
Insights from a Cross-Sectional Study on Knowledge, Attitudes and Behaviors Concerning Antibiotic Use in a Large Metropolitan Area: Implications for Public Health and Policy Interventions
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Setting and Sample
2.2. Procedures
2.3. Data Collection
2.4. Statistical Analysis
- (1)
- Knowledge about the proper use of antibiotics (Model 1);
- (2)
- Attitudes on the use of antibiotics (Model 2);
- (3)
- Behaviors related to the use of antibiotics in daily life (Model 3).
3. Results
4. Discussions
5. Limitation
6. Policies
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bell, B.G.; Schellevis, F.; Stobberingh, E.; Goossens, H.; Pringle, M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect. Dis. 2014, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibioticprescribing in primary care on antimicrobialresistance in individualpatients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef]
- Forslund, K.; Sunagawa, S.; Kultima, J.R.; Mende, D.R.; Arumugam, M.; Typas, A.; Bork, P. Country-specific antibiotic use practices impact the human gut resistome. Genome Res. 2010, 23, 1163–1169. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Antimicrobialresistance and Use Surveillance System (GLASS) Report: 2022. December 2022. Available online: https://www.who.int/publications/i/item/9789240062702 (accessed on 3 April 2023).
- Zhang, Y.; Steinman, M.A.; Kaplan, C.M. Geographic Variation in Outpatient Antibiotic Prescribing Among Older Adults. Arch. Intern. Med. 2012, 172, 1465. [Google Scholar] [CrossRef] [PubMed]
- Shallcross, L.J.; Howard, S.J.; Fowler, T.; Davies, S.C. Tackling the threat of antimicrobial resistance: From policy to sustainable action. Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20140082. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J. Antimicrobial Resistance, from bench-to-publicside. Microbes Infect. Chemother. 2021, 1, e1182. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Preventing the COVID-19 Pandemic from Causing an Antibiotic Resistance Catastrophe. November 2020. Available online: https://www.who.int/europe/news/item/18-11-2020-preventing-the-covid-19-pandemic-from-causing-an-antibiotic-resistance-catastrophe (accessed on 13 March 2023).
- Cantón, R.; Akova, M.; Langfeld, K.; Torumkuney, D. Relevance of the Consensus Principles for Appropriate Antibiotic Prescribing in 2022. J. Antimicrob. Chemother. 2022, 77, i2–i9. [Google Scholar] [CrossRef]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Naylor, N.R.; Atun, R.; Zhu, N.; Kulasabanathan, K.; Silva, S.; Chatterjee, A.; Knight, G.M.; Robotham, J.V. Estimating the burden of antimicrobial resistance: A systematic literature review. Antimicrob. Resist. Infect. Control 2018, 7, 58. [Google Scholar] [CrossRef]
- Ayukekbong, J.A.; Ntemgwa, M.; Atabe, A.N. The threat of antimicrobial resistance in developing countries: Causes and control strategies. Antimicrob. Resist. Infect. Control 2017, 6, 47. [Google Scholar] [CrossRef] [PubMed]
- Charani, E.; Smith, I.; Skodvin, B.; Perozziello, A.; Lucet, J.-C.; Lescure, F.-X.; Birgand, G.; Poda, A.; Ahmad, R.; Singh, S.; et al. Investigating the cultural and contextual determinants of antimicrobial stewardship programmes across low-, middle- and high-income countries—A qualitative study. PLoS ONE 2019, 14, e0209847. [Google Scholar] [CrossRef] [PubMed]
- Dunachie, S.J.; Day, N.P.; Dolecek, C. The challenges of estimating the human global burden of disease of antimicrobial resistant bacteria. Curr. Opin. Microbiol. 2020, 57, 95–101. [Google Scholar] [CrossRef]
- Musoke, D.; Namata, C.; Lubega, G.B.; Niyongabo, F.; Gonza, J.; Chidziwisano, K.; Nalinya, S.; Nuwematsiko, R.; Morse, T. The role of Environmental Health in preventing antimicrobial resistance in low- and middle-income countries. Environ. Health Prev. Med. 2021, 26, 100. [Google Scholar] [CrossRef]
- Pezzani, M.D.; Tornimbene, B.; Pessoa-Silva, C.; de Kraker, M.; Rizzardo, S.; Salerno, N.D.; Harbarth, S.; Tacconelli, E. Methodological quality of studies evaluating the burden of drug-resistant infections in humans due to the WHO Global Antimicrobial Resistance Surveillance System target bacteria. Clin. Microbiol. Infect. 2021, 27, 687–696. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Antimicrobial Resistance: Briefing to WHO Member States. March 2023. Available online: https://apps.who.int/gb/MSPI/pdf_files/2023/03/Item1_22-03.pdf (accessed on 20 April 2023).
