
Similarity Analysis of Klebsiella pneumoniae Producing Carbapenemases Isolated from UTI and Other Infections
 ,
,  , , , , , and
, , , , , and
Abstract
1. Introduction
2. Results
2.1. K. pneumoniae Isolation Sites
2.2. Drug Susceptibility
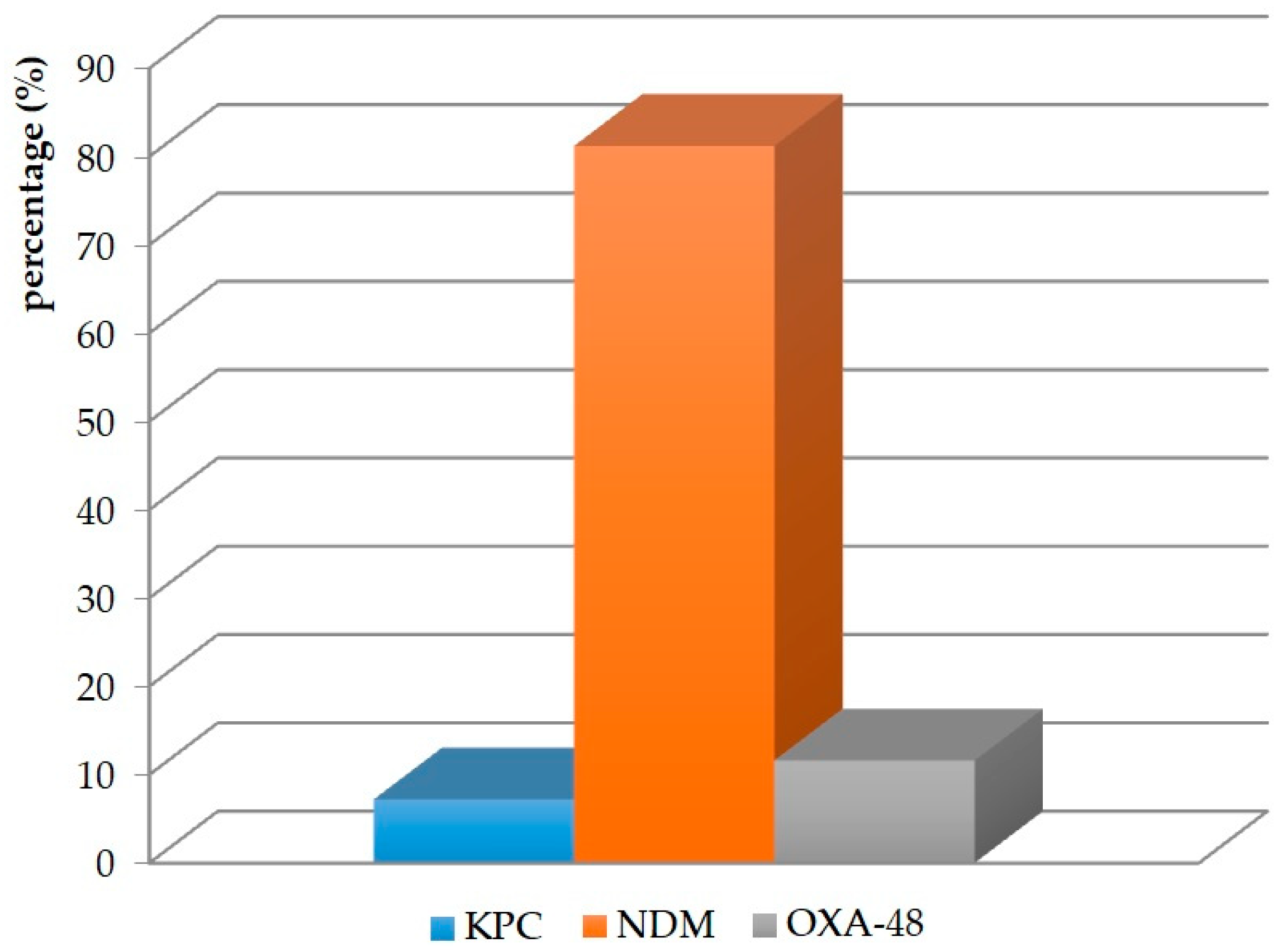
2.3. Production of Carbapenemases
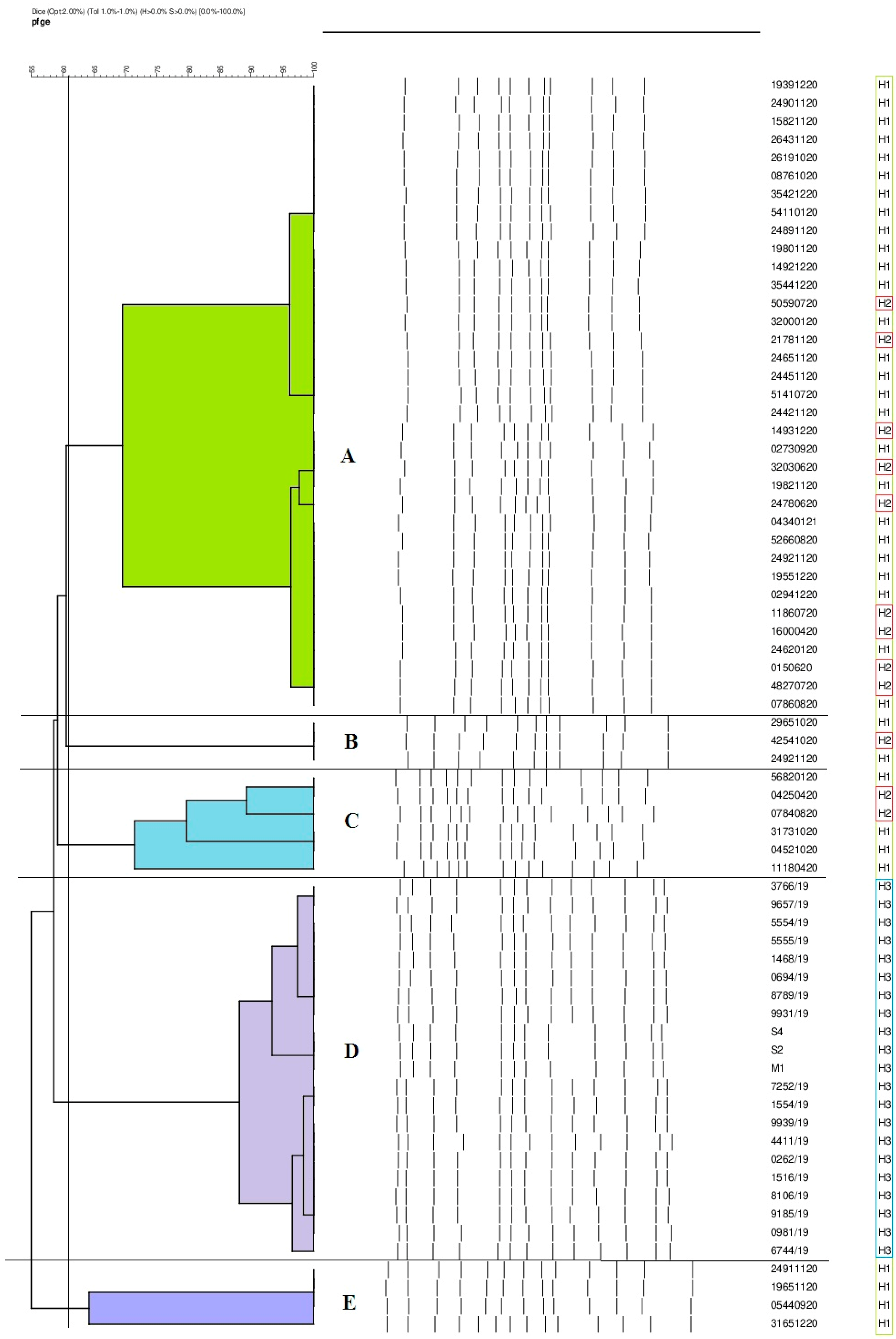
2.4. Phylogenetic Similarity of K. pneumoniae Strains
3. Discussion
4. Materials and Methods
4.1. Bacterial Strains
4.2. Identification and Determination of Drug Susceptibility
4.3. Determination of Carbapenemases
4.4. Determination of Phylogenetic Similarity of K. pneumoniae Strains by PFGE Method
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Austrian, R. Pneumococcus: The First One Hundred Years. Rev. Infect. Dis. 1981, 3, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.; Wu, S.; Hao, M.; Zhu, J.; Ding, B.; Yang, Y. The colonization of carbapenem-resistant Klebsiella pneumoniae. J. Infect. Dis. 2020, 221, 206–214. [Google Scholar] [CrossRef]
- Gomez-Simmonds, A.; Uhlemann, A.C. Clinical implications of genomic adaptation and evolution of carbapenem-resistant Klebsiella pneumoniae. J. Infect. Dis. 2017, 215, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Snitkin, E.S.; Zelazny, A.M.; Thomas, P.J.; Stock, F. Tracking a hospital outbreak of carbapenem-resistant Klebsiella pneumoniae with whole-genome sequencing. Sci. Transl. Med. 2012, 4, 148ra116. [Google Scholar] [CrossRef] [PubMed]
- Czekaj, T.; Ciszewski, M. Klebsiella pneumoniae NDM—New emerging superbacteria. Medycynarodzinna 2015, 1, 23–27. [Google Scholar]
- Paczosa, M.K.; Mecsas, J. Klebsiella pneumoniae: Going on the offense with a strong defense. Microbiol. Mol. Biol. Rev. 2016, 80, 629–661. [Google Scholar] [CrossRef]
- Moradigaravand, D.; Martin, V.; Peacock, S.J.; Parkhill, J. Evolution and epidemiology of multidrug-resistant Klebsiella pneumoniae in the United Kingdom and Ireland. mBio 2017, 8, e01976-16. [Google Scholar] [CrossRef]
- Gupta, A. Hospital-acquired infections in the neonatal intensive care unit-Klebsiella pneumoniae. Semin. Perinatol. 2002, 26, 340–345. [Google Scholar] [CrossRef]
- David, S.; Reuter, S.; Harris, S.R. Epidemic of carbapenem-resistant Klebsiella pneumoniae in Europe is driven by nosocomial spread. Nat. Microbiol. 2019, 4, 1919–1929. [Google Scholar] [CrossRef]
