
Reporting Antimicrobial-Related Adverse Drug Events in Jordan: An Analysis from the VigiBase Database

 , and
, and
Abstract
1. Introduction
2. Results
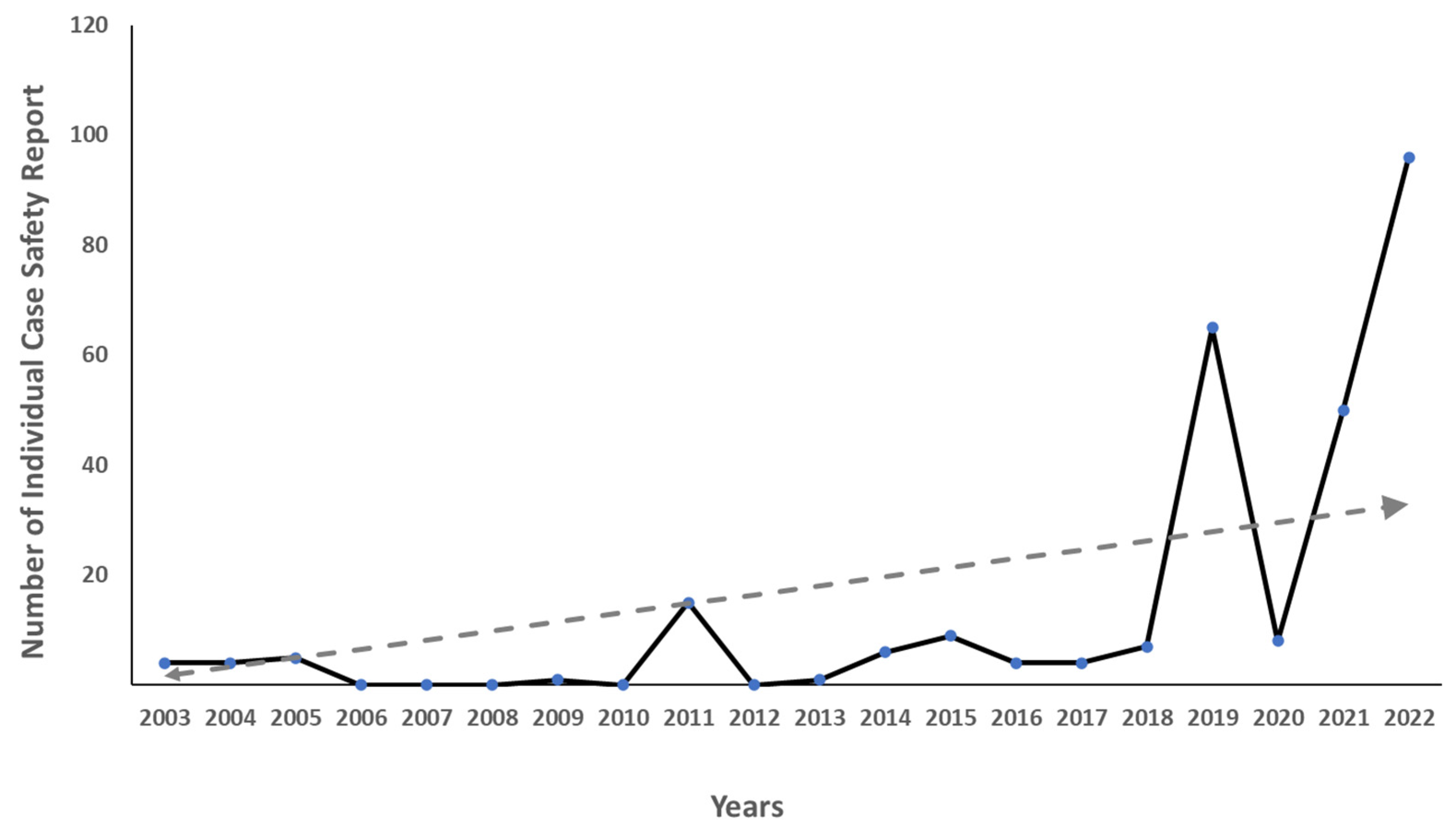
2.1. Trends in the Number of ICSRs
2.2. Demographics and General Characteristics
2.3. Chemical Subgroup of Drugs Included in the Search
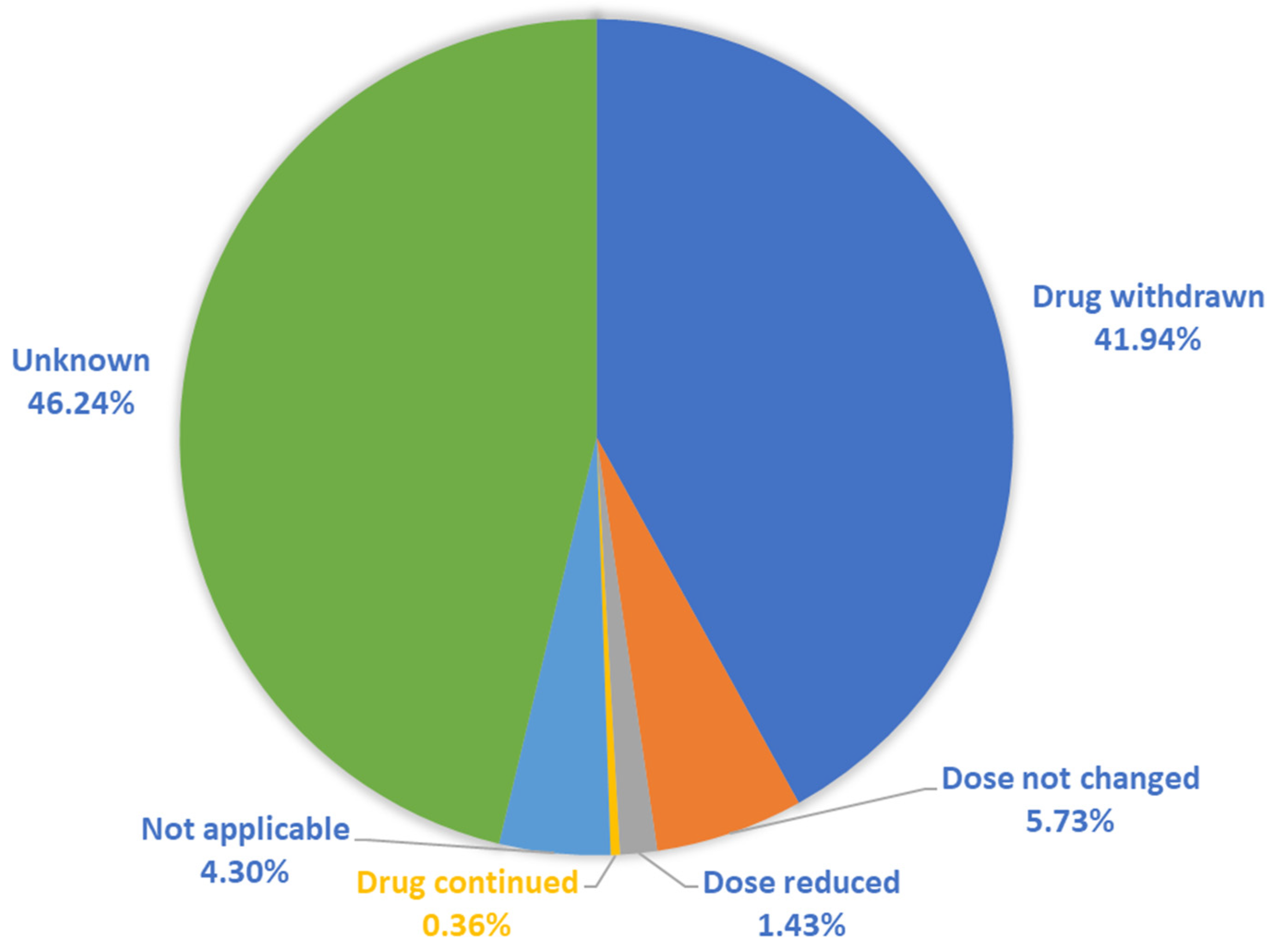
2.4. Seriousness and Actions Taken for Antimicrobial-Related ADEs
2.5. Types of Antimicrobial-Related ADEs
2.6. The Most Commonly Reported ADEs and Their Corresponding Antimicrobials
2.7. The Most Consumed Antibiotic and Their Corresponding ADEs
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Setting
4.3. Search Criteria
4.4. Data Extraction
4.5. Data Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Suyagh, M.; Farah, D.; Abu Farha, R. Pharmacist’s knowledge, practice and attitudes toward pharmacovigilance and adverse drug reactions reporting process. Saudi Pharm. J. SPJ Off. Publ. Saudi Pharm. Soc. 2015, 23, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Beijer, H.J.; de Blaey, C.J. Hospitalisations caused by adverse drug reactions (ADR): A meta-analysis of observational studies. Pharm. World Sci. PWS 2002, 24, 46–54. [Google Scholar] [CrossRef]
- Leape, L.L.; Brennan, T.A.; Laird, N.; Lawthers, A.G.; Localio, A.R.; Barnes, B.A.; Hebert, L.; Newhouse, J.P.; Weiler, P.C.; Hiatt, H. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N. Engl. J. Med. 1991, 324, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Committee of Experts on Management of Safety and Quality in Health Care (CEMSQHC). Expert Group on Safe Medication Practices: Glossary of Terms Related to Patient and Medication Safety; Council of Europe: Strasbourg, France, 2005. [Google Scholar]
- Leape, L.L.; Kabcenell, A.I.; Gandhi, T.K.; Carver, P.; Nolan, T.W.; Berwick, D.M. Reducing adverse drug events: Lessons from a breakthrough series collaborative. Jt. Comm. J. Qual. Improv. 2000, 26, 321–331. [Google Scholar] [CrossRef]
- Mjörndal, T.; Boman, M.D.; Hägg, S.; Bäckström, M.; Wiholm, B.E.; Wahlin, A.; Dahlqvist, R. Adverse drug reactions as a cause for admissions to a department of internal medicine. Pharmacoepidemiol. Drug Saf. 2002, 11, 65–72. [Google Scholar] [CrossRef]
