
Conventional Hospitalization versus Sequential Outpatient Parenteral Antibiotic Therapy for Staphylococcus aureus Bacteremia: Post-Hoc Analysis of a Multicenter Observational Cohort
 , , , , , , ,
, , , , , , ,  , , , and add
Show full author list
, , , and add
Show full author list
Abstract
1. Introduction
2. Methods
2.1. Study Design and Patients
2.2. Ethical Statement
2.3. Variables and Definitions
2.4. Statistical Analysis
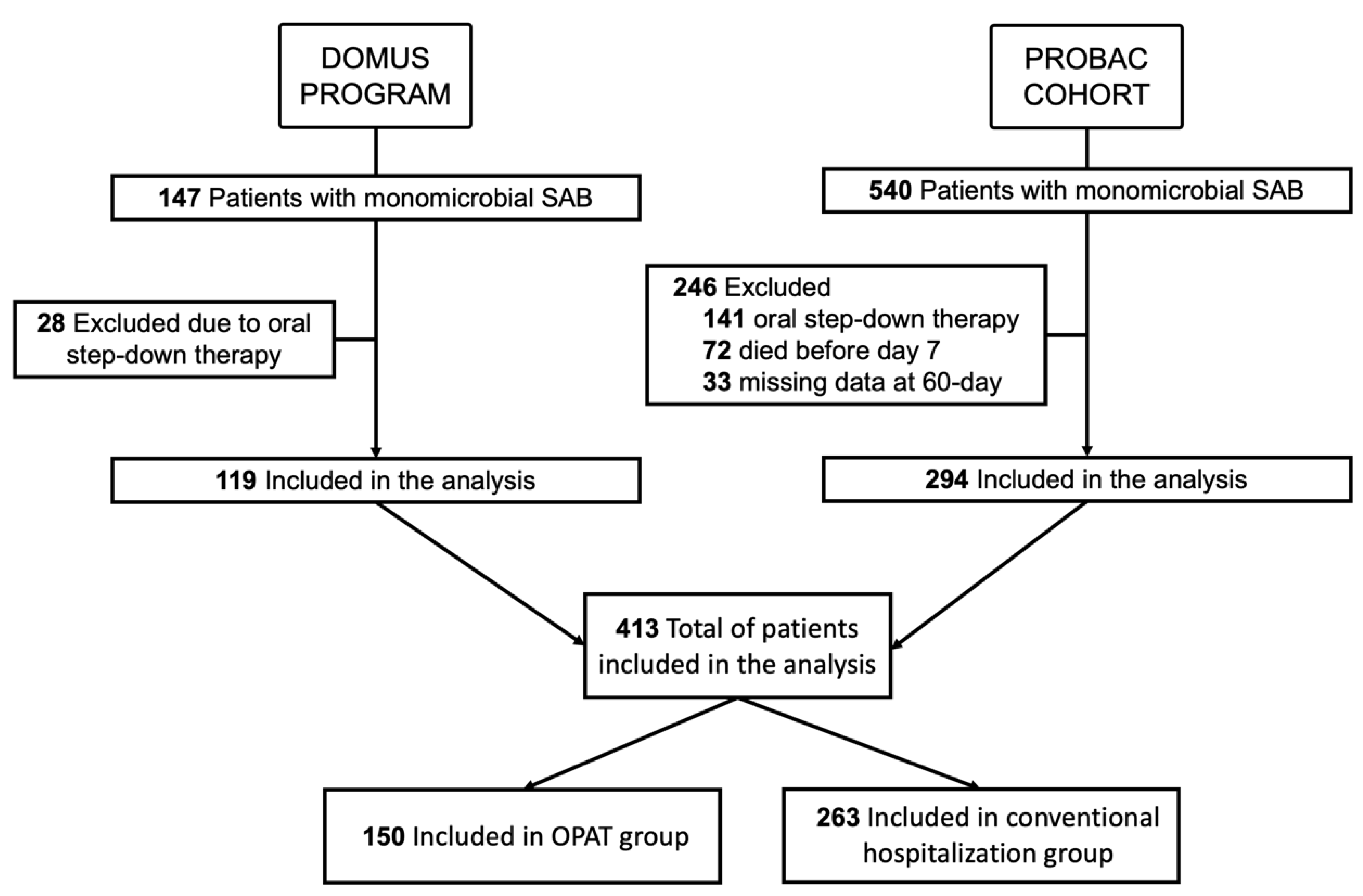
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eduardo, L.; Cortés, L.; Mujal, A.; Coordinator, M.; Fernández, M.; De Mandojana, M.; Martín, N.; Gil, M.; Solà, J.; Villegas, E.; et al. Executive Summary of Outpatient Parenteral Antimicrobial Therapy: Guidelines of the Spanish Society of Clinical Microbiology and Infectious Diseases and the Spanish Domiciliary Hospitalisation Society. Enferm. Infecc. Microbiol. Clín. 2019, 37, 405–409. [Google Scholar] [CrossRef]
- Norris, A.H.; Shrestha, N.K.; Allison, G.M.; Keller, S.C.; Bhavan, K.P.; Zurlo, J.J.; Hersh, A.L.; Gorski, L.A.; Bosso, J.A.; Rathore, M.H.; et al. 2018 Infectious Diseases Society of America Clinical Practice Guideline for the Management of Outpatient Parenteral Antimicrobial Therapy. Clin. Infect. Dis. 2019, 68, e1–e35. [Google Scholar] [CrossRef]
- Sriskandarajah, S.; Hobbs, J.; Roughead, E.; Reynolds, K. Safety and Effectiveness of ‘Hospital in the Home’ and ‘Outpatient Parenteral Antimicrobial Therapy’ in Different Age Groups: A Systematic Review of Observational Studies. Int. J. Clin. Pract. 2018, 72, e13216. [Google Scholar] [CrossRef]
- Psaltikidis, E.M.; Nunes, E.; Bustorff, J.M.; Moretti, M.L.; Resende, M.R. Economic Evaluation of Outpatient Parenteral Antimicrobial Therapy: A Systematic Review. Expert Rev. Pharmacoecon. Outcomes Res. 2017, 17, 355–375. [Google Scholar] [CrossRef]
- Staples, J.A.; Ho, M.; Ferris, D.; Hayek, J.; Liu, G.; Tran, K.C.; Sutherland, J.M. Outpatient Versus Inpatient Intravenous Antimicrobial Therapy: A Population-Based Observational Cohort Study of Adverse Events and Costs. Clin. Infect. Dis. 2022, 75, 1921–1929. [Google Scholar] [CrossRef]
- Cervera, C.; García, L.; Sala, M.; Almela, M.; Moreno, A.; Falces, C.; Mestres, C.A.; Marco, F.; Robau, M.; Gatell, J.M.; et al. Efficacy and Safety of Outpatient Parenteral Antibiotic Therapy for Infective Endocarditis: A Ten-Year Prospective Study. Med. Clin. 2011, 29, 587–592. [Google Scholar] [CrossRef]
- Pericàs, J.M.; Llopis, J.; González-ramallo, V.; Goenaga, M.Á.; Muñoz, P.; García-leoni, M.E.; Fariñas, M.C.; Pajarón, M.; Ambrosioni, J.; Luque, R.; et al. Outpatient Parenteral Antibiotic Treatment for Infective Endocarditis: A Prospective Cohort Study From the GAMES Cohort. Clin. Infect. Dis. 2019, 69, 1690–1700. [Google Scholar] [CrossRef]
