
Population Pharmacokinetic and Pharmacodynamic Analysis of Dalbavancin for Long-Term Treatment of Subacute and/or Chronic Infectious Diseases: The Major Role of Therapeutic Drug Monitoring

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Results
2.1. Population Characteristics
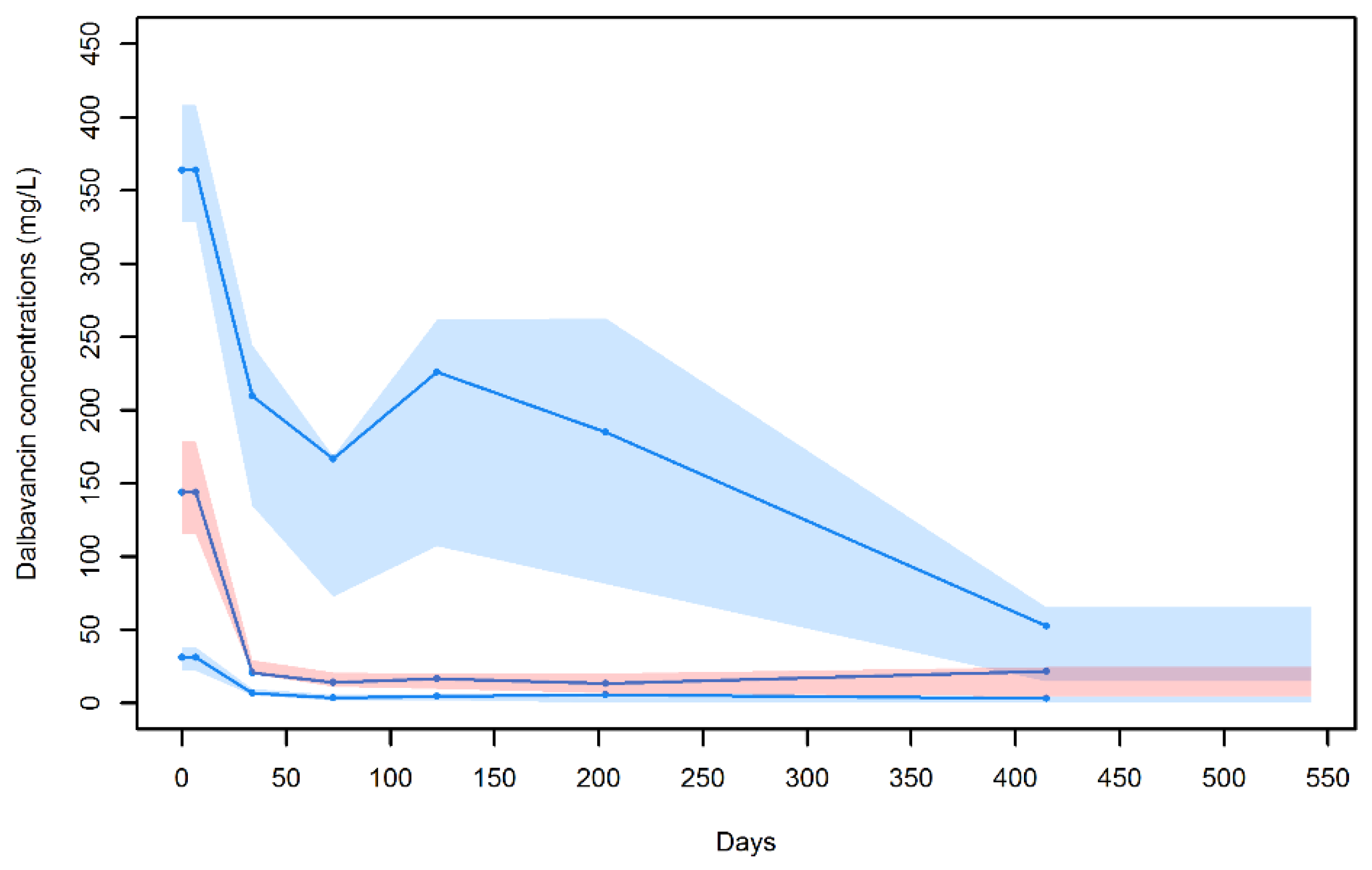
2.2. Population Pharmacokinetic Modeling
2.3. Monte Carlo Simulation for Estimating Pharmacodynamic Target Attainment
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Population Pharmacokinetic Modeling
4.3. Model Evaluation
4.4. Monte Carlo Simulation for Pharmacodynamic Target Attainment
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tong, S.Y.; Davis, J.S.; Eichenberger, E.; Holland, T.L.; Fowler, V.G., Jr. Staphylococcus aureus infections: Epidemiology, pathophysiology, clinical manifestations, and management. Clin. Microbiol. Rev. 2015, 28, 603–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karaman, R.; Jubeh, B.; Breijyeh, Z. Resistance of Gram-Positive Bacteria to Current Antibacterial Agents and Overcoming Approaches. Molecules 2020, 25, 2888. [Google Scholar] [CrossRef]
- Oliva, A.; Stefani, S.; Venditti, M.; Di Domenico, E.G. Biofilm-Related Infections in Gram-Positive Bacteria and the Potential Role of the Long-Acting Agent Dalbavancin. Front. Microbol. 2021, 12, 749685. [Google Scholar] [CrossRef]
- Purrello, S.M.; Garau, J.; Giamarellos, E.; Mazzei, T.; Pea, F.; Soriano, A.; Stefani, S. Methicillin-resistant Staphylococcus aureus infections: A review of the currently available treatment options. J. Glob. Antimicrob. Resist. 2016, 7, 178–186. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.R.; Roberts, K.D.; Rybak, M.J. Dalbavancin: A Novel Lipoglycopeptide Antibiotic with Extended Activity Against Gram-Positive Infections. Infect. Dis. Ther. 2015, 4, 245–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina, K.C.; Miller, M.A.; Mueller, S.W.; Van Matre, E.T.; Krsak, M.; Kiser, T.H. Clinical Pharmacokinetics and Pharmacodynamics of Dalbavancin. Clin. Pharmacokinet. 2022, 61, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Gatti, M.; Andreoni, M.; Pea, F.; Viale, P. Real-World Use of Dalbavancin in the Era of Empowerment of Outpatient Antimicrobial Treatment: A Careful Appraisal Beyond Approved Indications Focusing on Unmet Clinical Needs. Drug Des. Dev. Ther. 2021, 15, 3349–3378. [Google Scholar] [CrossRef]
- Dunne, M.W.; Puttagunta, S.; Sprenger, C.R.; Rubino, C.; Van Wart, S.; Baldassarre, J. Extended-duration dosing and distribution of dalbavancin into bone and articular tissue. Antimicrob. Agents Chemother. 2015, 59, 1849–1855. [Google Scholar] [CrossRef] [Green Version]
