Abstract
Background: Serratia marcescens (SM) is a Gram-negative pathogen discovered by Italian pharmacist, Bizio, in 1819. According to the literature, S. marcescens is resistant to a wide range of antibiotics, including penicillin, cephalosporin, tetracycline, macrolide, nitrofurantoin, and colistin. We conducted a systematic review of published reports, determined what invasive infections could cause SM, and established the most appropriate antibiotic therapy. Methods: We registered this systematic review on the PROSPERO registry of systematic reviews–meta-analyses before we started our research (registration number CRD42022323159). The online searches of published studies were implemented via MEDLINE, the Cochrane Central Register of Controlled Trials, EBSCO, Scopus, Google Scholar, SCIndex, and the registry of clinical studies of human participants (ClinicalTrials.gov). Results: Our study included 32 published articles (9 case series and 23 case reports). There were 57 individual cases, respectively. The oldest patient was 97 years and the youngest patient was a newborn. S. marcescens was, in most cases, isolated from blood followed by urine and cerebrospinal fluid. In most cases, sensitivity was tested to cotrimoxazole (from 27 isolates, 10 showed resistance) followed by gentamicin (from 26 isolates, 3 showed resistance) as well as amikacin (from 21 isolates, none showed resistance). Patients died from an infection in 21 cases (31%). Conclusions: Treatment of SM infections should include carbapenems or aminoglycosides in combination with third-generation (and eventually fourth-generation) cephalosporin. Cotrimoxazole should be considered in cases of uncomplicated urinary infections.
1. Introduction
Serratia marcescens (SM), a Gram-negative pathogen, belongs to the genus Serratia and the Yersiniaceae family. It was discovered by Bartolomeo Bizio in 1819. Bizio, an Italian pharmacist and later a professor at the University of Padua, Italy, reported a blood-like pigmentation on polenta and rice. He classified the microorganism as a fungus and named it S. marcescens. Serratia was chosen in honor of Serafino Serrati, a physicist who ran the first steamboat on the Arno River in 1787, while marcescens comes from the Latin word “to decay” [1,2,3]. SM has the ability to produce red-pigmented prodigiosin [4]. Nowadays, no pigmented strains of SM are predominant over pigmented strains, especially in compromised patients. Serratia marcescens is usually isolated from blood and cultivated on blood agar or with selective culture methods (MacConcey or chromogenic agars) [4].
SM is usually resistant to antibiotics by producing deoxyribonuclease (DNase), lipase, and gelatinase [4]. S. marcescens also produces a pore-forming hemolysin, ShIA, which can cause cell cytotoxicity and the release of inflammatory mediators [5]. Serratia marcescens causes both opportunistic and nosocomial infections as well as a wide range of infections in both adults and children. The urinary catheter is thought to be the main entry point for infections, such as intubation and the central venous catheter [4]. Catheter colonization increases bacterial survival, especially in biofilm communities. Biofilm also increases resistance to antibiotics because it prevents their penetration [6]. Different types of infection by SM were described, such as pneumonia, sepsis, wound infection, meningitis, endocarditis, ocular infections, etc. [7,8,9,10].
SM, along with the Enterobacter spp., Citrobacter freundii, Providencia spp., and Morganella morganii, makes up the ‘ESCPM’ group and may express high levels of AmpC [11]. According to the literature, S. marcescens is resistant to a wide range of antibiotics, including penicillin, cephalosporin, tetracycline, macrolide, nitrofurantoin, and colistin. In the past, antibiotics, such as fluoroquinolones, aminoglycosides, and third-generation cephalosporins, were the bases for the treatment of S. marcescens infections. However, many clinical isolates of S. marcescens now show multiple forms of antimicrobial resistance to these antibiotics [4].
Guidelines for the treatment of Serratia marcescens infections do not exist, mostly because the relevant publications were based on individual case reports. We conducted a systematic review of the published reports and determined what invasive infections could be caused by SM, as well as established what the most appropriate antibiotic therapy is.
2. Results
Our study included 32 published articles (9 case series and 23 case reports) (Figure 1). There were 57 individual cases, respectively. The oldest patient was 97 years old and the youngest patient was a newborn. As for the age distribution of the patients, there were 3 (5%) newborns (<28 days), 8 (14%) infants (1 month–1 year), 1 (1%) preschool child (3–5 years), 17 (30%) adults (18–64 years), and 10 (17%) elderly adults (>65 years). In 15 (26%) cases, age was not reported. Female patients were represented with 13 (22%) cases, and male patients were represented with 23 (40%) cases. Gender was not reported in 21 (37%) cases. Most of the cases were described in the United Kingdom (n = 13; 22%) followed by the United States of America and Turkey (n = 11; 19%) equally. Three cases of Serratia marcescens infections were described in Brazil, Germany, and Denmark. Two cases of SM infections were detected in Switzerland, Korea, Greece, and France. In Chile, Italy, Taiwan, Japan, and Argentina, one case of SM infection was detected. All patients were hospitalized. The longest duration of the study was reported in France (4 years). Characteristics of the included studies are shown in Table 1.