- Del Prete, R.; Ronga, L.; Addati, G.; Magrone, R.; Abbasciano, A.; Decimo, M. Trends in Klebsiella pneumoniae strains isolated from the bloodstream in a teaching hospital in southern Italy. Infez. Med. 2019, 27, 17–25. [Google Scholar]
- Politi, L.; Gartzonika, K.; Spanakis, N.; Zarkotou, O.; Poulou, A.; Skoura, L.; Vrioni, G.; Tsakris, A. Emergence of NDM-1-producing Klebsiella pneumoniae in Greece: Evidence of a widespread clonal outbreak. J. Antimicrob. Chemother. 2019, 74, 2197–2202. [Google Scholar] [CrossRef]
- Aires-de-Sousa, M.; Ortiz de la Rosa, J.M.; Gonçalves, M.L.; Pereira, A.L.; Nordmann, P.; Poirel, L. Epidemiology of carbapenemase-producing Klebsiella pneumoniae in a hospital, Portugal. Emerg. Infect. Dis. 2019, 25, 1632–1638. [Google Scholar] [CrossRef]
- Khairy, R.M.M.; Mahmoud, M.S.; Shady, R.R.; Esmail, M.A.M. Multidrug resistant Klebsiella pneumoniae in hospital-acquired infections: Concomitant analysis of antimicrobial resistant strains. Int. J. Clin. Pract. 2019, 74, 13463. [Google Scholar] [CrossRef]
- Hawken, S.E.; Snitkin, E.S. Genomic epidemiology of multidrug-resistant Gram-negative organisms. Ann. N. Y. Acad. Sci. 2019, 1435, 39–56. [Google Scholar] [CrossRef]
- Campos, A.C.; Albiero, J.; Ecker, A.B.; Kuroda, C.M.; Meirelles, L.E.F.; Polato, A. Outbreak of Klebsiella pneumoniae carbapenemase–producing K. pneumoniae: A systematic review. Am. J. Infect. Control 2016, 44, 1374–1380. [Google Scholar] [CrossRef]
- Li, Y.; Shen, H.; Zhu, C.; Yu, Y. Carbapenem-resistant Klebsiella pneumoniae infections among ICU admission patients in Central China: Prevalence and prediction model. Biomed. Res. Int. 2019, 2019, 9767313. [Google Scholar] [CrossRef]
- Santajit, S.; Indrawattana, N. Mechanisms of antimicrobial resistance in ESKAPE Pathogens. Biomed. Res. Int. 2016, 2016, 2475067. [Google Scholar] [CrossRef]
- Yang, X.; Dong, N.; Wai-Chi Chan, E.; Zhang, R.; Chen, S. Carbapenem resistance-encoding and virulence-encoding conjugative plasmids in Klebsiella pneumoniae. Trends Microbiol. 2021, 29, 65–83. [Google Scholar] [CrossRef]
- Gao, H.; Liu, Y.; Wang, R.; Wang, Q.; Jin, L.; Wang, H. The transferability and evolution of NDM-1 and KPC-2 co-producing Klebsiella pneumoniae from clinical settings. EBioMedicine 2020, 51, 102599. [Google Scholar] [CrossRef]