- Wester, K.; Jönsson, A.K.; Spigset, O.; Druid, H.; Hägg, S. Incidence of fatal adverse drug reactions: A population based study. Br. J. Clin. Pharmacol. 2008, 65, 573–579. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Planning for the Global Patient Safety Challenge on Medication Safety. Available online: https://www.who.int/patientsafety/medication-safety/planning-consultation/en/ (accessed on 16 March 2023).
- Pirmohamed, M.; James, S.; Meakin, S.; Green, C.; Scott, A.K.; Walley, T.J.; Farrar, K.; Park, B.K.; Breckenridge, A.M. Adverse drug reactions as cause of admission to hospital: Prospective analysis of 18 820 patients. BMJ 2004, 329, 15–19. [Google Scholar] [CrossRef]
- Moore, N.; Lecointre, D.; Noblet, C.; Mabille, M. Frequency and cost of serious adverse drug reactions in a department of general medicine. Br. J. Clin. Pharmacol. 1998, 45, 301–308. [Google Scholar] [CrossRef]
- WHO. What is Pharmacovigilance? Available online: https://www.who.int/teams/regulation-prequalification/regulation-and-safety/pharmacovigilance#:~:text=Pharmacovigilance%20is%20the%20science%20and,they%20are%20authorized%20for%20use (accessed on 8 March 2023).
- Kumar, S.; Baldi, A. Pharmacovigilance in india: Perspectives and prospects. J. Drug Deliv. Ther. 2013, 3, 237–246. [Google Scholar] [CrossRef]
- Institute of Medicine Committee on Quality of Health Care in America. To Err is Human: Building a Safer Health System; Kohn, L.T., Corrigan, J.M., Donaldson, M.S., Eds.; National Academies Press: Washington, DC, USA, 2000.
- Lazarou, J.; Pomeranz, B.H.; Corey, P.N. Incidence of adverse drug reactions in hospitalized patients: A meta-analysis of prospective studies. JAMA 1998, 279, 1200–1205. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.T.; Modesto, A.C.F.; Amaral, R.G.; Lopes, F.M. Hospitalizations and deaths related to adverse drug events worldwide: Systematic review of studies with national coverage. Eur. J. Clin. Pharmacol. 2022, 78, 435–466. [Google Scholar] [CrossRef] [PubMed]