- O’neill, J.I.M. Antimicrobial resistance: Tackling a crisis for the health and wealth of nations. Rev. Antimicrob. Resist. 2014, 1–20. [Google Scholar]
- Aponte-González, J.; González-Acuña, A.; Lopez, J.; Brown, P.; Eslava-Schmalbach, J. Perceptions in the community about the use of antibiotics without a prescription: Exploring ideas behind this practice. Pharm. Pract. 2019, 17, 1394. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; Alias, H.; Husin, S.A.; Ali, Z.B.; Sim, B.; Ponnampalavanar, S.S.L.S. Factors influencing inappropriate use of antibiotics: Findings from a nationwide survey of the general public in Malaysia. PLoS ONE 2021, 16, e0258698. [Google Scholar] [CrossRef]
- Aslam, A.; Gajdács, M.; Zin, C.S.; Ab Rahman, N.S.; Ahmed, S.I.; Zafar, M.Z.; Jamshed, S. Evidence of the Practice of Self-Medication with Antibiotics among the Lay Public in Low- and Middle-Income Countries: A Scoping Review. Antibiotics 2020, 9, 597. [Google Scholar] [CrossRef]
- Opalska, A.; Kwa, M.; Leufkens, H.; Gardarsdottir, H. Enabling appropriate use of antibiotics: Review of European Union procedures of harmonising product information, 2007 to 2020. Eurosurveillance 2020, 25, 2000035. [Google Scholar] [CrossRef]
- Abbo, L.M.; Cosgrove, S.E.; Pottinger, P.S.; Pereyra, M.; Sinkowitz-Cochran, R.; Srinivasan, A.; Webb, D.J.; Hooton, T.M. Medical students’ perceptions and knowledge about antimicrobial stewardship: How are we educating our future prescribers? Clin. Infect. Dis. 2013, 57, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Dyar, O.J.; Pulcini, C.; Howard, P.; Nathwani, D. ESGAP (ESCMID Study Group for Antibiotic Policies). European medical students: A first multicentre study of knowledge, attitudes and perceptions of antibiotic prescribing and antibiotic resistance. J. Antimicrob. Chemother. 2014, 69, 842–846. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Gu, J.; Zhang, M.; Ren, Z.; Yang, W.; Chen, Y.; Fu, Y.; Chen, X.; Cals, J.W.L.; Zhang, F. Knowledge, attitude and practice of antibiotics: A questionnaire study among 2500 Chinese students. BMC Med. Educ. 2013, 13, 163. [Google Scholar] [CrossRef]
- Khan, A.K.A.; Banu, G.; Reshma, K.K. Antibiotic Resistance and Usage-A Survey on the Knowledge, Attitude, Perceptions and Practices among the Medical Students of a Southern Indian Teaching Hospital. J. Clin. Diagn. Res. JCDR 2013, 7, 1613–1616. [Google Scholar] [CrossRef]
- Minen, M.T.; Duquaine, D.; Marx, M.A.; Weiss, D. A survey of knowledge, attitudes, and beliefs of medical students concerning antimicrobial use and resistance. Microb. Drug Resist. 2010, 16, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Scaioli, G.; Gualano, M.R.; Gili, R.; Masucci, S.; Bert, F.; Siliquini, R. Antibiotic Use: A Cross-Sectional Survey Assessing the Knowledge, Attitudes and Practices amongst Students of a School of Medicine in Italy. PLoS ONE 2015, 10, e0122476. [Google Scholar] [CrossRef]
