
Antimicrobial Susceptibility Testing of Porcine Bacterial Pathogens: Investigating the Prospect of Testing a Representative Drug for Each Antimicrobial Family

 and
and 
Abstract
:1. Introduction
2. Results
2.1. Clinical Samples
2.2. MIC Range, MIC50 and MIC90 for the Porcine Pathogens
2.3. Multivariate Analysis of MIC for Twelve Antimicrobials in Each Porcine Pathogen
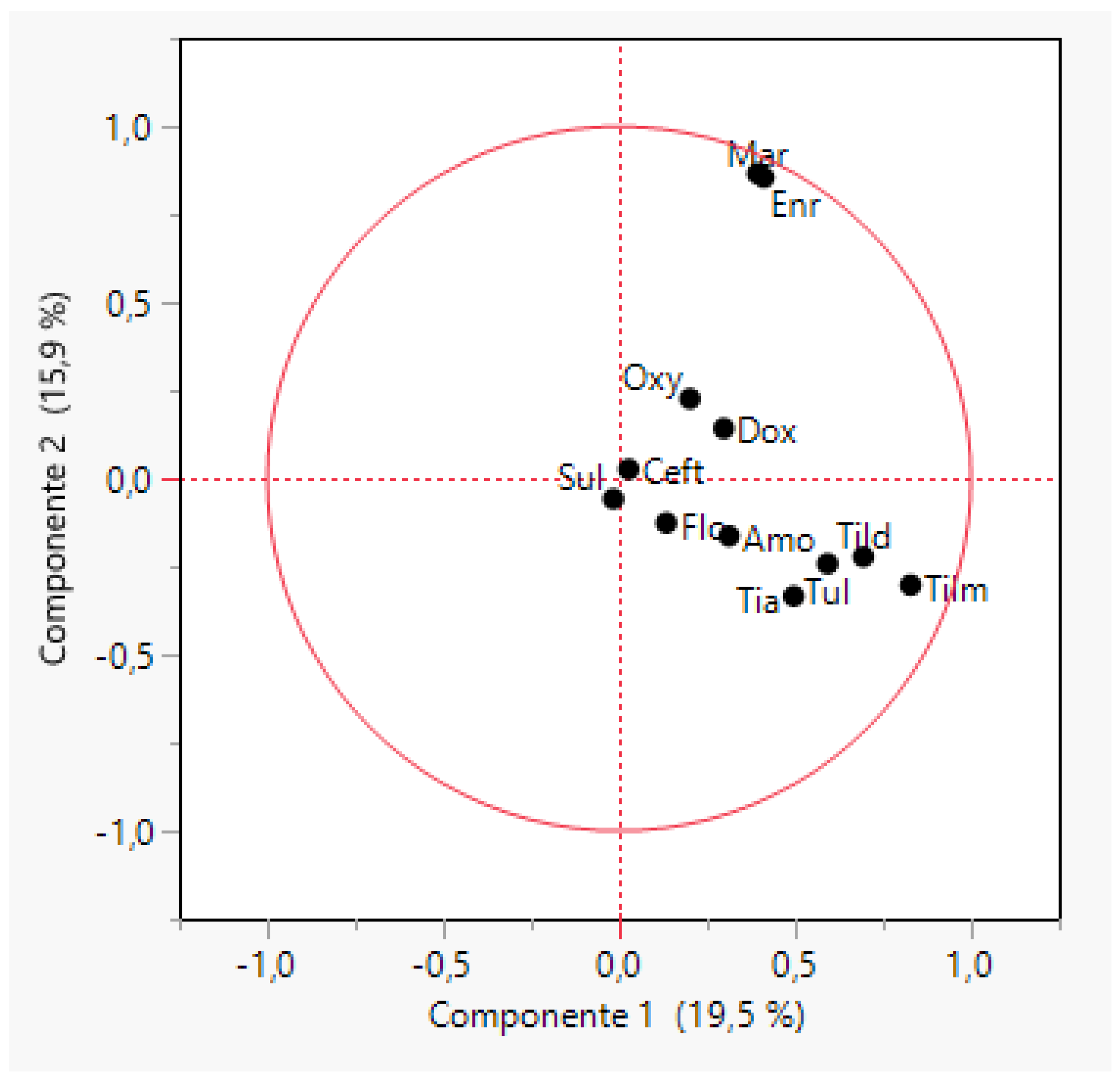
2.3.1. Actinobacillus pleuropneumoniae (APP)
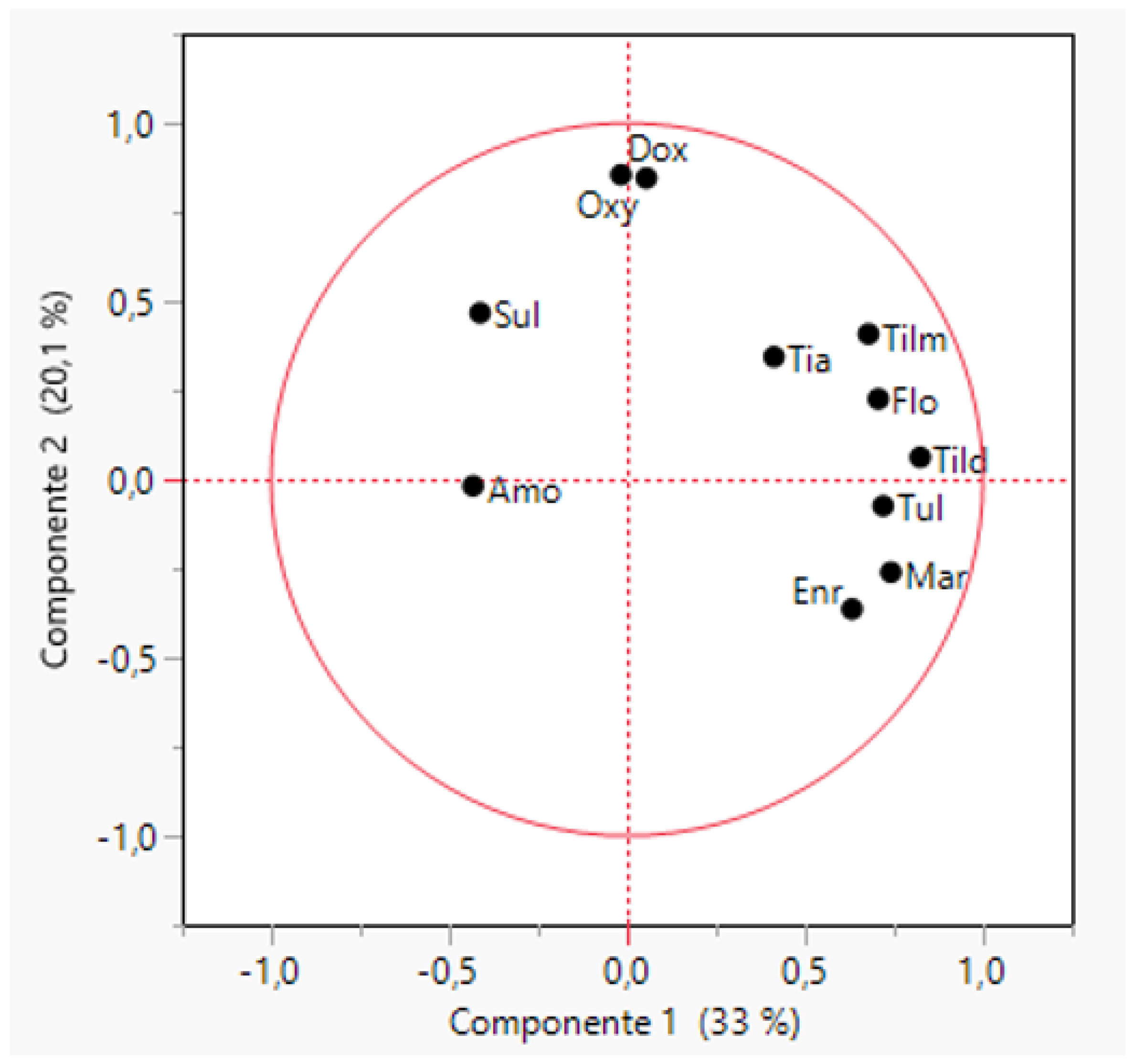
2.3.2. Pasteurella multocida
2.3.3. Bordetella bronchiseptica
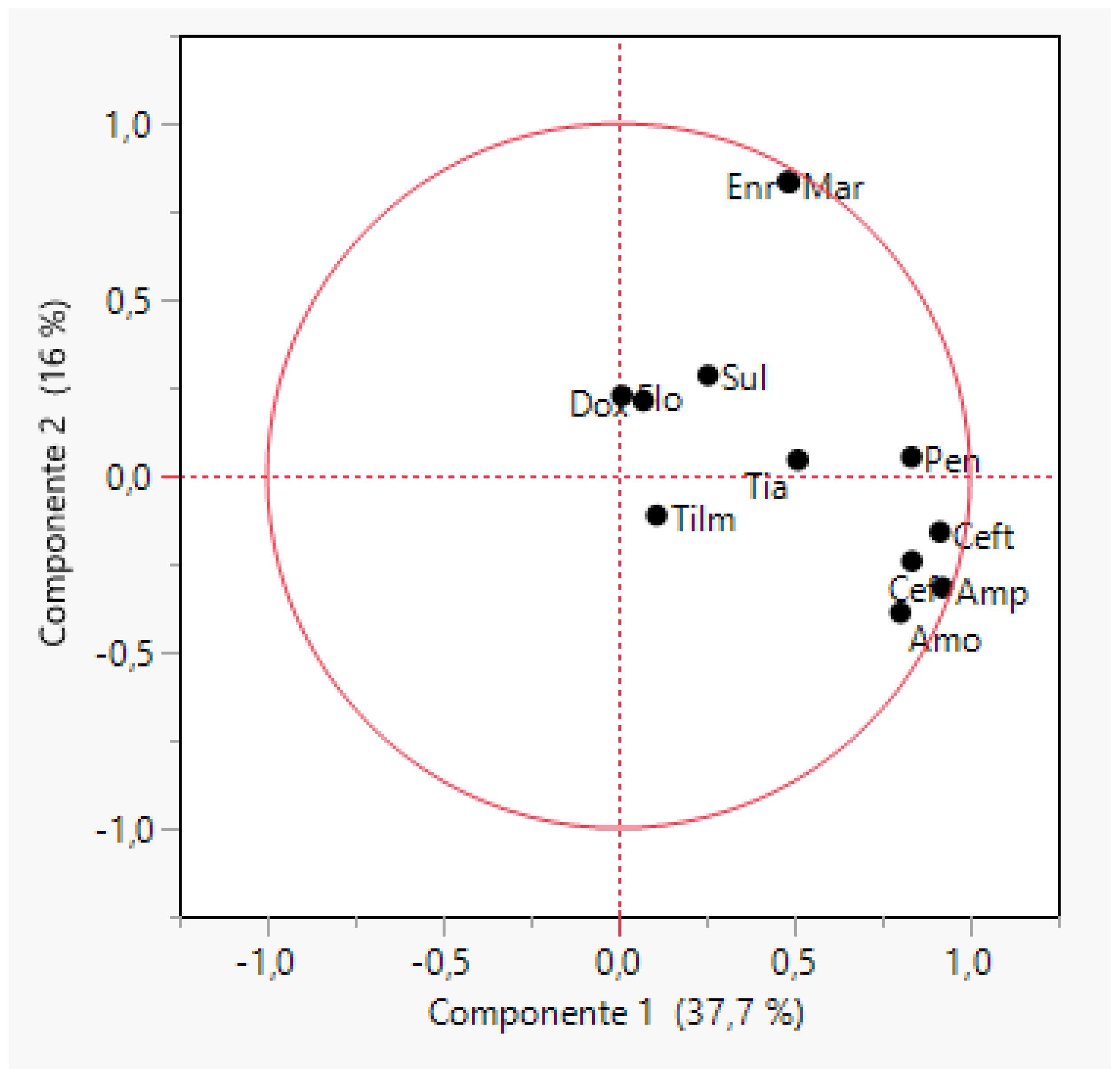
2.3.4. Streptococcus suis
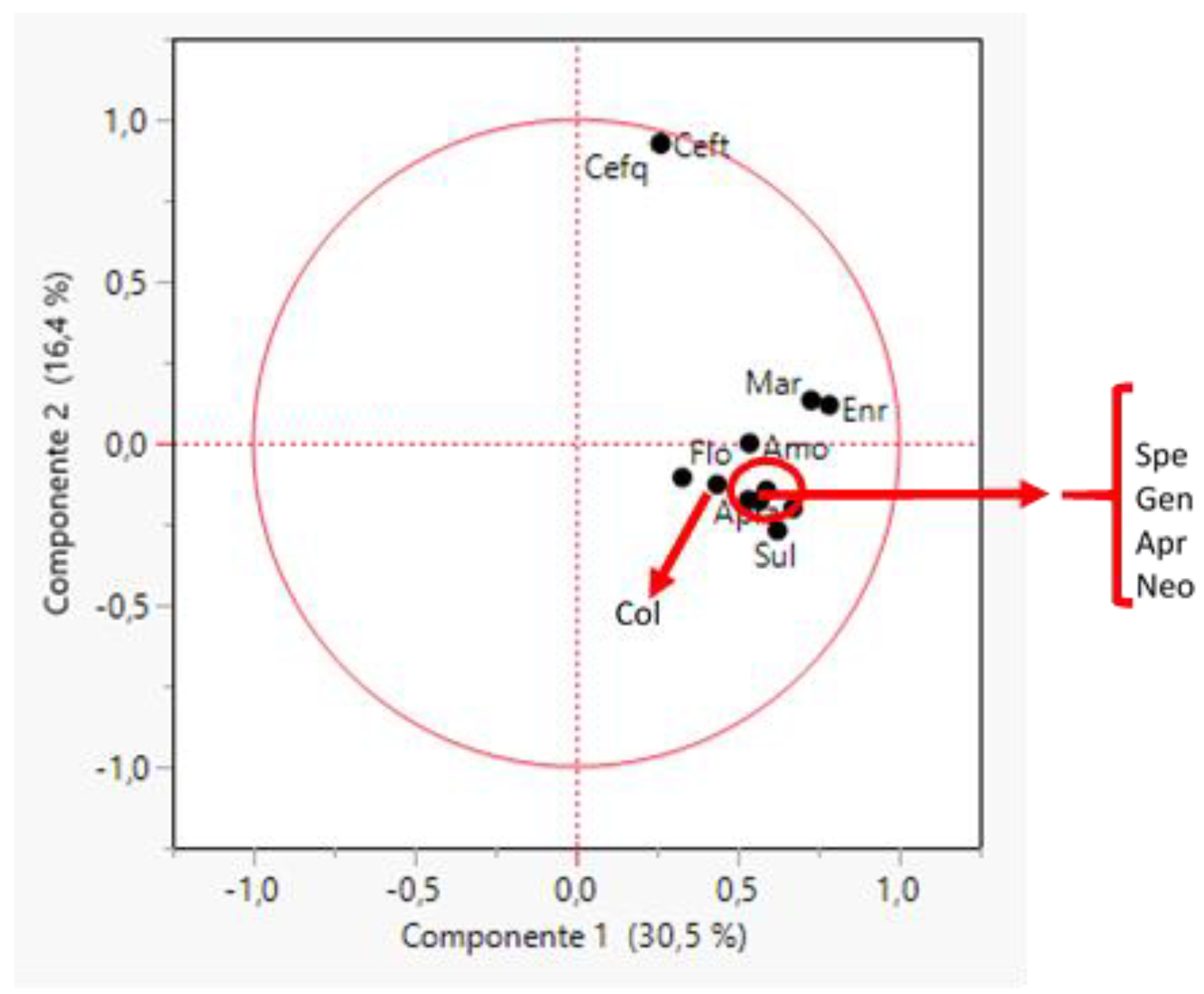
2.3.5. Escherichia coli
3. Discussion
4. Materials and Methods
4.1. Clinical Samples
4.2. Bacterial Isolation and Identification
4.3. Antimicrobial Susceptibility Testing
4.4. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gebhardt, J.T.; Tokach, M.D.; Dritz, S.S.; DeRouchey, J.M.; Woodworth, J.C.; Goodband, R.D.; Henry, S.C. Postweaning mortality in commercial swine production II: Review of infectious contributing factors. Transl. Anim. Sci. 2020, 4, 485–506. [Google Scholar] [CrossRef] [PubMed]
- Laird, T.J.; Abraham, S.; Jordan, D.; Pluske, J.R.; Hampson, D.J.; Trott, D.J.; O’Dea, M. Porcine enterotoxigenic Escherichia coli: Antimicrobial resistance and development of microbial-based alternative control strategies. Vet. Microbiol. 2021, 258, 109117. [Google Scholar] [CrossRef] [PubMed]