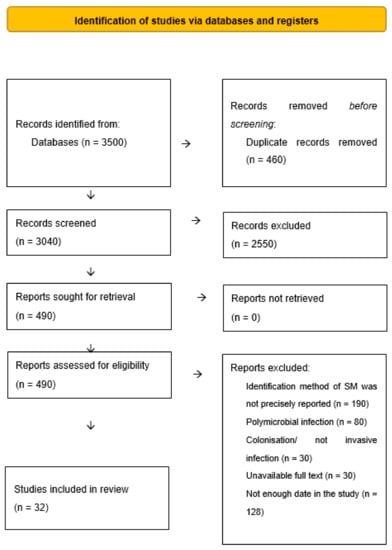
Figure 1.
Selection of the studies.

Table 1.
Overview of the reported Serratia marcescens cases.
2.1. Site of S. marcescens Isolation
S. marcescens was, in most cases, isolated from blood (n = 26; 45%), followed by urine (n = 8; 14%), the cerebrospinal fluid (n = 7; 12%), and part of the tissue, e.g., the thyroid gland, leg, meninges, myocardium, fascia (n = 6; 10%). From corpus vitreum, S. marcescens was isolated in 6 cases (10%); from wound pus, SM was isolated in 5 cases (8%); from bronchoalveolar lavage and sputum, SM was isolated in 4 cases each (6%). Moreover, SM was isolated from bone (n = 3; 5%), peritoneal fluid (n = 2; 3%), as well as thoracic fluid and vaginal discharge (n = 1; 1%).
2.2. Method for S. marcescens Identification
The most common method for SM identification was colony morphology in combination with the biochemical system (n = 18; 31%). Only colony morphology was used in 14 cases (24%) and only the biochemical system was used in 11 cases (19%). The PCR assay was reported in 5 cases (8%); a combination of the biochemical system, MALDI-TOF mass spectrometry, and gene sequencing was used in 4 cases (6%); colony morphology and gene sequencing was used in 2 cases (3%).
The biochemical system and MALDI-TOF mass spectrometry, the biochemical systems, and gene sequencing, as well as MALDI-TOF mass spectrometry and gene sequencing were represented in one case.
2.3. Clinical Manifestation of S. marcescens Infection
In 22 patients (38%), signs of systemic infection were present; in other patients, signs were not reported (62%). The maximum level of C-reactive protein (CRP) was reported in six patients (10%). The maximum reported value of CRP was 405 mg/L. A count of white blood cells (WBC) was reported in 8 patients (14%) with a maximum level of about 43.300/mm3. In 12 cases (21%), the results from morphological diagnostics (e.g., ultrasound, radiography, CT) were obtained.
2.4. Sensitivity of S. marcescens to Antibiotics
In 42 patients, the susceptibility of S. marcescens to antibiotics was tested (73%) and the results are shown in Figure 2. In most cases, sensitivity was tested to cotrimoxazole (from 27 isolates, 10 showed resistance) followed by gentamicin (from 26 isolates, 3 showed resistance), as well as amikacin (from 21 isolates, none showed resistance). Isolates were also tested for ciprofloxacin (from 19 isolates, 2 showed resistance) and cefotaxime (from 18 isolates, 13 showed resistance). The isolates were tested on ampicillin, tetracycline, ceftazidime, cefalotin, ceftriaxone, imipenem, etc.
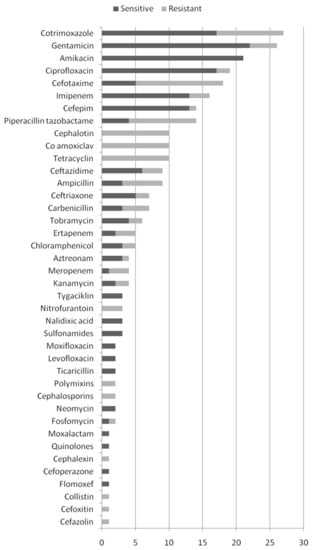
Figure 2.
Susceptibility of S. marcescens to antibiotics.
