
What to Do with the New Antibiotics?

 ,
,
Abstract
1. Epidemiology of Resistance
2. Microbiological Interest of These New Antibiotics
2.1. Ceftolozane/Tazobactam (CTZ)
2.2. Ceftazidime/Avibactam (CZA)
2.3. Imipenem/Relebactam (IMI/REL)
2.4. Meropenem/Vaborbactam (MEV)
2.5. Cefiderocol (CFD)
3. What Is to Be Learnt from the Published Studies?
3.1. Ceftolozane/Tazobactam (CTZ)
3.2. Ceftazidime/Avibactam (CZA)
3.3. Imipenem/Relebactam (IMI/REL)
3.4. Meropenem/Vaborbactam (MEV)
3.5. Cefiderocol (CFD)
3.6. Aztreonam + Ceftazidim/Avibactam
4. For Which Patient to Prescribe These New Antibiotics as Empirical Treatment?
4.1. “It Takes All the Running You Can Do, to Keep in the Same Place”
4.2. Rationale for an Empirical Use of Antibiotics
4.3. What Is the Hurry?
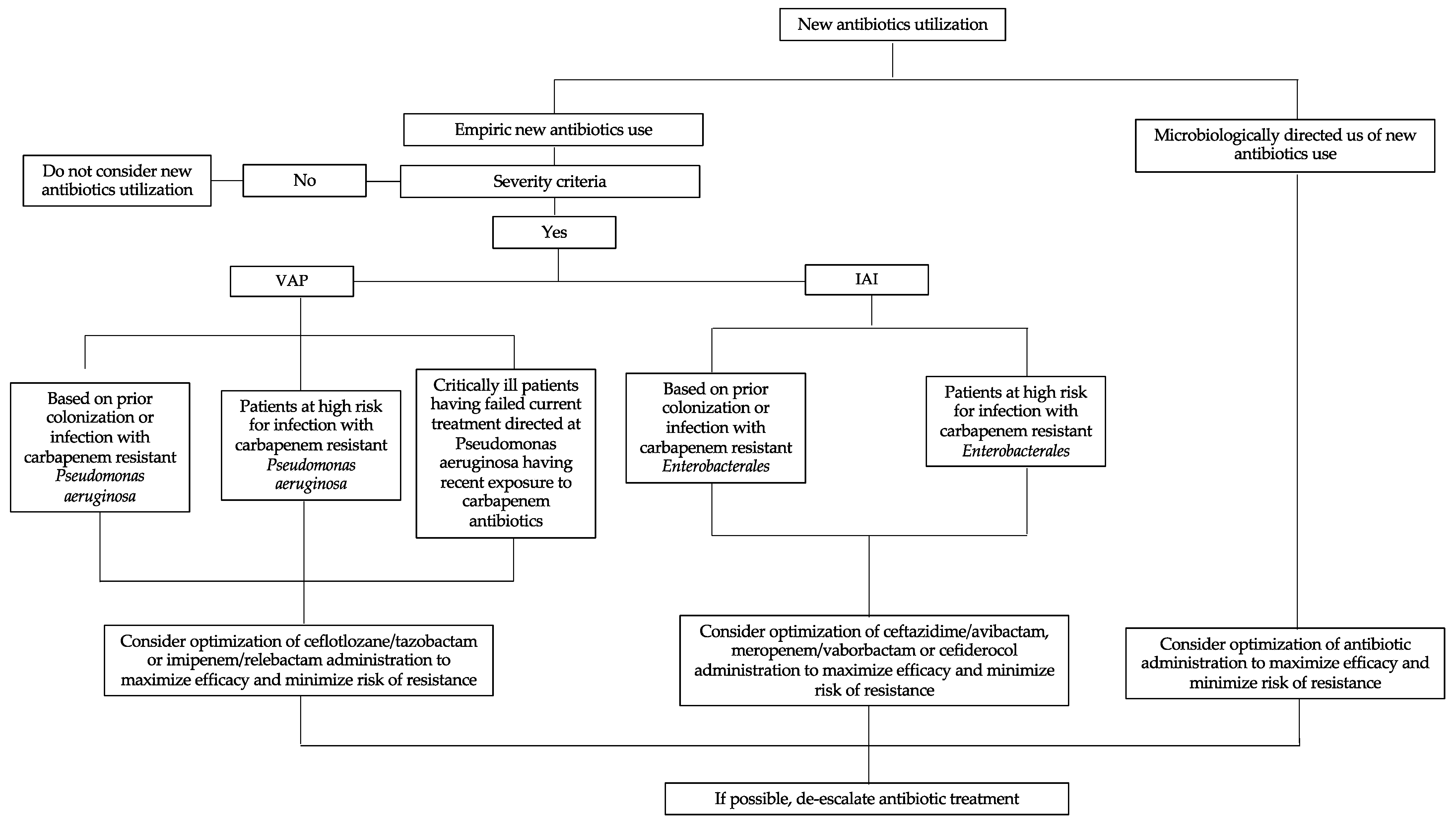
4.4. In Clinical Practice (Table 1)