- Thriemer, K.; Katuala, Y.; Batoko, B.; Alworonga, J.-P.; Devlieger, H.; Van Geet, C.; Ngbonda, D.; Jacobs, J. Antibiotic prescribing in DR Congo: A knowledge, attitude and practice survey among medical doctors and students. PLoS ONE 2013, 8, e55495. [Google Scholar] [CrossRef]
- Wright, E.P.; Jain, P. Survey of antibiotic knowledge amongst final year medical students. J. Antimicrob. Chemother. 2004, 53, 550–551. [Google Scholar] [CrossRef]
- Bhardwaj, K.; Shenoy, M.S.; Baliga, S.; Unnikrishnan, B.; Baliga, B.S. Knowledge, attitude, and practices related to antibiotic use and resistance among the general public of coastal south Karnataka, India—A cross-sectional survey. Clin. Epidemiol. Glob. Health 2021, 11, 100717. [Google Scholar] [CrossRef]
- Pogurschi, E.N.; Petcu, C.D.; Mizeranschi, A.E.; Zugravu, C.A.; Cirnatu, D.; Pet, I.; Ghimpețeanu, O.-M. Knowledge, Attitudes and Practices Regarding Antibiotic Use and Antibiotic Resistance: A Latent Class Analysis of a Romanian Population. Int. J. Environ. Res. Public Health 2022, 19, 7263. [Google Scholar] [CrossRef]
- Shehadeh, M.; Suaifan, G.; Darwish, R.M.; Wazaify, M.; Zaru, L.; Alja’fari, S. Knowledge, attitudes and behavior regarding antibiotics use and misuse among adults in the community of Jordan. A pilot study. Saudi Pharm. J. 2012, 20, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Sobeck, J.; Smith-Darden, J.; Gartner, D.; Kaljee, L.; Pieper, B.; Kilgore, P.; Zervos, M. Antibiotic Knowledge, Beliefs, and Behaviors: Testing Competing Hypotheses Using an Urban Community Sample. Health Commun. 2022, 37, 862–871. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Zhao, G.; Stålsby Lundborg, C.; Zhu, Y.; Zhao, Q.; Xu, B. Knowledge, attitudes, and practices of parents in rural China on the use of antibiotics in children: A cross-sectional study. BMC Infect. Dis. 2014, 14, 112. [Google Scholar] [CrossRef]
- Nepal, A.; Hendrie, D.; Robinson, S.; Selvey, L.A. Knowledge, attitudes and practices relating to antibiotic use among community members of the Rupandehi District in Nepal. BMC Public Health 2019, 19, 1558. [Google Scholar] [CrossRef] [PubMed]
- Paredes, J.L.; Navarro, R.; Watanabe, T.; Morán, F.; Balmaceda, M.P.; Reateguí, A.; Elias, R.; Bardellini, M.; Ochoa, T.J. Knowledge, attitudes and practices of parents towards antibiotic use in rural communities in Peru: A cross-sectional multicentre study. BMC Public Health 2022, 22, 459. [Google Scholar] [CrossRef]
- Alnasser, A.H.A.; Al-Tawfiq, J.A.; Ahmed, H.A.A.; Alqithami, S.M.H.; Alhaddad, Z.M.A.; Rabiah, A.S.M.; Albrahim, M.A.A.; Al Kalif, M.S.H.; Barry, M.; Temsah, M.-H.; et al. Public Knowledge, Attitude and Practice towards Antibiotics Use and Antimicrobial Resistance in Saudi Arabia: A Web-Based Cross-Sectional Survey. J. Public Health Res. 2021, 10, 2276. [Google Scholar] [CrossRef]
- Napolitano, F.; Izzo, M.T.; Di Giuseppe, G.; Angelillo, I.F. Public Knowledge, Attitudes, and Experience Regarding the Use of Antibiotics in Italy. PLoS ONE 2013, 8, e84177. [Google Scholar] [CrossRef]