- Laureau, M.; Vuillot, O.; Gourhant, V.; Perier, D.; Pinzani, V.; Lohan, L.; Faucanie, M.; Macioce, V.; Marin, G.; Giraud, I.; et al. Adverse Drug Events Detected by Clinical Pharmacists in an Emergency Department: A Prospective Monocentric Observational Study. J. Patient Saf. 2021, 17, e1040–e1049. [Google Scholar] [CrossRef] [PubMed]
- Al Damen, L.; Basheti, I. Preventability analysis of adverse drug reactions in a Jordanian hospital: A prospective observational study. Int. J. Clin. Pharm. 2019, 41, 1599–1610. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, L.A.; Winterstein, A.G.; Søndergaard, B.; Haugbølle, L.S.; Melander, A. Systematic review of the incidence and characteristics of preventable adverse drug events in ambulatory care. Ann. Pharmacother. 2007, 41, 1411–1426. [Google Scholar] [CrossRef] [PubMed]
- Winterstein, A.G.; Hatton, R.C.; Gonzalez-Rothi, R.; Johns, T.E.; Segal, R. Identifying clinically significant preventable adverse drug events through a hospital’s database of adverse drug reaction reports. Am. J. Health-Syst. Pharm. AJHP Off. J. Am. Soc. Health-Syst. Pharm. 2002, 59, 1742–1749. [Google Scholar] [CrossRef]
- Davies, E.C.; Green, C.F.; Mottram, D.R.; Rowe, P.H.; Pirmohamed, M. Emergency re-admissions to hospital due to adverse drug reactions within 1 year of the index admission. Br. J. Clin. Pharmacol. 2010, 70, 749–755. [Google Scholar] [CrossRef]
- Al Rabayah, A.A.; Hanoun, E.M.; Al Rumman, R.H. Assessing knowledge, attitude, and practices of health-care providers toward pharmacovigilance and adverse drug reaction reporting at a comprehensive cancer center in Jordan. Perspect. Clin. Res. 2019, 10, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Scripcaru, G.; Mateus, C.; Nunes, C. Adverse drug events-Analysis of a decade. A Portuguese case-study, from 2004 to 2013 using hospital database. PLoS ONE 2017, 12, e0178626. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, T.; Sakuma, M.; Matsui, K.; Kuramoto, N.; Toshiro, J.; Murakami, J.; Fukui, T.; Saito, M.; Hiraide, A.; Bates, D.W. Incidence of adverse drug events and medication errors in Japan: The JADE study. J. Gen. Intern. Med. 2011, 26, 148–153. [Google Scholar] [CrossRef]
- Tamma, P.D.; Avdic, E.; Li, D.X.; Dzintars, K.; Cosgrove, S.E. Association of Adverse Events With Antibiotic Use in Hospitalized Patients. JAMA Intern. Med. 2017, 177, 1308–1315. [Google Scholar] [CrossRef] [PubMed]
