

Educational Interventions to Reduce Prescription and Dispensing of Antibiotics in Primary Care: A Systematic Review of Economic Impact

 ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection and Eligibility Criteria
2.3. Data Extraction and Quality Assessment
2.4. Data Syntheses and Analysis
3. Results
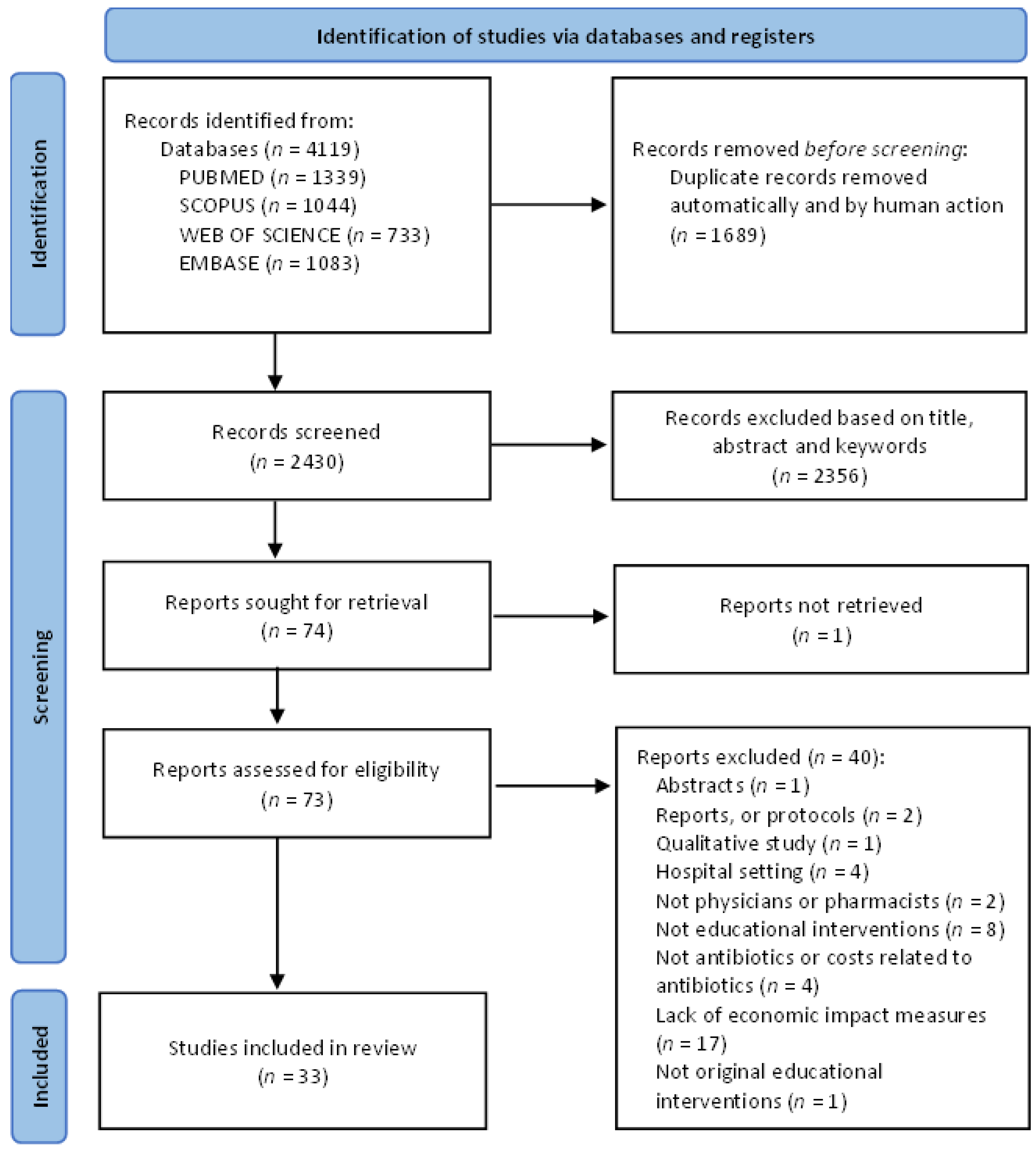
3.1. Study Selection and Quality Assessment
3.2. Study Characteristics
3.3. Educational Intervention Types
3.4. Antibiotic Consumption and Appropriateness of Prescription
3.4.1. Antibiotic Prescription Rate
3.4.2. Costs of Antibiotic Dispensing and Prescription
3.4.3. Antibiotic Treatment Success and Quality-Adjusted Life Years
3.5. Economic Effects of the Educational Interventions
4. Discussion
4.1. Antibiotic Consumption and Prescription
4.2. Antibiotic Cost and Costs of Antibiotic Prescription
4.3. Educational Interventions
4.4. Economic Effects of the Educational Interventions
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization WHO. Library Cataloguing-in-Publication Data. Global Action Plan on Antimicrobial Resistance. Microbe Mag. 2015, 10, 354–355. [Google Scholar]
- Schwartz, K.L.; Ivers, N.; Langford, B.J.; Taljaard, M.; Neish, D.; Brown, K.A.; Leung, V.; Daneman, N.; Alloo, J.; Silverman, M.; et al. Effect of Antibiotic-Prescribing Feedback to High-Volume Primary Care Physicians on Number of Antibiotic Prescriptions: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 1165–1173. [Google Scholar] [CrossRef]
- Acharya, K.R.; Brankston, G.; Soucy, J.P.R.; Cohen, A.; Hulth, A.; Löfmark, S.; Davidovitch, N.; Ellen, M.; Fisman, D.N.; Moran-Gilad, J.; et al. Evaluation of an OPEN Stewardship Generated Feedback Intervention to Improve Antibiotic Prescribing among Primary Care Veterinarians in Ontario, Canada and Israel: Protocol for Evaluating Usability and an Interrupted Time-Series Analysis. BMJ Open 2021, 11, e039760. [Google Scholar] [CrossRef]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. Review on Antimicrobial Resistance. Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf (accessed on 23 May 2022).
- Suda, K.J.; Hicks, L.A.; Roberts, R.M.; Hunkler, R.J.; Danziger, L.H. A National Evaluation of Antibiotic Expenditures by Healthcare Setting in the United States, 2009. J. Antimicrob. Chemother. 2013, 68, 715–718. [Google Scholar] [CrossRef]
- Wang, J.; Wang, P.; Wang, X.; Zheng, Y.; Xiao, Y. Use and Prescription of Antibiotics in Primary Health Care Settings in China. JAMA Intern. Med. 2014, 174, 1914–1920. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Canadian Antimicrobial Resistance Surveillance System—Update 2020. Available online: https://www.canada.ca/en/public-health/services/publications/drugs-health-products/canadian-antimicrobial-resistance-surveillance-system-2020-report.html (accessed on 23 May 2022).