- Obradovic, M.R.; Segura, M.; Segalés, J.; Gottschalk, M. Review of the speculative role of co-infections in Streptococcus suis-associated diseases in pigs. Vet. Res. 2021, 52, 49. [Google Scholar] [CrossRef]
- Saade, G.; Deblanc, C.; Bougon, J.; Marois-Créhan, C.; Fablet, C.; Auray, G.; Belloc, C.; Leblanc-Maridor, M.; Gagnon, C.A.; Zhu, J.; et al. Coinfections and their molecular consequences in the porcine respiratory tract. Vet. Res. 2020, 51, 80. [Google Scholar] [CrossRef] [PubMed]
- Gebhardt, J.T.; Tokach, M.D.; Dritz, S.S.; DeRouchey, J.M.; Woodworth, J.C.; Goodband, R.D.; Henry, S.C. Postweaning mortality in commercial swine production. I: Review of non-infectious contributing factors. Transl. Anim. Sci. 2020, 4, 462–484. [Google Scholar] [CrossRef]
- EFSA Panel on Animal Health and Welfare (AHAW); Nielsen, S.S.; Bicout, D.J.; Calistri, P.; Canali, E.; Drewe, J.A.; Garin-Bastuji, B.; Rojas, J.L.G.; Schmidt, C.G.; Herskin, M.; et al. Ad hoc method for the assessment of animal diseases caused by bacteria resistant to antimicrobials. EFSA J. 2021, 19, e06645. [Google Scholar] [CrossRef]