- Montalti, M.; Soldà, G.; Capodici, A.; Di Valerio, Z.; Gribaudo, G.; La Fauci, G.; Salussolia, A.; Scognamiglio, F.; Zannoner, A.; Gori, D. Antimicrobial Resistance (AMR) in Italy over the Past Five Years: A Systematic Review. Biologics 2022, 2, 151–164. [Google Scholar] [CrossRef]
- Barchitta, M.; Quattrocchi, A.; Maugeri, A.; La Rosa, M.C.; La Mastra, C.; Sessa, L.; Cananzi, P.; Murolo, G.; Oteri, A.; Basile, G.; et al. Antibiotic Consumption and Resistance during a 3-Year Period in Sicily, Southern Italy. Int. J. Environ. Res. Public Health 2019, 16, 2253. [Google Scholar] [CrossRef]
- Sijbom, M.; Büchner, F.L.; Saadah, N.H.; Numans, M.E.; De Boer, M.G.J. Trends in antibiotic selection pressure generated in primary care and their association with sentinel antimicrobial resistance patterns in Europe. J. Antimicrob. Chemother. 2023, 78, 1245–1252. [Google Scholar] [CrossRef]
- ISTAT. Bilancio Demografico Mensile e Popolazione Residente per Sesso, Anno 2022; ISTAT: Rome, Italy, 2022. [Google Scholar]
- Montuori, P.; Gioia, M.; Sorrentino, M.; Di Duca, F.; Pennino, F.; Messineo, G.; Maccauro, M.L.; Riello, S.; Trama, U.; Triassi, M.; et al. Determinants Analysis Regarding Household Chemical Indoor Pollution. Toxics 2023, 11, 264. [Google Scholar] [CrossRef] [PubMed]
- Montuori, P.; Sorrentino, M.; Sarnacchiaro, P.; Di Duca, F.; Nardo, A.; Ferrante, B.; D’Angelo, D.; Di Sarno, S.; Pennino, F.; Masucci, A.; et al. Job Satisfaction: Knowledge, Attitudes, and Practices Analysis in a Well-Educated Population. Int. J. Environ. Res. Public Health 2022, 19, 14214. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C.; Menon, V.; Ameen, S.; Kumar Praharaj, S. Designing and conducting knowledge, attitude, and practice surveys in psychiatry: Practical guidance. Indian J. Psychol. Med. 2020, 42, 478–481. [Google Scholar] [CrossRef] [PubMed]
- Khadka, S.; Hashmi, F.K.; Yadav, G.K.; Lamichhane, S.; Giri, S.; Tariq, F.; Amin, S.; Zaheer, W.; Akram, K.; Asghar, I.; et al. Rational use of antimicrobials: A nationwide cross-sectional survey among people of Pakistan. Int. J. Surg. Glob. Health 2023, 6, e103. [Google Scholar] [CrossRef]
- Moon, Z.; Zuchowski, M.; Moss-Morris, R.; Hunter, M.S.; Norton, S.; Hughes, L.D. Disparities in access to mobile devices and e-health literacy among breast cancer survivors. Support. Care Cancer 2022, 30, 117–126. [Google Scholar] [CrossRef]
- Özkan, O.; Özer, Ö.; Özmen, S.; Budak, F. Investigation of the Perceived Coronavirus Threat, E-Health Literacy, and Psychological Well-Being in Turkey. Soc. Work Public Health 2022, 37, 122–134. [Google Scholar] [CrossRef]
- Shi, Y.; Ma, D.; Zhang, J.; Chen, B. In the digital age: A systematic literature review of the e-health literacy and influencing factors among Chinese older adults. J. Public Health 2023, 31, 679–687. [Google Scholar] [CrossRef]
