.9 | –2.6 (–8.78, 3.57) | |
| Investigator-assessed cure at FU b | 172/331 | 52 | 166/329 | 50.5 | 1.5 (–6.11, 9.11) | |
| Investigator-assessed success at FU c | 270/331 | 81.6 | 274/329 | 83.3 | –1.7 (–7.55, 4.13) | |
| Investigator-assessed cure at LFU | 233/331 | 70.4 | 219/329 | 66.6 | 3.8 (–3.27, 10.89) | |
| Investigator-assessed success at LFU | 265/331 | 80.1 | 267/329 | 81.2 | –1.1 (–7.15, 4.97) | |
| CE | ||||||
| Objective response at 48–72 h a | 250/294 | 85 | 257/297 | 86.5 | –1.5 (–7.20, 4.18) | |
| Investigator-assessed cure at FU b | 142/240 | 59.2 | 142/244 | 58.2 | 1.0 (–7.79, 9.71) | |
| Investigator-assessed success at FU c | 233/240 | 97.1 | 238/244 | 97.5 | –0.5 (–3.75, 2.72) | |
| Investigator-assessed cure at LFU | 208/245 | 84.9 | 201/244 | 82.4 | 2.5 (–4.08, 9.15) | |
| Investigator-assessed success at LFU | 237/245 | 96.7 | 241/244 | 98.8 | –2.1 (–5.24, 0.70) | |
| O’Riordan et al., 2018 [3] | ITT | |||||
| Objective response at 48–72 h a | 354/423 | 83.7 | 344/427 | 80.6 | 3.1 (−2.0, 8.3) | |
| Investigator-assessed cure at FU b | 244/423 | 57.7 | 255/27 | 59.7 | −2.0 (−8.6, 4.6) | |
| Investigator-assessed success at FU c | 369/423 | 87.2 | 362/427 | 84.4 | 2.5 (−2.2, 7.2) | |
| Investigator-assessed cure at LFU | 287/423 | 67.8 | 303/427 | 71.0 | −3.1 (−9.3, 3.1) | |
| Investigator-assessed success at LFU | 353/423 | 83.5 | 351/427 | 82.2 | 1.3 (−3.8, 6.3) | |
| CE | ||||||
| Objective response at 48–72 h a | 346/395 | 87.6 | 327/387 | 84.5 | 3.1 (1.8, 8.0) | |
| Investigator-assessed cure at FU b | 220/353 | 62.3 | 224/329 | 68.1 | −5.8 (−12.9, 1.4) | |
| Investigator-assessed success at FU c | 340/353 | 96.3 | 319/329 | 97.0 | −0.6 (−3.5, 2.2) | |
| Investigator-assessed cure at LFU | 259/337 | 76.9 | 267/323 | 82.7 | −5.8 (−11.9, 0.3) | |
| Investigator-assessed success at LFU | 322/337 | 95.5 | 310/323 | 96.0 | −0.4 (−3.7, 2.8) | |
| Phase III Studies | ||||||||
| Studies | Design | Population Size | DLX Group | Comparators Group | Duration | Monitoring | Evaluation Criteria | Results |
| CABP, Horcajada et al., 2020 [5] | Multicenter, randomized (1:1), double-blind, non-inferiority | 859 | 300 mg (IV), 2/24 h with PO relay (450 mg) after 6 doses | MXF 400 mg, 1/24 h PO relay was conducted. If MRSA was found, a relay for linezolid 600 mg IV was conducted | 5–10 days | Early clinical response (ECR) at 96 h after first dose 5–10 days after end of treatment (TOC) Day 28 (FU) | Primary efficacy endpoint defined by FDA: early clinical response at 96 h: defined patients as responder to treatment or not Secondary efficacy endpoint defined by FDA: ECR in addition of improvement in vital signs Microbiological endpoint of eradication at TOC | Primary efficacy endpoint defined by FDA: DLX (88.9%), MXF (89%). No difference between both groups Secondary efficacy endpoint defined by FDA: DLX (52.7%), MXF (43%). Significant improvement in DLX groups Microbiological endpoint of eradication at TOC: No difference between both groups |
| Uncomplicated gonorrhea, Hook et al., 2019 [4] | Multicenter, randomized (2:1), open-label, non-inferiority | 460 | 900 mg PO, single dose | CTX 250 mg, intramuscular, single dose | Single dose | Visit at 7 ± 3 days (TOC) | Primary efficacy endpoint defined by FDA: microbiological outcomes: cure or failure | Primary efficacy endpoint defined by FDA: DLX (85.1%), CTX (91%). DLX did not show non-inferiority versus CTX |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turban, A.; Guérin, F.; Dinh, A.; Cattoir, V. Updated Review on Clinically-Relevant Properties of Delafloxacin. Antibiotics 2023, 12, 1241. https://doi.org/10.3390/antibiotics12081241
Turban A, Guérin F, Dinh A, Cattoir V. Updated Review on Clinically-Relevant Properties of Delafloxacin. Antibiotics. 2023; 12(8):1241. https://doi.org/10.3390/antibiotics12081241
Chicago/Turabian StyleTurban, Adrien, François Guérin, Aurélien Dinh, and Vincent Cattoir. 2023. "Updated Review on Clinically-Relevant Properties of Delafloxacin" Antibiotics 12, no. 8: 1241. https://doi.org/10.3390/antibiotics12081241
APA StyleTurban, A., Guérin, F., Dinh, A., & Cattoir, V. (2023). Updated Review on Clinically-Relevant Properties of Delafloxacin. Antibiotics, 12(8), 1241. https://doi.org/10.3390/antibiotics12081241