- Herrera-hidalgo, L.; Alarc, D.; Luis, E.L. Enterococcus Faecalis Endocarditis and Outpatient Treatment: A Systematic Review of Current Alternatives. J. Clin. Med. 2020, 11, 7. [Google Scholar] [CrossRef]
- Pericàs, J.M.; Llopis, J.; Muñoz, P.; González-Ramallo, V.; García-Leoni, M.E.; de Alarcón, A.; Luque, R.; Fariñas, M.C.; Goenaga, M.Á.; Hernández-Meneses, M.; et al. Outpatient Parenteral Antibiotic Treatment vs Hospitalization for Infective Endocarditis: Validation of the OPAT-GAMES Criteria. Open Forum Infect. Dis. 2022, 9, ofac442. [Google Scholar] [CrossRef]
- Van Hal, S.J.; Jensen, S.O.; Vaska, V.L.; Espedido, B.A.; Paterson, D.L.; Gosbell, I.B. Predictors of Mortality in Staphylococcus Aureus Bacteremia. Clin. Microbiol. Rev. 2012, 25, 362–386. [Google Scholar] [CrossRef]
- Tong, S.Y.C.; Davis, J.S.; Eichenberger, E.; Holland, T.L.; Fowler, V.G. Staphylococcus Aureus Infections: Epidemiology, Pathophysiology, Clinical Manifestations, and Management. Clin. Microbiol. Rev. 2015, 28, 623. [Google Scholar] [CrossRef]
- Kouijzer, I.J.E.; Van Leerdam, E.J.; Gompelman, M.; Tuinte, R.A.M.; Aarntzen, E.H.J.G.; Berrevoets, M.A.H.; Maat, I.; Bleeker-rovers, C.P.; Van Crevel, R.; Oever, J. Intravenous to Oral Switch in Complicated Staphylococcus Aureus Bacteremia without Endovascular Infection: A Retrospective Single- Center Cohort Study. Clin. Infect. Dis. 2021, 73, 895–898. [Google Scholar] [CrossRef]
- Rac, H. Transition from Intravenous to Oral Antimicrobial Therapy in Patients with Uncomplicated and Complicated Bloodstream Infections. Clin. Microbiol. Infect. 2020, 26, 299–306. [Google Scholar] [CrossRef]
- Yeager, S.D.; Oliver, J.E.; Shorman, M.A.; Wright, L.R.; Veve, M.P. International Journal of Antimicrobial Agents Comparison of Linezolid Step-down Therapy to Standard Parenteral Therapy in Methicillin-Resistant Staphylococcus Aureus Bloodstream Infections. Int. J. Antimicrob. Agents 2022, 57, 106329. [Google Scholar] [CrossRef]
- Veve, M.P.; Patel, N.; Smith, Z.A.; Yeager, S.D.; Wright, L.R.; Shorman, M.A. International Journal of Antimicrobial Agents Comparison of Dalbavancin to Standard-of-Care for Outpatient Treatment of Invasive Gram-Positive Infections. Int. J. Antimicrob. Agents 2020, 56, 106210. [Google Scholar] [CrossRef]
- Kaasch, A.J.; Fätkenheuer, G.; Prinz-langenohl, R.; Paulus, U.; Hellmich, M.; Weiß, V. Early Oral Switch Therapy in Low-Risk Staphylococcus Aureus Bloodstream Infection (SABATO): Study Protocol for a Randomized Controlled Trial Early Oral Switch Therapy in Low-Risk Staphylococcus Aureus Bloodstream Infection (SABATO): Study Protocol For. Trials 2015, 16, 450. [Google Scholar] [CrossRef]
- Boclé, H.; Lavigne, J.; Cellier, N.; Crouzet, J.; Kouyoumdjian, P.; Sotto, A.; Loubet, P. Effectiveness of Early Switching from Intravenous to Oral Antibiotic Therapy in Staphylococcus Aureus Prosthetic Bone and Joint or Orthopedic Metalware-Associated Infections. BMC Musculoskelet. Disord. 2021, 22, 315. [Google Scholar] [CrossRef]