- Walters, R.; Leslie, S.J.; Polson, R.; Cusack, T.; Gorely, T. Establishing the efficacy of interventions to improve health literacy and health behaviours: A systematic review. BMC Public Health 2020, 20, 1040. [Google Scholar] [CrossRef]
- Blix, H.S.; Hjellvik, V.; Litleskare, I.; Rønning, M.; Tverdal, A. Cigarette smoking and risk of subsequent use of antibacterials: A follow-up of 365,117 men and women. J. Antimicrob. Chemother. 2011, 66, 2159–2167. [Google Scholar] [CrossRef]
- De Mello, G.T.; da Silva, K.S.; da Costa, B.G.; Borgatto, A.F. Patterns of risk behaviors in Brazilian older adults: A latent class analysis. Geriatr. Gerontol. Int. 2019, 19, 245–248. [Google Scholar] [CrossRef]
- Burnside, C.; Hudson, T.; Williams, C.; Lawson, W.; Laiyemo, A.O. Sex differences in the use of healthcare services among US adults with and without a cancer diagnosis. Turk. J. Urol. 2018, 44, 298. [Google Scholar] [CrossRef] [PubMed]
- Shebehe, J.; Ottertun, E.; Carlén, K.; Gustafson, D. Knowledge about infections is associated with antibiotic use: Cross-sectional evidence from the health survey Northern Ireland. BMC Public Health 2021, 21, 1041. [Google Scholar] [CrossRef] [PubMed]
- Marzan, M.; Islam, D.Z.; Lugova, H.; Krishnapillai, A.; Haque, M.; Islam, S. Knowledge, Attitudes, and Practices of Antimicrobial Uses and Resistance Among Public University Students in Bangladesh. Infect. Drug Resist. 2021, 14, 519–533. [Google Scholar] [CrossRef] [PubMed]
- Awad, A.I.; Aboud, E.A. Knowledge, Attitude and Practice towards Antibiotic Use among the Public in Kuwait. PLoS ONE 2015, 10, e0117910. [Google Scholar] [CrossRef] [PubMed]
- Zucco, R.; Lavano, F.; Anfosso, R.; Bianco, A.; Pileggi, C.; Pavia, M. Internet and social media use for antibiotic-related information seeking: Findings from a survey among adult population in Italy. Int. J. Med. Inform. 2018, 111, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Parveen, S.; Garzon-Orjuela, N.; Amin, D.; McHugh, P.; Vellinga, A. Public health interventions to improve antimicrobial resistance awareness and behavioural change associated with antimicrobial use: A systematic review exploring the use of social media. Antibiotics 2022, 11, 669. [Google Scholar] [CrossRef]
- Waaseth, M.; Adan, A.; Røen, I.L.; Eriksen, K.; Stanojevic, T.; Halvorsen, K.H.; Garcia, B.H.; Holst, L.; Ulshagen, K.M.; Blix, H.S.; et al. Knowledge of antibiotics and antibiotic resistance among Norwegian pharmacy customers—A cross-sectional study. BMC Public Health 2019, 19, 66. [Google Scholar] [CrossRef]
- Smith, C.A.; Chang, E.; Gallego, G.; Khan, A.; Armour, M.; Balneaves, L.G. An education intervention to improve decision making and health literacy among older Australians: A randomised controlled trial. BMC Geriatr. 2019, 19, 129. [Google Scholar] [CrossRef]
- Anderson, A. Online health information and public knowledge, attitudes, and behaviours regarding antibiotics in the UK: Multiple regression analysis of Wellcome Monitor and Eurobarometer Data. PLoS ONE 2018, 13, e0204878. [Google Scholar] [CrossRef]
