


Trichosporon asahii Infective Endocarditis of Prosthetic Valve: A Case Report and Literature Review


Abstract
1. Introduction
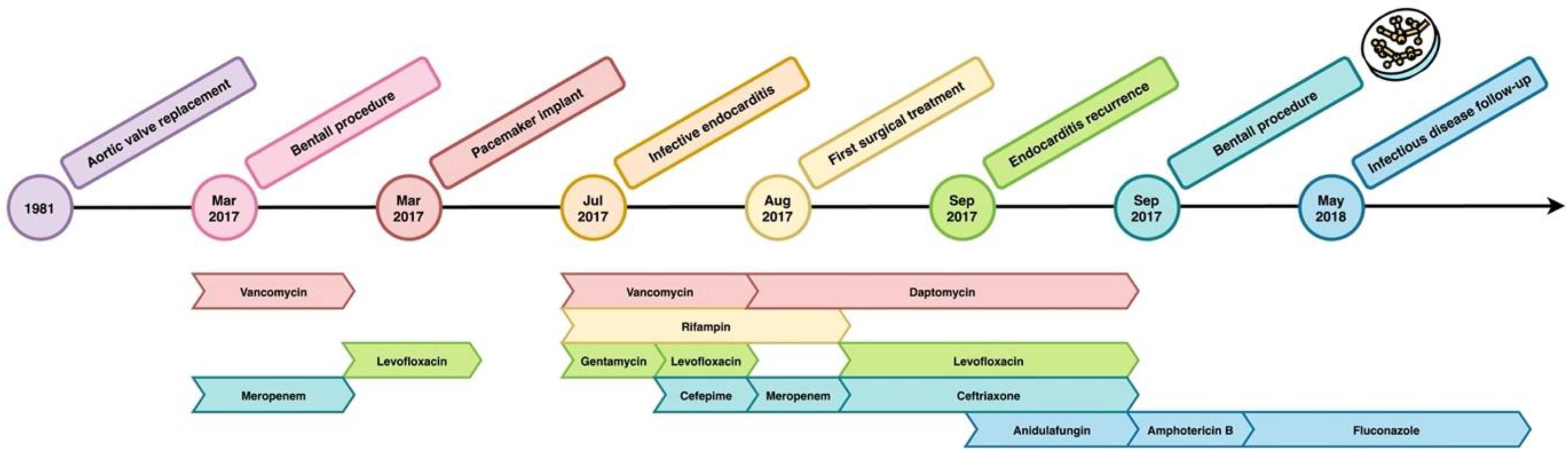
2. Case Report
3. Literature Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, S.C.-A.; Perfect, J.; Colombo, A.L.; Cornely, O.A.; Groll, A.H.; Seidel, D.; Albus, K.; de Almedia, J.N.; Garcia-Effron, G.; Gilroy, N.; et al. Global Guideline for the Diagnosis and Management of Rare Yeast Infections: An Initiative of the ECMM in Cooperation with ISHAM and ASM. Lancet Infect. Dis. 2021, 21, e375–e386. [Google Scholar] [CrossRef]
- Gross, J.W.; Kan, V.L. Trichosporon Asahii Infection in an Advanced AIDS Patient and Literature Review. AIDS 2008, 22, 793–795. [Google Scholar] [CrossRef] [PubMed]
- Bayramoglu, G.; Sonmez, M.; Tosun, I.; Aydin, K.; Aydin, F. Breakthrough Trichosporon Asahii Fungemia in Neutropenic Patient with Acute Leukemia While Receiving Caspofungin. Infection 2008, 36, 68–70. [Google Scholar] [CrossRef] [PubMed]
- Biasoli, M.S.; Carlson, D.; Chiganer, G.J.; Parodi, R.; Greca, A.; Tosello, M.E.; Luque, A.G.; Montero, A. Systemic Infection Caused by Trichosporon Asahii in a Patient with Liver Transplant. Med. Mycol. 2008, 46, 719–723. [Google Scholar] [CrossRef]
- Takashima, M.; Sugita, T. Taxonomy of Pathogenic Yeasts Candida, Cryptococcus, Malassezia, and Trichosporon. Med. Mycol. J. 2022, 63, 119–132. [Google Scholar] [CrossRef]
- Colombo, A.L.; Padovan, A.C.B.; Chaves, G.M. Current Knowledge of Trichosporon spp. and Trichosporonosis. Clin. Microbiol. Rev. 2011, 24, 682–700. [Google Scholar] [CrossRef] [PubMed]
- Chagas-Neto, T.C.; Chaves, G.M.; Colombo, A.L. Update on the Genus Trichosporon. Mycopathologia 2008, 166, 121–132. [Google Scholar] [CrossRef]
- Walsh, T.J. Trichosporonosis. Infect. Dis. Clin. N. Am. 1989, 3, 43–52. [Google Scholar] [CrossRef]
- Sugita, T.; Nishikawa, A.; Shinoda, T.; Kume, H. Taxonomic Position of Deep-Seated, Mucosa-Associated, and Superficial Isolates of Trichosporon Cutaneum from Trichosporonosis Patients. J. Clin. Microbiol. 1995, 33, 1368–1370. [Google Scholar] [CrossRef]
- Ruan, S.-Y.; Chien, J.-Y.; Hsueh, P.-R. Invasive Trichosporonosis Caused by Trichosporon asahii and Other Unusual Trichosporon Species at a Medical Center in Taiwan. Clin. Infect. Dis. 2009, 49, e11–e17. [Google Scholar] [CrossRef]
- Guého, E.; de Hoog, G.S.; Smith, M.T. Neotypification of the Genus Trichosporon. Antonie Van. Leeuwenhoek 1992, 61, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Pagnocca, F.C.; Legaspe, M.F.C.; Rodrigues, A.; Ruivo, C.C.C.; Nagamoto, N.S.; Bacci, M.; Forti, L.C. Yeasts Isolated from a Fungus-Growing Ant Nest, Including the Description of Trichosporon chiarellii sp. nov., an Anamorphic Basidiomycetous Yeast. Int. J. Syst. Evol. Microbiol. 2010, 60, 1454–1459. [Google Scholar] [CrossRef] [PubMed]