2.5. Antibiotics Used in the Treatment of Serratia marcescens Infection
In 15 cases (26%), antibiotic regimens were not reported. Only four patients were treated with one antibiotic. The most used antibiotic for the treatment of Serratia marcescens infection was ciprofloxacin (n = 17; 29%), followed by amikacin (n = 14; 24%) and gentamicin (n = 11; 19%). Antibiotic treatment is shown in Figure 3.
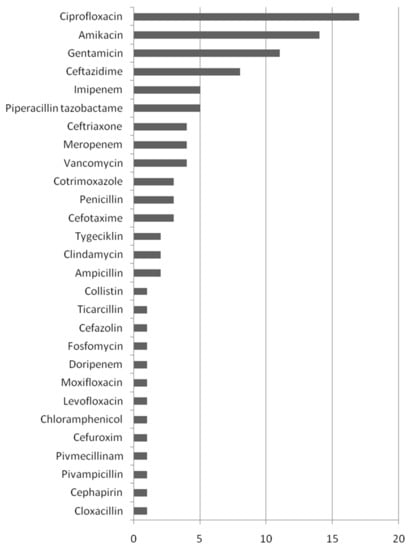
Figure 3.
Antibiotics used for the treatment of S. marcescens infections.
2.6. Treatment Outcomes
About half of the patients recovered completely (n = 29; 50%). Partial recovery was reported in five cases. In one case, the patient was cured of the infection but died from an underlying disease. Patients died from infections in 21 cases (31%). In one case, the outcome was not reported.
3. Discussion
Our results showed that Serratia marcescens may cause different types of infections in males and females, elderly patients, as well as newborns. SM was most frequently isolated from blood, urine, cerebrospinal fluid, and some tissues. Colony morphology in combination with the biochemical system (31%) was the most frequently used method for SM identification followed by only colony morphology and only the biochemical system. In most cases, isolates were susceptible to gentamicin, cotrimoxazole, amikacin, ciprofloxacin, and cefotaxime. Ciprofloxacin was the most frequently used antibiotic in the therapy of SM infections. The death rate was high (31%), which is what is worrying.
Serratia marcescens can produce a beta-lactamase, which influences resistance to the beta-lactam antibiotics and might complicate the therapy [4]. Carbapenem resistance in S. marcescens is associated with AmpC overexpression, Ambler class A production (KPC and SME), and B metallo-β-lactamase classes (MβLs; IMP, VIM). Serratia marcescens has carbapenem-hydrolyzing activity in the first production of KPC-2, and only in a few cases of KPC-3 and KPC-4 [19,23].
Aminoglycoside resistance is related to posttranscriptional methylation of 16S rRNA conferred by methyl transferases. To date, ten kinds of 16S rRNA methyl transferase genes (armA, rmtB, rmtA, rmtC, rmtE, rmtD, rmtF, rmtH, rmtG, and npmA) have been reported in Enterobacteriaceae. S. marcescens with rmtB, quinolone resistance genes, and various β-lactamase genes were also described [44]. Nowadays, gene sequencing is very popular for discovering antibiotic gene resistance and virulence factors of Serratia marcescens [45].
S. marcescens causes nosocomial infections in critically ill or immunocompromised patients, mostly in departments such as intensive care units [46]. SM can be found in soil, water, animals, plants, and insects [46]. There was an inverse relationship between virulence and the quantity of pigment (prodigiosin) produced [47]. In intensive care units, the most common reservoirs for infections are air-conditioning systems, washbasins, tap water, bronchoscopes, laryngoscopes, nebulizers, ventilation equipment, injectable solutions, liquid soap dispensers, etc. [46]. These are the reasons for the large number of hospital-related S. marcescens outbreaks [46].
There is no official therapy for SM infections. Results from our study showed sensitivity to gentamicin, cotrimoxazole, amikacin, ciprofloxacin, and cefotaxime. Sometimes gentamicin alone was the treatment of choice for SM infections but now it is more often used in combination with third-generation cephalosporins (e.g., cefotaxime) [4]. Trimethoprim-sulfamethoxazole (cotrimoxazole) is the most effective, especially for urinary tract infections. According to the literature, amikacin is active against gentamicin-resistant S. marcescens [4]. SM has a natural resistance to penicillin and first- and second-generation cephalosporin, tetracycline, macrolide, nitrofurantoin, and colistin [48]. When we look at the overall results, we notice that the therapy has changed over time; in the past, more aminoglycosides were prescribed. Today, it is colistin, tigecycline, and carbapenem.