- Alejandro, A.L.; Bruce, M.; Leo, C. Parents’ awareness of antimicrobial resistance: A qualitative study utilising the Health Belief Model in Perth, Western Australia. Aust. N. Z. J. Public Health 2022, 46, 764–770. [Google Scholar] [CrossRef]
- Higuita-Gutiérrez, L.F.; Roncancio Villamil, G.E.; Jiménez Quiceno, J.N. Knowledge, attitude, and practice regarding antibiotic use and resistance among medical students in Colombia: A cross-sectional descriptive study. BMC Public Health 2020, 20, 1861. [Google Scholar] [CrossRef]
- Gualano, M.R.; Gili, R.; Scaioli, G.; Bert, F.; Siliquini, R. General population’s knowledge and attitudes about antibiotics: A systematic review and meta-analysis. Pharmacoepidemiol. Drug Saf. 2015, 24, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Read, R.C.; Cornaglia, G.; Kahlmeter, G. Professional challenges and opportunities in clinical microbiology and infectious diseases in Europe. Lancet Infect. Dis. 2011, 11, 408–415. [Google Scholar] [CrossRef] [PubMed]
- McNulty, C.A.M.; Lecky, D.M.; Farrell, D.; Kostkova, P.; Adriaenssens, N.; KoprivovaHerotova, T.; Holt, J.; Touboul, P.; Merakou, K.; Koncan, R.; et al. Overview of e-Bug: An antibiotic and hygiene educational resource for schools. J. Antimicrob. Chemother. 2011, 66 (Suppl. 5), v3–v12. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Study Population | N | Percentage |
|---|---|---|
| Sex | (1158) | |
| Male | 479 | 41.36 |
| Female | 679 | 58.64 |
| Age | ||
| <25 | 378 | 32.64 |
| 25–35 | 486 | 41.97 |
| 36–55 | 70 | 6.05 |
| >55 | 224 | 19.34 |
| Education | ||
| Primary school | 57 | 4.92 |
| Middle school | 168 | 14.51 |
| High school | 579 | 50.00 |
| University degree | 354 | 30.57 |
| Sons | ||
| Yes | 235 | 20.30 |
| No | 923 | 79.70 |
| Smoking habits | ||
| Yes | 520 | 44.90 |
| No | 638 | 55.10 |
| Marital Status | ||
| Single | 535 | 46.20 |
| In a relationship | 623 | 53.80 |
| N. | Statement (Variables) | Agree (%) | Uncertain (%) | Disagree (%) |
|---|---|---|---|---|
| K1 | Antibiotics are effective against bacteria | 89.37 | 9.33 | 1.30 |
| K2 | Antibiotics are effective against viruses. | 37.82 | 15.98 | 46.20 |
| K3 | Antibiotics have side effects. | 83.94 | 13.64 | 2.42 |
| K4 | Antibiotics are useful for pain relief. | 37.30 | 13.30 | 49.40 |
| K5 | The antibiotic should be stopped when symptoms disappear. | 19.86 | 13.65 | 66.49 |
| K6 | Frequent use of antibiotics reduces their effectiveness. | 71.24 | 17.70 | 11.06 |
| K7 | There are bacteria that are resistant to all antibiotics. | 22.63 | 49.48 | 27.89 |
| K8 | The antibiogram evaluates antibiotic sensitivity. | 52.50 | 41.20 | 6.30 |
| K9 | Antibiotic resistance indicates the survival of bacteria against antibiotics. | 59.50 | 28.41 | 12.09 |
| K10 | Skipping one or two doses of antibiotic may contribute to antibiotic-resistance. | 46.98 | 28.93 | 24.09 |
| K11 | The sale of antibiotics without a prescription is prohibited. | 55.53 | 17.96 | 26.51 |
| K12 | Fascia A antibiotics are only used in hospitals. | 15.55 | 59.84 | 24.61 |