- Schwartz, K.L.; Langford, B.J.; Daneman, N.; Chen, B.; Brown, K.A.; McIsaac, W.; Tu, K.; Candido, E.; Johnstone, J.; Leung, V.; et al. Unnecessary Antibiotic Prescribing in a Canadian Primary Care Setting: A Descriptive Analysis Using Routinely Collected Electronic Medical Record Data. CMAJ Open 2020, 8, E360–E369. [Google Scholar] [CrossRef]
- Hicks, L.A.; Taylor, T.H.; Hunkler, R.J. U.S. Outpatient Antibiotic Prescribing, 2010. N. Engl. J. Med. 2013, 368, 1461–1462. [Google Scholar] [CrossRef]
- Fleming, D.M.; Taylor, R.J.; Haguinet, F.; Schuck-Paim, C.; Logie, J.; Webb, D.J.; Lustig, R.L.; Matias, G. Influenza-Attributable Burden in United Kingdom Primary Care. Epidemiol. Infect. 2016, 144, 537–547. [Google Scholar] [CrossRef]
- Tonkin-Crine, S.K.G.; Tan, P.S.; van Hecke, O.; Wang, K.; Roberts, N.W.; Mccullough, A.; Hansen, M.P.; Butler, C.C.; del Mar, C.B. Clinician-targeted Interventions to Influence Antibiotic Prescribing Behaviour for Acute Respiratory Infections in Primary Care: An Overview of Systematic Reviews. Cochrane Database Syst. Rev. 2017, 2017, CD012252. [Google Scholar] [CrossRef]
- Köchling, A.; Löffler, C.; Reinsch, S.; Hornung, A.; Böhmer, F.; Altiner, A.; Chenot, J.F. Reduction of Antibiotic Prescriptions for Acute Respiratory Tract Infections in Primary Care: A Systematic Review. Implement. Sci. 2018, 13, 47. [Google Scholar] [CrossRef]
- Roque, F.; Herdeiro, M.T.; Soares, S.; Rodrigues, A.T.; Breitenfeld, L.; Figueiras, A. Educational Interventions to Improve Prescription and Dispensing of Antibiotics: A Systematic Review. BMC Public Health 2014, 14, 1276. [Google Scholar] [CrossRef] [Green Version]
- Briel, M.; Langewitz, W.; Tschudi, P.; Young, J.; Hugenschmidt, C.; Bucher, H.C. Communication Training and Antibiotic Use in Acute Respiratory Tract Infections. A Cluster Randomised Controlled Trial in General Practice. Swiss Med. Wkly. 2006, 136, 241–247. [Google Scholar]
- Gonzales, R.; Anderer, T.; McCulloch, C.E.; Maselli, J.H.; Bloom, F.J.; Graf, T.R.; Stahl, M.; Yefko, M.; Molecavage, J.; Metlay, J.P. A Cluster-Randomized Trial of Decision Support Strategies for Reducing Antibiotic Use for Acute Bronchitis. JAMA Intern. Med. 2013, 173, 267–273. [Google Scholar] [CrossRef]
- Arnold, S.R.; Straus, S.E. Interventions to Improve Antibiotic Prescribing Practices in Ambulatory Care. Cochrane Database Syst. Rev. 2005, 2005, CD003539. [Google Scholar] [CrossRef]
- Boonacker, C.W.B.; Hoes, A.W.; Dikhoff, M.J.; Schilder, A.G.M.; Rovers, M.M. Interventions in Health Care Professionals to Improve Treatment in Children with Upper Respiratory Tract Infections. Int. J. Pediatr. Otorhinolaryngol. 2010, 74, 1113–1121. [Google Scholar] [CrossRef]
- Bjerrum, L.; Cots, J.M.; Llor, C.; Molist, N.; Munck, A. Effect of Intervention Promoting a Reduction in Antibiotic Prescribing by Improvement of Diagnostic Procedures: A Prospective, before and after Study in General Practice. Eur. J. Clin. Pharmacol. 2006, 62, 913–918. [Google Scholar] [CrossRef]
- Gjelstad, S.; Høye, S.; Straand, J.; Brekke, M.; Dalen, I.; Lindbæk, M. Improving Antibiotic Prescribing in Acute Respiratory Tract Infections: Cluster Randomised Trial from Norwegian General Practice (Prescription Peer Academic Detailing (Rx-PAD) Study). BMJ 2013, 347, f4403. [Google Scholar] [CrossRef]
- Cals, J.W.L.; Butler, C.C.; Hopstaken, R.M.; Hood, K.; Dinant, G.J. Effect of Point of Care Testing for C Reactive Protein and Training in Communication Skills on Antibiotic Use in Lower Respiratory Tract Infections: Cluster Randomised Trial. BMJ 2009, 338, 1112–1115. [Google Scholar] [CrossRef]
- Little, P.; Stuart, B.; Francis, N.; Douglas, E.; Tonkin-Crine, S.; Anthierens, S.; Cals, J.W.L.; Melbye, H.; Santer, M.; Moore, M.; et al. Effects of Internet-Based Training on Antibiotic Prescribing Rates for Acute Respiratory-Tract Infections: A Multinational, Cluster, Randomised, Factorial, Controlled Trial. Lancet 2013, 382, 1175–1182. [Google Scholar] [CrossRef]
- Linder, J.A.; Schnipper, J.L.; Tsurikova, R.; Yu, D.T.; Volk, L.A.; Melnikas, A.J.; Palchuk, M.B.; Olsha-Yehiav, M.; Middleton, B. Electronic Health Record Feedback to Improve Antibiotic Prescribing for Acute Respiratory Infections. Am. J. Manag. Care 2010, 16, e311–e319. [Google Scholar]
- Meeker, D.; Linder, J.A.; Fox, C.R.; Friedberg, M.W.; Persell, S.D.; Goldstein, N.J.; Knight, T.K.; Hay, J.W.; Doctor, J.N. Effect of Behavioral Interventions on Inappropriate Antibiotic Prescribing Among Primary Care Practices: A Randomized Clinical Trial. JAMA 2016, 315, 562–570. [Google Scholar] [CrossRef]
- Gulliford, M.C.; van Staa, T.; Dregan, A.; McDermott, L.; McCann, G.; Ashworth, M.; Charlton, J.; Little, P.; Moore, M.V.; Yardley, L. Electronic Health Records for Intervention Research: A Cluster Randomized Trial to Reduce Antibiotic Prescribing in Primary Care (ECRT Study). Ann. Fam. Med. 2014, 12, 344–351. [Google Scholar] [CrossRef]
- Cals, J.W.L.; Schot, M.J.C.; de Jong, S.A.M.; Dinant, G.J.; Hopstaken, R.M. Point-of-Care C-Reactive Protein Testing and Antibiotic Prescribing for Respiratory Tract Infections: A Randomized Controlled Trial. Ann. Fam. Med. 2010, 8, 124–133. [Google Scholar] [CrossRef]
- Aabenhus, R.; Jensen, J.U.S.; Jørgensen, K.J.; Hróbjartsson, A.; Bjerrum, L. Biomarkers as Point-of-Care Tests to Guide Prescription of Antibiotics in Patients with Acute Respiratory Infections in Primary Care. Cochrane Database Syst. Rev. 2014, 2014, CD010130. [Google Scholar] [CrossRef]
- Huang, Y.; Chen, R.; Wu, T.; Wei, X.; Guo, A. Association between Point-of-Care CRP Testing and Antibiotic Prescribing in Respiratory Tract Infections: A Systematic Review and Meta-Analysis of Primary Care Studies. Br. J. Gen. Pract. 2013, 63, e787–e794. [Google Scholar] [CrossRef]
- Altiner, A.; Brockmann, S.; Sielk, M.; Wilm, S.; Wegscheider, K.; Abholz, H.H. Reducing Antibiotic Prescriptions for Acute Cough by Motivating GPs to Change Their Attitudes to Communication and Empowering Patients: A Cluster-Randomized Intervention Study. J. Antimicrob. Chemother. 2007, 60, 638–644. [Google Scholar] [CrossRef]
- Coxeter, P.; del Mar, C.B.; Mcgregor, L.; Beller, E.M.; Hoffmann, T.C. Interventions to Facilitate Shared Decision Making to Address Antibiotic Use for Acute Respiratory Infections in Primary Care. Cochrane Database Syst. Rev. 2015, 2015, CD010907. [Google Scholar] [CrossRef]
- Worrall, G.J.; Kettle, A.; Graham, W.; Hutchinson, J. Postdated versus Usual Delayed Antibiotic Prescriptions in Primary Care: Reduction in Antibiotic Use for Acute Respiratory Infections? Can. Fam. Physician 2010, 56, 1032–1036. [Google Scholar]
- Smith, R.; Coast, J. The True Cost of Antimicrobial Resistance. BMJ 2013, 346, f1493. [Google Scholar] [CrossRef]
- Rocha, V.; Estrela, M.; Roque, F.; Figueiras, A.; Herdeiro, M.T. Educational Interventions to Reduce/Improve Prescription and Dispensing of Antibiotics in Primary Care: A Systematic Review of Economic Impact. PROSPERO 2022 CRD42022311272. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022311272 (accessed on 7 July 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating Guidance for Reporting Systematic Reviews: Development of the PRISMA 2020 Statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Joanna Briggs Institute. Joanna Briggs Institute Critical Appraisal Checklist for Economic Evaluations. Available online: https://jbi.global/critical-appraisal-tools (accessed on 23 May 2022).
