
Development of and User Feedback on a Board and Online Game to Educate on Antimicrobial Resistance and Stewardship

 ,
,  ,
,
Abstract
:1. Introduction
- Competition and goals, with players competing against other players both for the physical and online games.
- Clear rules that define how the game is played.
- Choice through the use of multiple-choice questions.
- Challenges—players are provided with problems to solve in this game. We use the case studies as a way to provide additional challenges.
- Coaching, debriefing, and feedback: to reinforce learning.
- Performance assessment, so players know how they did.
- Mechanics: the elements of the game that control gameplay.
2. Materials and Methods
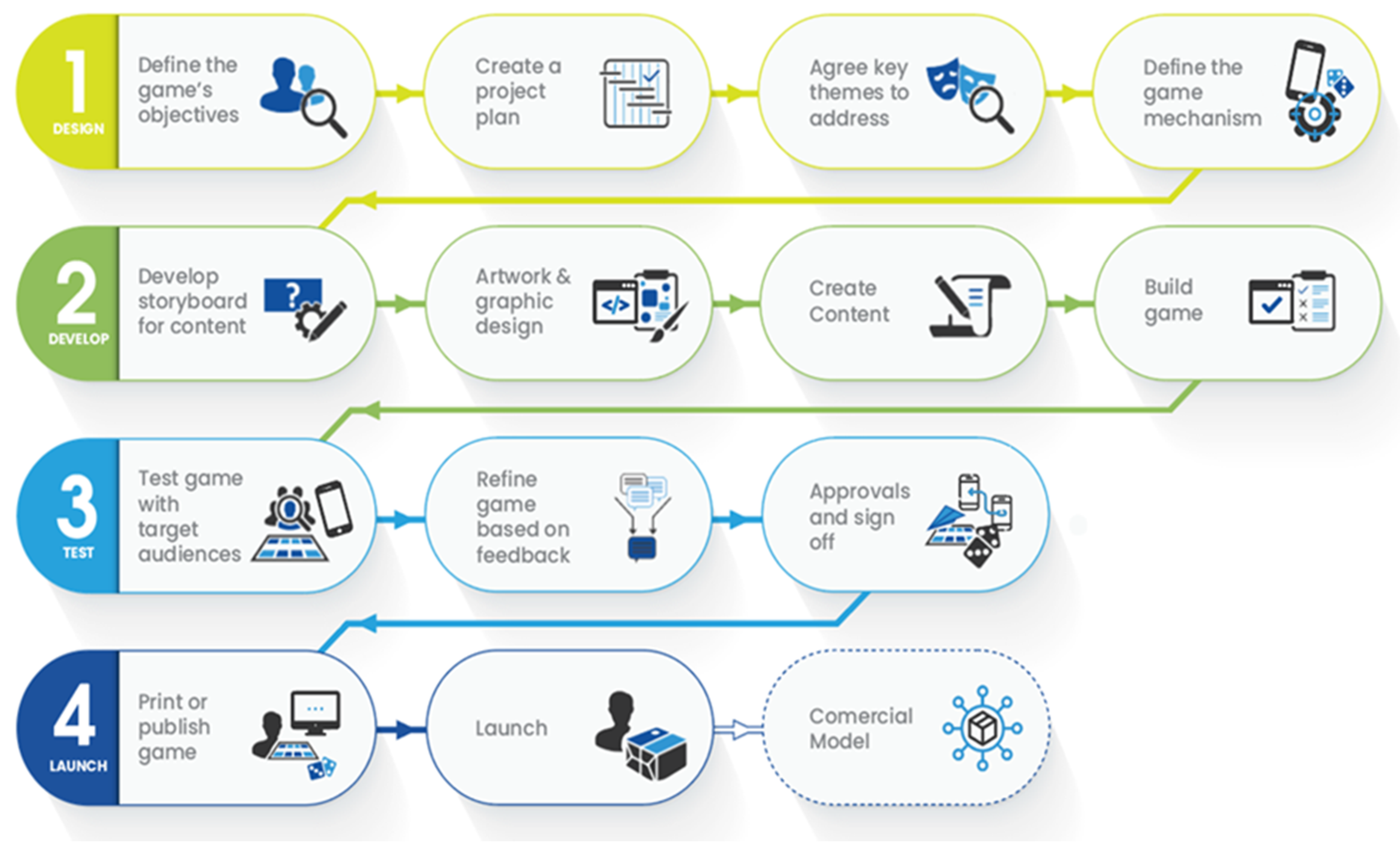
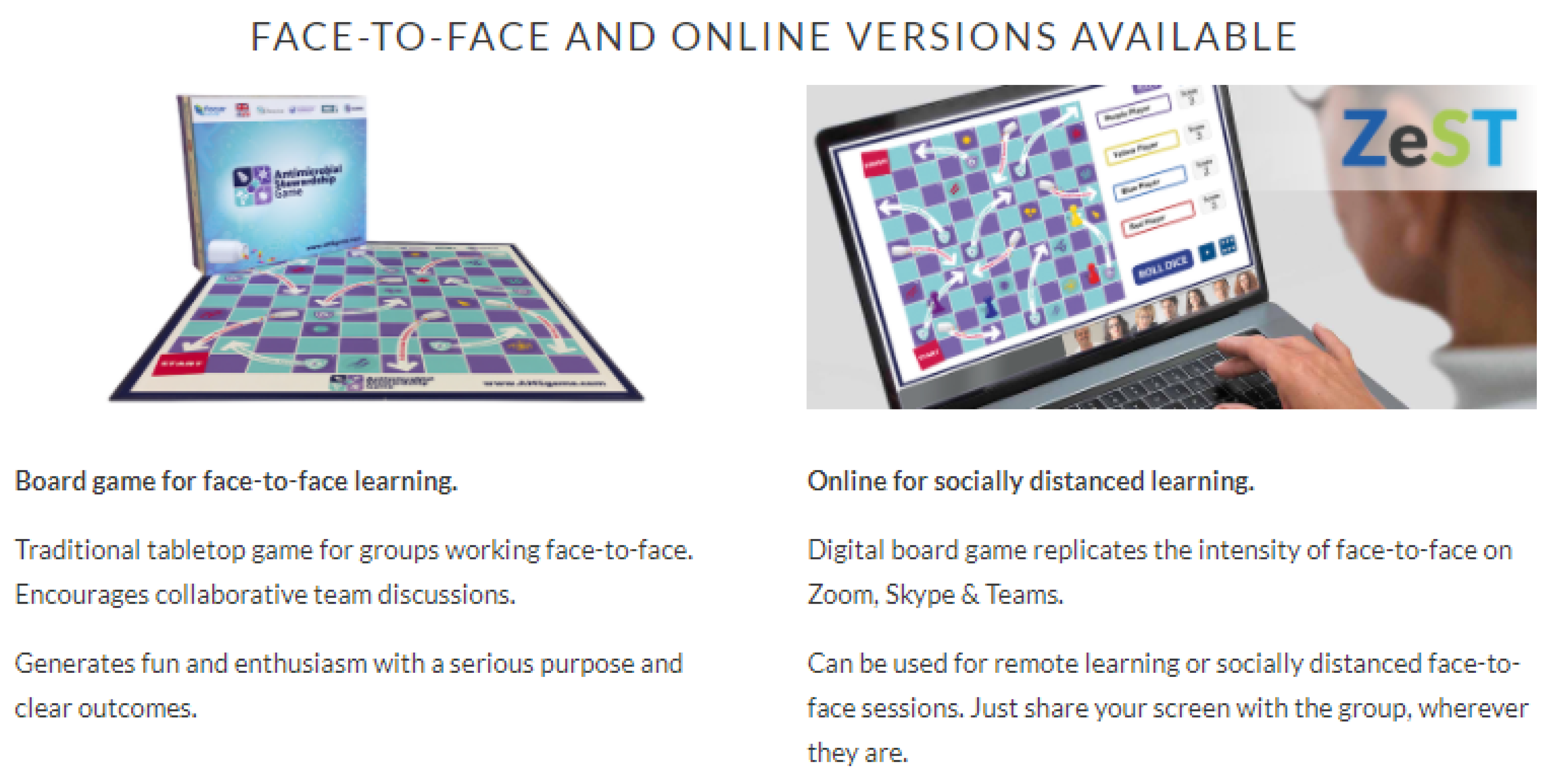
2.1. AMS Game Development
2.2. Target Audience for the AMS Game
2.3. Stakeholder Engagement
2.4. Recruitment of Participants and Playing the Game
2.5. Feedback from Players of the Game
2.6. Data Management
2.7. Data Analysis
3. Results
3.1. Developing the Game: Feedback on Relevance
3.1.1. Demographics of Respondents
3.1.2. Feedback on Relevance of Questions of the Game
“What is antibiotic resistance? The response needs to be modified to include inappropriate antibiotic use as a driver of antibiotic resistance not optimal use of the same. The response should also include that antibiotics are not effective against parasites.”“Perhaps consider adding some more questions on the role of IPC and the MTC in AMS.”“I would suggest to add the following topics on hospital-associated infections. Diagnostics on how to identify the presence of a microbe in a patient specimen.”