- Theodore, D.A.; Furuya, E.Y.; Austin, E.; Greendyke, W.G. Outcomes among Patients with Staphylococcus Aureus Bacteremia Enrolled in a Postdischarge Outpatient Parenteral Antibiotic Therapy Program at an Academic Medical Center. Antimicrob. Steward. Healthc. Epidemiol. 2022, 2, E167. [Google Scholar] [CrossRef]
- Winans, S.A.; Luce, A.M.; Hasbun, R. Outpatient Parenteral Antimicrobial Therapy for the Treatment of Methicillin-Susceptible Staphylococcus Aureus: A Comparison of Cefazolin and Ceftriaxone. Infection 2013, 41, 769–774. [Google Scholar] [CrossRef]
- Tice, A.D.; Rehm, S.J. Meeting the Challenges of Methicillin-Resistant Staphylococcus Aureus with Outpatient Parenteral Antimicrobial Therapy. Clin. Infect. Dis. 2010, 51, 171–175. [Google Scholar] [CrossRef]
- Hamad, Y.; Connor, L.; Bailey, T.C.; George, I.A. Outcomes of Outpatient Parenteral Antimicrobial Therapy with Ceftriaxone for Methicillin-Susceptible Staphylococcus Aureus Bloodstream Infections—A Single- Center Observational Study. Open Forum Infect. Dis. 2020, 7, ofaa341. [Google Scholar] [CrossRef]
- Shrestha, N.K.; Mason, P.; Gordon, S.M.; Neuner, E.; Nutter, B.; O’Rourke, C.; Rehm, S.J. Adverse Events, Healthcare Interventions and Healthcare Utilization during Home Infusion Therapy with Daptomycin and Vancomycin: A Propensity Score-Matched Cohort Study. J. Antimicrob. Chemother. 2014, 69, 1407–1415. [Google Scholar] [CrossRef] [PubMed]
- Townsend, J.; Pelletier, J.; Peterson, G.; Matulevicius, S.; Sreeramoju, P. Quality Improvement of Staphylococcus Aureus Bacteremia Management and Predictors of Relapse-Free Survival. Am. J. Med. 2016, 129, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Fowler, V.G.; Olsen, M.K.; Corey, G.R.; Cheng, A.C.; Dudley, T.; Oddone, E.Z. Clinical Identifiers of Complicated S. Aureus Bacteremia. Arch. Intern. Med. 2003, 163, 2066–2072. [Google Scholar] [CrossRef] [PubMed]
- Townsend, J.; Keller, S.; Tibuakuu, M.; Thakker, S.; Webster, B.; Siegel, M.; Psoter, K.J.; Mansour, O.; Perl, T.M. Outpatient Parenteral Therapy for Complicated Staphylococcus Aureus Infections: A Snapshot of Processes and Outcomes in the Real World. Open Forum Infect. Dis. 2018, 5, ofy274. [Google Scholar] [CrossRef] [PubMed]
- Rehm, S.; Campion, M.; Katz, D.E.; Russo, R.; Boucher, H.W. Community-Based Outpatient Parenteral Antimicrobial Therapy (CoPAT) for Staphylococcus Aureus Bacteraemia with or without Infective Endocarditis: Analysis of the Randomized Trial Comparing Daptomycin with Standard Therapy. J. Antimicrob. Chemother. 2009, 63, 1034–1042. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.; Tam, I.; Weigel, B.; Breeze, J.L.; Paulus, J.K.; Nelson, J.; Allison, G.M. Comparative Outcomes of β-Lactam Antibiotics in Outpatient Parenteral Antibiotic Therapy: Treatment Success, Readmissions and Antibiotic Switches. J. Antimicrob. Chemother. 2015, 70, 2389–2396. [Google Scholar] [CrossRef]