{kind=link}
| Enterobacterales | Multidrug Pseudomonas aeruginosa | |||
|---|---|---|---|---|
| Classe A KPC | Classe B NDM, VIM | Classe D Oxa-48 | ||
| Ceftolozane/tazobactam | 1st intention | |||
| Ceftazidime/avibactam | 1st intention | 1st intention | Possible | |
| Imipeneme/relebactam | Possible | Possible | ||
| Meropeneme/vaborbactam | Possible | |||
| Aztreonam/avibactam | Possible | 1st intention | Possible | Possible |
| Cefiderocol | Possible | Possible | Possible | Possible |
5. Disadvantage of These New Antibiotics?
5.1. Emergence of Resistance
5.1.1. Ceftolozane/Tazobactam (CTZ)
5.1.2. Ceftazidime/Avibactam (CZA)
5.1.3. Imipenem/Relebactam (IMI/REL)
5.1.4. Meropenem/Vaborbactam (MEV)
5.1.5. Cefiderocol
5.2. Consequences on Microbiota, Collateral Effects
6. How to Administer These New Antibiotics (PK/PD Criteria)
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Willems, R.P.J.; van Dijk, K.; Vehreschild, M.J.G.T.; Biehl, L.M.; Ket, J.C.F.; Remmelzwaal, S.; Vandenbroucke-Grauls, C.M.J.E. Incidence of Infection with Multidrug-Resistant Gram-Negative Bacteria and Vancomycin-Resistant Enterococci in Carriers: A Systematic Review and Meta-Regression Analysis. Lancet Infect. Dis. 2023. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Baño, J.; Gutiérrez-Gutiérrez, B.; Machuca, I.; Pascual, A. Treatment of Infections Caused by Extended-Spectrum-Beta-Lactamase-, AmpC-, and Carbapenemase-Producing Enterobacteriaceae. Clin. Microbiol. Rev. 2018, 31, e00079-17. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, M.A. Real-World Antibiotic Needs for Resistant Gram-Negative Infections. Lancet Infect. Dis. 2020, 20, 1108–1109. [Google Scholar] [CrossRef]
- Sader, H.S.; Mendes, R.E.; Streit, J.M.; Carvalhaes, C.G.; Castanheira, M. Antimicrobial Susceptibility of Gram-Negative Bacteria from Intensive Care Unit and Non-Intensive Care Unit Patients from United States Hospitals (2018–2020). Diagn. Microbiol. Infect. Dis. 2022, 102, 115557. [Google Scholar] [CrossRef]
- van Duin, D.; Bonomo, R.A. Ceftazidime/Avibactam and Ceftolozane/Tazobactam: Second-Generation β-Lactam/β-Lactamase Inhibitor Combinations. Clin. Infect. Dis. 2016, 63, 234–241. [Google Scholar] [CrossRef]
- Sader, H.S.; Farrell, D.J.; Flamm, R.K.; Jones, R.N. Ceftolozane/Tazobactam Activity Tested against Aerobic Gram-Negative Organisms Isolated from Intra-Abdominal and Urinary Tract Infections in European and United States Hospitals (2012). J. Infect. 2014, 69, 266–277. [Google Scholar] [CrossRef]
- Murano, K.; Yamanaka, T.; Toda, A.; Ohki, H.; Okuda, S.; Kawabata, K.; Hatano, K.; Takeda, S.; Akamatsu, H.; Itoh, K.; et al. Structural Requirements for the Stability of Novel Cephalosporins to AmpC Beta-Lactamase Based on 3D-Structure. Bioorg. Med. Chem. 2008, 16, 2261–2275. [Google Scholar] [CrossRef] [PubMed]
- Sader, H.S.; Farrell, D.J.; Castanheira, M.; Flamm, R.K.; Jones, R.N. Antimicrobial Activity of Ceftolozane/Tazobactam Tested against Pseudomonas Aeruginosa and Enterobacteriaceae with Various Resistance Patterns Isolated in European Hospitals (2011-12). J. Antimicrob. Chemother. 2014, 69, 2713–2722. [Google Scholar] [CrossRef]
- Stachyra, T.; Levasseur, P.; Péchereau, M.-C.; Girard, A.-M.; Claudon, M.; Miossec, C.; Black, M.T. In Vitro Activity of the {beta}-Lactamase Inhibitor NXL104 against KPC-2 Carbapenemase and Enterobacteriaceae Expressing KPC Carbapenemases. J. Antimicrob. Chemother. 2009, 64, 326–329. [Google Scholar] [CrossRef]
- Tuon, F.F.; Rocha, J.L.; Formigoni-Pinto, M.R. Pharmacological Aspects and Spectrum of Action of Ceftazidime-Avibactam: A Systematic Review. Infection 2018, 46, 165–181. [Google Scholar] [CrossRef]
- Karlowsky, J.A.; Biedenbach, D.J.; Kazmierczak, K.M.; Stone, G.G.; Sahm, D.F. Activity of Ceftazidime-Avibactam against Extended-Spectrum- and AmpC β-Lactamase-Producing Enterobacteriaceae Collected in the INFORM Global Surveillance Study from 2012 to 2014. Antimicrob. Agents Chemother. 2016, 60, 2849–2857. [Google Scholar] [CrossRef]
- Lahiri, S.D.; Mangani, S.; Jahić, H.; Benvenuti, M.; Durand-Reville, T.F.; De Luca, F.; Ehmann, D.E.; Rossolini, G.M.; Alm, R.A.; Docquier, J.-D. Molecular Basis of Selective Inhibition and Slow Reversibility of Avibactam against Class D Carbapenemases: A Structure-Guided Study of OXA-24 and OXA-48. ACS Chem. Biol. 2015, 10, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Castanheira, M.; Mills, J.C.; Costello, S.E.; Jones, R.N.; Sader, H.S. Ceftazidime-Avibactam Activity Tested against Enterobacteriaceae Isolates from U.S. Hospitals (2011 to 2013) and Characterization of β-Lactamase-Producing Strains. Antimicrob. Agents Chemother. 2015, 59, 3509–3517. [Google Scholar] [CrossRef]
- Castanheira, M.; Mendes, R.E.; Sader, H.S. Low Frequency of Ceftazidime-Avibactam Resistance among Enterobacteriaceae Isolates Carrying BlaKPC Collected in U.S. Hospitals from 2012 to 2015. Antimicrob. Agents Chemother. 2017, 61, e02369-16. [Google Scholar] [CrossRef] [PubMed]
- Winkler, M.L.; Papp-Wallace, K.M.; Hujer, A.M.; Domitrovic, T.N.; Hujer, K.M.; Hurless, K.N.; Tuohy, M.; Hall, G.; Bonomo, R.A. Unexpected Challenges in Treating Multidrug-Resistant Gram-Negative Bacteria: Resistance to Ceftazidime-Avibactam in Archived Isolates of Pseudomonas Aeruginosa. Antimicrob. Agents Chemother. 2015, 59, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Citron, D.M.; Tyrrell, K.L.; Merriam, V.; Goldstein, E.J.C. In Vitro Activity of Ceftazidime-NXL104 against 396 Strains of β-Lactamase-Producing Anaerobes ▿. Antimicrob. Agents Chemother. 2011, 55, 3616–3620. [Google Scholar] [CrossRef] [PubMed]