- Geller, A.I.; Lovegrove, M.C.; Shehab, N.; Hicks, L.A.; Sapiano, M.R.P.; Budnitz, D.S. National Estimates of Emergency Department Visits for Antibiotic Adverse Events Among Adults-United States, 2011–2015. J. Gen. Intern. Med. 2018, 33, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [CrossRef] [PubMed]
- Ampadu, H.H.; Hoekman, J.; de Bruin, M.L.; Pal, S.N.; Olsson, S.; Sartori, D.; Leufkens, H.G.; Dodoo, A.N. Adverse Drug Reaction Reporting in Africa and a Comparison of Individual Case Safety Report Characteristics Between Africa and the Rest of the World: Analyses of Spontaneous Reports in VigiBase®. Drug Saf. 2016, 39, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Habarugira, J.M.V.; Figueras, A. Antimicrobial stewardship: Can we add pharmacovigilance networks to the toolbox? Eur. J. Clin. Pharmacol. 2021, 77, 787–790. [Google Scholar] [CrossRef]
- Dellit, T.H.; Owens, R.C.; McGowan, J.E., Jr.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Carpenter, C.F.; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2007, 44, 159–177. [Google Scholar] [CrossRef]
- Bauer, K.A.; Kullar, R.; Gilchrist, M.; File, T.M., Jr. Antibiotics and adverse events: The role of antimicrobial stewardship programs in ‘doing no harm’. Curr. Opin. Infect. Dis. 2019, 32, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Venulet, J.; Helling-Borda, M. WHO’s international drug monitoring--the formative years, 1968–1975: Preparatory, pilot and early operational phases. Drug Saf. 2010, 33, e1–e23. [Google Scholar] [CrossRef]
- UMC. The WHO Programme for International Drug Monitoring. Available online: https://who-umc.org/about-the-who-programme-for-international-drug-monitoring/ (accessed on 7 February 2023).
- HMA. European Medecines Agency. In Guideline on Good Pharmacovigilance Practices (GVP). Available online: https://www.ema.europa.eu/en/human-regulatory/post-authorisation/pharmacovigilance/good-pharmacovigilance-practices (accessed on 7 February 2023).
- UMC (Uppsala Monitoring Centre). VigiBase. Available online: https://who-umc.org/vigibase/ (accessed on 3 February 2023).