- Herrera-Hidalgo, L.; Luque-Márquez, R.; de Alarcon, A.; Guisado-Gil, A.B.; Gutierrez-Gutierrez, B.; Navarro-Amuedo, M.D.; Praena-Segovia, J.; Carmona-Caballero, J.M.; Fraile-Ramos, E.; Gutierrez-Valencia, A.; et al. Clinical Outcomes of an Innovative Cefazolin Delivery Program for MSSA Infections in OPAT. J. Clin. Med. 2022, 11, 1551. [Google Scholar] [CrossRef]
- Youngster, I.; Shenoy, E.S.; Hooper, D.C.; Nelson, S.B. Comparative Evaluation of the Tolerability of Cefazolin and Nafcillin for Treatment of Methicillin-Susceptible Staphylococcus Aureus Infections in the Outpatient Setting. Clin. Infect. Dis. 2014, 59, 369–375. [Google Scholar] [CrossRef]
- Birrell, M.T.; Fuller, A. Twice Daily Cefazolin Is Effective for Treatment of Serious Methicillin-Sensitive Staphylococcus Aureus Infection in an Outpatient Parenteral Antimicrobial Therapy Program. Ther. Adv. Infect. Dis. 2019, 6, 1–8. [Google Scholar] [CrossRef]
- Alsowaida, Y.S.; Benitez, G.; Bin Saleh, K.; Almangour, T.A.; Shehadeh, F.; Mylonakis, E. Effectiveness and Safety of Ceftriaxone Compared to Standard of Care for Treatment of Bloodstream Infections Due to Methicillin-Susceptible Staphylococcus Aureus: A Systematic Review and Meta-Analysis. Antibiotics 2022, 11, 375. [Google Scholar] [CrossRef] [PubMed]
- López-Cortés, L.E.; Ayerbe-Garciá, R.; Carrasco-Hernández, L.; Fraile-Ramos, E.; Carmona-Caballero, J.M.; Quintana-Gallego, E.; Valido-Morales, A.; Praena, J.; Pachón-Diaz, J. Outpatient Parenteral Antimicrobial Treatment for Non-Cystic Fibrosis Bronchiectasis Exacerbations: A Prospective Multicentre Observational Cohort Study. Respiration 2019, 98, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Gil-Navarro, M.V.; Luque-Marquez, R.; Báez-Gutiérrez, N.; Álvarez-Marín, R.; Navarro-Amuedo, M.D.; Praena-Segovia, J.; Carmona-Caballero, J.M.; Fraile-Ramos, E.; López-Cortés, L.E. Antifungal Treatment Administered in OPAT Programs Is a Safe and Effective Option in Selected Patients. Enferm. Infecc. Microbiol. Clin. 2020, 38, 479–484. [Google Scholar] [CrossRef]
- Mary, C.; Pompei, P.; Ales, K.L.; Mackenzie, C.R. A New Method of Classifying Prognostic in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar]
- ECDC European Centre for Disease Prevention and Control. Healthcare-Associated Infections Acquired in Intensive Care Units. In ECDC. Annual Epidemiological Report 2015. Stock; ECDC: Solna, Sweden, 2017; pp. 1–10. [Google Scholar]
- Nambiar, K.; Seifert, H.; Rieg, S.; Kern, W.V.; Scarborough, M.; Gordon, N.C.; Bin, H.; Song, K.; Tilley, R.; Gott, H.; et al. Survival Following Staphylococcus Aureus Bloodstream Infection: A Prospective Multinational Cohort Study Assessing the Impact of Place of Care. J. Infect. 2018, 77, 516–525. [Google Scholar] [CrossRef]