- EFSA Panel on Animal Health and Welfare (AHAW); Nielsen, S.S.; Bicout, D.J.; Calistri, P.; Canali, E.; Drewe, J.A.; Garin-Bastuji, B.; Rojas, J.L.G.; Schmidt, C.G.; Herskin, M.; et al. Assessment of animal diseases caused by bacteria resistant to antimicrobials: Swine. EFSA J. 2021, 19, e06999. [Google Scholar] [CrossRef]
- Gottschalk, M.; Xu, J.; Calzas, C.; Segura, M. Streptococcus suis: A new emerging or an old neglected zoonotic pathogen? Future Microbiol. 2010, 5, 371–391. [Google Scholar] [CrossRef]
- Eisenberg, T.; Hudemann, C.; Hossain, H.M.; Hewer, A.; Tello, K.; Bandorski, D.; Rohde, M.; Valentin-Weigand, P.; Baums, C.G. Characterization of Five Zoonotic Streptococcus suis Strains from Germany, Including One Isolate from a Recent Fatal Case of Streptococcal Toxic Shock-Like Syndrome in a Hunter. J. Clin. Microbiol. 2015, 53, 3912–3915. [Google Scholar] [CrossRef] [Green Version]
- Fairbrother, J.M.; Nadeau, E.; Gyles, C.L. Escherichia coli in postweaning diarrhea in pigs: An update on bacterial types, pathogenesis, and prevention strategies. Anim. Health Res. Rev. 2005, 6, 17–39. [Google Scholar] [CrossRef] [Green Version]
- Rhouma, M.; Fairbrother, J.M.; Beaudry, F.; Letellier, A. Post weaning diarrhea in pigs: Risk factors and non-colistin-based control strategies. Acta Vet. Scand. 2017, 59, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luppi, A. Swine enteric colibacillosis: Diagnosis, therapy and antimicrobial resistance. Porc. Health Manag. 2017, 3, 16. [Google Scholar] [CrossRef] [PubMed]