- Hickey, P.W.; Sutton, D.A.; Fothergill, A.W.; Rinaldi, M.G.; Wickes, B.L.; Schmidt, H.J.; Walsh, T.J. Trichosporon mycotoxinivorans, a Novel Respiratory Pathogen in Patients with Cystic Fibrosis. J. Clin. Microbiol. 2009, 47, 3091–3097. [Google Scholar] [CrossRef] [PubMed]
- Rath, P.C.; Purohit, B.V.; Agrawal, B.; Reddy, K.; Nutankavala, L.; Narreddy, S.; Reddy, M.; Abu Salim, M. Pacemaker Lead Endocarditis Due to Trichosporon Species. J. Assoc. Physicians India 2015, 63, 66–68. [Google Scholar] [PubMed]
- Oh, T.H.; Shin, S.U.; Kim, S.S.; Kim, S.E.; Kim, U.J.; Kang, S.-J.; Jang, H.-C.; Jung, S.I.; Shin, J.-H.; Park, K.-H. Prosthetic Valve Endocarditis by Trichosporon mucoides: A Case Report and Review of Literature. Medicine 2020, 99, e22584. [Google Scholar] [CrossRef]
- Izumi, K.; Hisata, Y.; Hazama, S. A Rare Case of Infective Endocarditis Complicated by Trichosporon asahii Fungemia Treated by Surgery. Ann. Thorac. Cardiovasc. Surg. 2009, 15, 350–353. [Google Scholar]
- Tokimatsu, I.; Kushima, H.; Hashinaga, K.; Umeki, K.; Ohama, M.; Ishii, H.; Kishi, K.; Hiramatsu, K.; Kadota, J.-I. The Prophylactic Effectiveness of Various Antifungal Agents against the Progression of Trichosporonosis Fungemia to Disseminated Disease in a Neutropenic Mouse Model. Int. J. Antimicrob. Agents 2007, 29, 84–88. [Google Scholar] [CrossRef]
- Ye, X.; Wang, A.; Lin, W.; Xu, Y.; Dong, X.; Zhou, Y.; Tian, K.; Xu, X. The Role of Intestinal Flora in Anti-Tumor Antibiotic Therapy. Front. Biosci. 2022, 27, 281. [Google Scholar] [CrossRef]
- Couto, R.; Couto, G.; Abrahão, I.; Compagnoni, I.; Carnio, T.; Tolentino, J. Endocarditis Due to Trichosporon beigelii 11 Years after Mitral Valve Replacement. Rev. Port. De Cardiol. 2021, 40, 305.e1–305.e3. [Google Scholar] [CrossRef]
- Mehta, V.; Mohanty, A.; Meena, S.; Rahul, J.S.; Uttam Kumar, N.; Chattopadhyay, D.; Bakliwal, A.; Choudhary, R.; Gupta, P. Wickerhamomyces Anomalous: A Rare Cause of Fungemia Causing Febrile Neutropenia in Acute Lymphoblastic Leukemia. Case Rep. Infect. Dis. 2020, 2020, 8847853. [Google Scholar] [CrossRef]
- Ramos, J.M.; Cuenca-Estrella, M.; Gutierrez, F.; Elia, M.; Rodriguez-Tudela, J.L. Clinical Case of Endocarditis Due to Trichosporon Inkin and Antifungal Susceptibility Profile of the Organism. J. Clin. Microbiol. 2004, 42, 2341–2344. [Google Scholar] [CrossRef]
- Paniagua, L.M.; Sudhakar, D.; Perez, L.E.; Miranda, D.; Urena, P.; Gregoric, I.; Kar, B.; Jneid, H.; Ramirez, J.; Paniagua, D. Prosthetic Valve Endocarditis from Trichosporon asahii in an Immunocompetent Patient. JACC Case Rep. 2020, 2, 693–696. [Google Scholar] [CrossRef]
- Tse, C.; Boodman, C.; Wuerz, T. Trichosporon Mucoides Prosthetic Valve Endocarditis Managed with Antifungal Suppression Therapy. Med. Mycol. Case Rep. 2022, 36, 10–12. [Google Scholar] [CrossRef] [PubMed]