- Htin, A.K.F.; Friedman, N.D.; Hughes, A.; Brien, D.P.O.; Huffam, S.; Redden, A.; Athan, E. Outpatient Parenteral Antimicrobial Therapy Is Safe and Effective for the Treatment of Infective Endocarditis: A Retrospective Cohort Study. Intern. Med. J. 2013, 43, 700–705. [Google Scholar] [CrossRef]
- Rezar, R.; Lichtenauer, M.; Haar, M.; Hödl, G.; Kern, J.M.; Zhou, Z.; Wuppinger, T.; Kraus, J.; Strohmer, B.; Hoppe, U.C.; et al. Infective Endocarditis—A Review of Current Therapy and Future Challenges. Hell. J. Cardiol. 2021, 62, 190–200. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All Cases (n = 413) | OPAT Group (n = 150) | Full Hospital-Based Therapy (n = 263) | p Value | |
|---|---|---|---|---|
| Median age (IQR) | 69 (56–79) | 64 (51–77) | 70 (58–79) | 0.009 |
| Male gender | 283 (68.5%) | 105 (70.0%) | 178 (67.9%) | 0.664 |
| Comorbidities | ||||
| Charlson index ≥ 2 | 290 (79.2%) | 110 (73.3%) | 180 (68.4%) | 0.296 |
| Diabetes Mellitus | 121 (29.3%) | 42 (28.0%) | 79 (30.0%) | 0.662 |
| COPD | 57 (13.8%) | 25 (16.7%) | 32 (12.2%) | 0.202 |
| Chronic renal failure | 102 (24.7%) | 28 (18.7%) | 74 (28.1%) | 0.032 |
| Chronic heart failure | 91 (22.0%) | 50 (33.3%) | 41 (15.6%) | <0.001 |
| Malignancy | 137 (33.2%) | 67 (44.7%) | 70 (26.6%) | <0.001 |
| Chronic liver disease | 35 (8.5%) | 12 (8.0%) | 23 (8.7%) | 0.794 |
| Immunosuppressed | 40 (9.7%) | 16 (10.7%) | 24 (9.1%) | 0.611 |
| Acquisition of infection | ||||
| Community-acquired | 101 (24.5%) | 30 (20.0%) | 71 (27.0%) | 0.112 |
| Nosocomial/healthcare acquisition | 312 (75.5%) | 120 (80.0%) | 192 (73.0%) | 0.112 |
| Department | ||||
| Surgery | 65 (15.8%) | 29 (19.3%) | 36 (13.7%) | 0.134 |
| Medical | 347 (84.2%) | 121 (80.7%) | 226 (86.3%) | 0.134 |
| Source of infection | ||||
| Vascular catheter | 177 (42.9%) | 93 (62.0%) | 84 (31.9%) | < 0.001 |
| Osteoarticular | 24 (5.8%) | 5 (3.3%) | 19 (7.2%) | 0.104 |
| Unknown | 63 (15.3%) | 13 (8.7%) | 50 (19.9%) | 0.005 |
| Respiratory tract | 27 (6.5%) | 3 (2.0%) | 24 (9.1%) | 0.005 |
| Intra-abdominal | 9 (2.2%) | 1 (0.7%) | 8 (3.0%) | 0.165 |
| Skin and soft tissues | 62 (15.0%) | 17 (11.3%) | 45 (17.1%) | 0.114 |
| Endocarditis or vascular prosthesis | 21 (5.1%) | 9 (6.0%) | 12 (4.6%) | 0.523 |
| Others | 17 (4.1%) | 6 (4.0%) | 11 (4.2%) | 0.928 |
| Methicillin-resistant S. aureus | 83 (20.1%) | 20 (13.3%) | 63 (24.0%) | 0.011 |
| Complicated bacteremia | 157 (38.0%) | 68 (45.3%) | 89 (33.8%) | 0.027 |
| Infective endocarditis | 24 (5.8%) | 12 (8.0%) | 12 (4.6%) | 0.189 |
| Metastatic distant foci | 27 (6.5%) | 15 (10.0%) | 12 (4.6%) | 0.032 |
| Persistent bacteremia | 45 (10.9%) | 14 (9.3%) | 31 (11.8%) | 0.442 |
| Persistent fever > 72h | 43 (10.4%) | 5 (3.3%) | 38 (14.4%) | <0.001 |
| Vascular prosthesis | 12 (2.9%) | 6 (4.0%) | 6 (2.3%) | 0.317 |
| Valve prosthesis | 19 (4.6%) | 11 (7.3%) | 8 (3.0%) | 0.045 |
| Orthopedic prosthesis | 23 (5.6%) | 12 (8.0%) | 11 (4.2%) | 0.104 |