- Al-Azzam, S.; Mhaidat, N.M.; Banat, H.A.; Alfaour, M.; Ahmad, D.S.; Muller, A.; Al-Nuseirat, A.; Lattyak, E.A.; Conway, B.R.; Aldeyab, M.A. An Assessment of the Impact of Coronavirus Disease (COVID-19) Pandemic on National Antimicrobial Consumption in Jordan. Antibiotics 2021, 10, 690. [Google Scholar] [CrossRef]
- Abu Hammour, K.; El-Dahiyat, F.; Abu Farha, R. Health care professionals knowledge and perception of pharmacovigilance in a tertiary care teaching hospital in Amman, Jordan. J. Eval. Clin. Pract. 2017, 23, 608–613. [Google Scholar] [CrossRef]
- Mukattash, T.L.; Alwadi, M.W.; Abu-Farha, R.K.; Jarab, A.S.; Al-Zubiedi, S.A.; Alwedyan, T. Knowledge, Attitudes, and Practices of Pharmacovigilance and ADRs Spontaneous Reporting Among Pediatricians and Pediatric Residents in Jordan. Curr. Clin. Pharmacol. 2018, 13, 45–54. [Google Scholar] [CrossRef]
- Shroukh, W.A.; Shakhatreh, F.M.; Yasein, N.A.; Sharkas, G.F. A survey on the knowledge, attitudes and practices of physicians towards pharmacovigilance in Jordanian health centres. Int. Health 2018, 10, 363–370. [Google Scholar] [CrossRef]
- Thomas, F.; Abiri, O.T.; Komeh, J.P.; Conteh, T.A.; Bah, A.J.; Kanu, J.S.; Terry, R.; Abrahamyan, A.; Thekkur, P.; Zachariah, R. Inconsistent Country-Wide Reporting of Adverse Drug Reactions to Antimicrobials in Sierra Leone (2017–2021): A Wake-Up Call to Improve Reporting. Int. J. Environ. Res. Public Health 2022, 19, 3264. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Resistance—An Overlooked Adverse Event. Available online: https://www.who-mc.org/media/2775/web_uppsalareports_issue74.pdf (accessed on 28 January 2023).
- Habarugira, J.M.V.; Figueras, A. Pharmacovigilance network as an additional tool for the surveillance of antimicrobial resistance. Pharmacoepidemiol. Drug Saf. 2021, 30, 1123–1131. [Google Scholar] [CrossRef] [PubMed]
- Rational Drug Use & Pharmacovigilance Department. Jordan Pharmacovigilance Database Analysis. Available online: http://www.jfda.jo/EchoBusV3.0/SystemAssets/Documents/AR/DRUGD/Pharmacovigilance%20Booklet.pdf (accessed on 28 January 2023).
- MedDRA. Medical Dictionary for Regulatory Activities. Available online: https://www.meddra.org/how-to-use/basics/hierarchy (accessed on 24 January 2023).



{kind=link}
{kind=link}
| Number | Percentage (%) | |
|---|---|---|
| Age | ||
| 0–17 | 68 | 24.37 |
| 18–64 | 121 | 43.37 |
| ≥ 65 | 24 | 8.6 |
| NA | 66 | 23.66 |
| Gender | ||
| Female | 136 | 48.75 |
| Male | 100 | 35.84 |
| NA | 43 | 15.41 |
| Reporter qualification | ||
| Physician | 103 | 36.92 |
| Pharmacist | 84 | 30.10 |
| Other Health Professionals | 36 | 12.90 |
| Consumer/Non-Health Professional | 22 | 7.89 |
| Unknown | 34 | 12.19 |
| Chemical Subgroup | Number of Products | Number of ADEs |
|---|---|---|
| Antifungals | 12 | 35 |
| Antivirals | 8 | 24 |
| Fluoroquinolones | 5 | 54 |
| Third-generation cephalosporines | 5 | 48 |
| Carbapenems | 4 | 42 |
| Macrolides | 3 | 36 |
| Other beta-lactam antibacterials | 3 | 15 |
| Tetracyclines | 2 | 101 |
| Second-generation cephalosporins | 2 | 26 |
| Aminoglycosides | 2 | 3 |
| Glycopeptide | 1 | 28 |
| First-generation cephalosporins | 1 | 7 |
| Penicillin with extended spectrum | 1 | 6 |
| Beta-lactamase resistant penicillin | 1 | 3 |
| Polymyxins | 1 | 23 |
| Antimalarials | 1 | 24 |