- Tattevin, P.; Revest, M.; Lefort, A.; Michelet, C.; Lortholary, O. Fungal Endocarditis: Current Challenges. Int. J. Antimicrob. Agents 2014, 44, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Ghiasian, S.A.; Maghsood, A.H.; Mirhendi, S.H. Disseminated, Fatal Trichosporon asahii Infection in a Bone Marrow Transplant Recipient. J. Microbiol. Immunol. Infect. 2006, 39, 426–429. [Google Scholar] [PubMed]
- Fleming, R.V.; Walsh, T.J.; Anaissie, E.J. Emerging and Less Common Fungal Pathogens. Infect. Dis. Clin. N. Am. 2002, 16, 915–933. [Google Scholar] [CrossRef]
- Krcmery, V.; Mateicka, F.; Kunová, A.; Spánik, S.; Gyarfás, J.; Sycová, Z.; Trupl, J. Hematogenous Trichosporonosis in Cancer Patients: Report of 12 Cases Including 5 during Prophylaxis with Itraconazol. Support. Care Cancer 1999, 7, 39–43. [Google Scholar] [CrossRef]
- Walsh, T.J.; Groll, A.; Hiemenz, J.; Fleming, R.; Roilides, E.; Anaissie, E. Infections Due to Emerging and Uncommon Medically Important Fungal Pathogens. Clin. Microbiol. Infect. 2004, 10 (Suppl. 1), 48–66. [Google Scholar] [CrossRef]
- Kendirli, T.; Ciftçi, E.; Ince, E.; Oncel, S.; Dalgiç, N.; Güriz, H.; Unal, E.; Dogru, U. Successful Treatment of Trichosporon Mucoides Infection with Lipid Complex Amphotericin B and 5-Fluorocytosine. Mycoses 2006, 49, 251–253. [Google Scholar] [CrossRef]
- Padhi, S.; Dash, M.; Pattanaik, S.; Sahu, S. Fungemia Due to Trichosporon mucoides in a Diabetes Mellitus Patient: A Rare Case Report. Indian. J. Med. Microbiol. 2014, 32, 72–74. [Google Scholar] [CrossRef]
- Lopes, J.O.; Alves, S.H.; Klock, C.; Oliveira, L.T.; Dal Forno, N.R. Trichosporon Inkin Peritonitis during Continuous Ambulatory Peritoneal Dialysis with Bibliography Review. Mycopathologia 1997, 139, 15–18. [Google Scholar] [CrossRef]
- Watson, K.C.; Kallichurum, S. Brain Abscess Due to Trichosporon Cutaneum. J. Med. Microbiol. 1970, 3, 191–193. [Google Scholar] [CrossRef]
- Reyes, C.V.; Stanley, M.M.; Rippon, J.W. Trichosporon beigelii Endocarditis as a Complication of Peritoneovenous Shunt. Hum. Pathol. 1985, 16, 857–859. [Google Scholar] [CrossRef]
- McManus, E.J.; Jones, J.M. Detection of a Trichosporon beigelii Antigen Cross-Reactive with Cryptococcus Neoformans Capsular Polysaccharide in Serum from a Patient with Disseminated Trichosporon Infection. J. Clin. Microbiol. 1985, 21, 681–685. [Google Scholar] [CrossRef]
- Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; Fowler, V.G.; Tleyjeh, I.M.; Rybak, M.J.; Barsic, B.; Lockhart, P.B.; Gewitz, M.H.; Levison, M.E.; et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals from the American Heart Association. Circulation 2015, 132, 1435–1486. [Google Scholar] [CrossRef]