- Apondi, O.E.; Oduor, O.C.; Gye, B.K.; Kipkoech, M.K. High prevalence of multi-drug resistant Klebsiella pneumoniae in tertiary teaching hospital in western Kenya. Afr. J. Infect. Dis. 2016, 10, 89–95. [Google Scholar] [CrossRef]
- Durdu, B.; Koc, M.M.; Hakyemez, I.N.; Akkoyunlu, Y.; Daskaya, H.; Gultepe, B.S.; Aslan, T. Risk factors affecting patterns of antibiotic resistance and treatment efficacy in extreme drug resistance in intensive care unit-acquired Klebsiella pneumoniae infections: A 5-year analysis. Med. Sci. Monit. 2019, 25, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.K.; Mishra, M.; Sahoo, M.; Patole, S.; Sahu, S.; Misra, S.R. Antibiotic resistance determinants and clonal relationships among multidrug-resistant isolates of Klebsiella pneumoniae. Microb. Pathog. 2017, 110, 31–36. [Google Scholar] [CrossRef]
- Zheng, B.; Dai, Y.; Liu, Y.; Shi, W.; Dai, E.; Han, Y.; Zheng, D.; Yu, Y.; Li, M. Molecular epidemiology and risk factors of carbapenem-resistant Klebsiella pneumoniae infections in Eastern China. Front. Microbiol. 2017, 8, 1061. [Google Scholar] [CrossRef] [PubMed]
- Yonekawa, S.; Mizuno, T.; Nakano, R.; Nakano, A.; Suzuki, Y.; Asada, T.; Ishii, A.; Kakuta, N.; Tsubaki, K.; Mizuno, S.; et al. Molecular and epidemiological characteristics of carbapenemase-producing Klebsiella pneumoniae clinical isolates in Japan. mSphere 2020, 5, e00490-20. [Google Scholar] [CrossRef]
- Suay-García, B.; Pérez-Gracia, M.T. Present and future of carbapenem-resistant Enterobacteriaceae (CRE) infections. Antibiotics 2019, 8, 122. [Google Scholar] [CrossRef] [PubMed]
- Logan, L.K.; Weinstein, R.A. The Epidemiology of carbapenem-resistant Enterobacteriaceae: The impact and evolution of a global menace. J. Infect. Dis. 2017, 215, 28–36. [Google Scholar] [CrossRef]
- Han, R.; Shi, Q.; Wu, S.; Yin, D.; Peng, M.; Dong, D.; Zheng, Y. Dissemination of carbapenemases (KPC, NDM, OXA-48, IMP, and VIM) among carbapenem-resistant Enterobacteriaceae isolated from adult and children patients in China. Front. Cell Infect. Microbiol. 2020, 3, 314. [Google Scholar] [CrossRef]
- Kazi, M.; Drego, L.; Nikam, C. Molecular characterization of carbapenem-resistant Enterobacteriaceae at a tertiary care laboratory in Mumbai. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 467–472. [Google Scholar] [CrossRef]