Ciprofloxacin was the most frequently used antibiotic (29%) followed by amikacin and gentamicin. In most cases, ciprofloxacin was effective. According to the literature, ciprofloxacin use for the treatment of serious infections should be avoided due to its ability to develop resistance [4]. Amikacin and gentamicin were also frequently used. According to our results, carbapenems were not often used. According to some of the literature studies, it should be the antibiotic of choice [4,11,49]. This could be the reason for the mortality rate described in the literature according to our systematic review (31%). Third-generation cephalosporins (often combined with aminoglycosides) are the treatments of choice for uncomplicated infections. Fourth-generation cephalosporines are good treatment options where resistance to third-generation cephalosporins is evident [11]. They are active against AmpC chromosomal b-lactamase-producing strains as well as the treatment of ESBL-positive isolates [4]. According to the literature, piperacillin–tazobactam could also be an option for treating SM infections [50].
For the treatment of Serratia marcescens infections, in most cases, more than one antibiotic should be used, especially because of its ability to develop resistance [4]. Infections caused by SM could be fatal (according to our results in 31% of cases). According to the literature, the mortality rate is from 0% to 45% [4,51]. For this reason, infections caused by SM should be treated on time with the appropriate antibiotics.
The limitation of our systematic review involves the relatively small number of studies included. The second limitation was the reliability of the colony’s morphological identification as well as the biochemical identification of agents. More reliable methods, such as MALDI TOF or gene sequencing, were represented in smaller percentages of cases. Moreover, many cases (more than 50%) had high reporting biases, which may call into question the relevance of certain conclusions.
4. Materials and Methods
4.1. Data Sources
We registered this systematic review on the PROSPERO registry of systematic reviews–meta-analyses before we started our research (registration number CRD42022323159) [52].
An electronic database and collections of journals and books at the University Library, University of Kragujevac, Kragujevac, Serbia, were the bases for our search strategy in the identification of studies. The online searches of published studies were implemented via MEDLINE, the Cochrane Central Register of Controlled Trials, EBSCO, Scopus, Google Scholar, SCIndex, and the registry of clinical studies of human participants (ClinicalTrials.gov). Electronic databases were searched independently by three investigators: RZZ, MZ, and PC. The most extensive search strategy was made by RZZ on the MEDLINE database, i.e., ((Serratia Marcescens) AND (infection OR infections OR sepsis OR bacteremia OR pneumonia OR meningitis OR endocarditis OR osteomyelitis OR abscess OR peritonitis OR pericarditis OR pancreatitis OR pyelitis OR myocarditis OR arthritis OR bursitis OR endophthalmitis OR pyelonephritis OR septicemia OR meningoencephalitis OR urinary OR fasciitis) AND (case OR report OR series OR cohort OR observational OR case-control OR cross-sectional OR clinical trial) NOT (dermatitis OR keratitis OR ulcer OR scleritis OR conjunctivitis OR in vitro).
4.2. Participants and Study Eligibility Criteria
The inclusion criteria were as follows: type of study-case reports, case series, observational study, as well as clinical trial; characteristics of the participants—any age and gender with isolated Serratia marcescens as the only microorganism in the bodily fluids and tissues, identified by the following diagnostic methods: colony morphology, API, Vitek 2, or BD Phoenix biochemical systems, as well as matrix-assisted laser absorption ionization-time-of-flight mass spectrometry (MALDI-TOF MS) and specific PCR for S. marcescens. Exclusion criteria were as follows: review articles; cases of S. marcescens with non-human species; studies with incomplete dates. Papers were first assessed based on the titles and abstracts for eligibility, and then the full texts of the papers were read and analyzed. If all authors (RZZ, MZ, PC, MS, NZ, MS, MV, JN, VN, TV, JJ, DP, and SJ) agreed that the manuscript satisfied the inclusion criteria, it was further processed. In cases where the reviewers had different opinions about the eligibility of a study, the matter was resolved by the senior author (RZZ).
4.3. Interventions
The data from the studies included in the review were extracted to an Excel table with the following columns: publication ID, report ID, review author initials, design of the study, duration of the study, risk of bias, number of patients, age of patients, gender of patients, country, site of SM isolation, sampling method, method of SM identification, the maximal level of C-reactive protein, the maximal level of white blood cells, morphological diagnostics which confirmed invasive infection, presence of clinical sign of infection, antibiotics used, the outcome of antibiotic treatment, the resistance rate of SM to antibiotics.
The data were extracted by three investigators (RZZ, MZ, and PC) and the final extraction table was conducted by RZZ.