- Kontoyiannis, D.P.; Torres, H.A.; Chagua, M.; Hachem, R.; Tarrand, J.J.; Bodey, G.P.; Raad, I.I. Trichosporonosis in a Tertiary Care Cancer Center: Risk Factors, Changing Spectrum and Determinants of Outcome. Scand. J. Infect. Dis. 2004, 36, 564–569. [Google Scholar] [CrossRef]
- Nucci, M.; Anaissie, E. Revisiting the Source of Candidemia: Skin or Gut? Clin. Infect. Dis. 2001, 33, 1959–1967. [Google Scholar] [CrossRef]
- Colombo, A.L.; Branchini, M.L.; Geiger, D.; Schimidt, A.L.; Pignatari, A.C.; Fischman, O. Gastrointestinal Translocation as a Possible Source of Candidemia in an AIDS Patient. Rev. Inst. Med. Trop. Sao Paulo 1996, 38, 197–200. [Google Scholar] [CrossRef]
- Serena, C.; Pastor, F.J.; Gilgado, F.; Mayayo, E.; Guarro, J. Efficacy of Micafungin in Combination with Other Drugs in a Murine Model of Disseminated Trichosporonosis. Antimicrob. Agents Chemother. 2005, 49, 497–502. [Google Scholar] [CrossRef]
- Singh, S.; Capoor, M.R.; Varshney, S.; Gupta, D.K.; Verma, P.K.; Ramesh, V. Epidemiology and Antifungal Susceptibility of Infections Caused by Trichosporon Species: An Emerging Non-Candida and Non-Cryptococcus Yeast Worldwide. Indian. J. Med. Microbiol. 2019, 37, 536–541. [Google Scholar] [CrossRef]
- Girmenia, C.; Pagano, L.; Martino, B.; D’Antonio, D.; Fanci, R.; Specchia, G.; Melillo, L.; Buelli, M.; Pizzarelli, G.; Venditti, M.; et al. Invasive Infections Caused by Trichosporon Species and Geotrichum Capitatum in Patients with Hematological Malignancies: A Retrospective Multicenter Study from Italy and Review of the Literature. J. Clin. Microbiol. 2005, 43, 1818–1828. [Google Scholar] [CrossRef]
- Lacasse, A.; Cleveland, K.O. Trichosporon mucoides Fungemia in a Liver Transplant Recipient: Case Report and Review. Transpl. Infect. Dis. 2009, 11, 155–159. [Google Scholar] [CrossRef]
- Francisco, E.C.; de Almeida Junior, J.N.; de Queiroz Telles, F.; Aquino, V.R.; Mendes, A.V.A.; de Andrade Barberino, M.G.M.; de Tarso O Castro, P.; Guimarães, T.; Hahn, R.C.; Padovan, A.C.B.; et al. Species Distribution and Antifungal Susceptibility of 358 Trichosporon Clinical Isolates Collected in 24 Medical Centres. Clin. Microbiol. Infect. 2019, 25, 909.e1–909.e5. [Google Scholar] [CrossRef]
- Iturrieta-González, I.A.; Padovan, A.C.B.; Bizerra, F.C.; Hahn, R.C.; Colombo, A.L. Multiple Species of Trichosporon Produce Biofilms Highly Resistant to Triazoles and Amphotericin B. PLoS ONE 2014, 9, e109553. [Google Scholar] [CrossRef]
- Baddley, J.W.; Benjamin, D.K.; Patel, M.; Miró, J.; Athan, E.; Barsic, B.; Bouza, E.; Clara, L.; Elliott, T.; Kanafani, Z.; et al. Candida Infective Endocarditis. Eur. J. Clin. Microbiol. Infect. Dis. 2008, 27, 519–529. [Google Scholar] [CrossRef]
- Boland, J.M.; Chung, H.H.; Robberts, F.J.L.; Wilson, W.R.; Steckelberg, J.M.; Baddour, L.M.; Miller, D. V Fungal Prosthetic Valve Endocarditis: Mayo Clinic Experience with a Clinicopathological Analysis. Mycoses 2011, 54, 354–360. [Google Scholar] [CrossRef]