- Gomersall, J.S.; Jadotte, Y.T.; Xue, Y.; Lockwood, S.; Riddle, D.; Preda, A. Conducting Systematic Reviews of Economic Evaluations. Int. J. Evid.-Based Healthc. 2015, 13, 170–178. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What Kind of Systematic Review Should I Conduct? A Proposed Typology and Guidance for Systematic Reviewers in the Medical and Health Sciences. BMC Med. Res. Methodol. 2018, 18, 5. [Google Scholar] [CrossRef]
- Farris, K.B.; Kirking, D.M.; Shimp, L.A.; Opdycke, R.A.C. Design and Results of a Group Counter-Detailing DUR Educational Program. Pharm. Res. 1996, 13, 1445–1452. [Google Scholar] [CrossRef]
- O’Connor, P.J.; Amundson, G.; Christianson, J. Performance Failure of an Evidence-Based Upper Respiratory Infection Clinical Guideline. J. Fam. Pract. 1999, 48, 690–697. [Google Scholar]
- Ornstein, S.M. Medication Cost Information in a Computer-Based Patient Record System: Impact on Prescribing in a Family Medicine Clinical Practice. Arch. Fam. Med. 1999, 8, 118–121. [Google Scholar] [CrossRef]
- Hux, J.E.; Melady, M.P.; DeBoer, D. Confidential Prescriber Feedback and Education to Improve Antibiotic Use in Primary Care. CMAJ 1999, 161, 388–392. [Google Scholar]
- Fürst, J.; Čižman, M.; Mrak, J.; Kos, D.; Campbell, S.; Coenen, S.; Gustafsson, L.L.; Fürst, L.; Godman, B. The Influence of a Sustained Multifaceted Approach to Improve Antibiotic Prescribing in Slovenia during the Past Decade: Findings and Implications. Expert Rev. Anti-Infect. Ther. 2015, 13, 279–289. [Google Scholar] [CrossRef]
- McNulty, C.A.M.; Kane, A.; Foy, C.J.W.; Sykes, J.; Saunders, P.; Cartwright, K.A.V. Primary Care Workshops Can Reduce and Rationalize Antibiotic Prescribing. J. Antimicrob. Chemother. 2000, 46, 493–499. [Google Scholar] [CrossRef]
- Chazan, B.; zur Turjeman, R.B.; Frost, Y.; Besharat, B.; Tabenkin, H.; Stainberg, A.; Sakran, W.; Raz, R. Antibiotic Consumption Successfully Reduced by a Community Intervention Program. Isr. Med. Assoc. J. 2007, 9, 16–20. [Google Scholar]
- Aksoy, M.; Isli, F.; Kadi, E.; Varimli, D.; Gursoz, H.; Tolunay, T.; Kara, A.; Unal, S.; Alp Mese, E. Evaluation of More than One Billion Outpatient Prescriptions and Eight-Year Trend Showing a Remarkable Reduction in Antibiotic Prescription in Turkey: A Success Model of Governmental Interventions at National Level. Pharmacoepidemiol. Drug Saf. 2021, 30, 1242–1249. [Google Scholar] [CrossRef]
- Armstrong, E.P.A. Clinical and Economic Outcomes of an Ambulatory Urinary Tract Infection Disease Management Program. Am. J. Manag. Care 2001, 7, 269–280. [Google Scholar] [PubMed]
- Gong, C.L.; Zangwill, K.M.; Hay, J.W.; Meeker, D.; Doctor, J.N. Behavioral Economics Interventions to Improve Outpatient Antibiotic Prescribing for Acute Respiratory Infections: A Cost-Effectiveness Analysis. J. Gen. Intern. Med. 2019, 34, 846–854. [Google Scholar] [CrossRef]
- Michaelidis, C.I.; Kern, M.S.; Smith, K.J. Cost-Effectiveness of Decision Support Strategies in Acute Bronchitis. J. Gen. Intern. Med. 2015, 30, 1505–1510. [Google Scholar] [CrossRef]
- Pittenger, K.; Williams, B.L.; Mecklenburg, R.S.; Blackmore, C.C. Improving Acute Respiratory Infection Care through Nurse Phone Care and Academic Detailing of Physicians. J. Am. Board Fam. Med. 2015, 28, 195–204. [Google Scholar] [CrossRef]
- Walker, S.; Willey, C.W. Impact on Drug Costs and Utilization of a Clinical Pharmacist in a Multisite Primary Care Medical Group. J. Manag. Care Pharm. 2004, 10, 345–354. [Google Scholar] [CrossRef]
- Cals, J.W.L.; Ament, A.J.H.A.; Hood, K.; Butler, C.C.; Hopstaken, R.M.; Wassink, G.F.; Dinant, G.J. C-Reactive Protein Point of Care Testing and Physician Communication Skills Training for Lower Respiratory Tract Infections in General Practice: Economic Evaluation of a Cluster Randomized Trial. J. Eval. Clin. Pract. 2011, 17, 1059–1069. [Google Scholar] [CrossRef]
- Coenen, S.; van Royen, P.; Michiels, B.; Denekens, J. Optimizing Antibiotic Prescribing for Acute Cough in General Practice: A Cluster-Randomized Controlled Trial. J. Antimicrob. Chemother. 2004, 54, 661–672. [Google Scholar] [CrossRef]
- Dekker, A.R.J.; van der Velden, A.W.; Luijken, J.; Verheij, T.J.M.; van Giessen, A. Cost-Effectiveness Analysis of a GP- and Parent-Directed Intervention to Reduce Antibiotic Prescribing for Children with Respiratory Tract Infections in Primary Care. J. Antimicrob. Chemother. 2019, 74, 1137–1142. [Google Scholar] [CrossRef]
- Oppong, R.; Smith, R.D.; Little, P.; Verheij, T.; Butler, C.C.; Goossens, H.; Coenen, S.; Jowett, S.; Roberts, T.E.; Achana, F.; et al. Cost-Effectiveness of Internet-Based Training for Primary Care Clinicians on Antibiotic Prescribing for Acute Respiratory Tract Infections in Europe. J. Antimicrob. Chemother. 2018, 73, 3189–3198. [Google Scholar] [CrossRef] [PubMed]
- Balcioğlu, H.; Çulhaci, A.; Tirpan, K.; Turan, S. Algorithmic Approach to Upper Respiratory Tract Infections in Primary Care. Biomed. Res. 2017, 28, 7546–7551. [Google Scholar]
- Butler, C.C.; Simpson, S.A.; Dunstan, F.; Rollnick, S.; Cohen, D.; Gillespie, D.; Evans, M.R.; Alam, M.F.; Bekkers, M.J.; Evans, J.; et al. Effectiveness of Multifaceted Educational Programme to Reduce Antibiotic Dispensing in Primary Care: Practice Based Randomised Controlled Trial. BMJ 2012, 344, d8173. [Google Scholar] [CrossRef] [PubMed]
- Figueiras, A.; López-Vázquez, P.; Gonzalez-Gonzalez, C.; Vázquez-Lago, J.M.; Piñeiro-Lamas, M.; López-Durán, A.; Sánchez, C.; Herdeiro, M.T.; Zapata-Cachafeiro, M.; Caamaño, F.; et al. Impact of a Multifaceted Intervention to Improve Antibiotic Prescribing: A Pragmatic Cluster-Randomised Controlled Trial. Antimicrob. Resist. Infect. Control 2020, 9, 195. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, P.; Callan, A.; O’Shea, E.; Duane, S.; Murphy, A.W.; Domegan, C.; Galvin, S.; Vellinga, A. The Cost Effectiveness of the SIMPle Intervention to Improve Antimicrobial Prescribing for Urinary Tract Infection in Primary Care. J. Public Health 2017, 39, e282–e289. [Google Scholar] [CrossRef] [PubMed]