| N. | Statement (Variables) | Agree (%) | Uncertain (%) | Disagree (%) |
|---|---|---|---|---|
| A1 | It is essential to always carry a drug. | 45.51 | 15.37 | 39.12 |
| A2 | One antibiotic is as good as another. | 10.79 | 11.92 | 77.29 |
| A3 | Antibiotics do not cause harm. | 7.25 | 15.98 | 76.77 |
| A4 | You should take antibiotics immediately when you have a sore throat. | 11.31 | 9.24 | 79.45 |
| A5 | It is useless to have a blood test if you feel good. | 10.54 | 4.66 | 84.80 |
| A6 | Often, consulting your doctor is superfluous. | 14.43 | 13.64 | 71.93 |
| A7 | It is preferable to take drugs that you already have at home. | 23.75 | 14.85 | 61.40 |
| A8 | It is possible to take antibiotics from friends and relatives, if used to treat the same symptom. | 23.84 | 17.44 | 58.72 |
| A9 | Reading the package’s leaflet is useless. | 19.17 | 2.33 | 78.50 |
| A10 | The expiry of a drug is not relevant. | 5.10 | 5.35 | 89.55 |
| A11 | Antibiotics should not be taken without an antibiogram. | 17.27 | 42.57 | 40.16 |
| A12 | Skipping one or two doses of antibiotics is irrelevant. | 9.24 | 10.54 | 80.22 |
| N. | Questions | Yes/Always (%) | Often (%) | Sometimes (%) | Never (%) |
|---|---|---|---|---|---|
| B1 | Do you take antibiotics when you have the flu? | 13.73 | 6.30 | 52.94 | 27.03 |
| B2 | Do you take antibiotics when you have a sore throat? | 31.52 | 49.05 | 10.36 | 9.07 |
| B3 | Do you take antibiotics to treat urinary infections? | 21.16 | 12.61 | 32.72 | 33.51 |
| B4 | Do you only take antibiotics after medical consultation? | 52.16 | 14.94 | 32.38 | 0.52 |
| B5 | Do you take the same antibiotic to treat the same symptom? | 23.23 | 23.49 | 36.70 | 16.58 |
| B6 | Do you stop the antibiotic if you forget to take a dose? | 5.96 | 9.15 | 8.81 | 76.08 |
| B7 | Do you stop the antibiotic if your symptoms disappear? | 13.99 | 7.86 | 28.50 | 49.65 |
| B8 | Do you usually carry antibiotics when you travel? | 32.47 | 18.83 | 22.19 | 26.51 |
| B9 | Do you read the drug’s leaflet? | 45.94 | 19.43 | 20.29 | 14.34 |
| B10 | Do you read the drug’s expiration date? | 83.25 | 7.51 | 7.17 | 2.07 |
| B11 | Do you take antibiotics without doing an antibiogram? | 76.42 | 2.42 | 14.34 | 6.82 |
| B12 | Have you happened to miss one or two doses of antibiotics? | 37.39 | 4.84 | 23.49 | 34.28 |
| Coefficients Not Standardized | Coefficients Standardized | |||||
|---|---|---|---|---|---|---|
| b | Standard Error | t | 95% Conf. Interval | p-Value | ||
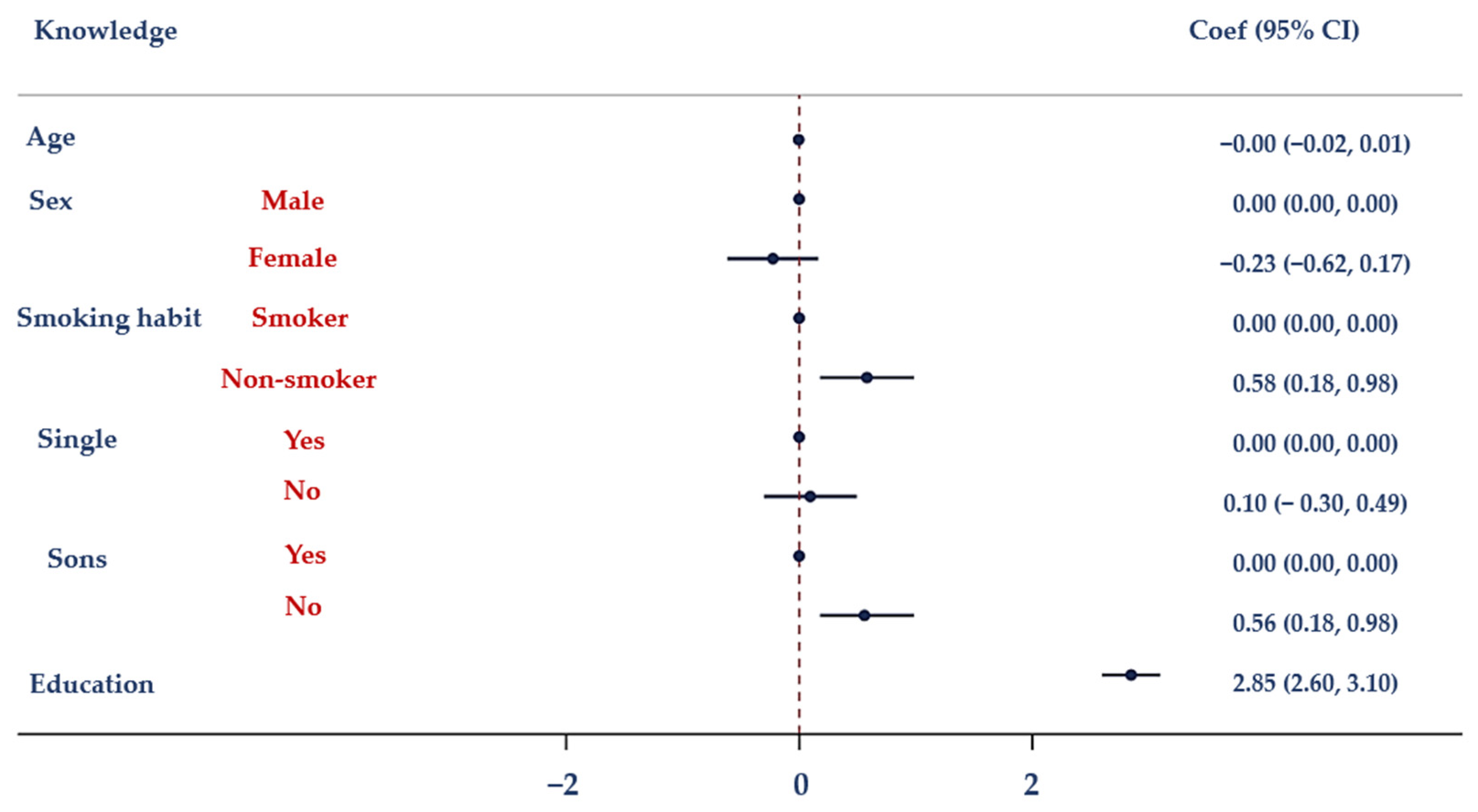
| Model I—Dependent variable: Knowledge | ||||||
| Prob > F = 0.000 | R-squared = 0.4744 | Root-MSE = 3.4311 | ||||
| Age | −0.004 | 0.008 | −0.50 | −0.019 | 0.011 | 0.615 |
| Sex | −0.225 | 0.199 | −0.13 | −0.616 | 0.165 | 0.258 |
| Marital status | 0.096 | 0.203 | 0.47 | −0.303 | 0.495 | 0.636 |
| Children | 0.561 | 0.331 | 1.70 | −0.88 | 1.21 | 0.090 |
| Smoking habits | 0.582 | 0.205 | 2.84 | 0.180 | 0.985 | 0.005 |