- Zhanel, G.G.; Lawrence, C.K.; Adam, H.; Schweizer, F.; Zelenitsky, S.; Zhanel, M.; Lagacé-Wiens, P.R.S.; Walkty, A.; Denisuik, A.; Golden, A.; et al. Imipenem-Relebactam and Meropenem-Vaborbactam: Two Novel Carbapenem-β-Lactamase Inhibitor Combinations. Drugs 2018, 78, 65–98. [Google Scholar] [CrossRef]
- Karlowsky, J.A.; Lob, S.H.; Young, K.; Motyl, M.R.; Sahm, D.F. Activity of Imipenem/Relebactam against Pseudomonas Aeruginosa with Antimicrobial-Resistant Phenotypes from Seven Global Regions: SMART 2015-2016. J. Glob Antimicrob. Resist 2018, 15, 140–147. [Google Scholar] [CrossRef]
- Castanheira, M.; Huband, M.D.; Mendes, R.E.; Flamm, R.K. Meropenem-Vaborbactam Tested against Contemporary Gram-Negative Isolates Collected Worldwide during 2014, Including Carbapenem-Resistant, KPC-Producing, Multidrug-Resistant, and Extensively Drug-Resistant Enterobacteriaceae. Antimicrob. Agents Chemother. 2017, 61, e00567-17. [Google Scholar] [CrossRef]
- Blomquist, K.C.; Nix, D.E. A Critical Evaluation of Newer β-Lactam Antibiotics for Treatment of Pseudomonas Aeruginosa Infections. Ann. Pharmacother. 2021, 55, 1010–1024. [Google Scholar] [CrossRef]
- Ito, A.; Sato, T.; Ota, M.; Takemura, M.; Nishikawa, T.; Toba, S.; Kohira, N.; Miyagawa, S.; Ishibashi, N.; Matsumoto, S.; et al. In Vitro Antibacterial Properties of Cefiderocol, a Novel Siderophore Cephalosporin, against Gram-Negative Bacteria. Antimicrob. Agents Chemother. 2018, 62, e01454-17. [Google Scholar] [CrossRef]
- Shortridge, D.; Streit, J.M.; Mendes, R.; Castanheira, M. In Vitro Activity of Cefiderocol against U.S. and European Gram-Negative Clinical Isolates Collected in 2020 as Part of the SENTRY Antimicrobial Surveillance Program. Microbiol. Spectr. 2022, 10, e0271221. [Google Scholar] [CrossRef]
- Wagenlehner, F.M.; Umeh, O.; Steenbergen, J.; Yuan, G.; Darouiche, R.O. Ceftolozane-Tazobactam Compared with Levofloxacin in the Treatment of Complicated Urinary-Tract Infections, Including Pyelonephritis: A Randomised, Double-Blind, Phase 3 Trial (ASPECT-CUTI). Lancet 2015, 385, 1949–1956. [Google Scholar] [CrossRef] [PubMed]
- Solomkin, J.; Hershberger, E.; Miller, B.; Popejoy, M.; Friedland, I.; Steenbergen, J.; Yoon, M.; Collins, S.; Yuan, G.; Barie, P.S.; et al. Ceftolozane/Tazobactam Plus Metronidazole for Complicated Intra-Abdominal Infections in an Era of Multidrug Resistance: Results From a Randomized, Double-Blind, Phase 3 Trial (ASPECT-CIAI). Clin. Infect. Dis. 2015, 60, 1462–1471. [Google Scholar] [CrossRef]
- Kollef, M.H.; Nováček, M.; Kivistik, Ü.; Réa-Neto, Á.; Shime, N.; Martin-Loeches, I.; Timsit, J.-F.; Wunderink, R.G.; Bruno, C.J.; Huntington, J.A.; et al. Ceftolozane-Tazobactam versus Meropenem for Treatment of Nosocomial Pneumonia (ASPECT-NP): A Randomised, Controlled, Double-Blind, Phase 3, Non-Inferiority Trial. Lancet Infect. Dis. 2019, 19, 1299–1311. [Google Scholar] [CrossRef]
- Miller, B.; Popejoy, M.W.; Hershberger, E.; Steenbergen, J.N.; Alverdy, J. Characteristics and Outcomes of Complicated Intra-Abdominal Infections Involving Pseudomonas Aeruginosa from a Randomized, Double-Blind, Phase 3 Ceftolozane-Tazobactam Study. Antimicrob. Agents Chemother. 2016, 60, 4387–4390. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.G.; Bruno, C.; Castanheira, M.; Yu, B.; Huntington, J.A.; Carmelitano, P.; Rhee, E.G.; De Anda, C.; Motyl, M. Evaluating the Emergence of Nonsusceptibility among Pseudomonas Aeruginosa Respiratory Isolates from a Phase-3 Clinical Trial for Treatment of Nosocomial Pneumonia (ASPECT-NP). Int. J. Antimicrob. Agents 2021, 57, 106278. [Google Scholar] [CrossRef] [PubMed]
- Bergas, A.; Albasanz-Puig, A.; Fernández-Cruz, A.; Machado, M.; Novo, A.; van Duin, D.; Garcia-Vidal, C.; Hakki, M.; Ruiz-Camps, I.; Del Pozo, J.L.; et al. Real-Life Use of Ceftolozane/Tazobactam for the Treatment of Bloodstream Infection Due to Pseudomonas Aeruginosa in Neutropenic Hematologic Patients: A Matched Control Study (ZENITH Study). Microbiol. Spectr. 2022, 10, e0229221. [Google Scholar] [CrossRef]
- Pogue, J.M.; Lee, J.; Marchaim, D.; Yee, V.; Zhao, J.J.; Chopra, T.; Lephart, P.; Kaye, K.S. Incidence of and Risk Factors for Colistin-Associated Nephrotoxicity in a Large Academic Health System. Clin. Infect. Dis. 2011, 53, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Mogyoródi, B.; Csékó, A.B.; Hermann, C.; Gál, J.; Iványi, Z.D. Ceftolozane/Tazobactam versus Colistin in the Treatment of Ventilator-Associated Pneumonia Due to Extensively Drug-Resistant Pseudomonas Aeruginosa. Sci. Rep. 2022, 12, 4455. [Google Scholar] [CrossRef]
- A Multicentre, Parallel Group Open-Label Randomised Controlled Non-Inferiority Phase 3 Trial, of Ceftolozane-Tazobactam Versus Meropenem for Definitive Treatment of Bloodstream Infection Due to Extended-Spectrum Beta-Lactamase (ESBL) and AmpC-Producing Enterobacterales. Clinicaltrials.Gov; 2022 Mai. Report No.: NCT04238390. Available online: Https://Clinicaltrials.Gov/Ct2/Show/NCT04238390 (accessed on 21 June 2022).