- le Corvoisier, P.; Renard, V.; Roudot-Thoraval, F.; Cazalens, T.; Veerabudun, K.; Canoui-Poitrine, F.; Montagne, O.; Attali, C. Long-Term Effects of an Educational Seminar on Antibiotic Prescribing by GPs: A Randomised Controlled Trial. Br. J. Gen. Pract. 2013, 63, e455. [Google Scholar] [CrossRef]
- Naughton, C.; Feely, J.; Bennett, K. A RCT Evaluating the Effectiveness and Cost-Effectiveness of Academic Detailing versus Postal Prescribing Feedback in Changing GP Antibiotic Prescribing. J. Eval. Clin. Pract. 2009, 15, 807–812. [Google Scholar] [CrossRef]
- Wei, X.; Zhang, Z.; Walley, J.D.; Hicks, J.P.; Zeng, J.; Deng, S.; Zhou, Y.; Yin, J.; Newell, J.N.; Sun, Q.; et al. Effect of a Training and Educational Intervention for Physicians and Caregivers on Antibiotic Prescribing for Upper Respiratory Tract Infections in Children at Primary Care Facilities in Rural China: A Cluster-Randomised Controlled Trial. Lancet Glob. Health 2017, 5, e1258–e1267. [Google Scholar] [CrossRef]
- Wei, X.; Zhang, Z.; Hicks, J.P.; Walley, J.D.; King, R.; Newell, J.N.; Yin, J.; Zeng, J.; Guo, Y.; Lin, M.; et al. Long-Term Outcomes of an Educational Intervention to Reduce Antibiotic Prescribing for Childhood Upper Respiratory Tract Infections in Rural China: Follow-up of a Cluster-Randomised Controlled Trial. PLoS Med. 2019, 16, e1002733. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Dawkins, B.; Hicks, J.P.; Walley, J.D.; Hulme, C.; Elsey, H.; Deng, S.; Lin, M.; Zeng, J.; Wei, X. Cost-Effectiveness Analysis of a Multi-Dimensional Intervention to Reduce Inappropriate Antibiotic Prescribing for Children with Upper Respiratory Tract Infections in China. Trop. Med. Int. Health 2018, 23, 1092–1100. [Google Scholar] [CrossRef]
- Conklin, M.H.; Culley, E.J.; O’Donnell, J. Case Study of the Effects of Office-Based Generic Drug Sampling on Antibiotic Drug Costs and First-Line Antibiotic Prescribing Ratios. J. Manag. Care Pharm. 2009, 15, 55–61. [Google Scholar] [CrossRef]
- Wensing, M.; Broge, B.; Kaufmann-Kolle, P.; Andres, E.; Szecsenyi, J. Quality Circles to Improve Prescribing Patterns in Primary Medical Care: What Is Their Actual Impact? J. Eval. Clin. Pract. 2004, 10, 457–466. [Google Scholar] [CrossRef]
- Me’emary, F.; Ottmani, S.E.; Pio, A.; Baghdadi, S.; Assafin, G.; Koraym, M.; Saleh, M.; Bashour, H.; Seita, A.; Blanc, L. Results of the Feasibility Test of the Practical Approach to Lung Health in the Syrian Arab Republic. East. Mediterr. Health J. 2009, 15, 504–515. [Google Scholar] [CrossRef] [PubMed]
- Madridejos-Mora, R.; Amado-Guirado, E.; Pérez-Rodríguez, M.T. Effectiveness of the Combination of Feedback and Educational Recommendations for Improving Drug Prescription in General Practice. Med. Care 2004, 42, 643–648. [Google Scholar] [CrossRef] [PubMed]
- March-López, P.; Madridejos, R.; Tomas, R.; Boix, L.; Arcenillas, P.; Gómez, L.; Padilla, E.; Xercavins, M.; Martinez, L.; Riera, M.; et al. Impact of a Multifaceted Antimicrobial Stewardship Intervention in a Primary Health Care Area: A Quasi-Experimental Study. Front. Pharmacol. 2020, 11, 398. [Google Scholar] [CrossRef] [PubMed]
- Lanbeck, P.; Ragnarson Tennvall, G.; Resman, F. A Cost Analysis of Introducing an Infectious Disease Specialist-Guided Antimicrobial Stewardship in an Area with Relatively Low Prevalence of Antimicrobial Resistance. BMC Health Serv. Res. 2016, 16, 311. [Google Scholar] [CrossRef] [PubMed]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of Antibiotic Prescribing in Primary Care on Antimicrobial Resistance in Individual Patients: Systematic Review and Meta-Analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef]
- Hay, A.D. Antibiotic Prescribing in Primary Care. BMJ 2019, 364, 1780. [Google Scholar] [CrossRef]
- Saha, S.K.; Hawes, L.; Mazza, D. Improving Antibiotic Prescribing by General Practitioners: A Protocol for a Systematic Review of Interventions Involving Pharmacists. BMJ Open 2018, 8, e020583. [Google Scholar] [CrossRef]
- Sulis, G.; Adam, P.; Nafade, V.; Gore, G.; Daniels, B.; Daftary, A.; Das, J.; Gandra, S.; Pai, M. Antibiotic Prescription Practices in Primary Care in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. PLoS Med. 2020, 17, e1003139. [Google Scholar] [CrossRef]
- Gerber, J.S.; Ross, R.K.; Bryan, M.; Localio, A.R.; Szymczak, J.E.; Wasserman, R.; Barkman, D.; Odeniyi, F.; Conaboy, K.; Bell, L.; et al. Association of Broad- vs Narrow-Spectrum Antibiotics With Treatment Failure, Adverse Events, and Quality of Life in Children With Acute Respiratory Tract Infections. JAMA 2017, 318, 2325–2336. [Google Scholar] [CrossRef]
- Melander, R.J.; Zurawski, D.V.; Melander, C. Narrow-Spectrum Antibacterial Agents. Medchemcomm 2018, 9, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Mollahaliloglu, S.; Alkan, A.; Donertas, B.; Ozgulcu, S.; Akici, A. Assessment of Antibiotic Prescribing at Different Hospitals and Primary Health Care Facilities. Saudi Pharm. J. 2013, 21, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Ait Ouakrim, D.; Cassini, A.; Cecchini, M.; Plachouras, D. The Health and Economic Burden of Antimicrobial Resistance. In Challenges to Tackling Antimicrobial Resistance; Cambridge University Press: Cambridge, UK, 2020; pp. 23–44. [Google Scholar]
- McGowan, J.E. Economic Impact of Antimicrobial Resistance. Emerg. Infect. Dis. 2001, 7, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, I.; Rego, C.; Semedo, G.; Gomes, D.; Figueiras, A.; Roque, F.; Herdeiro, M.T. Systematic Review on the Impact of Guidelines Adherence on Antibiotic Prescription in Respiratory Infections. Antibiotics 2020, 9, 546. [Google Scholar] [CrossRef]
- Jamison, D.T.; Breman, J.G.; Measham, A.R.; Alleyne, G.; Claeson, M.; Evans, D.B.; Jha, P.; Mills, A.; Musgrove, P. (Eds.) Cost-Effectiveness Analysis. In Priorities in Health; Disease Control Priorities Project: Washington, DC, USA, 2006; pp. 39–57. [Google Scholar]
- Shi, C.R.; Nambudiri, V.E. Research Techniques Made Simple: Cost-Effectiveness Analysis. J. Investig. Dermatol. 2017, 137, e143–e147. [Google Scholar] [CrossRef]
- Ibrahim, N.H.; Maruan, K.; Mohd Khairy, H.A.; Hong, Y.H.; Dali, A.F.; Neoh, C.F. Economic Evaluations on Antimicrobial Stewardship Programme: A Systematic Review. J. Pharm. Pharm. Sci. 2017, 20, 397–406. [Google Scholar] [CrossRef]