- Lopes, E.; Saavedra, M.J.; Costa, E.; de Lencastre, H.; Poirel, L.; Aires-de-Sousa, M. Epidemiology of carbapenemase-producing Klebsiella pneumoniae in northern Portugal: Predominance of KPC-2 and OXA-48. J. Glob. Antimicrob. Resist. 2020, 2, 349–353. [Google Scholar] [CrossRef]
- Ojdana, D.; Sacha, P.T.; Gutowska, A.; Majewski, P.; Wieczorek, P.; Tryniszewska, E.A. Antibiotic resistance profiles of KPC and NDM carbapenemases-producing Klebsiella pneumoniae. Zakażenia XXI Wieku 2019, 2, 131–137. [Google Scholar] [CrossRef]
- Albiger, B.; Glasner Struelens, M.J.; Grundmann, H.; Monnet, D.L. Carbapenemase-producing Enterobacteriaceae in Europe: Assessment by national experts from 38 countries. Eurosurveillance 2015, 20, 30062. [Google Scholar] [CrossRef]
- Navon-Venezia, S.; Kondratyeva, K.; Carattoli, A. Klebsiella pneumoniae: A major worldwide source and shuttle for antibiotic resistance. FEMS Microbiol. Rev. 2017, 41, 252–275. [Google Scholar] [CrossRef]
- Lixandru, B.E.; Cotar, A.I.; Straut, M. Carbapenemase-producing Klebsiella pneumoniae in Romania: A six-month survey. PLoS ONE 2015, 10, 0143214. [Google Scholar] [CrossRef]
- Wang, Z.; Li, M.; Shen, X.; Wang, L.; Liu, L.; Hao, Z. Outbreak of blaNDM-5-harboring Klebsiella pneumoniae ST290 in a tertiary hospital in China. Mary Ann. Libert. 2019, 25, 1443–1448. [Google Scholar] [CrossRef]
- Kong, Z.; Cai, R.; Cheng, C.; Zhang, C.; Kang, H.; Ma, P. First reported nosocomial outbreak of NDM-5-producing Klebsiella pneumoniae in a neonatal unit in China. Infect. Drug Resist. 2019, 12, 3557–3566. [Google Scholar] [CrossRef]
- Mansour, W.; Haenni, M.; Saras, E.; Grami, R.; Mani, Y.; Khalifa, A.B.H.; El Atrouss, S.; Kheder, M.; Hassen, M.F.; Boujâafar, N.; et al. Outbreak of colistin-resistant carbapenemase-producing Klebsiella pneumoniae in Tunisia. J. Glob. Antimicrob. Resist. 2017, 10, 88–94. [Google Scholar] [CrossRef]
- Duman, Y.; Ersoy, Y.; Gursoy, N.C.; AltunisikToplu, S.; Otlu, B. A silent outbreak due to Klebsiella pneumoniae that co-produced NDM-1 and OXA-48 carbapenemases, and infection control measures. Iran J. Basic Med. Sci. 2020, 23, 46–50. [Google Scholar]