| Education | 2.85 | 0.128 | 22.23 | 2.60 | 3.10 | 0.000 |
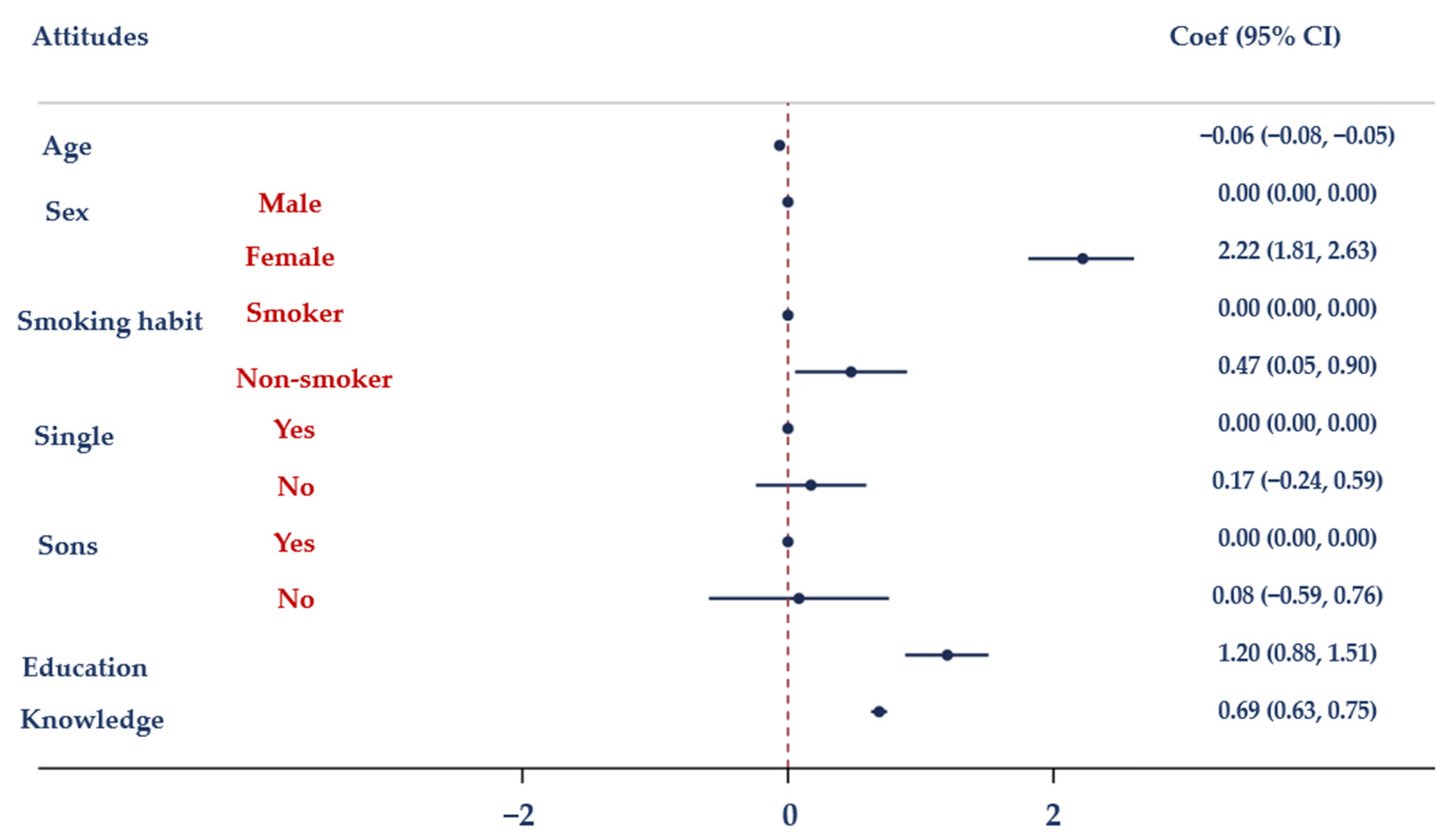
| Model II—Dependent variable: Attitudes | ||||||
| Prob > F = 0.000 | R-squared = 0.4744 | Root-MSE = 3.4311 | ||||
| Age | −0.063 | 0.008 | −7.96 | −0.079 | −0.048 | 0.000 |
| Sex | 2.22 | 0.208 | 10.68 | 1.81 | 2.63 | 0.000 |
| Marital status | 0.173 | 0.212 | 0.82 | −0.242 | 0.590 | 0.414 |
| Children | 0.083 | 0.345 | 0.24 | −0.595 | 0.761 | 0.810 |
| Smoking habits | 0.475 | 0.215 | 2.21 | 0.053 | 0.897 | 0.027 |
| Education | 1.20 | 0.160 | 7.49 | 0.883 | 1.51 | 0.000 |
| Knowledge | 0.687 | 0.031 | 22.33 | 0.626 | 0.747 | 0.000 |
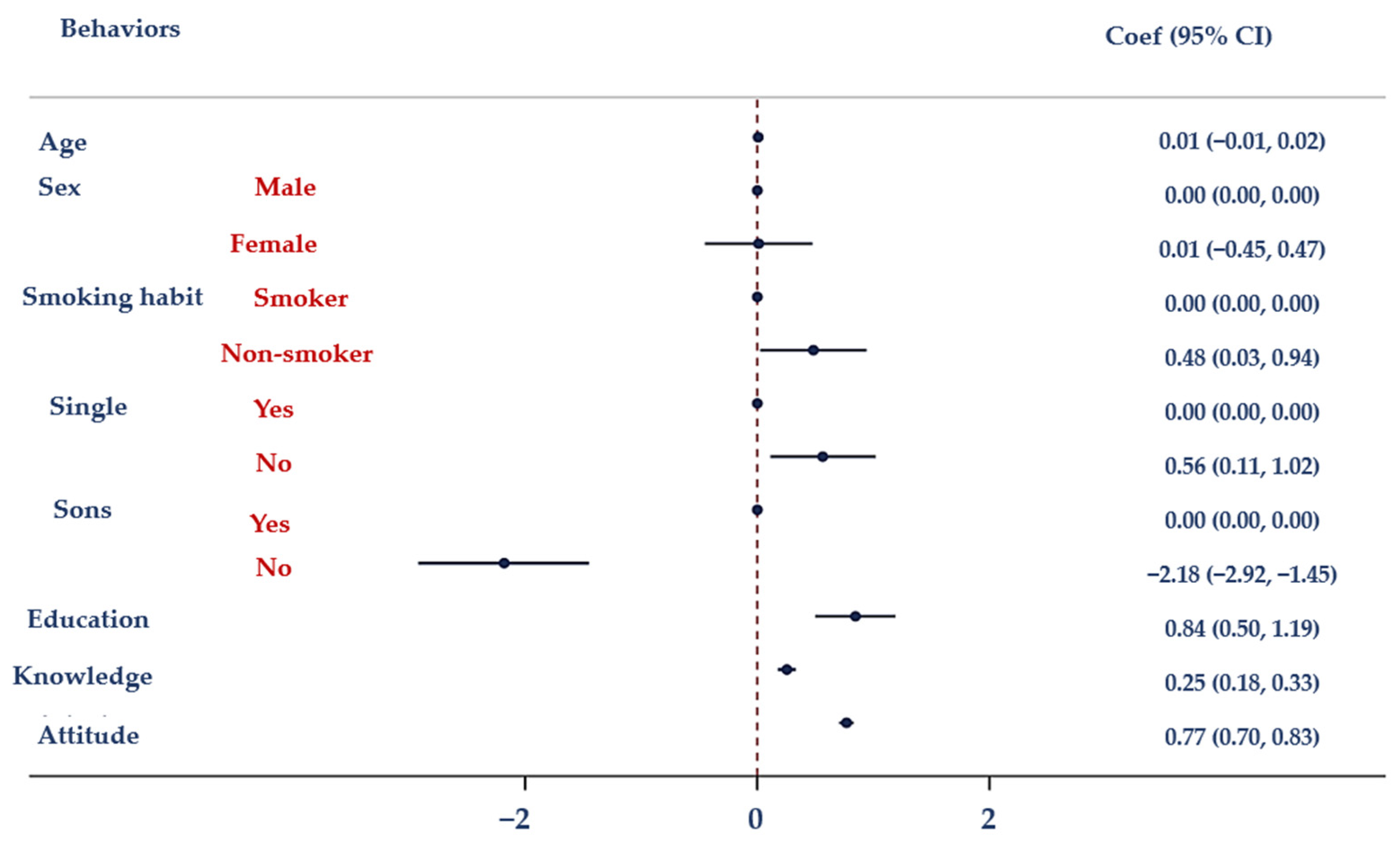
| Model III—Dependent variable: Behaviour | ||||||
| Prob > F = 0.000 | R-squared = 0.4744 | Root-MSE = 3.4311 | ||||
| Age | 0.007 | 0.088 | 0.76 | −0.011 | 0.024 | 0.446 |
| Sex | 0.011 | 0.236 | 0.05 | −0.452 | 0.474 | 0.962 |
| Marital status | 0.563 | 0.230 | 2.45 | 0.112 | 1.02 | 0.015 |
| Children | −2.18 | 0.374 | −5.84 | −2.92 | −1.45 | 0.000 |
| Smoking habits | 0.483 | 0.233 | 2.07 | 0.025 | 0.94 | 0.039 |
| Education | 0.845 | 0.177 | 4.76 | 0.497 | 1.19 | 0.000 |
| Knowledge | 0.254 | 0.040 | 6.37 | 0.176 | 0.332 | 0.000 |
| Attitude | 0.768 | 0.032 | 24.03 | 0.705 | 0.830 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pennino, F.; Maccauro, M.L.; Sorrentino, M.; Gioia, M.; Riello, S.; Messineo, G.; Di Rosa, C.; Montuori, P.; Triassi, M.; Nardone, A. Insights from a Cross-Sectional Study on Knowledge, Attitudes and Behaviors Concerning Antibiotic Use in a Large Metropolitan Area: Implications for Public Health and Policy Interventions. Antibiotics 2023, 12, 1476. https://doi.org/10.3390/antibiotics12101476
Pennino F, Maccauro ML, Sorrentino M, Gioia M, Riello S, Messineo G, Di Rosa C, Montuori P, Triassi M, Nardone A. Insights from a Cross-Sectional Study on Knowledge, Attitudes and Behaviors Concerning Antibiotic Use in a Large Metropolitan Area: Implications for Public Health and Policy Interventions. Antibiotics. 2023; 12(10):1476. https://doi.org/10.3390/antibiotics12101476
Chicago/Turabian StylePennino, Francesca, Maria Luisa Maccauro, Michele Sorrentino, Mariagiovanna Gioia, Simonetta Riello, Giuseppe Messineo, Carmela Di Rosa, Paolo Montuori, Maria Triassi, and Antonio Nardone. 2023. "Insights from a Cross-Sectional Study on Knowledge, Attitudes and Behaviors Concerning Antibiotic Use in a Large Metropolitan Area: Implications for Public Health and Policy Interventions" Antibiotics 12, no. 10: 1476. https://doi.org/10.3390/antibiotics12101476
APA StylePennino, F., Maccauro, M. L., Sorrentino, M., Gioia, M., Riello, S., Messineo, G., Di Rosa, C., Montuori, P., Triassi, M., & Nardone, A. (2023). Insights from a Cross-Sectional Study on Knowledge, Attitudes and Behaviors Concerning Antibiotic Use in a Large Metropolitan Area: Implications for Public Health and Policy Interventions. Antibiotics, 12(10), 1476. https://doi.org/10.3390/antibiotics12101476