- Muka, T.; Glisic, M.; Milic, J.; Verhoog, S.; Bohlius, J.; Bramer, W.; Chowdhury, R.; Franco, O.H. A 24-Step Guide on How to Design, Conduct, and Successfully Publish a Systematic Review and Meta-Analysis in Medical Research. Eur. J. Epidemiol. 2020, 35, 49–60. [Google Scholar] [CrossRef]

{kind=link}
| Author Year, Country | Antibiotic-Related Measures (Not Cost-Related) | Type of Economic Evaluation | Antibiotics Cost before Intervention or in the CG | Antibiotics Cost after Intervention or in the IG | Cost of the Intervention(s) | Incremental Cost-Effectiveness (Change in Costs) | Interpretation |
|---|---|---|---|---|---|---|---|
| Aksoy et al., 2021 [45] Turkey | -Reduction in antibiotics prescriptions from 34.94 to 30.25% -Reduction in antibiotics items from 14.14 to 4.12% -Reduction in antibiotics boxes from 12.71 to 6.64% | Cost analysis | -Antibiotics cost before intervention: 11.38% | -Antibiotics cost after intervention: 4.12% | NR | Costs savings of 7.26% | Favor intervention |
| Armstrong 2001 [46] USA | -Kidney infection: 49% success rate with the antibiotics treatment guideline compared to 42% with no guideline (p = 0.59) -Bladder infection: 72% success rate with the antibiotics treatment guideline compared to 42% with no guideline (p = 0.68) | Cost minimization analysis | Before intervention: Kidney infection event cost: 452 ± USD 1287~452 ± 1287 ppp Bladder infection event cost: 125 ± USD 611~125 ± 611 ppp | After intervention: Kidney infection event cost: 289 ± USD 470~289 ± 470 ppp Bladder infection event cost: 116 ± USD 400~116 ± 400 ppp | NR | -Decrease of 36% in health event costs (p = 0.696) -Decrease of 7% in health event costs (p < 0.05) | Favor intervention |
| Balcioğlu et al., 2017 [55] Turkey | APR: IG (Algorithm group): n = 23 (0.1%) CG: n = 65 (0.4%) | Cost analysis | Prescription cost in CG: TRY 26.9~19.44 ppp | Prescription cost in IG: TRY 15.4~11.13 ppp | NR | Cost savings of 8.31 ppp | Favor intervention |
| Butler et al., 2012 [56] UK | -Reduction of 4.2% (95% confidence interval 0.6% to 7.7%) in total oral antibiotic dispensing per 1000 patients -No significant differences in hospital admissions and re-consultation rates between IG and CG | Cost analysis | Antibiotics costs in baseline: CG: GBP 2254.6~3211.68 ppp IG: GBP 2199.7~3133.48 ppp | Antibiotics costs in follow-up CG: GBP 2252.3~3208.40 ppp IG: GBP 2078.9~2961.40 ppp | Total costs of intervention: GBP 96,460~137,407.41 ppp | -Cost savings of GBP 120.8~172.08 ppp in the intervention group -Decrease of 5.5% (−0.4; 11.4, p = 0.07) in antibiotic cost | Favor intervention |
| Cals et al., 2011 [51] Netherlands | -IG1 (CRP group): 43 ± 39.1 antibiotics at index consultation; 3.35 ± 4.54 days of work; EUR 98 ± 89.1 diary cost -IG2 (Communication skills training group): 28 ± 33.3 antibiotics at index consultation; 3.37 ± 4.02 days of work; EUR 74 ± 88.1 diary cost -IG3 (CRP + communication skills training group): 27 ± 23.1 antibiotics at index consultation; 3.39 ± 4.08 days of work; EUR 110 ± 94 diary cost -CG (Usual care): 80 ± 66.71 antibiotics at index consultation; 3.37 ± 3.77 days of work; EUR 104 ± 86.7 diary cost | Cost effectiveness analysis | NR | NR | Total costs -IG1: EUR 37.58 ± 45.24~117.22 ± 54.11 ppp -IG2: EUR 25.61 ± 44.49~30.63 ± 53.22 ppp -IG3: EUR 37.78 ± 42.08~45.19 ± 50.33 ppp -CG: EUR 35.96 ± 58.12~43.01 ppp | Incremental cost-effectiveness ratio: -IG1: 5.79 -IG2: Dominant -IG3: 4.15 | Favor intervention |
| Chazan et al., 2007 [44] Israel | Seasonal intervention: -change from 27.8 to 23.2 DDD/1000 patients/day in total antibiotics use -NS difference in the narrow-spectrum antibiotics use Continuous intervention: -change from 28.7 to 22.9 DDD/1000 patients/day in total antibiotics use -reduction in broad-spectrum antibiotic use (17.6%) | Cost analysis | NR | NR | NR | -Cost savings of USD 186~186 ppp per 1000/patients/season in the seasonal intervention -Cost savings of USD 330~330 ppp per 1000/patients/season in the continuous intervention | Favor intervention |
| Coenen et al., 2004 [52] Netherlands | In IG: -APR, pre-test: 43%; post-test: 27.4%; −15.6% of change; -Use of recommended antibiotics, pre-test: 40.1%; post-test: 53.8%; −13.6% of change In CG: -APR, pre-test: 37.8%; post-test: 28.7%; −9.1% of change; -Use of recommended antibiotics, pre-test: 37.5%; post-test: 37.4%; −0.1% of change | Cost analysis | Medication cost in CG, pre-test: EUR 21.48~23.66 ppp post-test: EUR 22.35~24.61 ppp | Medication cost in IG, pre-test: EUR 22.35~24.61 ppp post-test: EUR 16.75~18.75 ppp | NR | Change in medication cost: CG: EUR 0.87~0.96 ppp IG: EUR 6.11~6.73 ppp Mean difference: −6.76 (95% CI: −12.30; −1.89) | Favor intervention |
| Conklin et al., 2009 [64] Pennsylvania | In kiosk prescribers: First line APR decreased from 49.1 to 47.0%; median decrease of 2.3% (SD, 13.0%) | Cost analysis | In non-kiosk prescribers: Mean antibiotic cost per claim: USD 33.56~33.56 ppp | In kiosk prescribers: Mean antibiotic cost per claim: USD 29.42~29.42 ppp | NR | A median cost decrease of antibiotic per claim of USD 3.56~3.56 ppp | Favor intervention |
| Dekker et al., 2018 [53] Netherlands | IG: mean antibiotics of 0.25; 4.5 h of work absence; 0.5 h of non-productivity CG: mean antibiotics of 0.50; 3.1 h of work absence; 1.5 h of non-productivity | Cost effectiveness analysis | -Prescribed medication cost per child: EUR 8.81~11.31 ppp -Mean total cost: EUR 207.68 (140–284)~267.28 (18.18; 365.50) ppp | -Prescribed medication cost per child: EUR 4.77~6.14 ppp -Mean total cost: EUR 217.95 (150; 301)~280.50 (193.05; 470.40) ppp | Costs of intervention per child: EUR 2.9~3.73 ppp | Cost savings per child of EUR 4.04~5.20 ppp Mean incremental cost-effectiveness ratio: EUR 0.85~1.09 ppp per percentage decrease in antibiotic prescription | Favor intervention |
| Farris et al., 1996 [38] USA | 1st study period -change in APR: −9.5% -change in amoxicillin ratio: −5.5% 2nd study period -change in APR: −3.2% -change in amoxicillin ratio: −12.1% | Cost analysis | NR | Average cost per prescription: 1st study period, USD 40.54~40.54 ppp 2nd study period, USD 41.08~41.08 ppp | USD 3700~3700 ppp | Cost savings: USD 3784~3784 ppp Net savings: USD 84~84 ppp | Favor intervention |