4.4. Data Analysis
All three investigators assessed the risk of bias (RZZ, MZ, and PC). The following sources of bias were accessed: reporting bias and attrition bias. The reporting bias was evaluated by checking what percentage of the target outcome was reported. For attrition bias, the number and percent of lost patients from the initial pool were estimated [53].
The categorical outcomes were the gender of patients, a method for SM identification, morphological diagnostics, outcomes of antibiotic treatment, adverse event rate, antibiotics used, as well as the resistance rate to SM. Continuous outcomes were the ages of patients, study duration, number of patients, the maximal level of C-reactive protein, and the maximal level of white blood cells.
5. Conclusions
Serratia marcescens infections should be taken seriously, especially because the bacterium causes high mortality and can lead to a high degree of resistance to antibiotics. The treatment of SM infections should include carbapenems or aminoglycosides in combination with third-generation (eventually fourth-generation cephalosporins). Cotrimoxazole should be considered in cases of uncomplicated urinary infections.
Author Contributions
Conceptualization, R.Z.Z. and M.Z.; methodology, P.C.; validation M.S. (Marko Spasic) and M.S. (Marija Sekulic); formal analysis, S.J. and N.Z.; investigation, V.R., J.N., T.V. and M.V.; writing—original draft preparation, J.J. and R.Z.Z.; writing—review and editing, R.Z.Z. and D.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
There are no available data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Khanna, A.; Khanna, M.; Aggarwal, A. Serratia marcescens—A rare opportunistic nosocomial pathogen and measures to limit its spread in hospitalized patients. J. Clin. Diagn. Res. 2013, 7, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Adeolu, M.; Alnajar, S.; Naushad, S.; Gupta, R.S. Genome-based phylogeny and taxonomy of the ‘Enterobacteriales’: Proposal for Enterobacterales ord. nov. divided into the families Enterobacteriaceae, Erwiniaceae fam. nov., Pectobacteriaceae fam. nov., Yersiniaceae fam. nov., Hafniaceae fam. nov., Morganellaceae fam. nov., and Budviciaceae fam. nov. Int. J. Syst. Evol. Microbiol. 2016, 66, 5575–5599. [Google Scholar] [CrossRef] [PubMed]
- Nazzaro, G. Serratia marcescens: An Italian story. Int. J. Dermatol. 2017, 56, 795–796. [Google Scholar] [CrossRef] [PubMed]
- Herra, C.; Falkiner, F. Serratia marcescens. Available online: http://www.antimicrobe.org/b26.asp (accessed on 1 September 2022).
- Hertle, R. The family of Serratia type pores forming toxins. Curr. Protein Pept. Sci. 2005, 6, 313–325. [Google Scholar] [CrossRef] [PubMed]
- Ray, C.; Shenoy, A.T.; Orihuela, C.J.; Gonzales Juarbe, N. Killing of Serratia marcescens biofilms with chloramphenicol. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 19. [Google Scholar] [CrossRef]
- Jones, R.N. Microbial etiologies of hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia. Clin. Infect. Dis. 2010, 51 (Suppl. S1), S81–S87. [Google Scholar] [CrossRef]
- Mills, J.; Drew, D. Serratia marcescens endocarditis: A regional illness associated with intravenous drug abuse. Ann. Intern. Med. 1976, 84, 29–35. [Google Scholar] [CrossRef]
- Merkier, A.K.; Rodríguez, M.C.; Togneri, A.; Brengi, S.; Osuna, C.; Pichel, M.; Cassini, M.H.; Centrón, D. Serratia marcescens Argentinean Collaborative Group Outbreak of a Cluster with Epidemic Behavior Due to Serratia marcescens after Colistin Administration in a Hospital Setting. J. Clin. Microbiol. 2013, 51, 2295–2302. [Google Scholar] [CrossRef]