3.2. Players’ Feedback on the AMS Game
3.2.1. Demographics of Respondents
3.2.2. Player Enjoyment of the AMS Game
“The game was highly entertaining and enriching. You get to learn more of the AMS or rather, fine-tune your knowledge via the game. Will really love to partake again. Kindly keep me posted. Thanks.”“The game was very interesting, straight forward and all-round included the One Health aspect which I am really interested in that I think is the way to go if mitigation of antimicrobial resistance is to be achieved.”“The game is a good way of bringing the awareness to health workers. It should be rolled out across and include students in medicine, nursing, pharmacy, and laboratory.”“What I loved most was that the answers provided by the game were simple, understandable and straightforward to the point and also there was more valuable information attached to the answer thus giving more understanding and meaning.”
“The demonstration was a bit rushed so difficult to get a real feel for the game. I can see it could be a useful tool to facilitate discussion around AMS with more junior/inexperienced staff. The game needs to be seen in this light because I feel if the focus becomes on playing the game, answering questions as quickly as possible, etc., then it’s true value will be lost.”“A good fun, learned few things for a very short time.”“Cross talking among participants making it difficult to respond…time constraints…facilitators should not talk much.”
3.2.3. Knowledge Gain after Playing the Game
“I understood that not only human health must be emphasised so as to end antimicrobial resistance but also animal and environmental health. Interacting with more informed players was more informing.”“The game was a quick mind check for the principles on AMR.”
“Actually, it’s funny to say but today I learnt that there is a difference between antibiotics and antimicrobials. At first, I thought there was no difference. And I have also learnt about antimicrobial and antibiotic resistance.”“I learned that simple practices such as handwashing play a big role in fighting AMR.”“Learning is fun when made simple in such innovative ways. I also think it can stick to the brain and allows easy replication in actual practice settings.”
“I can now educate my colleagues, the nation and the entire world about the goodness of antimicrobial stewardship.”“I think the game is great, since am just an undergraduate student but I have been able to reason out different things with people already in the profession. This has boosted my confidence.”
3.2.4. Sharing Lessons Gained from Playing the Game
“I have to share what I have learnt with others so as to facilitate continuation of learning and flow of information.”“I will share during our grants meetings and AMS meeting.”“I will promote for use in WAAW (World Antimicrobial Awareness Week).”“It was such an engaging experience and will be helpful for bonding in our hospital teams.”
“Completing one’s dosage as prescribed by a trained health personnel helps minimise antimicrobial resistance.”“The patients can use the game to learn more about AMS.”
4. Discussion
4.1. AMS Game Development
4.2. Players’ Feedback on the Game
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Antimicrobial Resistance: Fact Sheets. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 4 March 2022).