| Intracardiac device | 30 (7.3%) | 19 (12.7%) | 11 (4.2%) | 0.001 |
| Total duration of therapy, days, median (IQR) | 17 (14–27) | 20 (15–29) | 16 (12–22) | <0.001 |
| Length of hospital stay, days, median (IQR) | 17 (12–28) | 16 (11–21) | 22 (12–35) | <0.001 |
| 60-day overall mortality | 93 (22.5%) | 10 (6.7%) | 83 (31.6%) | <0.001 |
| Treatment failure | 108 (26.2%) | 15 (10.0%) | 93 (35.4%) | <0.001 |
| Treatment Failure (n = 108) | Treatment Success (n = 305) | p Value | OR (95% CI) | |
|---|---|---|---|---|
| OPAT group | 15 (13.9%) | 135 (44.3%) | <0.001 | 0.203 (0.113–0.367) |
| Age ≥ 65 years | 79 (73.1%) | 161 (52.8%) | <0.001 | 2.436 (1.506–3.943) |
| Male sex | 74 (68.5%) | 209 (68.8%) | 0.964 | 0.989 (0.616–1.588) |
| Comorbidities | ||||
| Charlson index ≥ 2 | 81 (75.0%) | 209 (68.5%) | 0.206 | 1.378 (0.837–2.268) |
| Diabetes mellitus | 29 (26.9%) | 92 (30.2%) | 0.516 | 0.850 (0.520–1.388) |
| COPD | 21 (19.4%) | 36 (11.8%) | 0.048 | 1.804 (1.000–3.254) |
| Chronic renal failure | 34 (31.5%) | 68 (22.3%) | 0.057 | 1.601 (0.984–2.607) |
| Chronic heart failure | 26 (24.1%) | 65 (21.3%) | 0.552 | 1.171 (0.696–1.968) |
| Malignancy | 39 (36.1%) | 98 (32.1%) | 0.450 | 1.194 (0.753–1.892) |
| Chronic liver disease | 11 (10.2%) | 24 (7.9%) | 0.458 | 1.328 (0.627–2.811) |
| Dialysis therapy | 9 (8.3%) | 22 (7.2%) | 0.704 | 1.169 (0.521–2.625) |
| Immunosuppression | 11 (10.2%) | 29 (9.5%) | 0.838 | 1.079 (0.519–2.243) |
| Acquisition of infection | ||||
| Community-acquired | 30 (27.8%) | 71 (23.3%) | 0.350 | 1.268 (0.771–2.085) |
| Department | ||||
| Medical | 98 (90.7%) | 249 (81.9%) | 0.031 | 2.165 (1.061–4.417) |
| Source of infection | ||||
| Vascular catheter | 32 (29.6%) | 145 (47.5%) | 0.001 | 0.465 (0.290–0.744) |
| Osteoarticular | 5 (4.6%) | 19 (6.2%) | 0.541 | 0.731 (0.266–2.007) |
| Unknown | 24 (22.2%) | 39 (12.8%) | 0.019 | 1.949 (1.108–3.427) |
| Respiratory tract | 9 (8.3%) | 18 (5.9%) | 0.380 | 1.449 (0.631–3.331) |
| Intra-abdominal | 6 (5.6%) | 3 (1.0%) | 0.012 | 5.922 (1.454–24.108) |
| Skin and soft tissues | 18 (16.7%) | 44 (14.4%) | 0.575 | 1.186 (0.652–2.158) |
| Endocarditis or vascular prosthesis | 6 (5.6%) | 15 (4.9%) | 0.796 | 1.137 (0.430–3.010) |
| Others | 6 (4.6%) | 11 (3.6%) | 0.401 | 1.572 (0.567–4.360) |
| Methicillin-resistant S. aureus | 34 (31.5%) | 49 (16.1%) | 0.001 | 2.400 (1.444–3.990) |
| Complicated bacteremia | 55 (50.9%) | 102 (33.4%) | 0.001 | 2.065 (1.322–3.226) |
| Endocarditis | 7 (6.5%) | 17 (5.6%) | 0.729 | 1.174 (0.473–2.914) |
| Metastatic distant foci | 10 (9.3%) | 17 (5.6%) | 0.183 | 1.729 (0.766–3.902) |
| Persistent bacteremia | 24 (22.2%) | 21 (6.9%) | <0.001 | 3.864 (2.049–7.286) |
| Persistent fever > 72 h | 20 (18.5%) | 23 (7.5%) | 0.001 | 2.787 (1.462–5.313) |
| Vascular prosthesis | 4 (3.7%) | 8 (2.6%) | 0.521 | 1.428 (0.421–4.841) |