- Dağ, A.; Cerikçioğlu, N. Investigation of Some Virulence Factors of Trichosporon asahii Strains Isolated from the Clinical Samples of Hospitalized Patients. Mikrobiyol. Bul. 2006, 40, 225–235. [Google Scholar]
- Di Bonaventura, G.; Pompilio, A.; Picciani, C.; Iezzi, M.; D’Antonio, D.; Piccolomini, R. Biofilm Formation by the Emerging Fungal Pathogen Trichosporon asahii: Development, Architecture, and Antifungal Resistance. Antimicrob. Agents Chemother. 2006, 50, 3269–3276. [Google Scholar] [CrossRef]
- Sun, W.; Su, J.; Xu, S.; Yan, D. Trichosporon asahii Causing Nosocomial Urinary Tract Infections in Intensive Care Unit Patients: Genotypes, Virulence Factors and Antifungal Susceptibility Testing. J. Med. Microbiol. 2012, 61, 1750–1757. [Google Scholar] [CrossRef]
- Walsh, T.J.; Lee, J.W.; Melcher, G.P.; Navarro, E.; Bacher, J.; Callender, D.; Reed, K.D.; Wu, T.; Lopez-Berestein, G.; Pizzo, P.A. Experimental Trichosporon Infection in Persistently Granulocytopenic Rabbits: Implications for Pathogenesis, Diagnosis, and Treatment of an Emerging Opportunistic Mycosis. J. Infect. Dis. 1992, 166, 121–133. [Google Scholar] [CrossRef]


{kind=link}
| Age, Sex, Country | Comorbidities and Previous Surgery | Cultures and Pathogen | Site of Infection | Induction Therapy | Maintenance Therapy | Cardiac Surgery | Medical Suppression | Clinical Outcome | Follow-Up | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 [21] | 52, M, Spain | Biological valve replacement | Blood cultures: T. inkin post-mortem | Vegetation of the prosthetic aortic valve | None | None | None | None | Exitus 30 h after hospital admission | NA |
| 2 [16] | 58, M, Japan | HTN | Blood cultures: S. oralis later T. asahii | Endocarditis of prosthetic mitral valve and aortic valve cusp | IV fluconazole 400 mg/day | Fluconazole 200 mg q24h | Aortic and mitral valve replacement | None | Recovery | NA |
| 3 [14] | 57, F, India | HTN, DM, COPD, PM implant | Blood cultures: Trichosporon spp. | PM infection all valves were normal | IV voriconazole 200 mg q12h | Oral voriconazole 200 mg q12h | None | Voriconazole 200 mg q12h | Recovery | No recurrence, increased size of vegetation |
| 4 [22] | 20, M, Texas, USA | Biological aortic valve replacement | Blood cultures: negative Valve cultures: T. asahii | Large vegetations on the anterior wall of the aorta | Amphotericin B and ketoconazole for 2 weeks | Voriconazole | Valve replacement, patching of the aorta’s wall | Voriconazole 400 mg q8h for 6 months, q12h for 6 months, qd for 6 months | Complete recovery, resolution of hemiplegia | Normal echocardiogram at 5 years FU |