- Ghosh, S.; Bornman, C.; Zafer, M.M. Antimicrobial Resistance threats in the emerging COVID-19 pandemic: Where do we stand? J. Infect. Public Health 2021, 14, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Pokharel, S.; Raut, S.; Adhikari, B. Tackling antimicrobial resistance in low-income and middle-income countries. BMJ Glob. Health 2019, 4, e002104. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Renwick, R.; Turner, N.E.; Kirsh, B. Understanding the lives of problem gamers: The meaning, purpose, and influences of video gaming. Comput. Hum. Behav. 2019, 97, 291–303. [Google Scholar] [CrossRef]
- Looyestyn, J.; Kernot, J.; Boshoff, K.; Ryan, J.; Edney, S.; Maher, C. Does gamification increase engagement with online programs? A systematic review. PLoS ONE 2017, 12, e0173403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakao, M. Special series on “effects of board games on health education and promotion” board games as a promising tool for health promotion: A review of recent literature. BioPsychoSocial Med. 2019, 13, 5. [Google Scholar] [CrossRef] [PubMed]
- Guest, E.; Jarman, H.; Sharratt, N.; Williamson, H.; White, P.; Harcourt, D.; Slater, A. ‘Everybody’s Different: The Appearance Game’. A randomised controlled trial evaluating an appearance-related board game intervention with children aged 9–11 years. Body Image 2021, 36, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Akl, E.A.; Sackett, K.M.; Pretorius, R.; Bhoopathi, P.S.S.; Mustafa, R.; Schünemann, H.; Erdley, W.S. Educational games for health professionals. Cochrane Database Syst. Rev. 2013, 2013, Cd006411. [Google Scholar]
- Ijaz, A.; Khan, M.Y.; Ali, S.M.; Qadir, J.; Boulos, M.N.K. Serious games for healthcare professional training: A systematic review. Eur. J. Biomed. Inform. 2019, 15, 30. [Google Scholar]
- Tudor Car, L.; Soong, A.; Kyaw, B.M.; Chua, K.L.; Low-Beer, N.; Majeed, A. Health professions digital education on clinical practice guidelines: A systematic review by Digital Health Education collaboration. BMC Med. 2019, 17, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, G.; Leonard, L.; Carter, G.; Santin, O.; Brown Wilson, C. Evaluation of a ‘serious game’on nursing student knowledge and uptake of influenza vaccination. PLoS ONE 2021, 16, e0245389. [Google Scholar] [CrossRef] [PubMed]
- Aboalshamat, K.; Khayat, A.; Halwani, R.; Bitan, A.; Alansari, R. The effects of gamification on antimicrobial resistance knowledge and its relationship to dentistry in Saudi Arabia: A randomized controlled trial. BMC Public Health 2020, 20, 680. [Google Scholar] [CrossRef] [PubMed]
- Hale, A.R.; Young, V.L.; Grand, A.; McNulty, C.A.M. Can gaming increase antibiotic awareness in children? A mixed-methods approach. JMIR Serious Games 2017, 5, e6420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Focus Games. Case Studies [Online]. 2021. Available online: https://focusgames.com/case_studies.html (accessed on 20 April 2022).
- Lameras, P.; Arnab, S.; Dunwell, I.; Stewart, C.; Clarke, S.; Petridis, P. Essential features of serious games design in higher education: Linking learning attributes to game mechanics. Br. J. Educ. Technol. 2017, 48, 972–994. [Google Scholar] [CrossRef]
- Focus Games. Develop a Game [Online]. 2021. Available online: https://focusgames.com/develop_a_game.html (accessed on 17 March 2022).
- Focus Games. Antimicrobial Stewardship Game. 2021. Available online: https://www.amsgame.com/ (accessed on 17 March 2022).