- Carmeli, Y.; Armstrong, J.; Laud, P.J.; Newell, P.; Stone, G.; Wardman, A.; Gasink, L.B. Ceftazidime-Avibactam or Best Available Therapy in Patients with Ceftazidime-Resistant Enterobacteriaceae and Pseudomonas Aeruginosa Complicated Urinary Tract Infections or Complicated Intra-Abdominal Infections (REPRISE): A Randomised, Pathogen-Directed, Phase 3 Study. Lancet Infect. Dis. 2016, 16, 661–673. [Google Scholar] [CrossRef]
- Wagenlehner, F.M.; Sobel, J.D.; Newell, P.; Armstrong, J.; Huang, X.; Stone, G.G.; Yates, K.; Gasink, L.B. Ceftazidime-Avibactam Versus Doripenem for the Treatment of Complicated Urinary Tract Infections, Including Acute Pyelonephritis: RECAPTURE, a Phase 3 Randomized Trial Program. Clin. Infect. Dis. 2016, 63, 754–762. [Google Scholar] [CrossRef]
- Mazuski, J.E.; Gasink, L.B.; Armstrong, J.; Broadhurst, H.; Stone, G.G.; Rank, D.; Llorens, L.; Newell, P.; Pachl, J. Efficacy and Safety of Ceftazidime-Avibactam Plus Metronidazole Versus Meropenem in the Treatment of Complicated Intra-Abdominal Infection: Results From a Randomized, Controlled, Double-Blind, Phase 3 Program. Clin. Infect. Dis. 2016, 62, 1380–1389. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Zhong, N.; Pachl, J.; Timsit, J.-F.; Kollef, M.; Chen, Z.; Song, J.; Taylor, D.; Laud, P.J.; Stone, G.G.; et al. Ceftazidime-Avibactam versus Meropenem in Nosocomial Pneumonia, Including Ventilator-Associated Pneumonia (REPROVE): A Randomised, Double-Blind, Phase 3 Non-Inferiority Trial. Lancet Infect. Dis. 2018, 18, 285–295. [Google Scholar] [CrossRef]
- Mendes, R.E.; Castanheira, M.; Woosley, L.N.; Stone, G.G.; Bradford, P.A.; Flamm, R.K. Molecular β-Lactamase Characterization of Gram-Negative Pathogens Recovered from Patients Enrolled in the Ceftazidime-Avibactam Phase 3 Trials (RECAPTURE 1 and 2) for Complicated Urinary Tract Infections: Efficacies Analysed against Susceptible and Resistant Subsets. Int. J. Antimicrob. Agents 2018, 52, 287–292. [Google Scholar] [CrossRef]
- Mendes, R.E.; Castanheira, M.; Woosley, L.N.; Stone, G.G.; Bradford, P.A.; Flamm, R.K. Characterization of β-Lactamase Content of Ceftazidime-Resistant Pathogens Recovered during the Pathogen-Directed Phase 3 REPRISE Trial for Ceftazidime-Avibactam: Correlation of Efficacy against β-Lactamase Producers. Antimicrob. Agents Chemother. 2019, 63, e02655-18. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.G.; Newell, P.; Gasink, L.B.; Broadhurst, H.; Wardman, A.; Yates, K.; Chen, Z.; Song, J.; Chow, J.W. Clinical Activity of Ceftazidime/Avibactam against MDR Enterobacteriaceae and Pseudomonas Aeruginosa: Pooled Data from the Ceftazidime/Avibactam Phase III Clinical Trial Programme. J. Antimicrob. Chemother. 2018, 73, 2519–2523. [Google Scholar] [CrossRef] [PubMed]
- van Duin, D.; Lok, J.J.; Earley, M.; Cober, E.; Richter, S.S.; Perez, F.; Salata, R.A.; Kalayjian, R.C.; Watkins, R.R.; Doi, Y.; et al. Colistin Versus Ceftazidime-Avibactam in the Treatment of Infections Due to Carbapenem-Resistant Enterobacteriaceae. Clin. Infect. Dis. 2018, 66, 163–171. [Google Scholar] [CrossRef]
- Almangour, T.A.; Ghonem, L.; Aljabri, A.; Alruwaili, A.; Al Musawa, M.; Damfu, N.; Almalki, M.S.; Alattas, M.; Abed, H.; Naeem, D.; et al. Ceftazidime-Avibactam versus Colistin for the Treatment of Infections Due to Carbapenem-Resistant Enterobacterales: A Multicenter Cohort Study. Infect. Drug Resist. 2022, 15, 211–221. [Google Scholar] [CrossRef]
- Hakeam, H.A.; Alsahli, H.; Albabtain, L.; Alassaf, S.; Al Duhailib, Z.; Althawadi, S. Effectiveness of Ceftazidime-Avibactam versus Colistin in Treating Carbapenem-Resistant Enterobacteriaceae Bacteremia. Int. J. Infect. Dis. 2021, 109, 1–7. [Google Scholar] [CrossRef]
- Fang, J.; Li, H.; Zhang, M.; Shi, G.; Liu, M.; Wang, Y.; Bian, X. Efficacy of Ceftazidime-Avibactam Versus Polymyxin B and Risk Factors Affecting Clinical Outcomes in Patients With Carbapenem-Resistant Klebsiella Pneumoniae Infections a Retrospective Study. Front. Pharmacol. 2021, 12, 780940. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Hu, J.; Liu, P.; Wang, T.; Wang, H.; Liu, Y.; Cao, Q.; Zuo, X. Ceftazidime-Avibactam-Based Versus Tigecycline-Based Regimen for the Treatment of Carbapenem-Resistant Klebsiella Pneumoniae-Induced Pneumonia in Critically Ill Patients. Infect. Dis. Ther. 2021, 10, 2721–2734. [Google Scholar] [CrossRef] [PubMed]
- Castón, J.J.; Cano, A.; Pérez-Camacho, I.; Aguado, J.M.; Carratalá, J.; Ramasco, F.; Soriano, A.; Pintado, V.; Castelo-Corral, L.; Sousa, A.; et al. Impact of Ceftazidime/Avibactam versus Best Available Therapy on Mortality from Infections Caused by Carbapenemase-Producing Enterobacterales (CAVICOR Study). J. Antimicrob. Chemother. 2022, 77, 1452–1460. [Google Scholar] [CrossRef] [PubMed]
- Motsch, J.; Murta de Oliveira, C.; Stus, V.; Köksal, I.; Lyulko, O.; Boucher, H.W.; Kaye, K.S.; File, T.M.; Brown, M.L.; Khan, I.; et al. RESTORE-IMI 1: A Multicenter, Randomized, Double-Blind Trial Comparing Efficacy and Safety of Imipenem/Relebactam vs Colistin Plus Imipenem in Patients With Imipenem-Nonsusceptible Bacterial Infections. Clin. Infect. Dis. 2020, 70, 1799–1808. [Google Scholar] [CrossRef]