| Figueiras et al., 2020 [57] Spain | % of reduction in IG relative to CG: -Reduction of −4.23 (95% CI: −5.26; −3.21) DDD in antibiotics for systemic use; -Reduction of −6.51 (95% CI: −7.92; −5.22) DDD in penicillins; -Reduction of −3.89 (95% CI: −6.18; −1.65) DDD in cephalosporins; -Reduction of −3.45 (95% CI: −5.23; −1.70) DDD in macrolides, lincosamides and streptogramins -Reduction of −0.47 (95% CI: −2.37; 0.93) DDD in quinolones; Reduction of −8.97 (95% CI: −13.99; −4.12) in consumption ratio of broad-to narrow-spectrum antibiotics | Cost analysis | NR | NR | Total cost of intervention: 105. EUR 834~168.79 ppp | Savings in absolute direct costs of −4.33% (95% CI: −5.38; −3.29) Savings in cost per physician of −4.33% (95% CI: −5.38; −3.29) Savings in direct costs per 1000 inhabitants −4.46 (95% CI: −5.54; −3.4)% Total direct cost savings of EUR 697.38 (−861.79; −533.22)~−1112.25 (−1374.47; −850.43) ppp | Favor intervention |
| Furst et al., 2015 [42] Slovenia | Antibiotics prescriptions decreased 53% | Cost analysis | NR | NR | Cost of the intervention EUR 325,000~591,596.64 ppp + EUR 500,000~840,336.13 ppp | Cost savings in antibiotics of EUR 13.1 million~22.02 million ppp | Favor intervention |
| Gillespie et al., 2016 [58] Ireland | -IG1 (Arm A): 78.6% antimicrobial prescriptions; EUR 84.2 (SD: 24.6) of cost per consultation; 68.2% first-line antimicrobials -IG2 (Arm B): 75.8% antimicrobial prescriptions; EUR 88.7 (SD: 24.3) of cost per consultation; 66.5% first-line antimicrobials -CG: 66.5% prescriptions; EUR 67 (SD: 26.1) of cost per consultation; 44.1% first-line antimicrobials | Cost effectiveness analysis | Antimicrobial prescriptions cost per consultation in CG: EUR 5.3 (SD: 4.0)~6.68 (SD: 5.04) ppp | Antimicrobial prescriptions cost per consultation: -IG1: EUR 5.1 (SD: 3.4)~6.42 (SD: 4.28) ppp -IG2: EUR 5.2 (SD: 3.5)~6.55 (SD: 4.41) ppp | Cost related to intervention set-up, audit and feedback -IG1: EUR 16.3~20.53 ppp per consultation -IG2: EUR 16.4~20.65 ppp per consultation | ICERs per % increase in first-line antimicrobial prescription for UTI: -IG1: EUR 64.2 (95% CI: 22.0, 121.8)~80.86 (95% CI: 27.71; 153.40) ppp -IG2: EUR 105.4 (95% CI: 46.6, 241.7)~132.75 (95% CI: 58.69; 304.41) ppp | Favor intervention |
| Gong et al., 2019 [47] USA | -CG: 14.68 QALYs; Intervention cost of 178.21$~178.21 ppp -IG1 (suggested alternatives): 14.73 QALYs; Intervention cost of USD 173.22~173.22 ppp -IG2 (accountable justifications): 14.74 QALYs; Intervention cost of USD 172.82~172.82 ppp -IG3 (peer comparison): 14.74 QALYs; Intervention cost of USD 172.52~172.52 ppp | Cost effectiveness analysis | NR | NR | Cost of implementation-IG1: 1.91 (0–5.73) -IG2 3.82 (0–9.55) -IG3 0.95 (0–3.82) | Overall budget impact: -CG: USD17.82 million~17.82 million ppp -IG1: USD 17.32 million~17.32 million ppp -IG2: USD 17.28 million~17.28 million ppp -IG3: USD 17.25 million~17.25 million ppp | Favor intervention |
| Hux et al., 1999 [41] Canada | IG: pre, 67.2%; post, 69.8% in first-line antibiotics CG: pre, 68.5%; post, 66.8% in first-line antibiotics (p < 0.001) | Cost analysis | Median antibiotic cost in CG: pre, CAD 10.78~8.77 ppp; post, CAD 14.15~11.52 | Median antibiotic cost in IG: pre, CAD 11.50~9.36 ppp; post, CAD 11.55~9.41 ppp | NR | No savings in median antibiotic cost in the IG and an increase in CG cost | Unclear |
| Lanbeck et al., 2016 [69] Sweden | IG: 7193 days at the hospital; 108 deaths; 180 patients readmitted within 28 days. CG: 7402 days at hospital; 117 deaths; 203 patients readmitted within 28 days. | Cost analysis | Oral antibiotic treatment cost: SEK 94,367~10,695.57 ppp Intravenous antibiotic treatment cost: SEK 690,440~78,254.56 ppp | Oral antibiotic treatment cost: SEK 46,850~5309.99 ppp Intravenous antibiotic treatment cost: SEK 616,264~69,847.44 ppp | Cost of intervention: SEK 161,990~18,359.97 ppp | Cost savings in oral antibiotic of SEK 47,517~5385.58 ppp Cost savings in intravenous antibiotic of SEK 74,176~8407.12 ppp | Favor intervention |
| Le Corvoisier et al., 2013 [59] France | IG: Reduction in antibiotics prescriptions from 15.2 ± 5.4% to 12.3 ± 5.8% (−2.8% [95% CI: −3.8; 1.9]; p < 0.001) CG: Increase in antibiotics prescriptions from 15.3 ± 6.0% to 16.4 ± 6.7% (+1.1% [95% CI; 0.4; 1.8], p < 0.01) | Cost analysis | Cost of antibiotic prescriptions in CG: EUR 393 (95% CI: 201; 585)~429.04 (95% CI: 219.43; 638.65) ppp | Cost of antibiotic prescriptions in IG: -EUR 313 (95% CI: −512; −113)~341.70 (95% CI: −558.95; −123.36) ppp | NR | Significant reduction (EUR 80~87.34 ppp) in antibiotic prescription cost (p < 0.001) | Favor intervention |
| Madridejos-Mora et al., 2004 [67] Spain | Antibiotics over prescription: -IG (individualised feedback group): Pre, 16.4 (SD: 7.27); Post, 16.4 (SD: 6.15); p = 0.986 -CG (minimal intervention group): Pre, 15.7 (SD: 8.44); Post, 13.7 (SD: 6.81); p = 0.006 | Cost analysis | Antibiotics cost in CG: Pre, 3.18 (SD: 1.59) EUR/inhabitant~4.15 (SD: 2.08) ppp/inhabitant Post, 3.25(SD: 1.31) EUR/inhabitant~4.24 (SD: 1.71) ppp/inhabitant | Antibiotics cost in IG: Pre, 2.94 (SD: 1.89) EUR/inhabitant~3.84 (SD: 2.47) ppp/inhabitant Post, 2.49 (SD: 1.42) EUR/inhabitant~3.25 (SD: 1.85) ppp/inhabitant | NR | Significant reduction (EUR −0.45~0.59 ppp/inhabitant) in antibiotic prescription cost (p = 0.004) | Favor intervention |
| March-Lopez et al., 2020 [68] Spain | -A decrease from 26.99 to 22.41% (−4.57%; p < 0.05) in antibiotic consumption -An increase from 31.32 to 32.35% (+1.04%; p < 0.05) in narrow-spectrum antibiotics | Cost analysis | Total antibiotic spending in 2016 (control): EUR 905,700.76~1,444,498.82 ppp | Total antibiotic spending in 2018 (sustainability phase): EUR 793,765.89~1,265,974.31 ppp | NR | Cost savings in antibiotic spending: EUR 111,934.87~178,524.51 ppp | Favor intervention |