- Cojutti, P.G.; Rinaldi, M.; Zamparini, E.; Rossi, N.; Tedeschi, S.; Conti, M.; Pea, F.; Viale, P. Population pharmacokinetics of dalbavancin and dosing consideration for optimal treatment of adult patients with staphylococcal osteoarticular infections. Antimicrob. Agents Chemother. 2021, 65, e02260-20. [Google Scholar] [CrossRef]
- Cojutti, P.G.; Rinaldi, M.; Gatti, M.; Tedeschi, S.; Viale, P.; Pea, F. Usefulness of therapeutic drug monitoring in estimating the duration of dalbavancin optimal target attainment in staphylococcal osteoarticular infections: A proof-of-concept. Int. J. Antimicrob. Agents 2021, 58, 106445. [Google Scholar] [CrossRef]
- Buckwalter, M.; Dowell, J.A. Population pharmacokinetic analysis of dalbavancin, a novel lipoglycopeptide. J. Clin. Pharmacol. 2005, 45, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Carrothers, T.J.; Chittenden, J.T.; Critchley, I. Dalbavancin Population Pharmacokinetic Modeling and Target Attainment Analysis. Clin. Pharmacol. Drug Dev. 2020, 9, 21–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marbury, T.; Dowell, J.A.; Seltzer, E.; Buckwalter, M. Pharmacokinetics of dalbavancin in patients with renal or hepatic impairment. J. Clin. Pharmacol. 2009, 49, 465–476. [Google Scholar] [CrossRef] [PubMed]
- Leighton, A.; Gottlieb, A.B.; Dorr, M.B.; Jabes, D.; Mosconi, G.; VanSaders, C.; Mroszczak, E.J.; Campbell, K.C.; Kelly, E. Tolerability, pharmacokinetics, and serum bactericidal activity of intravenous dalbavancin in healthy volunteers. Antimicrob. Agents Chemother. 2004, 48, 940–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morata, L.; Cobo, J.; Fernandez-Sampedro, M.; Guisado Vasco, P.; Ruano, E.; Lora-Tamayo, J.; Sanchez Somolinos, M.; Gonzalez Ruano, P.; Rico Nieto, A.; Arnaiz, A.; et al. Safety and Efficacy of Prolonged Use of Dalbavancin in Bone and Joint Infections. Antimicrob. Agents Chemother. 2019, 63, e02280-18. [Google Scholar] [CrossRef] [Green Version]
- Almangour, T.A.; Perry, G.K.; Terriff, C.M.; Alhifany, A.A.; Kaye, K.S. Dalbavancin for the management of gram-positive osteomyelitis: Effectiveness and potential utility. Diagn. Microbiol. Infect. Dis. 2019, 93, 213–218. [Google Scholar] [CrossRef]
- Hidalgo-Tenorio, C.; Vinuesa, D.; Plata, A.; Martin Davila, P.; Iftimie, S.; Sequera, S.; Loeches, B.; Lopez-Cortes, L.E.; Farinas, M.C.; Fernandez-Roldan, C.; et al. DALBACEN cohort: Dalbavancin as consolidation therapy in patients with endocarditis and/or bloodstream infection produced by gram-positive cocci. Ann. Clin. Microbiol. Antimicrob. 2019, 18, 30. [Google Scholar] [CrossRef] [Green Version]