- Titov, I.; Wunderink, R.G.; Roquilly, A.; Rodríguez Gonzalez, D.; David-Wang, A.; Boucher, H.W.; Kaye, K.S.; Losada, M.C.; Du, J.; Tipping, R.; et al. A Randomized, Double-Blind, Multicenter Trial Comparing Efficacy and Safety of Imipenem/Cilastatin/Relebactam Versus Piperacillin/Tazobactam in Adults With Hospital-Acquired or Ventilator-Associated Bacterial Pneumonia (RESTORE-IMI 2 Study). Clin. Infect. Dis. 2021, 73, e4539–e4548. [Google Scholar] [CrossRef] [PubMed]
- Kaye, K.S.; Bhowmick, T.; Metallidis, S.; Bleasdale, S.C.; Sagan, O.S.; Stus, V.; Vazquez, J.; Zaitsev, V.; Bidair, M.; Chorvat, E.; et al. Effect of Meropenem-Vaborbactam vs Piperacillin-Tazobactam on Clinical Cure or Improvement and Microbial Eradication in Complicated Urinary Tract Infection: The TANGO I Randomized Clinical Trial. JAMA 2018, 319, 788–799. [Google Scholar] [CrossRef]
- Wunderink, R.G.; Giamarellos-Bourboulis, E.J.; Rahav, G.; Mathers, A.J.; Bassetti, M.; Vazquez, J.; Cornely, O.A.; Solomkin, J.; Bhowmick, T.; Bishara, J.; et al. Effect and Safety of Meropenem-Vaborbactam versus Best-Available Therapy in Patients with Carbapenem-Resistant Enterobacteriaceae Infections: The TANGO II Randomized Clinical Trial. Infect. Dis. Ther. 2018, 7, 439–455. [Google Scholar] [CrossRef]
- Ackley, R.; Roshdy, D.; Meredith, J.; Minor, S.; Anderson, W.E.; Capraro, G.A.; Polk, C. Meropenem-Vaborbactam versus Ceftazidime-Avibactam for Treatment of Carbapenem-Resistant Enterobacteriaceae Infections. Antimicrob. Agents Chemother. 2020, 64, e02313-19. [Google Scholar] [CrossRef]
- Athans, V.; Neuner, E.A.; Hassouna, H.; Richter, S.S.; Keller, G.; Castanheira, M.; Brizendine, K.D.; Mathers, A.J. Meropenem-Vaborbactam as Salvage Therapy for Ceftazidime-Avibactam-Resistant Klebsiella Pneumoniae Bacteremia and Abscess in a Liver Transplant Recipient. Antimicrob. Agents Chemother. 2019, 63, e01551-18. [Google Scholar] [CrossRef] [PubMed]
- Oliva, A.; Curtolo, A.; Volpicelli, L.; Cogliati Dezza, F.; De Angelis, M.; Cairoli, S.; Dell’Utri, D.; Goffredo, B.M.; Raponi, G.; Venditti, M. Synergistic Meropenem/Vaborbactam Plus Fosfomycin Treatment of KPC Producing K. Pneumoniae Septic Thrombosis Unresponsive to Ceftazidime/Avibactam: From the Bench to the Bedside. Antibiotics 2021, 10, 781. [Google Scholar] [CrossRef]
- Belati, A.; Bavaro, D.F.; Diella, L.; De Gennaro, N.; Di Gennaro, F.; Saracino, A. Meropenem/Vaborbactam Plus Aztreonam as a Possible Treatment Strategy for Bloodstream Infections Caused by Ceftazidime/Avibactam-Resistant Klebsiella Pneumoniae: A Retrospective Case Series and Literature Review. Antibiotics 2022, 11, 373. [Google Scholar] [CrossRef]
- Portsmouth, S.; van Veenhuyzen, D.; Echols, R.; Machida, M.; Ferreira, J.C.A.; Ariyasu, M.; Tenke, P.; Nagata, T.D. Cefiderocol versus Imipenem-Cilastatin for the Treatment of Complicated Urinary Tract Infections Caused by Gram-Negative Uropathogens: A Phase 2, Randomised, Double-Blind, Non-Inferiority Trial. Lancet Infect. Dis. 2018, 18, 1319–1328. [Google Scholar] [CrossRef]
- Wunderink, R.G.; Matsunaga, Y.; Ariyasu, M.; Clevenbergh, P.; Echols, R.; Kaye, K.S.; Kollef, M.; Menon, A.; Pogue, J.M.; Shorr, A.F.; et al. Cefiderocol versus High-Dose, Extended-Infusion Meropenem for the Treatment of Gram-Negative Nosocomial Pneumonia (APEKS-NP): A Randomised, Double-Blind, Phase 3, Non-Inferiority Trial. Lancet Infect. Dis. 2021, 21, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Echols, R.; Matsunaga, Y.; Ariyasu, M.; Doi, Y.; Ferrer, R.; Lodise, T.P.; Naas, T.; Niki, Y.; Paterson, D.L.; et al. Efficacy and Safety of Cefiderocol or Best Available Therapy for the Treatment of Serious Infections Caused by Carbapenem-Resistant Gram-Negative Bacteria (CREDIBLE-CR): A Randomised, Open-Label, Multicentre, Pathogen-Focused, Descriptive, Phase 3 Trial. Lancet Infect. Dis. 2021, 21, 226–240. [Google Scholar] [CrossRef] [PubMed]
- Pascale, R.; Pasquini, Z.; Bartoletti, M.; Caiazzo, L.; Fornaro, G.; Bussini, L.; Volpato, F.; Marchionni, E.; Rinaldi, M.; Trapani, F.; et al. Cefiderocol Treatment for Carbapenem-Resistant Acinetobacter Baumannii Infection in the ICU during the COVID-19 Pandemic: A Multicentre Cohort Study. JAC Antimicrob. Resist. 2021, 3, dlab174. [Google Scholar] [CrossRef]
- Falcone, M.; Tiseo, G.; Leonildi, A.; Della Sala, L.; Vecchione, A.; Barnini, S.; Farcomeni, A.; Menichetti, F. Cefiderocol- Compared to Colistin-Based Regimens for the Treatment of Severe Infections Caused by Carbapenem-Resistant Acinetobacter Baumannii. Antimicrob. Agents Chemother. 2022, 66, e0214221. [Google Scholar] [CrossRef]
- Cefiderocol Versus Standard Therapy for Healthcare Associated and Hospital Acquired Gram-Negative Blood Stream Infection: Study Protocol (the GAME CHANGER Trial). Clinicaltrials.Gov; 2022 Juin. Report No.: NCT03869437. Available online: Https://Clinicaltrials.Gov/Ct2/Show/NCT03869437 (accessed on 23 June 2022).