| Valve prosthesis | 4 (3.7%) | 15 (4.9%) | 0.791 | 0.744 (0.241–2.291) |
| Orthopedic prosthesis | 7 (6.5%) | 16 (5.2%) | 0.630 | 1.252 (0.501–3.131) |
| Intracardiac device | 8 (7.4%) | 22 (7.2%) | 0.947 | 1.029 (0.444–2.385) |
| p Value | Adjusted OR (95% CI) a | |
|---|---|---|
| OPAT therapy | 0.001 | 0.275 (0.129–0.584) |
| Age ≥ 65 years | 0.061 | 1.719 (0.975–3.030) |
| Comorbidities | ||
| COPD | 0.049 | 2.076 (1.002–4.299) |
| Chronic renal failure | 0.468 | 1.258 (0.677–2.335) |
| Chronic heart failure | 0.833 | 1.083 (0.514–2.283) |
| Malignancy | 0.039 | 1.869 (1.033–3.380) |
| Medical department | 0.036 | 2.455 (1.061–5.680) |
| Source of infection | ||
| Vascular catheter | 0.420 | 0.758 (0.387–1.485) |
| Unknown | 0.506 | 1.265 (0.633–2.531) |
| Intra-abdominal | 0.088 | 4.264 (0.807–22.525) |
| Methicillin-resistant S. aureus | 0.017 | 2.125 (1.147–3.935) |
| Complicated bacteremia | <0.001 | 2.967 (1.722–5.109) |
| High-risk center | 0.001 | 3.389 (1.629–7.049) |
| Crude Analysis a | Adjusted Analysis b | |||||
|---|---|---|---|---|---|---|
| All Cases (n = 202) | OPAT Group (n = 101) | Full Hospital-Based Therapy (n = 101) | p Value | OR Adjusted (95%CI) | p Value | |
| Median age (IQR) | 65 (53–76) | 64 (53–77) | 65 (54–76) | 0.790 c | ||
| Age ≥ 65 years | 102 (50.5%) | 50 (49.5%) | 52 (51.5%) | 0.778 | 0.983 (0.658–1.469) | 0.932 |
| Comorbidities | ||||||
| Charlson index ≥ 2 | 144 (71.3%) | 70 (69.3%) | 74 (73.3%) | 0.534 | 0.874 (0.560–1.365) | 0.554 |
| Diabetes mellitus | 61 (30.2%) | 29 (28.7%) | 32 (31.7%) | 0.646 | ||
| COPD | 24 (11.9%) | 12 (11.9%) | 12 (11.9%) | 1.000 | ||
| Chronic renal failure | 36 (17.8%) | 17 (16.8%) | 19 (18.8%) | 0.713 | ||
| Chronic heart failure | 52 (25.7%) | 26 (25.7%) | 26 (25.7%) | 1.000 | ||
| Malignancy | 82 (40.6%) | 44 (43.6%) | 38 (37.6%) | 0.390 | ||
| Chronic liver disease | 19 (9.4%) | 9 (8.9%) | 10 (9.9%) | 0.810 | ||
| Immunosuppressed | 20 (9.9%) | 7 (6.9%) | 13 (12.9%) | 0.158 | ||
| Nosocomial/healthcare acquisition | 152 (75.2%) | 77 (76.2%) | 75 (74.3%) | 0.744 | ||
| Medical department | 170 (84.6%) | 84 (83.2%) | 86 (86.0%) | 0.578 | 0.882 (0.506–1.536) | 0.656 |
| Source of infection | ||||||
| Vascular catheter | 108 (53.5%) | 56 (55.4%) | 52 (51.5%) | 0.573 | 1.109 (0.702–1.754) | 0.656 |
| Unknown | 26 (12.9%) | 12 (11.9%) | 14 (13.9%) | 0.674 | 1.212 (0.602–2.439) | 0.590 |
| Respiratory tract | 7 (3.5%) | 2 (2.0%) | 5 (5.0%) | 0.445 d | ||
| Intra-abdominal | 3 (1.5%) | 0 | 3 (3.0%) | 0.246 d | ||
| Others e | 58 (28.7%) | 31 (30.7%) | 27 (26.7%) | 0.534 | ||
| Methicillin-resistant S. aureus | 23 (11.4%) | 14 (13.9%) | 9 (8.9%) | 0.268 | 1.225 (0.689–2.179) | 0.489 |
| Complicated bacteremia | 67 (33.2%) | 35 (34.7%) | 32 (31.7%) | 0.654 | 0.645 | 1.108 (0.716–1.717) |
| Infective endocarditis | 9 (4.5%) | 4 (4.0%) | 5 (5.0%) | 1.000 d | ||