- Fraile, L. Antimicrobial Therapy in Swine. A Practical Approach, 1st ed.; Editorial Servet: Zaragoza, Spain, 2013; pp. 1–35. [Google Scholar]
- Holmer, I.; Salomonsen, C.M.; Jorsal, S.E.; Astrup, L.B.; Jensen, V.F.; Høg, B.B.; Pedersen, K. Antibiotic resistance in porcine pathogenic bacteria and relation to antibiotic usage. BMC Vet. Res. 2019, 15, 449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guardabassi, L.; Apley, M.; Olsen, J.E.; Toutain, P.-L.; Weese, S. Optimization of Antimicrobial Treatment to Minimize Resistance Selection. Microbiol. Spectr. 2018, 6, 16. [Google Scholar] [CrossRef]
- Henderson, A.; Bursle, E.; Stewart, A.; Harris, P.N.; Paterson, D.; Chatfield, M.D.; Paul, M.; Dickstein, Y.; Rodriguez-Baño, J.; Turnidge, J.D.; et al. A systematic review of antimicrobial susceptibility testing as a tool in clinical trials assessing antimicrobials against infections due to gram-negative pathogens. Clin. Microbiol. Infect. 2021, 27, 1746–1753. [Google Scholar] [CrossRef]
- Vilaró, A.; Novell, E.; Enrique-Tarancón, V.; Balielles, J.; Vilalta, C.; Martinez, S.; Sauce, L.J.F. Antimicrobial Susceptibility Pattern of Porcine Respiratory Bacteria in Spain. Antibiotics 2020, 9, 402. [Google Scholar] [CrossRef]