- Mauri, C.; Maraolo, A.E.; Di Bella, S.; Luzzaro, F.; Principe, L. The Revival of Aztreonam in Combination with Avibactam against Metallo-β-Lactamase-Producing Gram-Negatives: A Systematic Review of In Vitro Studies and Clinical Cases. Antibiotics 2021, 10, 1012. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Daikos, G.L.; Tiseo, G.; Bassoulis, D.; Giordano, C.; Galfo, V.; Leonildi, A.; Tagliaferri, E.; Barnini, S.; Sani, S.; et al. Efficacy of Ceftazidime-Avibactam Plus Aztreonam in Patients With Bloodstream Infections Caused by Metallo-β-Lactamase-Producing Enterobacterales. Clin. Infect. Dis. 2021, 72, 1871–1878. [Google Scholar] [CrossRef]
- Stockmann, C.; Ampofo, K.; Pavia, A.T.; Blaschke, A.J.; Mason, E.O.; Presson, A.P.; Forney, L.J.; Byington, C.L. Clinical and Epidemiological Evidence of the Red Queen Hypothesis in Pneumococcal Serotype Dynamics. Clin. Infect. Dis. 2016, 63, 619–626. [Google Scholar] [CrossRef]
- Podolsky, S.H. The Evolving Response to Antibiotic Resistance (1945–2018). Palgrave Commun. 2018, 4, 1–8. [Google Scholar] [CrossRef]
- European Food Safety Authority; European Centre for Disease Prevention and Control; European Medicines Agency. Antimicrobial Consumption and Resistance in Bacteria from Humans and Animals: Third JoInt. Inter-Agency Report on Integrated Analysis of Antimicrobial Agent Consumption and Occurrence of Antimicrobial Resistance in Bacteria from Humans and Food-Producing Animals in the EU/EEA: JIACRA III 2016–2018. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/JIACRA-III-Antimicrobial-Consumption-and-Resistance-in-Bacteria-from-Humans-and-Animals.pdf (accessed on 20 February 2023).
- Bassetti, D.; Bassetti, M.; Mantero, E. Strategies for Antibiotic Selection in Empirical Therapy. Clin. Microbiol. Infect. 2000, 6, 98–100. [Google Scholar] [CrossRef]
- Paul, M.; Carrara, E.; Retamar, P.; Tängdén, T.; Bitterman, R.; Bonomo, R.A.; de Waele, J.; Daikos, G.L.; Akova, M.; Harbarth, S.; et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Guidelines for the Treatment of Infections Caused by Multidrug-Resistant Gram-Negative Bacilli (Endorsed by European Society of Intensive Care Medicine). Clin. Microbiol. Infect. 2022, 28, 521–547. [Google Scholar] [CrossRef]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America 2022 Guidance on the Treatment of Extended-Spectrum β-Lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas Aeruginosa with Difficult-to-Treat Resistance (DTR-P. Aeruginosa). Clin. Infect. Dis. 2022, 75, 187–212. [Google Scholar] [CrossRef]
- Detsis, M.; Karanika, S.; Mylonakis, E. ICU Acquisition Rate, Risk Factors, and Clinical Significance of Digestive Tract Colonization With Extended-Spectrum Beta-Lactamase-Producing Enterobacteriaceae: A Systematic Review and Meta-Analysis. Crit. Care Med. 2017, 45, 705–714. [Google Scholar] [CrossRef]
- Hranjec, T.; Rosenberger, L.H.; Swenson, B.; Metzger, R.; Flohr, T.R.; Politano, A.D.; Riccio, L.M.; Popovsky, K.A.; Sawyer, R.G. Aggressive versus Conservative Initiation of Antimicrobial Treatment in Critically Ill Surgical Patients with Suspected Intensive-Care-Unit-Acquired Infection: A Quasi-Experimental, before and after Observational Cohort Study. Lancet Infect. Dis. 2012, 12, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Tumbarello, M.; Trecarichi, E.M.; Corona, A.; De Rosa, F.G.; Bassetti, M.; Mussini, C.; Menichetti, F.; Viscoli, C.; Campoli, C.; Venditti, M.; et al. Efficacy of Ceftazidime-Avibactam Salvage Therapy in Patients With Infections Caused by Klebsiella Pneumoniae Carbapenemase-Producing K. Pneumoniae. Clin. Infect. Dis. 2019, 68, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Karakonstantis, S.; Rousaki, M.; Kritsotakis, E.I. Cefiderocol: Systematic Review of Mechanisms of Resistance, Heteroresistance and In Vivo Emergence of Resistance. Antibiotics 2022, 11, 723. [Google Scholar] [CrossRef]
- Gaibani, P.; Giani, T.; Bovo, F.; Lombardo, D.; Amadesi, S.; Lazzarotto, T.; Coppi, M.; Rossolini, G.M.; Ambretti, S. Resistance to Ceftazidime/Avibactam, Meropenem/Vaborbactam and Imipenem/Relebactam in Gram-Negative MDR Bacilli: Molecular Mechanisms and Susceptibility Testing. Antibiotics 2022, 11, 628. [Google Scholar] [CrossRef] [PubMed]
- Papp-Wallace, K.M.; Mack, A.R.; Taracila, M.A.; Bonomo, R.A. Resistance to Novel β-Lactam-β-Lactamase Inhibitor Combinations: The “Price of Progress”. Infect. Dis. Clin. N. Am. 2020, 34, 773–819. [Google Scholar] [CrossRef] [PubMed]
- Yahav, D.; Giske, C.G.; Grāmatniece, A.; Abodakpi, H.; Tam, V.H.; Leibovici, L. New β-Lactam-β-Lactamase Inhibitor Combinations. Clin. Microbiol. Rev. 2020, 34, e00115-20. [Google Scholar] [CrossRef]
- Gomis-Font, M.A.; Pitart, C.; Del Barrio-Tofiño, E.; Zboromyrska, Y.; Cortes-Lara, S.; Mulet, X.; Marco, F.; Vila, J.; López-Causapé, C.; Oliver, A. Emergence of Resistance to Novel Cephalosporin-β-Lactamase Inhibitor Combinations through the Modification of the Pseudomonas Aeruginosa MexCD-OprJ. Efflux Pump. Antimicrob. Agents Chemother. 2021, 65, e0008921. [Google Scholar] [CrossRef]
- Rapid Risk Assessment: Emergence of Resistance to Ceftazidime-AvibactAm. in Carbapenem-Resistant Enterobacteriaceae. Available online: https://www.ecdc.europa.eu/en/publications-data/rapid-risk-assessment-emergence-resistance-ceftazidime-avibactam-carbapenem (accessed on 20 February 2023).