- Arslan, U.; Erayman, I.; Kirdar, S.; Yuksekkaya, S.; Cimen, O.; Tuncer, I.; Bozdogan, B. Serratia marcescens sepsis outbreak in a neonatal intensive care unit. Pediatr. Int. 2010, 52, 208–212. [Google Scholar] [CrossRef]
- Harris, P.N.; Ferguson, J.K. Antibiotic therapy for inducible AmpC β-lactamase-producing Gram-negative bacilli: What are the alternatives to carbapenems, quinolones and aminoglycosides? Int. J. Antimicrob. Agents 2012, 40, 297–305. [Google Scholar] [CrossRef]
- Altwegg, M.; Lüthy-Hottenstein, J.; Grehn, M.; von Graevenitz, A. Automated analysis of 35-S-methionine labeled proteins by SDS-PAGE as a typing method in a suspected cluster of Serratia marcescens. Zentralbl. Bakteriol. 1989, 271, 372–380. [Google Scholar] [CrossRef]
- Blajchman, M.A.; Thornley, J.H.; Richardson, H.; Elder, D.; Spiak, C.; Racher, J. Platelet transfusion-induced Serratia marcescens sepsis due to vacuum tube contamination. Transfusion 1979, 19, 39–44. [Google Scholar] [CrossRef]
- Campbell, J.R.; Diacovo, T.; Baker, C.J. Serratia marcescens meningitis in neonates. Pediatr. Infect. Dis. J. 1992, 11, 881–886. [Google Scholar] [CrossRef]
- Castro-Moraga, M.E.; Coria, P.; Conca, N.; Berho, J.; King, A. Osteomielitis multifocal por Serratia marcescens en un niño con enfermedadgranulomatosacrónica [Serratia marcescens multifocal osteomyelitis in a child with chronic granulomatous disease]. Rev. Chil. De Infectología 2021, 38, 574–579. [Google Scholar] [CrossRef]
- Cayô, R.; Leme, R.C.P.; Streling, A.P.; Matos, A.P.; Nodari, C.S.; Chaves, J.R.E.; Brandão, J.L.F.; de Almeida, M.F.; Carrareto, V.; Pereira, M.A.D.C.; et al. Serratia marcescens harboring SME-4 in Brazil: A silent threat. Diagn. Microbiol. Infect. Dis. 2017, 87, 357–358. [Google Scholar] [CrossRef]
- Connacher, A.A.; Old, D.C.; Phillips, G.; Stewart, W.K.; Grimont, F.; Grimont, P.A. Recurrent peritonitis caused by Serratia marcescens in a diabetic patient receiving continuous ambulatory peritoneal dialysis. J. Hosp. Infect. 1988, 11, 155–160. [Google Scholar] [CrossRef]
- Cope, T.E.; Cope, W.; Beaumont, D.M. A case of necrotising fasciitis caused by Serratia marsescens: Extreme age as functional immunosuppression? Age Ageing 2013, 42, 266–268. [Google Scholar] [CrossRef]
- Da Silva, K.E.; Rossato, L.; Jorge, S.; de Oliveira, N.R.; Kremer, F.S.; Campos, V.F.; Pinto, L.D.S.; Dellagostin, O.A.; Simionatto, S. Three challenging cases of infections by multidrug-resistant Serratia marcescens in patients admitted to intensive care units. Braz. J. Microbiol. 2021, 52, 1341–1345. [Google Scholar] [CrossRef]
- Esel, D.; Doganay, M.; Bozdemir, N.; Yildiz, O.; Tezcaner, T.; Sumerkan, B.; Aygen, B.; Selcuklu, A. Polymicrobial ventriculitis and evaluation of an outbreak in a surgical intensive care unit due to inadequate sterilization. J. Hosp. Infect. 2002, 50, 170–174. [Google Scholar] [CrossRef]
- Esmaeilzadeh, M.; Islamian, A.; Lang, J.; Hornef, M.; Suerbaum, S.; Krauss, J. An unusual cause of ventriculoperitoneal shunt infection. JAAPA 2015, 28, 39–42. [Google Scholar] [CrossRef]
- Gammon, J.A.; Schwab, I.; Joseph, P. Gentamicin-resistant Serratia marcescens endophthalmitis. Arch Ophthalmol. 1980, 98, 1221–1223. [Google Scholar] [CrossRef] [PubMed]
- Gona, F.; Caio, C.; Iannolo, G.; Monaco, F.; Di Mento, G.; Cuscino, N.; Fontana, I.; Panarello, G.; Maugeri, G.; Mezzatesta, M.L.; et al. Detection of the IncX3 plasmid carrying bla KPC-3 in a Serratia marcescens strain isolated from a kidney–liver transplanted patient. J. Med. Microbiol. 2017, 66, 1454–1456. [Google Scholar] [CrossRef] [PubMed]