- Vilaró, A.; Novell, E.; Enrique-Tarancón, V.; Balielles, J.; Allué, E.; Fraile, L. Antimicrobial Stewardship for Respiratory Pathogens in Swine. Antibiotics 2020, 9, 727. [Google Scholar] [CrossRef]
- Richter, A.; Feßler, A.T.; Böttner, A.; Köper, L.M.; Wallmann, J.; Schwarz, S. Reasons for antimicrobial treatment failures and predictive value of in-vitro susceptibility testing in veterinary practice: An overview. Vet. Microbiol. 2020, 245, 108694. [Google Scholar] [CrossRef]
- Mader, R.; Damborg, P.; Amat, J.-P.; Bengtsson, B.; Bourély, C.; Broens, E.M.; Busani, L.; Crespo-Robledo, P.; Filippitzi, M.-E.; Fitzgerald, W.; et al. Building the European Antimicrobial Resistance Surveillance network in veterinary medicine (EARS-Vet). Eurosurveillance 2021, 26, 2001359. [Google Scholar] [CrossRef]
- Depka, D.; Mikucka, A.; Bogiel, T.; Gospodarek-Komkowska, E. Comparison of the recommended colistin susceptibility testing methods with colistin gradient strips and semi-automated method for antimicrobial-resistant non-fermenting rods. J. Microbiol. Methods 2020, 172, 105905. [Google Scholar] [CrossRef]
- Magnusson, U.; Sternberg, S.; Eklund, G.; Rozstalnyy, A. Prudent and Efficient Use of Antimicrobials in Pigs and Poultry. FAO Animal Production and Health Manual. 2019. Available online: https://www.fao.org/3/ca6729en/CA6729EN.pdf (accessed on 2 March 2022).