- Gaibani, P.; Campoli, C.; Lewis, R.E.; Volpe, S.L.; Scaltriti, E.; Giannella, M.; Pongolini, S.; Berlingeri, A.; Cristini, F.; Bartoletti, M.; et al. In Vivo Evolution of Resistant Subpopulations of KPC-Producing Klebsiella Pneumoniae during Ceftazidime/AvibactAm. Treatment. J. Antimicrob. Chemother. 2018, 73, 1525–1529. [Google Scholar] [CrossRef] [PubMed]
- Cano, Á.; Guzmán-Puche, J.; García-Gutiérrez, M.; Castón, J.J.; Gracia-Ahufinger, I.; Pérez-Nadales, E.; Recio, M.; Natera, A.M.; Marfil-Pérez, E.; Martínez-Martínez, L.; et al. Use of Carbapenems in the Combined Treatment of Emerging Ceftazidime/Avibactam-Resistant and Carbapenem-Susceptible KPC-Producing Klebsiella Pneumoniae Infections: Report of a Case and Review of the Literature. J. Glob. Antimicrob. Resist. 2020, 22, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Li, H.; Wang, Q.; Liu, Y.; Cao, B. Increased Gene Expression and Copy Number of Mutated BlaKPC Lead to High-Level Ceftazidime/AvibactAm. Resistance in Klebsiella Pneumoniae. BMC Microbiol. 2021, 21, 230. [Google Scholar] [CrossRef]
- Di Bella, S.; Giacobbe, D.R.; Maraolo, A.E.; Viaggi, V.; Luzzati, R.; Bassetti, M.; Luzzaro, F.; Principe, L. Resistance to Ceftazidime/AvibactAm. in Infections and Colonisations by KPC-Producing Enterobacterales: A Systematic Review of Observational Clinical Studies. J. Glob. Antimicrob. Resist. 2021, 25, 268–281. [Google Scholar] [CrossRef]
- Chalhoub, H.; Sáenz, Y.; Nichols, W.W.; Tulkens, P.M.; Van Bambeke, F. Loss of Activity of Ceftazidime-AvibactAm. Due to MexAB-OprM Efflux and Overproduction of AmpC Cephalosporinase in Pseudomonas Aeruginosa Isolated from Patients Suffering from Cystic Fibrosis. Int. J. Antimicrob. Agents 2018, 52, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Zamudio, R.; Hijazi, K.; Joshi, C.; Aitken, E.; Oggioni, M.R.; Gould, I.M. Phylogenetic Analysis of Resistance to Ceftazidime/Avibactam, Ceftolozane/TazobactAm. and Carbapenems in Piperacillin/Tazobactam-Resistant Pseudomonas Aeruginosa from Cystic Fibrosis Patients. Int. J. Antimicrob. Agents 2019, 53, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Lapuebla, A.; Abdallah, M.; Olafisoye, O.; Cortes, C.; Urban, C.; Quale, J.; Landman, D. Activity of Meropenem Combined with RPX7009, a Novel β-Lactamase Inhibitor, against Gram-Negative Clinical Isolates in New York City. Antimicrob. Agents Chemother. 2015, 59, 4856–4860. [Google Scholar] [CrossRef]
- Mushtaq, S.; Meunier, D.; Vickers, A.; Woodford, N.; Livermore, D.M. Activity of Imipenem/RelebactAm. against Pseudomonas Aeruginosa Producing ESBLs and Carbapenemases. J. Antimicrob. Chemother. 2021, 76, 434–442. [Google Scholar] [CrossRef]
- Lomovskaya, O.; Sun, D.; Rubio-Aparicio, D.; Nelson, K.; Tsivkovski, R.; Griffith, D.C.; Dudley, M.N. Vaborbactam: Spectrum of Beta-Lactamase Inhibition and Impact of Resistance Mechanisms on Activity in Enterobacteriaceae. Antimicrob. Agents Chemother. 2017, 61, e01443-17. [Google Scholar] [CrossRef]
- Zhou, M.; Yang, Q.; Lomovskaya, O.; Sun, D.; Kudinha, T.; Xu, Z.; Zhang, G.; Chen, X.; Xu, Y. In Vitro Activity of Meropenem Combined with VaborbactAm. against KPC-Producing Enterobacteriaceae in China. J. Antimicrob. Chemother. 2018, 73, 2789–2796. [Google Scholar] [CrossRef] [PubMed]
- Choby, J.E.; Ozturk, T.; Satola, S.W.; Jacob, J.T.; Weiss, D.S. Widespread Cefiderocol Heteroresistance in Carbapenem-Resistant Gram-Negative Pathogens. Lancet Infect. Dis. 2021, 21, 597–598. [Google Scholar] [CrossRef] [PubMed]
- Choby, J.E.; Ozturk, T.; Satola, S.W.; Jacob, J.T.; Weiss, D.S. Does Cefiderocol Heteroresistance Explain the Discrepancy between the APEKS-NP and CREDIBLE-CR Clinical Trial Results? Lancet Microbe 2021, 2, e648–e649. [Google Scholar] [CrossRef]
- Simner, P.J.; Mostafa, H.H.; Bergman, Y.; Ante, M.; Tekle, T.; Adebayo, A.; Beisken, S.; Dzintars, K.; Tamma, P.D. Progressive Development of Cefiderocol Resistance in Escherichia Coli During Therapy Is Associated With an Increase in BlaNDM-5 Copy Number and Gene Expression. Clin. Infect. Dis. 2022, 75, 47–54. [Google Scholar] [CrossRef]
- Sadek, M.; Le Guern, R.; Kipnis, E.; Gosset, P.; Poirel, L.; Dessein, R.; Nordmann, P. Progressive in Vivo Development of Resistance to Cefiderocol in Pseudomonas Aeruginosa. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 42, 61–66. [Google Scholar] [CrossRef]
- Sansone, P.; Giaccari, L.G.; Coppolino, F.; Aurilio, C.; Barbarisi, A.; Passavanti, M.B.; Pota, V.; Pace, M.C. Cefiderocol for Carbapenem-Resistant Bacteria: Handle with Care! A Review of the Real-World Evidence. Antibiotics 2022, 11, 904. [Google Scholar] [CrossRef]
- Rashid, M.-U.; Rosenborg, S.; Panagiotidis, G.; Löfdal, K.S.; Weintraub, A.; Nord, C.E. Ecological Effect of Ceftazidime/AvibactAm. on the Normal Human Intestinal Microbiota. Int. J. Antimicrob. Agents 2015, 46, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Vardakas, K.Z.; Voulgaris, G.L.; Maliaros, A.; Samonis, G.; Falagas, M.E. Prolonged versus Short-Term Intravenous Infusion of Antipseudomonal β-Lactams for Patients with Sepsis: A Systematic Review and Meta-Analysis of Randomised Trials. Lancet Infect. Dis. 2018, 18, 108–120. [Google Scholar] [CrossRef]