| McNulty et al., 2000 [43] UK | -IG (workshop group): a reduction of −2458 (−3.4%) in antibiotics units; a reduction of −139 (−0.9%) in narrow-spectrum antibiotics; a reduction of −1612 (−15.4%) in broad-spectrum antibiotics -CG (non-workshop group): a reduction of −1209 (−2.2%) in antibiotics units; a reduction of −1248 (−11.7%) in narrow-spectrum antibiotics; an increase of 561 (6.5%) in broad-spectrum antibiotics | Cost analysis | CG: an increase of GBP 8710~12,354.61 ppp (3.8%) in antibiotics units; a reduction of -GBP 1160~1645.39 ppp (−10.8%) in narrow- spectrum antibiotics; an increase of GBP 7100~10,070.92 ppp (8.8%) in broad-spectrum antibiotics | IG: a reduction of -GBP 3400~4822.70 ppp (−3.4%) in antibiotics units; an increase of GBP 220~312.06 ppp (1.5%) in narrow- spectrum antibiotics; a reduction of GBP 8330~11,815.60 ppp (−9.3%) in broad-spectrum antibiotics | NR | -Cost savings in antibiotic units of 3.8% (NS) -Cost savings in broad-spectrum antibiotics of −9.3% (p < 0.001) -Cost increase in narrow-spectrum antibiotics of 1.5% (p = 0.016) | Favor intervention |
| Me’emary et al., 2009 [66] Syria | -CG (baseline survey group): 86.5% of antibiotic prescriptions; SYP 356,223~NA ppp of total antibiotics cost -IG (impact survey group): 62.8% of antibiotic prescriptions; SYP 157,182~NA ppp of total antibiotics cost | Cost analysis | CG: 66.5% of total antibiotics cost | IG: 55.1% of total antibiotics cost | NR | Cost savings of −17.1% (p < 0.001) in antibiotics cost | Favor intervention |
| Michaelidis et al., 2015 [48] USA | -IG1 (printed decision support): 3.78 antibiotic prescriptions per 5 cases of disease; <1.9 days of work loss compared to CG; -IG2 (computerized decision support): 3.94 antibiotic prescriptions per 5 cases of disease -CG (usual care): 4.60 antibiotic prescriptions per 5 cases of disease | Cost effectiveness analysis | NR | NR | -IG1: USD 2574~2574 ppp -IG2: USD 2802~2802 ppp -CG: USD 2768~2768 ppp | The IG1 showed to be the most cost-effective strategy to reduce antibiotic use, specifically safely avoiding antibiotics prescriptions of −0.16 and −0.82 (incremental effectiveness) compared to IG2 and CG | Favor intervention |
| Naughton et al., 2008 [60] Ireland | Immediate response: -IG1 (postal bulletin group): decrease of −0.02 (−0.04; −0.001) in APR; increase of 0.02 (0.002; 0.05) in first-line antibiotics; decrease in second-line antibiotics of −0.03 (−0.05; −0.01) in co-amoxiclav and −0.02 (−0.03; −0.007) in cephalosporins -IG2 (academic detailing group): decrease of −0.02 (−0.03; −0.001) in APR; increase of 0.05 (0.01; 0.09) in first-line antibiotics; decrease in second-line antibiotics of −0.03 (−0.05; −0.01) in co-amoxiclav and −0.02 (−0.03; −0.003) in cephalosporins | Cost effectiveness analysis | NR | NR | Total cost of implementation in IG1 was EUR 210,000~222,457.61 ppp with a cost per GP practice of EUR 175~185.38 ppp Total cost of implementation in IG2 was EUR 1,868,000~1,978,814 ppp with a cost per GP practice of EUR 1556~1648.31 ppp | The cost-effectiveness ratio for the IG1 was EUR 88~93.22 ppp per %change in practice compared with EUR 778~824.15 ppp for academic detailing | Favor intervention |
| O’Connor et al., 1999 [39] USA | -Pre-guideline: 24% using antibiotics and 76% not using antibiotics -Post-guideline: 16% using antibiotics and 84% not using antibiotics | Cost analysis | Pre-guideline cost of initial care: USD 37.8~37.8 ppp | Post-guideline cost of initial care: USD 36.2~36.2 ppp | NR | Net savings of 4.2% (NS) | Favor intervention |
| Oppong et al., 2018 [54] Belgium, Netherlands, Poland, Spain, UK | -EG1 (CRP group): 222 (33.64%) antibiotic prescriptions; 0.0651 QALYs; -EG2 (Communication skills group): 303 (40.95%) antibiotic prescriptions; 0.0651 QALYs; -EG3 (CRP + communication skills group): 242 (34.13%) antibiotic prescriptions; 0.0648 QALYs -CG (Usual care): 307 (59.61%) antibiotic prescriptions; 0.065 QALYs; | Cost effectiveness analysis | Antibiotic cost: -CG: EUR 27.96~41.24 ppp | Antibiotic cost: -EG1: EUR 49.34~72.77 ppp -EG2: EUR 39.56~58.35 ppp -EG3: EUR 60.32~88.97 ppp | Cost of delivering the intervention: -EG1: EUR 11.42 (SD: 7.45)~16.84 (SD: 10.99) ppp -EG2: EUR 5.62 (SD: 3.69)~8.29 (SD: 5.44) ppp -EG3: EUR 13.43 (SD: 8.53)~19.81 (SD: 12.58) ppp | -EG3: ICER of EUR 338.89~499.84 ppp -EG1: ICER of EUR 176.53~260.37 ppp -EG2: ICER of EUR 68.80~101.47 ppp All per percentage reduction in antibiotic prescription when compared with CG | Favor intervention |
| Ornstein et al., 1999 [40] USA | CG (non-cost information in prescriptions): 23.85% of antibiotics prescriptions EG (cost information in prescriptions): 21.59% of antibiotics prescriptions p = 0.001 | Cost analysis | CG: USD 14.51~14.51 ppp mean antibiotic prescription cost; 15.85% total prescription costs | EG: USD 16.85~16.85 ppp mean antibiotic prescription cost; 16.15% total prescription costs | The mean cost per contact: CG: 12.49 ± 29.35 $~12.49 ± 29.35 ppp EG: 13.03 ± 30.06 $~13.03 ± 30.06 ppp NS difference | An increase (USD 2.34~2.34 ppp) in mean antibiotic cost (p = 0.002) and in % of total antibiotic cost | Reject intervention |
| Pittenger et al., 2014 [49] USA | -A decrease of −29.4% in APR per ARI episode (absolute decrease −16.5 %points, 95% CI: −20.5; −12.5; p < 0.001) -A decrease of −9.4% in number of ARI episodes (p = 0.25) -A decrease of −17.0% in ARI primary care visits (p = 0.035) | Cost analysis | NR | NR | Cost of academic detailing per year was USD 35,192 (33,315; 37,069)~35,192 (33,315; 37,069) ppp | Cost savings related to the intervention -from the payer perspective: -avoided antibiotic prescription per year: USD 21,539 (16,317; 26,763)~21,539 (16,317; 26,763) ppp -total annual cost: USD 178,000~178,000 ppp -from the healthcare perspective: -visits avoided per year: USD 156,806 (152,358; 160,384)~156,806 (152,358; 160,384) ppp -Antibiotic costs avoided per year: USD 21,539 (16,317; 26,763)~21,539 (16,317; 26,763) ppp | Favor intervention |