- Chen, D.; Hu, X.; Chen, F.; Li, H.; Wang, D.; Li, X. Co-outbreak of multidrug resistance and a novel ST3006 Klebsiella pneumoniae in a neonatal intensive care unit: A retrospective study. Medicine 2019, 98, 14285. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing: Breakpoints Tables for Interpretation of MICs and Zone Diameters. Version 11.0. Available online: http.//www.eucast.org (accessed on 1 January 2021).



{kind=link}
{kind=link}
| Antibiotic | Antibiotic Concentration [µg] | Susceptible n (%) | Resistant n (%) |
|---|---|---|---|
| Amoxicillin with clavulanic acid | 20/10 | 0 (0) | 69 (100) |
| Piperacillin/tazobactam | 100/10 | 0 (0) | 69 (100) |
| Cefotaxime | 30 | 0 (0) | 69 (100) |
| Cefepime | 30 | 0 (0) | 69 (100) |
| Gentamicin | 10 | 12 (17.4) | 57 (82.6) |
| Amikacin | 30 | 32 (46.4) | 37 (53.6) |
| Ciprofloxacin | 5 | 0 (0) | 69 (100) |
| Imipenem | 10 | 2 (2.9) | 67 (97.1) |
| Meropenem | 10 | 1 (1.5) | 68 (98.5) |
| Genotype | Number of Strains n = 69 | Hospital |
|---|---|---|
| A | 35 | H1 (25), H2 (10) |
| B | 3 | H1 (2), H2 (1) |
| C | 6 | H1 (4), H2 (2) |
| D | 21 | H3 |
| E | 4 | H1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pruss, A.; Kwiatkowski, P.; Sienkiewicz, M.; Masiuk, H.; Łapińska, A.; Kot, B.; Kilczewska, Z.; Giedrys-Kalemba, S.; Dołęgowska, B. Similarity Analysis of Klebsiella pneumoniae Producing Carbapenemases Isolated from UTI and Other Infections. Antibiotics 2023, 12, 1224. https://doi.org/10.3390/antibiotics12071224
Pruss A, Kwiatkowski P, Sienkiewicz M, Masiuk H, Łapińska A, Kot B, Kilczewska Z, Giedrys-Kalemba S, Dołęgowska B. Similarity Analysis of Klebsiella pneumoniae Producing Carbapenemases Isolated from UTI and Other Infections. Antibiotics. 2023; 12(7):1224. https://doi.org/10.3390/antibiotics12071224
Chicago/Turabian StylePruss, Agata, Paweł Kwiatkowski, Monika Sienkiewicz, Helena Masiuk, Agnieszka Łapińska, Barbara Kot, Zuzanna Kilczewska, Stefania Giedrys-Kalemba, and Barbara Dołęgowska. 2023. "Similarity Analysis of Klebsiella pneumoniae Producing Carbapenemases Isolated from UTI and Other Infections" Antibiotics 12, no. 7: 1224. https://doi.org/10.3390/antibiotics12071224
APA StylePruss, A., Kwiatkowski, P., Sienkiewicz, M., Masiuk, H., Łapińska, A., Kot, B., Kilczewska, Z., Giedrys-Kalemba, S., & Dołęgowska, B. (2023). Similarity Analysis of Klebsiella pneumoniae Producing Carbapenemases Isolated from UTI and Other Infections. Antibiotics, 12(7), 1224. https://doi.org/10.3390/antibiotics12071224