| Metastatic distant foci | 11 (5.4%) | 7 (6.9%) | 4 (4.0%) | 0.352 | ||
| Persistent bacteremia | 16 (7.9%) | 8 (7.9%) | 8 (7.9%) | 1.000 | ||
| Persistent fever > 72 h | 9 (4.5%) | 5 (5.0%) | 4 (4.0%) | 1.000 | ||
| Vascular prosthesis | 7 (3.5%) | 3 (3.0%) | 4 (4.0%) | 1.000 d | ||
| Valve prosthesis | 12 (5.9%) | 6 (5.9%) | 6 (5.9%) | 1.000 | ||
| Orthopedic prosthesis | 12 (5.9%) | 5 (5.0%) | 7 (6.9%) | 0.552 | ||
| Intracardiac device | 17 (8.4%) | 8 (7.9%) | 9 (8.9%) | 0.800 | ||
| 60-day overall mortality | 28 (13.9%) | 6 (5.9%) | 22 (21.8%) | 0.001 | ||
| Treatment failure | 31 (15.3%) | 9 (8.9%) | 22 (21.8%) | 0.011 | 0.660 (0.324–1.345) | 0.253 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castillo-Fernández, N.; Pérez-Crespo, P.M.M.; Salamanca-Rivera, E.; Herrera-Hidalgo, L.; de Alarcón, A.; Navarro-Amuedo, M.D.; Marrodán Ciordia, T.; Pérez-Rodríguez, M.T.; Sevilla-Blanco, J.; Jover-Saenz, A.; et al. Conventional Hospitalization versus Sequential Outpatient Parenteral Antibiotic Therapy for Staphylococcus aureus Bacteremia: Post-Hoc Analysis of a Multicenter Observational Cohort. Antibiotics 2023, 12, 129. https://doi.org/10.3390/antibiotics12010129
Castillo-Fernández N, Pérez-Crespo PMM, Salamanca-Rivera E, Herrera-Hidalgo L, de Alarcón A, Navarro-Amuedo MD, Marrodán Ciordia T, Pérez-Rodríguez MT, Sevilla-Blanco J, Jover-Saenz A, et al. Conventional Hospitalization versus Sequential Outpatient Parenteral Antibiotic Therapy for Staphylococcus aureus Bacteremia: Post-Hoc Analysis of a Multicenter Observational Cohort. Antibiotics. 2023; 12(1):129. https://doi.org/10.3390/antibiotics12010129
Chicago/Turabian StyleCastillo-Fernández, Nerea, Pedro María Martínez Pérez-Crespo, Elena Salamanca-Rivera, Laura Herrera-Hidalgo, Arístides de Alarcón, María Dolores Navarro-Amuedo, Teresa Marrodán Ciordia, María Teresa Pérez-Rodríguez, Juan Sevilla-Blanco, Alfredo Jover-Saenz, and et al. 2023. "Conventional Hospitalization versus Sequential Outpatient Parenteral Antibiotic Therapy for Staphylococcus aureus Bacteremia: Post-Hoc Analysis of a Multicenter Observational Cohort" Antibiotics 12, no. 1: 129. https://doi.org/10.3390/antibiotics12010129
APA StyleCastillo-Fernández, N., Pérez-Crespo, P. M. M., Salamanca-Rivera, E., Herrera-Hidalgo, L., de Alarcón, A., Navarro-Amuedo, M. D., Marrodán Ciordia, T., Pérez-Rodríguez, M. T., Sevilla-Blanco, J., Jover-Saenz, A., Fernández-Suárez, J., Armiñanzas-Castillo, C., Reguera-Iglesias, J. M., Natera Kindelán, C., Boix-Palop, L., León Jiménez, E., Galán-Sánchez, F., del Arco Jiménez, A., Bahamonde-Carrasco, A., ... López Cortés, L. E. (2023). Conventional Hospitalization versus Sequential Outpatient Parenteral Antibiotic Therapy for Staphylococcus aureus Bacteremia: Post-Hoc Analysis of a Multicenter Observational Cohort. Antibiotics, 12(1), 129. https://doi.org/10.3390/antibiotics12010129