| Combinations of penicillin, incl. beta-lactamase inhibitors | 1 | 24 |
| Other cephalosporins and penems | 1 | 15 |
| Sulfonamides and trimethoprim | 1 | 7 |
| Aminoquinolines | 1 | 3 |
| Combinations of antibacterial | 1 | 8 |
| Other antibacterial | 1 | 1 |
| Antimycobacterial | 1 | 5 |
| Antiprotozoals | 1 | 1 |
| Total | 60 | 539 |
| Number | Percentage (%) | |
|---|---|---|
| Seriousness of ADE | ||
| Yes | 120 | 43.01 |
| No | 132 | 47.31 |
| Unknown | 27 | 9.68 |
| Seriousness criteria of ADE | ||
| Caused/prolonged hospitalization | 58 | 20.79 |
| Death | 13 | 4.66 |
| Life-threatening | 10 | 3.58 |
| Disabling/incapacitating | 1 | 0.36 |
| Congenital anomaly/birth defect | 1 | 0.36 |
| Other medically important conditions | 37 | 13.26 |
| Unknown | 159 | 56.99 |
| Adverse Drug Events | Number of ADEs | Percentage of the Total ADEs (%) |
|---|---|---|
| Total ADEs | 539 | 100 |
| Skin and subcutaneous tissue disorders | 105 | 19.48 |
| Rash | 58 | 10.76 |
| Urticaria | 22 | 4.08 |
| Pruritus | 14 | 2.60 |
| Erythema | 11 | 2.04 |
| General disorders and administration condition | 88 | 16.33 |
| Facial edema/periorbital edema/peripheral edema | 28 | 5.19 |
| Drug ineffective | 28 | 5.19 |
| Asthenia/fatigue/malaise | 11 | 2.04 |
| Fever | 9 | 1.67 |
| Other (chills, sweating, hotness, flushing, pallor, jaundice, and lymphadenopathy) | 12 | 2.23 |
| Gastrointestinal disorders | 69 | 12.8 |
| Vomiting | 23 | 4.27 |
| Abdominal pain | 15 | 2.78 |
| Diarrhea | 12 | 2.23 |
| Nausea | 7 | 1.30 |
| Other (eructation, constipation, gastritis, hematemesis, taste disorders, tongue pigmentation, and pancreatitis) | 12 | 2.23 |
| Nervous system disorder | 43 | 7.98 |
| Seizure | 13 | 2.41 |
| Dizziness | 8 | 1.48 |
| Headache | 6 | 1.11 |
| Altered LOC | 5 | 0.93 |
| Other (stroke, gait disturbance, memory impairment, paresthesia, photophobia, somnolence, and others) | 11 | 2.04 |
| Injury, poisoning, and procedure complications | 34 | 6.31 |
| Off-label use | 13 | 2.41 |
| Incorrect route of administration | 10 | 1.86 |
| Unapproved indication | 6 | 1.11 |
| Overdose | 2 | 0.37 |
| Drug interaction | 2 | 0.37 |
| Treatment non-compliance | 1 | 0.19 |
| Renal and urinary disorders (AKI, abnormal renal function, abnormal electrolytes, glycosuria, and others) | 30 | 5.57 |
| Cardiac disorders | 28 | 5.19 |
| Hypotension | 10 | 1.86 |
| Palpitations | 4 | 0.74 |
| Chest pain or discomfort | 4 | 0.74 |
| Myocardial infarction | 3 | 0.56 |
| Tachycardia | 3 | 0.56 |
| Other (syncope, AV block, cardiac arrest, syncope) | 4 | 0.74 |
| Blood and lymphatic system disorders (anemia, leukocytosis, leukopenia, thrombocytosis, thrombocytopenia, bleeding, and coagulation) | 27 | 5.01 |
| Immune system disorders (allergy and hypersensitivity) | 22 | 4.08 |
| Respiratory, thoracic, and mediastinal disorders | 21 | 3.90 |
| Dyspnea | 14 | 2.60 |
| Other (cough, cyanosis, tachypnea, and apnea) | 7 | 1.30 |
| Pregnancy, puerperium, and perinatal conditions (fetal exposure, premature labor, and others) | 21 | 3.90 |
| Musculoskeletal and connective tissue disorders (arthralgia, myalgia, and stiffness) | 9 | 1.67 |
| Product issues | 9 | 1.67 |
| Hepatobiliary disorders (AST, ALT, and bilirubin) | 9 | 1.67 |
| Metabolism and nutrition disorders (hypoglycemia) | 7 | 1.30 |