- Sharifzadeh, N.; Kharrazi, H.; Nazari, E.; Tabesh, H.; Khodabandeh, M.E.; Heidari, S.; Tara, M. Health education serious games targeting health care providers, patients, and public health users: Scoping review. JMIR Serious Games 2020, 8, e13459. [Google Scholar] [CrossRef] [PubMed]
- Brox, E.; Fernandez-Luque, L.; Tøllefsen, T. Healthy gaming–video game design to promote health. Appl. Clin. Inform. 2011, 2, 128–142. [Google Scholar] [PubMed] [Green Version]
- Schwarz, A.F.; Huertas-Delgado, F.J.; Cardon, G.; DeSmet, A. Design features associated with user engagement in digital games for healthy lifestyle promotion in youth: A systematic review of qualitative and quantitative studies. Games Health J. 2020, 9, 150–163. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Singh, A.; Dar, M.A.; Kaur, R.J.; Charan, J.; Iskandar, K.; Haque, M.; Murti, K.; Ravichandiran, V.; Dhingra, S. Menace of antimicrobial resistance in LMICs: Current surveillance practices and control measures to tackle hostility. J. Infect. Public Health 2021, 15, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Fasina, F.O.; LeRoux-Pullen, L.; Smith, P.; Debusho, L.K.; Shittu, A.; Jajere, S.M.; Adebowale, O.; Odetokun, I.; Agbaje, M.; Fasina, M.M.; et al. Knowledge, attitudes, and perceptions associated with antimicrobial stewardship among veterinary students: A multi-country survey from Nigeria, South Africa, and Sudan. Front. Public Health 2020, 8, 630. [Google Scholar] [CrossRef] [PubMed]
- Chukwu, E.E.; Oladele, D.A.; Awoderu, O.B.; Afocha, E.E.; Lawal, R.G.; Abdus-Salam, I.; Ogunsola, F.T.; Audu, R.A. A national survey of public awareness of antimicrobial resistance in Nigeria. Antimicrob. Resist. Infect. Control. 2020, 9, 72. [Google Scholar] [CrossRef] [PubMed]
- WHO. Health Workers’ Education and Training on Antimicrobial Resistance: Curricula Guide; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Higuita-Gutiérrez, L.F.; Roncancio Villamil, G.E.; Jiménez Quiceno, J.N. Knowledge, attitude, and practice regarding antibiotic use and resistance among medical students in Colombia: A cross-sectional descriptive study. BMC Public Health 2020, 20, 1861. [Google Scholar] [CrossRef] [PubMed]
- Commonwealth Pharmacists Association. Tweets of the #AMSGame in Use. Available online: https://twitter.com/hashtag/AMSGame?src=hashtag_click&f=live (accessed on 11 March 2022).
- NHS. Is My Study Research? Available online: http://www.hra-decisiontools.org.uk/research/result7.html (accessed on 9 January 2022).

{kind=link}
{kind=link}
| Number of Respondents | Percentage (%) | |
|---|---|---|
| Questions broadly relevant to your country | n = 25 | |
| Yes | 25 | 100 |
| No | 0 | 0 |
| Some questions not at all relevant or inaccurate for your country | n = 25 | |
| Yes | 10 | 40 |
| No | 15 | 60 |
| Questions and case studies address key aspects of AMS | n = 24 | |
| Yes | 24 | 100 |
| No | 0 | 0 |
| Country | Number of Respondents (n = 74) | Percentage (%) |
| European Region | 39 | 52.8 |
| United Kingdom | 38 | 51.4 |
| Hungary | 1 | 1.4 |
| South-East Asia Region | 2 | 2.7 |
| India | 1 | 1.4 |
| Sri Lanka | 1 | 1.4 |
| African region | 32 | 43.2 |
| Uganda | 15 | 20.3 |
| Kenya | 7 | 9.5 |
| Ghana | 2 | 2.7 |
| Nigeria | 3 | 4.1 |
| Sierra Leone | 3 | 4.1 |
| Eswatini | 1 | 1.4 |
| Malawi | 1 | 1.4 |
| Western Pacific Region | 1 | 1.4 |
| Fiji | 1 | 1.4 |
| Number of respondents (n = 74) | Percentage (%) | |
| Role/Profession | ||
| Pharmacist | 46 | 62.2 |
| Student | 7 | 9.5 |