- Heltberg, O.; Skov, F.; Gerner-Smidt, P.; Kolmos, H.; Dybkjaer, E.; Gutschik, E.; Jerne, D.; Jepsen, O.; Weischer, M.; Frederiksen, W. Nosocomial epidemic of Serratia marcescens septicemia ascribed to contaminated blood transfusion bags. Transfusion 1993, 33, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.T.; Cheng, J.F.; Liu, Y.T.; Mao, Y.C.; Wu, M.S.; Liu, P.Y. Genome-based analysis of virulence determinants of a Serratia marcescens strain from soft tissues following a snake bite. Future Microbiol. 2018, 13, 331–343. [Google Scholar] [CrossRef]
- Johnson, J.S.; Croall, J.; Power, J.S.; Armstrong, G.R. Fatal Serratia marcescens meningitis and myocarditis in a patient with an indwelling urinary catheter. J Clin. Pathol. 1998, 51, 789–790. [Google Scholar] [CrossRef]
- Kufel, W.D.; Scrimenti, A.; Steele, J.M. A Case of Septic Shock Due to Serratia marcescens Pyelonephritis and Bacteremia in a Patient Receiving Empagliflozin. J. Pharm. Pract. 2017, 30, 672–675. [Google Scholar] [CrossRef]
- Lee, S.H.; Woo, S.J.; Park, K.H.; Kim, J.H.; Song, J.H.; Heo, J.W.; Yu, H.G.; Yu, Y.S.; Chung, H.; Park, K.U. Serratia marcescens endophthalmitis associated with intravitreal injections of bevacizumab. Eye 2009, 24, 226–232. [Google Scholar] [CrossRef]
- Lewis, A.M.; Stephenson, J.R.; Garner, J.; Afshar, F.; Tabaqchali, S. A hospital outbreak of Serratia marcescens in neurosurgical patients. Epidemiol. Infect. 1989, 102, 69–74. [Google Scholar] [CrossRef]
- Liangpunsakul, S.; Pursell, K. Community-acquired necrotizing fasciitis caused by Serratia marcescens: Case report and review. Eur. J. Clin. Microbiol. Infect. Dis. 2001, 20, 509–510. [Google Scholar] [CrossRef]
- Memon, M.; Raman, V. Serratia marcescens endogenous endophthalmitis in an immunocompetent host. BMJ Case Rep. 2016, 20, bcr2015209887. [Google Scholar] [CrossRef]
- Neonakis, I.; Messaritakis, H.; Stafylaki, D.; Maraki, S. First detection of a metallo-β-lactamase producing Serratia marcescens in a European university hospital. Indian J. Med. Microbiol. 2014, 32, 352–353. [Google Scholar] [CrossRef]
- Paquin, A.; Lepelletier, D.; Leprince, C.; Chamoux, C.; Treilhaud, M.; Despins, P.; Reynaud, A.; Corvec, S. Relapse of Serratia marcescens Sternal Osteitis 15 Years after the First Episode. J. Clin. Microbiol. 2012, 50, 184–186. [Google Scholar] [CrossRef]
- Rehman, T.; Moore, T.A.; Seoane, L. Serratia marcescens necrotizing fasciitis presenting as bilateral breast necrosis. J. Clin. Microbiol. 2012, 50, 3406–3408. [Google Scholar] [CrossRef]
- Reichling, J.J.; Rose, D.N.; Mendelson, M.H.; Hirschman, S.Z. Acute suppurative thyroiditis caused by Serratia marcescens. J. Infect. Dis. 1984, 149, 281. [Google Scholar] [CrossRef]
- Rieber, H.; Frontzek, A.; Pfeifer, Y. Emergence of metallo-β-lactamase GIM-1 in a clinical isolate of Serratia marcescens. Antimicrob. Agents Chemother. 2012, 56, 4945–4947. [Google Scholar] [CrossRef]
- Rodríguez, C.; Brengi, S.; Cáceres, M.A.; Mochi, S.; Viñas, M.R.; Rizza, C.A.; Merletti, G.; Bru, E.; Assa, J.D.; Raya, R.R.; et al. Successful management with fosfomycin + ceftazidime of an infection caused by multiple highly-related subtypes of multidrug-resistant and extensively drug-resistant KPC-producing Serratia marcescens. Int. J. Antimicrob. Agents 2018, 52, 737–739. [Google Scholar] [CrossRef]
- Rowsey, J.J.; Newsom, D.L.; Sexton, D.J.; Harms, W.K. Endophthalmitis: Current approaches. Ophthalmology 1982, 89, 1055–1066. [Google Scholar] [CrossRef]
- Rubens, C.E.; McGee, Z.A.; Farrar, W.E., Jr. Loss of an aminoglycoside resistance plasmid by Serratia marcescens during treatment of meningitis with amikacin. J. Infect. Dis. 1980, 141, 346–350. [Google Scholar] [CrossRef]