- Roberts, J.A.; Ulldemolins, M.; Roberts, M.S.; McWhinney, B.; Ungerer, J.; Paterson, D.L.; Lipman, J. Therapeutic Drug Monitoring of Beta-Lactams in Critically Ill Patients: Proof of Concept. Int. J. Antimicrob. Agents 2010, 36, 332–339. [Google Scholar] [CrossRef]
- Griffith, D.C.; Loutit, J.S.; Morgan, E.E.; Durso, S.; Dudley, M.N. Phase 1 Study of the Safety, Tolerability, and Pharmacokinetics of the β-Lactamase Inhibitor VaborbactAm. (RPX7009) in Healthy Adult Subjects. Antimicrob. Agents Chemother. 2016, 60, 6326–6332. [Google Scholar] [CrossRef]
- Cada, D.J.; Wageman, J.; Baker, D.E.; Levien, T.L. Ceftolozane/Tazobactam. Hosp. Pharm. 2015, 50, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, S.; Singley, C.M.; Hoover, J.; Nakamura, R.; Echols, R.; Rittenhouse, S.; Tsuji, M.; Yamano, Y. Efficacy of Cefiderocol against Carbapenem-Resistant Gram-Negative Bacilli in Immunocompetent-Rat Respiratory Tract Infection Models Recreating Human Plasma Pharmacokinetics. Antimicrob. Agents Chemother. 2017, 61, e00700-17. [Google Scholar] [CrossRef]
- Das, S.; Li, J.; Armstrong, J.; Learoyd, M.; Edeki, T. Randomized Pharmacokinetic and Drug-Drug Interaction Studies of Ceftazidime, Avibactam, and Metronidazole in Healthy Subjects. Pharmacol. Res. Perspect. 2015, 3, e00172. [Google Scholar] [CrossRef] [PubMed]
- Rubino, C.M.; Bhavnani, S.M.; Loutit, J.S.; Morgan, E.E.; White, D.; Dudley, M.N.; Griffith, D.C. Phase 1 Study of the Safety, Tolerability, and Pharmacokinetics of VaborbactAm. and Meropenem Alone and in Combination Following Single and Multiple Doses in Healthy Adult Subjects. Antimicrob. Agents Chemother. 2018, 62, e02228-17. [Google Scholar] [CrossRef] [PubMed]
- Saisho, Y.; Katsube, T.; White, S.; Fukase, H.; Shimada, J. Pharmacokinetics, Safety, and Tolerability of Cefiderocol, a Novel Siderophore Cephalosporin for Gram-Negative Bacteria, in Healthy Subjects. Antimicrob. Agents Chemother. 2018, 62, e02163-17. [Google Scholar] [CrossRef]
- Nicolau, D.P.; Siew, L.; Armstrong, J.; Li, J.; Edeki, T.; Learoyd, M.; Das, S. Phase 1 Study Assessing the Steady-State Concentration of Ceftazidime and AvibactAm. in Plasma and Epithelial Lining Fluid Following Two Dosing Regimens. J. Antimicrob. Chemother. 2015, 70, 2862–2869. [Google Scholar] [CrossRef]
- Wenzler, E.; Gotfried, M.H.; Loutit, J.S.; Durso, S.; Griffith, D.C.; Dudley, M.N.; Rodvold, K.A. Meropenem-RPX7009 Concentrations in Plasma, Epithelial Lining Fluid, and Alveolar Macrophages of Healthy Adult Subjects. Antimicrob. Agents Chemother. 2015, 59, 7232–7239. [Google Scholar] [CrossRef]
- Rizk, M.L.; Rhee, E.G.; Jumes, P.A.; Gotfried, M.H.; Zhao, T.; Mangin, E.; Bi, S.; Chavez-Eng, C.M.; Zhang, Z.; Butterton, J.R. Intrapulmonary Pharmacokinetics of Relebactam, a Novel β-Lactamase Inhibitor, Dosed in Combination with Imipenem-Cilastatin in Healthy Subjects. Antimicrob. Agents Chemother. 2018, 62, e01411-17. [Google Scholar] [CrossRef]
- Sheffield, M.; Nelson, D.; O’Neal, M.; Gould, A.P.; Bouchard, J.; Nicolau, D.; Justo, J.A.; Hucks, J.; Bookstaver, P.B. Use of Continuous-Infusion Ceftolozane/TazobactAm. for Resistant Gram-Negative Bacterial Infections: A Retrospective Analysis and Brief Review of the Literature. Int. J. Antimicrob. Agents 2020, 56, 106158. [Google Scholar] [CrossRef]
- Goncette, V.; Layios, N.; Descy, J.; Frippiat, F. Continuous Infusion, Therapeutic Drug Monitoring and Outpatient Parenteral Antimicrobial Therapy with Ceftazidime/Avibactam: A Retrospective Cohort Study. J. Glob. Antimicrob. Resist. 2021, 26, 15–19. [Google Scholar] [CrossRef]
- Loeuille, G.; D’Huart, E.; Vigneron, J.; Nisse, Y.-E.; Beiler, B.; Polo, C.; Ayari, G.; Sacrez, M.; Demoré, B.; Charmillon, A. Stability Studies of 16 Antibiotics for Continuous Infusion in Intensive Care Units and for Performing Outpatient Parenteral Antimicrobial Therapy. Antibiotics 2022, 11, 458. [Google Scholar] [CrossRef] [PubMed]
- EUCAST: Clinical Breakpoints and Dosing of Antibiotics. Available online: Https://Www.Eucast.Org/Clinical_breakpoints/ (accessed on 23 August 2022).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaïbi, K.; Jaureguy, F.; Do Rego, H.; Ruiz, P.; Mory, C.; El Helali, N.; Mrabet, S.; Mizrahi, A.; Zahar, J.-R.; Pilmis, B. What to Do with the New Antibiotics? Antibiotics 2023, 12, 654. https://doi.org/10.3390/antibiotics12040654
Chaïbi K, Jaureguy F, Do Rego H, Ruiz P, Mory C, El Helali N, Mrabet S, Mizrahi A, Zahar J-R, Pilmis B. What to Do with the New Antibiotics? Antibiotics. 2023; 12(4):654. https://doi.org/10.3390/antibiotics12040654
Chicago/Turabian StyleChaïbi, Khalil, Françoise Jaureguy, Hermann Do Rego, Pablo Ruiz, Céline Mory, Najoua El Helali, Sara Mrabet, Assaf Mizrahi, Jean-Ralph Zahar, and Benoît Pilmis. 2023. "What to Do with the New Antibiotics?" Antibiotics 12, no. 4: 654. https://doi.org/10.3390/antibiotics12040654
APA StyleChaïbi, K., Jaureguy, F., Do Rego, H., Ruiz, P., Mory, C., El Helali, N., Mrabet, S., Mizrahi, A., Zahar, J.-R., & Pilmis, B. (2023). What to Do with the New Antibiotics? Antibiotics, 12(4), 654. https://doi.org/10.3390/antibiotics12040654