- Holmes, A.H.; Moore, L.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.; Piddock, L. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef]
- Coyne, L.; Latham, S.; Dawson, S.; Donald, I.; Pearson, R.; Smith, R.; Williams, N.; Pinchbeck, G. Antimicrobial use practices, attitudes and responsibilities in UK farm animal veterinary surgeons. Prev. Vet. Med. 2018, 161, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Wallmann, J. Antimicrobial resistance: Challenges ahead. Vet. Rec. 2014, 175, 323–324. [Google Scholar] [CrossRef] [PubMed]
- CLSI (Clinical and Laboratory Standards Institute). Performance Standards for Antimicrobial Disk and Dilution Susceptibility Tests for Bacteria Isolated from Animals, 4th ed.; CLSI Supplement VET08: Wayne, PA, USA, 2018. [Google Scholar]
- CLSI (Clinical and Laboratory Standards Institute). Performance Standards for Antimicrobial Susceptibility Testing, 28th ed.; CLSI Supplement M100: Wayne, PA, USA, 2018. [Google Scholar]
- Aarestrup, F.M. Characterization of Glycopeptide-Resistant Enterococcus faecium (GRE) from Broilers and Pigs in Denmark: Genetic Evidence that Persistence of GRE in Pig Herds Is Associated with Coselection by Resistance to Macrolides. J. Clin. Microbiol. 2000, 38, 2774–2777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, H.E.; Tokach, M.D.; Dritz, S.S.; Woodworth, J.C.; DeRouchey, J.M.; Nagaraja, T.G.; Goodband, R.D.; Pluske, J.; Chitakasempornkul, K.; Bello, N.M.; et al. Effects of chlortetracycline alone or in combination with direct fed microbials on nursery pig growth performance and antimicrobial resistance of fecal Escherichia coli1. J. Anim. Sci. 2018, 96, 5166–5178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Migura-Garcia, L.; González-López, J.J.; Martinez-Urtaza, J.; Sánchez, J.R.A.; Moreno-Mingorance, A.; De Rozas, A.P.; Höfle, U.; Ramiro, Y.; Gonzalez-Escalona, N. mcr-Colistin Resistance Genes Mobilized by IncX4, IncHI2, and IncI2 Plasmids in Escherichia coli of Pigs and White Stork in Spain. Front. Microbiol. 2020, 10, 3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drlica, K.; Zhao, X. DNA gyrase, topoisomerase IV, and the 4-quinolones. Microbiol. Mol. Biol. Rev. 1997, 61, 377–392. [Google Scholar] [CrossRef]
- Pham, T.D.M.; Ziora, Z.M.; Blaskovich, M.A.T. Quinolone antibiotics. MedChemComm 2019, 10, 1719–1739. [Google Scholar] [CrossRef]
- Hu, P.; Yang, M.; Zhang, A.; Wu, J.; Chen, B.; Hua, Y.; Yu, J.; Chen, H.; Xiao, J.; Jin, M. Comparative Genomics Study of Multi-Drug-Resistance Mechanisms in the Antibiotic-Resistant Streptococcus suis R61 Strain. PLoS ONE 2011, 6, e24988. [Google Scholar] [CrossRef] [Green Version]
- Jacoby, G.A. Mechanisms of Resistance to Quinolones. Clin. Infect. Dis. 2005, 41, S120–S126. [Google Scholar] [CrossRef] [Green Version]
- Nedbalcova, K.; Nechvatalova, K.; Pokludova, L.; Bures, J.; Kucerova, Z.; Koutecka, L.; Hera, A. Resistance to selected beta-lactam antibiotics. Vet. Microbiol. 2014, 171, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Moennighoff, C.; Thomas, N.; Nienhaus, F.; Hartmann, M.; Menrath, A.; Merkel, J.; Detlefsen, H.; Kreienbrock, L.; Hennig-Pauka, I. Phenotypic antimicrobial resistance in Escherichia coli strains isolated from swine husbandries in North Western Germany—temporal patterns in samples from laboratory practice from 2006 to 2017. BMC Vet. Res. 2020, 16, 37. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-Z.; Mehrotra, M.; Ghimire, S.; Adewoye, L. β-Lactam resistance and β-lactamases in bacteria of animal origin. Vet. Microbiol. 2007, 121, 197–214. [Google Scholar] [CrossRef] [PubMed]
- Reflection Paper on the Use of Aminopenicillins and their Beta-Lactamase Inhibitor Combinations in Animals in the European Union: Development of Resistance and Impact on Human and Animal Health. 2021. Available online: https://www.ema.europa.eu/en/use-aminopenicillins-their-beta-lactamase-inhibitor-combinations-animals-european-union-development (accessed on 2 January 2022).