- Tobudic, S.; Forstner, C.; Burgmann, H.; Lagler, H.; Ramharter, M.; Steininger, C.; Vossen, M.G.; Winkler, S.; Thalhammer, F. Dalbavancin as Primary and Sequential Treatment for Gram-Positive Infective Endocarditis: 2-Year Experience at the General Hospital of Vienna. Clin. Infect. Dis. 2018, 67, 795–798. [Google Scholar] [CrossRef]
- Raad, I.; Darouiche, R.; Vazquez, J.; Lentnek, A.; Hachem, R.; Hanna, H.; Goldstein, B.; Henkel, T.; Seltzer, E. Efficacy and safety of weekly dalbavancin therapy for catheter-related bloodstream infection caused by gram-positive pathogens. Clin. Infect. Dis. 2005, 40, 374–380. [Google Scholar] [CrossRef]
- Kussmann, M.; Karer, M.; Obermueller, M.; Schmidt, K.; Barousch, W.; Moser, D.; Nehr, M.; Ramharter, M.; Poeppl, W.; Makristathis, A.; et al. Emergence of a dalbavancin induced glycopeptide/lipoglycopeptide non-susceptible Staphylococcus aureus during treatment of a cardiac device-related endocarditis. Emerg. Microb. Infect. 2018, 7, 202. [Google Scholar] [CrossRef] [Green Version]
- Bartoletti, M.; Mikus, E.; Pascale, R.; Giannella, M.; Tedeschi, S.; Calvi, S.; Tenti, E.; Tumietto, F.; Viale, P. Clinical experience with dalbavancin for the treatment of deep sternal wound infection. J. Glob. Antimicrob. Resist. 2019, 18, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Lepak, A.; Marchillo, K.; VanHecker, J.; Andes, D. Impact of Glycopeptide Resistance in Staphylococcus aureus on the Dalbavancin In Vivo Pharmacodynamic Target. Antimicrob. Agents Chemother. 2015, 59, 7833–7836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alebic-Kolbah, T.; Demers, R.; Cojocaru, L. Dalbavancin: Quantification in human plasma and urine by a new improved high performance liquid chromatography-tandem mass spectrometry method. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2011, 879, 2632–2641. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Demographics | |
|---|---|
| Total number of patients | 69 |
| Age (years) | 62 (51–73) |
| Gender (male/female) | 44/25 |
| Weight (kg) | 75 (62–88) |
| Height (cm) | 170 (165–177) |
| Baseline laboratory parameters | |
| CLCR (mL/min/1.73 m2) | 93.0 (72.0–104.0) |
| Albumin (g/dL) | 3.7 (3.3–4.0) |
| C-RP (mg/L) | 3.21 (1.41–6.26) |
| Type of infections | |
| Prosthetic joint infection | 26 (37.7) |
| Osteomyelitis | 11 (15.9) |
| Endovascular prosthetic infections | 9 (13.0) |
| Endocarditis | 7 (10.1) |
| Spondilodiscitis | 5 (7.2) |
| Infected pseudoarthrosis non-unions | 4 (5.8) |
| Septic arthritis | 1 (1.5) |
| Multiple site infections | |
| Endocarditis + spondilodiscitis | 2 (2.9) |
| Endocarditis + septic arthitis | 1 (1.5) |
| Endovascular prosthetic infection + spondilodiscitis | 2 (2.9) |
| Endovascular prosthetic infection + osteomyelitis | 1 (1.5) |
| Patients with identified microbiological isolates | 63 (91.3) |