| Eye disorders (blindness, visual impairment, corneal edema, keratitis, and scleromalacia) | 6 | 1.11 |
| Psychiatric disorders (narcolepsy and suicide attempt) | 3 | 0.56 |
| Ear and labyrinth disorders (vertigo, hearing impairment, and others) | 3 | 0.56 |
| Death * | 3 | 0.56 |
| Reproductive system and breast disorders (mastoiditis) | 2 | 0.37 |
| Antibiotic Group | Rash (n = 58) | Renal and Urinary Disorders (n = 30) | Facial Edema/Periorbital Edema/Peripheral Edema (n = 28) | Drug Ineffective (n = 28) | Blood and lymphatic System Disorders (n = 27) | Vomiting (n = 23) | Urticaria (n = 22) | Immune System Disorders (Allergy and Hypersensitivity) (n = 22) | Pregnancy, Puerperium, and Perinatal Conditions (n = 21) |
|---|---|---|---|---|---|---|---|---|---|
| Aminoglycosides | - | - | - | 3 | - | - | - | - | - |
| Aminoquinolines | - | - | - | - | - | - | 1 | 1 | |
| Antifungals | 2 | 1 | 1 | 3 | 3 | - | - | - | - |
| Antimalarials | 5 | - | - | - | - | - | - | - | 7 |
| Antimycobacterial | 2 | - | - | - | 1 | - | 1 | - | - |
| Antiprotozoals | 1 | - | - | - | - | - | - | - | - |
| Antivirals | - | 13 | - | 1 | 8 | - | - | - | - |
| Beta-lactamase Resistant penicillin | - | - | - | - | - | 1 | - | - | - |
| Carbapenems | 1 | - | - | 9 | - | 7 | - | 1 | 1 |
| Tetracyclines | 7 | - | 15 | 8 | 6 | 1 | 17 | 8 | - |
| Fluoroquinolones | 6 | - | 5 | - | 3 | - | 2 | 1 | - |
| Penicillin with extended spectrum | 2 | - | - | - | - | 1 | - | - | - |
| Combinations of penicillin, incl. beta-lactamase inhibitors | 1 | - | - | - | - | 2 | - | - | - |
| First-generation cephalosporins | 3 | - | - | - | - | 1 | - | - | - |
| Second-generation cephalosporins | 4 | - | 1 | - | 2 | 1 | - | 2 | 8 |
| Third-generation cephalosporines | 11 | - | 3 | 3 | - | 3 | 2 | 2 | 4 |
| Other cephalosporins and penems | - | - | - | - | 2 | 1 | - | - | - |
| Glycopeptide | 4 | 11 | 1 | 1 | 1 | 1 | - | 4 | - |
| Macrolides | - | - | 1 | - | - | 4 | - | 1 | - |
| Other beta-lactam antibacterials | 4 | 1 | - | - | - | - | 1 | - | |
| Polymyxins | 2 | 3 | - | - | 1 | - | - | 1 | - |
| Sulfonamides and trimethoprim | 2 | 1 | - | - | - | - | - | - | - |
| Combinations of antibacterial | 1 | - | 1 | - | - | - | - | - | - |
| Amoxicillin/Clavulanic Acid | Amoxicillin | Azithromycin | Cefuroxime | Clarithromycin | Ciprofloxacin | Cefixime | Doxycycline | Clindamycin | Levofloxacin | |
|---|---|---|---|---|---|---|---|---|---|---|
| AWaRe Classification | ACCESS | ACCESS | WATCH | WATCH | WATCH | WATCH | WATCH | ACCESS | ACCESS | WATCH |
| Gastrointestinal disorders | 11 | 2 | 4 | 3 | 10 | 7 | - | No Adverse Reactions | No Adverse Reactions | - |
| Abdominal pain | 2 | - | 1 | - | 3 | 4 | - | - | ||
| Abnormal taste | - | - | - | - | 1 | - | - | - | ||
| Belching | - | - | - | 1 | - | 2 | - | - | ||
| Constipation | 1 | - | - | - | - | - | - | - | ||
| Diarrhea | 4 | 1 | 1 | 1 | 1 | 1 | - | - | ||
| Gastritis | - | - | - | - | 1 | - | - | - | ||
| Hematemesis | 2 | - | - | - | - | - | - | - | ||
| Nausea | 1 | - | 1 | - | 1 | - | - | - | ||
| Pancreatitis | - | - | - | - | 1 | - | - | - | ||
| Vomiting | 1 | 1 | 1 | 1 | 2 | - | - | - | ||
| General disorders | 2 | - | 1 | 1 | - | 2 | - | 3 | ||
| Facial edema/periorbital edema/peripheral edema | - | - | 1 | 1 | - | 1 | - | 1 | ||
| Fever | 2 | - | - | - | - | - | - | - | ||