| Doctor | 6 | 8.1 |
| Other (Academic, Environmental Health) | 5 | 6.8 |
| Support staff | 4 | 5.4 |
| Other clinical staff | 3 | 4.05 |
| Laboratory staff | 2 | 2.7 |
| Nurse | 1 | 1.4 |
| Level of Experience in AMS | ||
| Some knowledge of AMS | 30 | 40.5 |
| Experienced in AMS | 21 | 28.4 |
| Specialist in AMS | 15 | 20.3 |
| New to AMS | 8 | 10.8 |
| Enjoyed Playing the AMS Game | Number of Respondents (n = 74) | Percentage (%) |
|---|---|---|
| Strongly disagree | 2 | 2.7 |
| Disagree | 0 | 0 |
| Neither disagree nor agree | 4 | 5.4 |
| Agree | 26 | 35.1 |
| Strongly agree | 42 | 56.8 |
| Number of Respondents | Percentage (%) | |
|---|---|---|
| Know more about AMS after playing the game | n = 74 | |
| Strongly disagree | 6 | 8.1 |
| Disagree | 3 | 4.1 |
| Neither disagree nor agree | 9 | 12.2 |
| Agree | 35 | 47.3 |
| Strongly agree | 21 | 28.4 |
| More confident about AMS | n = 73 | |
| Strongly disagree | 4 | 5.5 |
| Disagree | 3 | 4.1 |
| Neither disagree nor agree | 8 | 11 |
| Agree | 41 | 56.2 |
| Strongly agree | 17 | 23.3 |
| Knowledge Gain | Region | |||
|---|---|---|---|---|
| African | Europe | South-East Asia | Western Pacific | |
| Strongly disagree | 3 (9.3%) | 3 (7.7%) | 0 (0%) | 0 (0%) |
| Disagree | 1 (3.1%) | 2 (5.1%) | 0 (0%) | 0 (0%) |
| Neither disagree nor agree | 2 (6.3%) | 7 (17.9%) | 0 (0%) | 0 (0%) |
| Agree | 14 (43.8%) | 19 (48.7%) | 1 (50%) | 1 (100%) |
| Strongly agree | 12 (37.5%) | 8 (20.5%) | 1 (50%) | 0 (0%) |
| Total | 32 (100%) | 39 (100%) | 2 (100%) | 1 (100%) |
| Number of Respondents | Percentage (%) | |
|---|---|---|
| Sharing lessons with colleagues | n = 74 | |
| Strongly disagree | 2 | 2.7 |
| Disagree | 0 | 0 |
| Neither disagree nor agree | 3 | 4.1 |
| Agree | 38 | 51.4 |
| Strongly agree | 31 | 41.9 |
| Sharing lessons with patients | n = 73 | |
| Strongly disagree | 3 | 4.1 |
| Disagree | 0 | 0 |
| Neither disagree nor agree | 17 | 23.3 |
| Agree | 34 | 46.6 |
| Strongly agree | 19 | 26 |
| Recommending game to colleagues | ||
| No | 2 | 2.7 |
| Yes | 71 | 97.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashiru-Oredope, D.; Nabiryo, M.; Yeoman, A.; Bell, M.; Cavanagh, S.; D’Arcy, N.; Townsend, W.; Demenciukas, D.; Yadav, S.; Garraghan, F.; et al. Development of and User Feedback on a Board and Online Game to Educate on Antimicrobial Resistance and Stewardship. Antibiotics 2022, 11, 611. https://doi.org/10.3390/antibiotics11050611
Ashiru-Oredope D, Nabiryo M, Yeoman A, Bell M, Cavanagh S, D’Arcy N, Townsend W, Demenciukas D, Yadav S, Garraghan F, et al. Development of and User Feedback on a Board and Online Game to Educate on Antimicrobial Resistance and Stewardship. Antibiotics. 2022; 11(5):611. https://doi.org/10.3390/antibiotics11050611
Chicago/Turabian StyleAshiru-Oredope, Diane, Maxencia Nabiryo, Andy Yeoman, Melvin Bell, Sarah Cavanagh, Nikki D’Arcy, William Townsend, Dalius Demenciukas, Sara Yadav, Frances Garraghan, and et al. 2022. "Development of and User Feedback on a Board and Online Game to Educate on Antimicrobial Resistance and Stewardship" Antibiotics 11, no. 5: 611. https://doi.org/10.3390/antibiotics11050611
APA StyleAshiru-Oredope, D., Nabiryo, M., Yeoman, A., Bell, M., Cavanagh, S., D’Arcy, N., Townsend, W., Demenciukas, D., Yadav, S., Garraghan, F., Carter, V., Rutter, V., & Skone-James, R. (2022). Development of and User Feedback on a Board and Online Game to Educate on Antimicrobial Resistance and Stewardship. Antibiotics, 11(5), 611. https://doi.org/10.3390/antibiotics11050611