| Dalbavancin treatment | |
| Number of doses per patient | 2 (2–4) |
| Number of TDM instances per patient | 3 (2–5) |
| Parameter | Base Model Typical Value (%RSE) | Final Model Typical Value (%RSE) |
|---|---|---|
| Fixed-Effects | ||
| CL (L/h) | 0.041 (4.91) | 0.029 (11.6) |
| βCLcr-CL | - | 0.0043 (28.9) |
| V1 (L) | 6.15 (4.79) | 6.14 (5.26) |
| Q (L/h) | 0.026 (17.9) | 0.026 (18.1) |
| V2 (L) | 10.51 (13.7) | 9.52 (19.0) |
| Random Effects (Inter-patient %CV) | ||
| IIVCL | 31.76 (16.2) | 26.44 (13.3) |
| IIVV1 | 16.10 (33.2) | 16.10 (40.1) |
| IIVQ | 45.06 (34.6) | 50.90 (32.9) |
| IIVV2 | 37.19 (207) | 37.15 (61.7) |
| Residual variability | ||
| b (proportional) | 33.92 (7.96) | 33.92 (5.97) |
| Drug Dosages | Classes of CLCR (mL/min/1.73 m2) | |||
|---|---|---|---|---|
| ≤30 | 30–59 | 60–89 | 90–120 | |
| 1000 d1 + 1000 d8 | 28 ± 3 | - | - | - |
| 1500 d1 + 1500 d8 | - | 35 ± 3 | 28 ± 3 | 21 ± 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cojutti, P.G.; Tedeschi, S.; Gatti, M.; Zamparini, E.; Meschiari, M.; Siega, P.D.; Mazzitelli, M.; Soavi, L.; Binazzi, R.; Erne, E.M.; et al. Population Pharmacokinetic and Pharmacodynamic Analysis of Dalbavancin for Long-Term Treatment of Subacute and/or Chronic Infectious Diseases: The Major Role of Therapeutic Drug Monitoring. Antibiotics 2022, 11, 996. https://doi.org/10.3390/antibiotics11080996
Cojutti PG, Tedeschi S, Gatti M, Zamparini E, Meschiari M, Siega PD, Mazzitelli M, Soavi L, Binazzi R, Erne EM, et al. Population Pharmacokinetic and Pharmacodynamic Analysis of Dalbavancin for Long-Term Treatment of Subacute and/or Chronic Infectious Diseases: The Major Role of Therapeutic Drug Monitoring. Antibiotics. 2022; 11(8):996. https://doi.org/10.3390/antibiotics11080996
Chicago/Turabian StyleCojutti, Pier Giorgio, Sara Tedeschi, Milo Gatti, Eleonora Zamparini, Marianna Meschiari, Paola Della Siega, Maria Mazzitelli, Laura Soavi, Raffaella Binazzi, Elke Maria Erne, and et al. 2022. "Population Pharmacokinetic and Pharmacodynamic Analysis of Dalbavancin for Long-Term Treatment of Subacute and/or Chronic Infectious Diseases: The Major Role of Therapeutic Drug Monitoring" Antibiotics 11, no. 8: 996. https://doi.org/10.3390/antibiotics11080996
APA StyleCojutti, P. G., Tedeschi, S., Gatti, M., Zamparini, E., Meschiari, M., Siega, P. D., Mazzitelli, M., Soavi, L., Binazzi, R., Erne, E. M., Rizzi, M., Cattelan, A. M., Tascini, C., Mussini, C., Viale, P., & Pea, F. (2022). Population Pharmacokinetic and Pharmacodynamic Analysis of Dalbavancin for Long-Term Treatment of Subacute and/or Chronic Infectious Diseases: The Major Role of Therapeutic Drug Monitoring. Antibiotics, 11(8), 996. https://doi.org/10.3390/antibiotics11080996