- Bush, K.; Jacoby, G.A. Updated Functional Classification of β-Lactamases. Antimicrob. Agents Chemother. 2010, 54, 969–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grebe, T.; Hakenbeck, R. Penicillin-binding proteins 2b and 2x of Streptococcus pneumoniae are primary resistance determinants for different classes of beta-lactam antibiotics. Antimicrob. Agents Chemother. 1996, 40, 829–834. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Metcalf, B.J.; Chochua, S.; Li, Z.; Gertz, R.E.; Walker, H.; Hawkins, P.A.; Tran, T.; Whitney, C.G.; McGee, L.; et al. Penicillin-Binding Protein Transpeptidase Signatures for Tracking and Predicting β-Lactam Resistance Levels in Streptococcus pneumoniae. mBio 2016, 7, e00756-16. [Google Scholar] [CrossRef] [Green Version]
- Hadjirin, N.F.; Miller, E.L.; Murray, G.G.R.; Yen, P.L.K.; Phuc, H.D.; Wileman, T.M.; Hernandez-Garcia, J.; Williamson, S.M.; Parkhill, J.; Maskell, D.J.; et al. Large-scale genomic analysis of antimicrobial resistance in the zoonotic pathogen Streptococcus suis. BMC Biol. 2021, 19, 191. [Google Scholar] [CrossRef]
- Kocaoglu, O.; Tsui, H.-C.T.; Winkler, M.E.; Carlson, E.E. Profiling of β-Lactam Selectivity for Penicillin-Binding Proteins in Streptococcus pneumoniae D39. Antimicrob. Agents Chemother. 2015, 59, 3548–3555. [Google Scholar] [CrossRef] [Green Version]
- Gurung, M.; Tamang, M.D.; Moon, D.C.; Kim, S.-R.; Jeong, J.-H.; Jang, G.-C.; Jung, S.-C.; Park, Y.-H.; Lim, S.-K. Molecular Basis of Resistance to Selected Antimicrobial Agents in the Emerging Zoonotic Pathogen Streptococcus suis. J. Clin. Microbiol. 2015, 53, 2332–2336. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Ku, X.; Yu, X.; Sun, Q.; Wu, H.; Chen, F.; Zhang, X.; Guo, L.; Tang, X.; He, Q. Prevalence and antimicrobial susceptibilities of bacterial pathogens in Chinese pig farms from 2013 to 2017. Sci. Rep. 2019, 9, 9908. [Google Scholar] [CrossRef]
- Petrocchi-Rilo, M.; Martínez-Martínez, S.; Aguarón-Turrientes, A.; Roca-Martínez, E.; García-Iglesias, M.-J.; Pérez-Fernández, E.; González-Fernández, A.; Herencia-Lagunar, E.; Gutiérrez-Martín, C.-B. Anatomical Site, Typing, Virulence Gene Profiling, Antimicrobial Susceptibility and Resistance Genes of Streptococcus suis Isolates Recovered from Pigs in Spain. Antibiotics 2021, 10, 707. [Google Scholar] [CrossRef] [PubMed]
- Grossman, T.H. Tetracycline Antibiotics and Resistance. Cold Spring Harb. Perspect. Med. 2016, 6, a025387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chukwudi, C.U. rRNA Binding Sites and the Molecular Mechanism of Action of the Tetracyclines. Antimicrob. Agents Chemother. 2016, 60, 4433–4441. [Google Scholar] [CrossRef] [Green Version]
- Van Duijkeren, E.; Schwarz, C.; Bouchard, D.; Catry, B.; Pomba, C.; Baptiste, K.E.; Moreno, M.A.; Rantala, M.; Ruzauskas, M.; Sanders, P.; et al. The use of aminoglycosides in animals within the EU: Development of resistance in animals and possible impact on human and animal health: A review. J. Antimicrob. Chemother. 2019, 74, 2480–2496. [Google Scholar] [CrossRef] [PubMed]
- Leclercq, R. Mechanisms of Resistance to Macrolides and Lincosamides: Nature of the Resistance Elements and Their Clinical Implications. Clin. Infect. Dis. 2002, 34, 482–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A: Actinobacillus pleuropneumoniae | |||
|---|---|---|---|
| Antimicrobial | Range (μg/mL) | MIC50 (μg/mL) | MIC90 (μg/mL) |
| Amoxicillin | 0.06–16 | 0.5 | 8 |
| Ceftiofur | 0.06–0.25 | 0.06 | 0.06 |
| Doxycycline | 0.12–16 | 2 | 4 |
| Enrofloxacin | 0.03–4 | 0.06 | 0.5 |
| Florfenicol | 0.06–8 | 0.25 | 0.5 |