| Hemorrhage | - | - | - | - | - | - | - | 2 | ||
| Hot flush | - | - | - | - | - | 1 | - | - | ||
| Lymphadenopathy | - | - | - | - | - | - | - | - | ||
| Injury, poisoning, and procedure complications | 2 | 1 | 5 | - | - | - | 2 | 3 | ||
| Incorrect route of administration | 1 | - | - | - | - | - | 1 | 1 | ||
| Off-label use | - | 1 | 5 | - | - | - | 1 | |||
| Overdose | 1 | - | - | - | - | - | ||||
| Drug interaction | - | - | - | - | - | - | - | 2 | ||
| Nervous system disorder | 3 | - | - | 1 | 2 | 4 | - | - | ||
| Dizziness | 1 | - | - | - | 2 | 1 | - | - | ||
| Headache | 1 | - | - | - | - | - | - | |||
| Loss of consciousness | 1 | - | - | 1 | - | 3 | - | - | ||
| Respiratory, thoracic, and mediastinal disorders | 1 | - | 1 | 2 | - | - | - | - | ||
| Apnea | - | - | 1 | - | - | - | - | |||
| Arthralgia | 1 | - | - | - | - | - | ||||
| Cardiac disorders | - | - | 4 | 2 | 1 | - | - | - | ||
| Chest pain | - | - | 2 | 1 | - | - | - | |||
| Dyspnea | - | - | 1 | 1 | - | - | - | - | ||
| Hypotension | - | - | 1 | 2 | - | - | - | - | ||
| Palpitation | - | - | 1 | - | - | - | - | |||
| Skin and subcutaneous tissue disorders | 1 | 2 | - | 4 | - | 8 | 2 | 1 | ||
| Erythema | - | - | - | - | - | 1 | - | - | ||
| Pruritus | - | - | - | - | - | 3 | - | - | ||
| Rash | 1 | 2 | - | 4 | - | 2 | 2 | 1 | ||
| Urticaria | - | - | - | - | - | 2 | - | - | ||
| Lymphadenopathy | - | - | - | - | - | - | - | - | ||
| Ear and labyrinth disorders (hypoacusis) | - | - | - | - | 1 | - | - | - | ||
| Hepatobiliary disorders (abnormal INR) | - | - | - | - | - | - | - | 1 | ||
| Immune system disorders (hypersensitivity) | - | - | 1 | 2 | - | - | - | 1 | ||
| Metabolism and nutrition disorders (hypoglycemia) | - | - | - | - | 5 | - | - | |||
| Product issues | - | - | 1 | - | - | - | - | |||
| Pregnancy, puerperium, and perinatal conditions | - | - | - | 8 | - | - | 3 | - | ||
| Psychiatric disorders (suicide attempt) | 1 | - | - | 1 | - | - | - | - | ||
| Reproductive system and breast disorders (mastoiditis) | 1 | 1 | - | - | - | - | ||||
| Total ADEs | 22 | 6 | 17 | 24 | 14 | 26 | 7 | 0 | 0 | 9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mhaidat, N.M.; Al-Azzam, S.; Banat, H.A.; Jaber, J.M.; Araydah, M.; Alshogran, O.Y.; Aldeyab, M.A. Reporting Antimicrobial-Related Adverse Drug Events in Jordan: An Analysis from the VigiBase Database. Antibiotics 2023, 12, 624. https://doi.org/10.3390/antibiotics12030624
Mhaidat NM, Al-Azzam S, Banat HA, Jaber JM, Araydah M, Alshogran OY, Aldeyab MA. Reporting Antimicrobial-Related Adverse Drug Events in Jordan: An Analysis from the VigiBase Database. Antibiotics. 2023; 12(3):624. https://doi.org/10.3390/antibiotics12030624
Chicago/Turabian StyleMhaidat, Nizar Mahmoud, Sayer Al-Azzam, Hayaa Abdallah Banat, Jaber Mohammad Jaber, Mohammad Araydah, Osama Y. Alshogran, and Mamoon A. Aldeyab. 2023. "Reporting Antimicrobial-Related Adverse Drug Events in Jordan: An Analysis from the VigiBase Database" Antibiotics 12, no. 3: 624. https://doi.org/10.3390/antibiotics12030624
APA StyleMhaidat, N. M., Al-Azzam, S., Banat, H. A., Jaber, J. M., Araydah, M., Alshogran, O. Y., & Aldeyab, M. A. (2023). Reporting Antimicrobial-Related Adverse Drug Events in Jordan: An Analysis from the VigiBase Database. Antibiotics, 12(3), 624. https://doi.org/10.3390/antibiotics12030624