| Schwartz et al., 2021 [2] Canada | Total antibiotic prescriptions (Relative risk): -IG1 (mailed letter on antibiotic initiation) versus CG (no letter): 0.96 (0.92; 1.01), p = 0.06 -IG2 (mailed letter on antibiotic duration) versus CG: 0.95 (0.91; 1.00), p = 0.01 -IG1 versus IG2: 0.99 (0.96; 1.02), p = 0.42 -IG1 and EG2 versus CG: 0.96 (0.92; 1.00), p = 0.02 Prolonged-duration prescriptions (>7 days) (Relative risk): -IG1 versus CG: 0.98 (0.93; 1.03), p = 0.42 -IG2 versus CG: 0.92 (0.87; 0.97), p < 0.001 -IG1 versus IG2: 0.94 (0.90; 0.98), p = 0.001 -IG1 and IG2 versus CG: 0.95 (0.91; 1.00), p = 0.02 | Cost analysis | NR | Antibiotic costs (Relative risk): -IG1 versus CG: 0.97 (0.92; 1.02), p = 0.19 -IG2 versus CG: 0.94 (0.89; 0.99), p = 0.01 -IG1 versus IG2: 0.97 (0.93; 1.00), p = 0.03 -IG1 and IG2 versus CG: 0.96 (0.91; 1.00), p = 0.03 | NR | The initiation letter (IG1) had no statistically significant effect. Compared with CG, the duration letter (IG2) resulted in 42 fewer antibiotic prescriptions, 24 fewer prolonged-duration prescriptions, and CAD 771~599.07 ppp in drug cost savings on average per PCP over 12 months. | Favor intervention |
| Walker et al., 2004 [50] USA | In 1998: 1.17 of antibiotics; 13.6% of total drugs volume In 1999: 1.08 of antibiotics; 12.1% of total drugs volume A reduction of −8.1%. | Cost analysis | In 1998: USD 19.38~19.38 ppp mean antibiotic cost per claim; 7.9% of total cost; USD 16.46~16.46 ppp mean antibiotic cost per prescription | In 1999: USD 15.09~15.09 ppp mean antibiotic cost per claim; 6.1% of total cost; USD 14.04~14.04 ppp mean antibiotic cost per prescription | NR | The average antibiotic cost per claim decreased 14.7%; The average antibiotic cost per claim decreased 22.1%; The decrease in the cost per claim for antibiotics resulted from an increase in the use of generic first-line antibiotics | Favor intervention |
| Wei et al., 2017 [61] China | IG (educational intervention) versus CG: -a reduction of −30% (−43 to −17) in the APR; -an increase of 2% (−1 to 5) in the multiple APR; -an increase of 5% (−10 to 20) in broad-spectrum APR; -a reduction of −8% (−20 to 5) in the intravenous APR. | Cost effectiveness analysis | CG: Antibiotic cost > Individual-Baseline: USD 0.5 (0.4)~0.5 (0.4) ppp Endline: USD 0.5 (0.4)~0.5 (0.4) ppp Cluster–Baseline: USD 0.7 (0.07)~0.7 (0.07) ppp Endline: USD 0.7 (0.06)~0.7 (0.06) ppp | IG: Antibiotic cost > Individual-Baseline: USD 0.6 (0.4)~0.6 (0.4) ppp Endline: USD 0.3 (0.4)~0.3 (0.4) ppp Cluster–Baseline: 0.7 (0.04)$~0.7 (0.04) ppp Endline: USD 0.7 (0.05)~0.7 (0.05) | NR | No significant effect of the intervention on the full prescription cost [adjusted mean difference: 0.01 (−0.03 to 0.05)] The mean antibiotic cost was significantly lower in the IG than in CG, although the crude results showed no significant difference | Reject intervention |
| Wei et al., 2019 [62] China | After the intervention (Antimicrobial stewardship programme > -Reduction in the APR of −49%points (95% CI: −63; −35, p < 0.0001); -A modest reduction in the broad-spectrum APR (−12%points (95% CI: −21; −4); After the follow-up> -Reduction in the antibiotic prescription rate of −36% points (95% CI: −55; −17, p < 0.0001); -A moderate reduction in the broad-spectrum APR (−20% points (95% CI: −34; −6). | Cost effectiveness analysis | Antibiotic cost in CG Baseline: USD 0.5 (±0.4)~0.5 (±0.4) ppp Post intervention: USD 0.5 (±0.4)~0.5 (±0.4) ppp Post follow-up: USD 0.5 (±0.4)~0.5 (±0.4) ppp | Antibiotic cost in IG Baseline: USD 0.6 (±0.4)~0.6 (±0.4) ppp Post intervention: USD 0.3 (±0.4)~0.3 (±0.4) ppp Post follow-up: USD 0.4 (±0.4)~0.4 (±0.4) ppp | NR | -After the intervention, a reduction in the cost of antibiotics per prescription of −0.35 (95% CI: −0.45; −0.25)$~−0.35 (95% CI: −0.45; −0.25) ppp -After the follow-up, a reduction in the cost of antibiotics of −0.26 (95% CI: −0.38; −0.13)$~−0.26 (95% CI: −0.38; −0.13) ppp | Favor intervention |
| Wensing et al., 2004 [65] Germany | -APR EG> baseline: 83.1%; post-intervention: 76.7% CG> baseline: 86.1%; post-intervention: 75.8% -Recommended Antibiotics EG> baseline: 46.3%; post-intervention: 47.2% CG> baseline: 43.6%; post-intervention: 44.6% | Cost analysis | Antibiotic costs per prescription: CG> baseline: EUR 21.6~24.69 ppp Post-intervention: EUR 20.9~23.89 ppp | Antibiotic costs per prescription: EG> baseline: EUR 22.5~25.71 ppp Post-intervention: EUR 21.2~24.23 ppp | NR | The intervention effect on antibiotic cost was a decrease of EUR −0.92~1.05 ppp (p < 0.20) | Favor intervention |
| Zang et al., 2018 [63] China | CG> APR: 70 (SD: 14); 4.79 (SD: 1.64) of total healthcare cost; EG> APR: 40 (SD: 19); 5.16 (SD: 1.94) of total healthcare cost; Difference of −29 (95% CI: −42; −16, p < 0.001) in APR and 1.02 (95% CI: −0.36; 2.4; p > 0.05) | Cost effectiveness analysis | Cost per %point decrease in APR in CG: USD 4.83~4.83 ppp | Cost per %point decrease in APR in EG > USD 5.33~5.33 ppp Incremental cost per percentage point reduction in APR: USD 1.02 (−0.36; 2.4)~1.02 (−0.36; 2.4) ppp | USD 390.65 (SD: 145.68)~390.65 (SD 145.68) ppp per facility, including doctors training and information resources for patients | The APR in the IG reduced by 29.23% points at an additional cost of USD 1.02 (−0.36; 2.4)~1.02 (−0.36; 2.4) ppp per patient compared to the CG, producing an ICER of USD 0.03~0.03 ppp per %point reduction in APR | Favor intervention |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rocha, V.; Estrela, M.; Neto, V.; Roque, F.; Figueiras, A.; Herdeiro, M.T. Educational Interventions to Reduce Prescription and Dispensing of Antibiotics in Primary Care: A Systematic Review of Economic Impact. Antibiotics 2022, 11, 1186. https://doi.org/10.3390/antibiotics11091186
Rocha V, Estrela M, Neto V, Roque F, Figueiras A, Herdeiro MT. Educational Interventions to Reduce Prescription and Dispensing of Antibiotics in Primary Care: A Systematic Review of Economic Impact. Antibiotics. 2022; 11(9):1186. https://doi.org/10.3390/antibiotics11091186
Chicago/Turabian StyleRocha, Vânia, Marta Estrela, Vanessa Neto, Fátima Roque, Adolfo Figueiras, and Maria Teresa Herdeiro. 2022. "Educational Interventions to Reduce Prescription and Dispensing of Antibiotics in Primary Care: A Systematic Review of Economic Impact" Antibiotics 11, no. 9: 1186. https://doi.org/10.3390/antibiotics11091186
APA StyleRocha, V., Estrela, M., Neto, V., Roque, F., Figueiras, A., & Herdeiro, M. T. (2022). Educational Interventions to Reduce Prescription and Dispensing of Antibiotics in Primary Care: A Systematic Review of Economic Impact. Antibiotics, 11(9), 1186. https://doi.org/10.3390/antibiotics11091186