| Marbofloxacin | 0.03–4 | 0.03 | 0.5 |
| Oxytetracycline | 0.12–8 | 8 | 8 |
| Sulfamethoxazole/trimethropim & | 0.06–32 | 0.12 | 2 |
| Tiamulin | 2–32 | 16 | 16 |
| Tildipirosin | 1–64 | 8 | 8 |
| Tilmicosin | 4–64 | 16 | 16 |
| Tulathromycin | 8–64 | 32 | 64 |
| B: Pasteurella multocida | |||
| Amoxicillin | 0.12–8 | 0.25 | 0.5 |
| Ceftiofur | 0.06–1 | 0.06 | 0.12 |
| Doxycycline | 0.12–16 | 0.5 | 2 |
| Enrofloxacin | 0.03–1 | 0.03 | 0.06 |
| Florfenicol | 0.12–8 | 0.5 | 0.5 |
| Marbofloxacin | 0.03–1 | 0.03 | 0.12 |
| Oxytetracycline | 0.12–8 | 1 | 8 |
| Sulfamethoxazole/trimethropim & | 0.03–8 | 0.12 | 4 |
| Tiamulin | 2–64 | 16 | 32 |
| Tildipirosin | 0.5–64 | 2 | 4 |
| Tilmicosin | 1–64 | 8 | 16 |
| Tulathromycin | 0.5–64 | 2 | 4 |
| C: Bordetella bronchiseptica | |||
| Amoxicillin | 8–16 | 8 | 16 |
| Ceftiofur | 4 | 4 | 4 |
| Doxycycline | 0.12–4 | 1 | 2 |
| Enrofloxacin | 0.12–4 | 0.5 | 1 |
| Florfenicol | 1–8 | 4 | 4 |
| Marbofloxacin | 0.12–2 | 0.5 | 1 |
| Oxytetracycline | 0.25–8 | 2 | 4 |
| Sulfamethoxazole/trimethropim & | 0.06–8 | 4 | 4 |
| Tiamulin | 32–64 | 64 | 64 |
| Tildipirosin | 0.5–16 | 8 | 8 |
| Tilmicosin | 8–64 | 32 | 64 |
| Tulathromycin | 2–16 | 8 | 16 |
| Antimicrobial | Range (μg/mL) | MIC50 (μg/mL) | MIC90 (μg/mL) |
|---|---|---|---|
| Amoxicillin | 0.06–8 | 0.06 | 0.5 |
| Ampicillin | 0.06–4 | 0.06 | 0.5 |
| Ceftiofur | 0.06–4 | 0.25 | 1 |
| Cefquinome | 0.06–4 | 0.06 | 0.25 |
| Doxycycline | 0.12–16 | 8 | 16 |
| Enrofloxacin | 0.03–4 | 0.5 | 1 |
| Florfenicol | 1–8 | 2 | 4 |
| Marbofloxacin | 0.03–4 | 1 | 2 |
| Penicillin G | 0.06–8 | 0.25 | 2 |
| Sulfamethoxazole/trimethropim & | 0.06–4 | 1 | 4 |
| Tiamulin | 0.5–64 | 2 | 32 |
| Tilmicosin | 4–64 | 64 | 64 |
| Antimicrobial | Range (μg/mL) | MIC50 (μg/mL) | MIC90 (μg/mL) |
|---|---|---|---|
| Amoxicillin | 0.12–16 | 8 | 16 |
| Apramycin | 0.5–64 | 4 | 32 |
| Ceftiofur | 0.06–8 | 0.5 | 8 |
| Cefquinome | 0.06–8 | 0.12 | 8 |
| Colistin | 0.25–32 | 1 | 4 |
| Enrofloxacin | 0.03–4 | 1 | 4 |
| Florfenicol | 1–8 | 8 | 8 |
| Gentamycin | 0.12–64 | 1 | 16 |
| Marbofloxacin | 0.03–4 | 0.5 | 4 |
| Neomycin | 0.5–64 | 4 | 64 |
| Spectinomycin | 4–128 | 128 | 128 |
| Sulfamethoxazole/trimethropim & | 0.03–8 | 4 | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vilaró, A.; Novell, E.; Enrique-Tarancon, V.; Balielles, J.; Migura-García, L.; Fraile, L. Antimicrobial Susceptibility Testing of Porcine Bacterial Pathogens: Investigating the Prospect of Testing a Representative Drug for Each Antimicrobial Family. Antibiotics 2022, 11, 638. https://doi.org/10.3390/antibiotics11050638
Vilaró A, Novell E, Enrique-Tarancon V, Balielles J, Migura-García L, Fraile L. Antimicrobial Susceptibility Testing of Porcine Bacterial Pathogens: Investigating the Prospect of Testing a Representative Drug for Each Antimicrobial Family. Antibiotics. 2022; 11(5):638. https://doi.org/10.3390/antibiotics11050638
Chicago/Turabian StyleVilaró, Anna, Elena Novell, Vicens Enrique-Tarancon, Jordi Balielles, Lourdes Migura-García, and Lorenzo Fraile. 2022. "Antimicrobial Susceptibility Testing of Porcine Bacterial Pathogens: Investigating the Prospect of Testing a Representative Drug for Each Antimicrobial Family" Antibiotics 11, no. 5: 638. https://doi.org/10.3390/antibiotics11050638
APA StyleVilaró, A., Novell, E., Enrique-Tarancon, V., Balielles, J., Migura-García, L., & Fraile, L. (2022). Antimicrobial Susceptibility Testing of Porcine Bacterial Pathogens: Investigating the Prospect of Testing a Representative Drug for Each Antimicrobial Family. Antibiotics, 11(5), 638. https://doi.org/10.3390/antibiotics11050638