| 5 [15] | 66, M, Republic of Korea | Aortic valve replacement and mitral annuloplasty | Blood cultures and valve cultures: T. mucoides | Endocarditis of the prosthetic aortic and mitral valves | IV voriconazole and amphotericin B for 22 days | Voriconazole for 3 months | Valve replacement, removal of the prosthetic ring and pannus | None | Recovery | No evidence of relapse at 18 months FU |
| 6 [19] | 57, M, Portugal | Mitral valve replacement | Blood cultures: negative Valve cultures: T. beigelii | Endocarditis of prosthetic biological valve | Amphotericin B | Voriconazole | Valve replacement | None | Exitus 13 days after surgery | NA |
| 7 [23] | 63, M, Canada | DM, bioprosthetic aortic root and valve | Blood cultures: T. mucoides | Endocarditis of prosthetic aortic valve and valve abscess | Amphotericin B q24h for 6 days, IV voriconazole q12h for 2 weeks | Voriconazole 300 mg q12h and terbinafine 250 mg q24h | None | Voriconazole | Recovery | No recurrence but increased valve abscess at 12 months FU |
| 8 | 75, M, Italy | COPD, DM, OSAS Bioprosthetic aortic root and valve | Blood cultures: negative Valve cultures: T. asahii | Abscess of bioprosthetic aortic valve and several vegetations | Amphotericin B for 10 days | Fluconazole 600 mg q24h | Bioprosthetic valve replacement | Fluconazole 400 mg, later reduced to 100 mg, later reduced to 50 mg | Complete recovery | No recurrences, no valve vegetations at 5 years FU |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mulè, A.; Rossini, F.; Sollima, A.; Lenzi, A.; Fumarola, B.; Amadasi, S.; Chiari, E.; Lorenzotti, S.; Saccani, B.; Van Hauwermeiren, E.; et al. Trichosporon asahii Infective Endocarditis of Prosthetic Valve: A Case Report and Literature Review. Antibiotics 2023, 12, 1181. https://doi.org/10.3390/antibiotics12071181
Mulè A, Rossini F, Sollima A, Lenzi A, Fumarola B, Amadasi S, Chiari E, Lorenzotti S, Saccani B, Van Hauwermeiren E, et al. Trichosporon asahii Infective Endocarditis of Prosthetic Valve: A Case Report and Literature Review. Antibiotics. 2023; 12(7):1181. https://doi.org/10.3390/antibiotics12071181
Chicago/Turabian StyleMulè, Alice, Francesco Rossini, Alessio Sollima, Angelica Lenzi, Benedetta Fumarola, Silvia Amadasi, Erika Chiari, Silvia Lorenzotti, Barbara Saccani, Evelyn Van Hauwermeiren, and et al. 2023. "Trichosporon asahii Infective Endocarditis of Prosthetic Valve: A Case Report and Literature Review" Antibiotics 12, no. 7: 1181. https://doi.org/10.3390/antibiotics12071181
APA StyleMulè, A., Rossini, F., Sollima, A., Lenzi, A., Fumarola, B., Amadasi, S., Chiari, E., Lorenzotti, S., Saccani, B., Van Hauwermeiren, E., Lanza, P., Matteelli, A., Castelli, F., & Signorini, L. (2023). Trichosporon asahii Infective Endocarditis of Prosthetic Valve: A Case Report and Literature Review. Antibiotics, 12(7), 1181. https://doi.org/10.3390/antibiotics12071181