- Sevencan, N.O.; Cakmakliogullari, E.K.; Ozkan, A.E.; Kayhan, B. An unusual location of squamous cell carcinoma and a rare cutaneous infection caused by Serratia marcescens on the tumoral tissue: A case report. Medicine 2018, 97, e12596. [Google Scholar] [CrossRef]
- Shimizu, S.; Kojima, H.; Yoshida, C.; Suzukawa, K.; Mukai, H.Y.; Hasegawa, Y.; Hitomi, S.; Nagasawa, T. Chorioamnionitis caused by Serratia marcescens in a non-immunocompromised host. J. Clin. Pathol. 2003, 56, 871–872. [Google Scholar] [CrossRef]
- Smith, P.J.; Brookfield, D.S.; Shaw, D.A.; Gray, J. An outbreak of Serratia marcescens infections in a neonatal unit. Lancet 1984, 1, 151–153. [Google Scholar] [CrossRef] [PubMed]
- Tsakris, A.; Voulgari, E.; Poulou, A.; Kimouli, M.; Pournaras, S.; Ranellou, K.; Kosmopoulou, O.; Petropoulou, D. In Vivo Acquisition of a Plasmid-Mediated bla KPC-2 Gene among Clonal Isolates of Serratia marcescens. J. Clin. Microbiol. 2010, 48, 2546–2549. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.-J.; Yang, H.-F.; Liu, Y.-Y.; Mei, Q.; Ye, Y.; Li, H.-R.; Cheng, J.; Li, J.-B. The Emergence of the 16S rRNA Methyltransferase RmtB in a Multidrug-Resistant Serratia marcescens Isolate in China. Ann. Lab. Med. 2015, 35, 172–174. [Google Scholar] [CrossRef] [PubMed]
- Piccirilli, A.; Cherubini, S.; Brisdelli, F.; Fazii, P.; Stanziale, A.; Di Valerio, S.; Chiavaroli, V.; Principe, L.; Perilli, M. Molecular Characterization by Whole-Genome Sequencing of Clinical and Environmental Serratia marcescens Strains Isolated during an Outbreak in a Neonatal Intensive Care Unit (NICU). Diagnostics 2022, 12, 2180. [Google Scholar] [CrossRef]
- Cristina, M.L.; Sartini, M.; Spagnolo, A.M. Serratia marcescens Infections in Neonatal Intensive Care Units (NICUs). Int. J. Environ. Res. Public Health 2019, 16, 610. [Google Scholar] [CrossRef]
- Casolari, C.; Pecorari, M.; Fabio, G.; Cattani, S.; Venturelli, C.; Piccinini, L.; Tamassia, M.; Gennari, W.; Sabbatini, A.; Leporati, G.; et al. A simultaneous outbreak of Serratia marcescens and Klebsiella pneumoniae in a neonatal intensive care unit. J. Hosp. Infect. 2005, 61, 312–320. [Google Scholar] [CrossRef]
- Stock, I.; Grueger, T.; Wiedemann, B. Natural antibiotic susceptibility of strains of Serratia marcescens and the S. liquefaciens complex: S. liquefacienssensustricto, S. proteamaculans and S. grimesii. Int. J. Antimicrob. Agents 2003, 22, 35–47. [Google Scholar] [CrossRef]
- Qureshi, Z.A.; Paterson, D.; Pakstis, D.L.; Adams-Haduch, J.M.; Sandkovsky, G.; Sordillo, E.; Polsky, B.; Peleg, A.; Bhussar, M.K.; Doi, Y. Risk factors and outcome of extended-spectrum β-lactamase-producing Enterobacter cloacae bloodstream infections. Int. J. Antimicrob. Agents 2011, 37, 26–32. [Google Scholar] [CrossRef]
- Douglas, S.; Catessa, H.; Garret, C.C. An Antimicrobial Treatment Assessment of Serratia marcescens Bacteremia and Endocarditis. Front. Antibiot. 2022, 1, 942721. [Google Scholar] [CrossRef]
- Sarvikivi, E.; Lyytikäinen, O.; Salmenlinna, S.; Vuopio-Varkila, J.; Luukkainen, P.; Tarkka, E.; Saxén, H. Clustering of Serratia marcescens Infections in a Neonatal Intensive Care Unit. Infect. Control. Hosp. Epidemiol. 2004, 25, 723–729. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Zaric, R.Z.; Jankovic, S.; Zaric, M.; Milosavljevic, M.; Stojadinovic, M.; Pejcic, A. Antimicrobial treatment of Morganella morganii invasive infections: Systematic review. Indian J. Med. Microbiol. 2021, 39, 404–412. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).