
Extended Infusion of Meropenem in Neonatal Sepsis: A Historical Cohort Study

 ,
,
Abstract
:1. Introduction
2. Results
2.1. EI of Meropenem in Effectiveness Outcomes
2.2. EI of Meropenem in Safety Outcomes
2.3. Subgroup Analysis
2.3.1. EI of Meropenem in Very Low Birth Weight Infants
2.3.2. Two-Hour EI of Meropenem in Neonatal Sepsis
3. Discussion
4. Materials and Methods
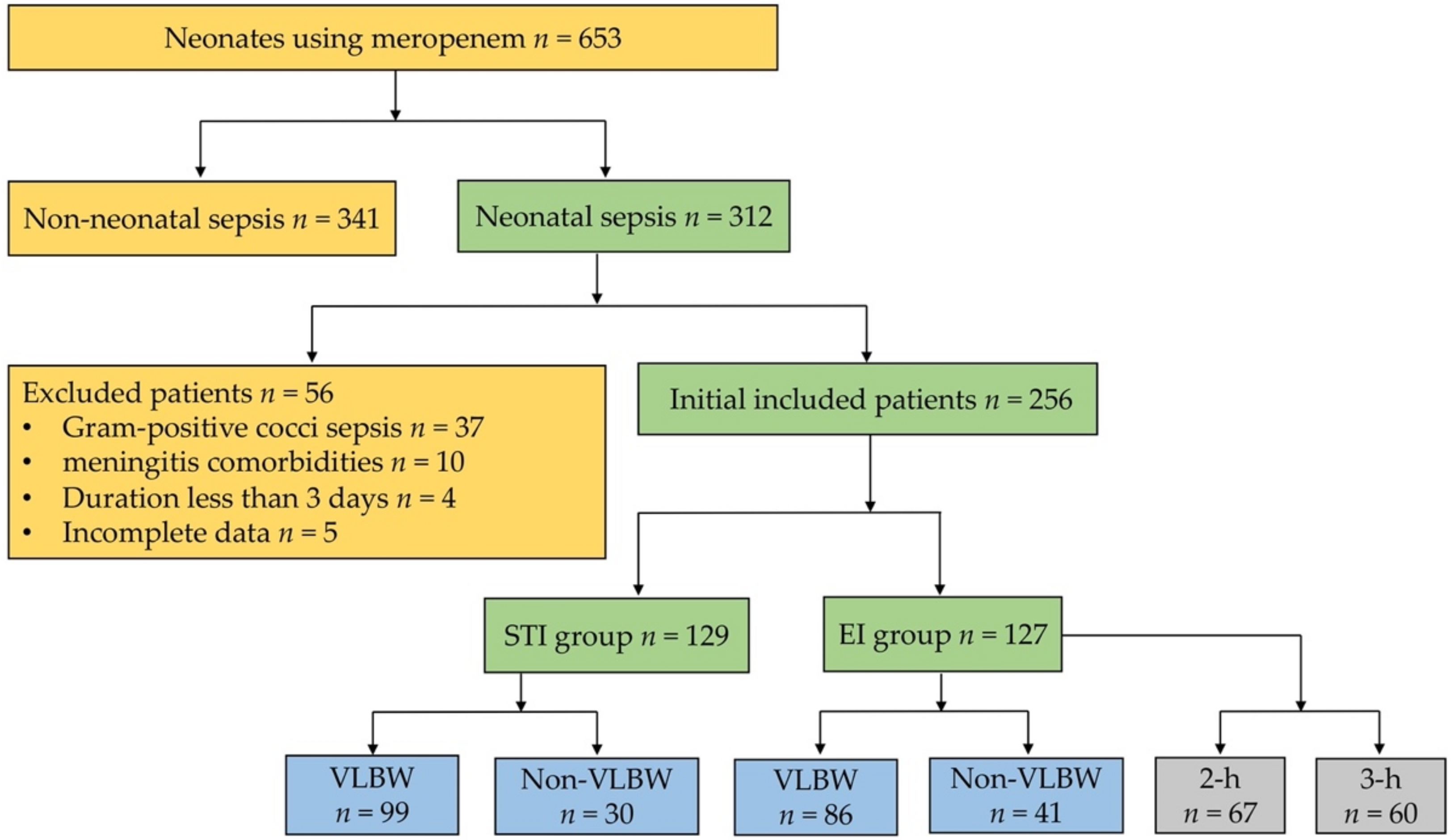
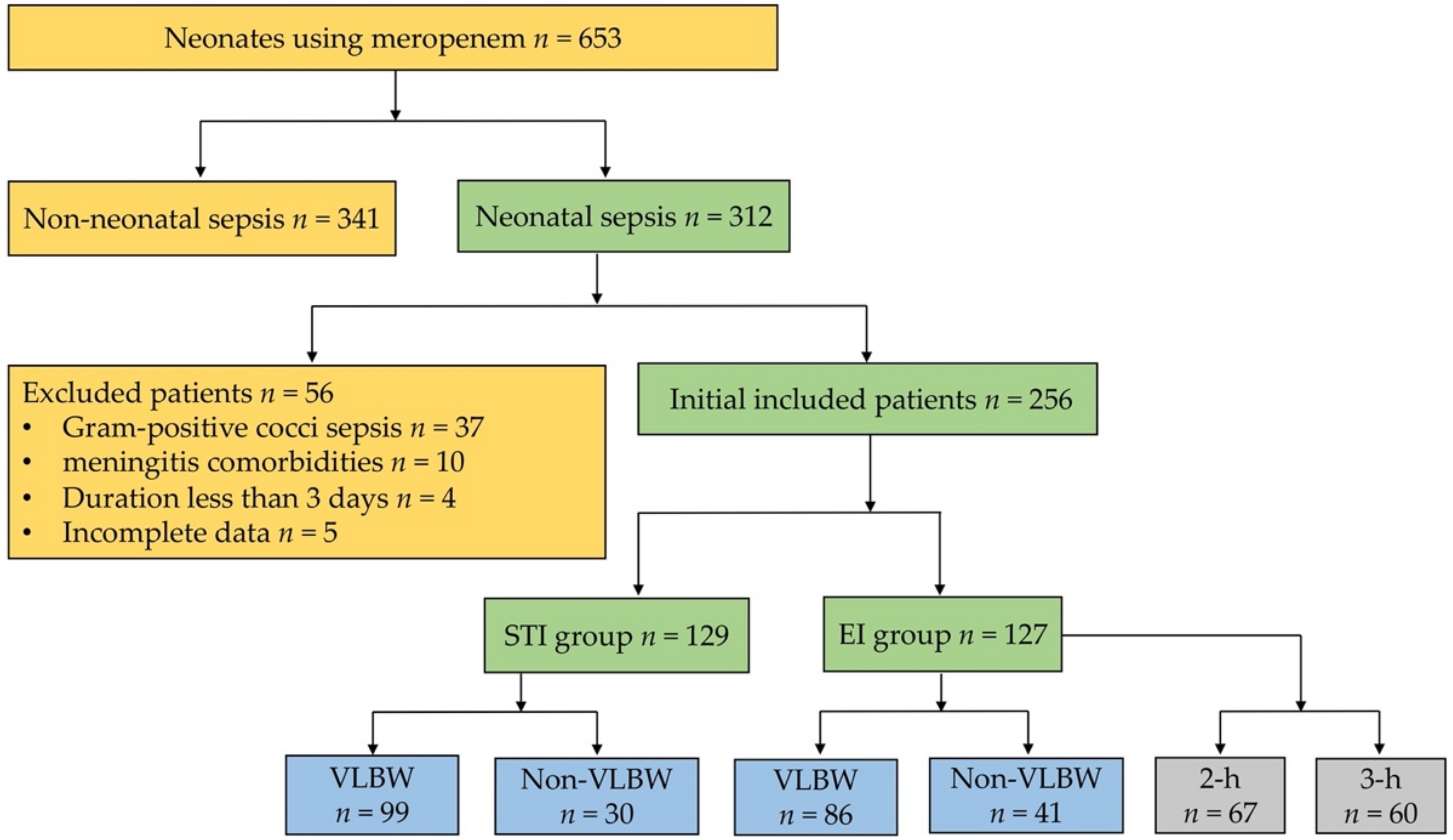
4.1. Study Sample
4.2. Exposure and Outcomes
4.3. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Popescu, C.R.; Cavanagh, M.M.M.; Tembo, B.; Chiume, M.; Lufesi, N.; Goldfarb, D.; Kissoon, N.; Lavoie, P. Neonatal sepsis in low-income countries: Epidemiology, diagnosis and prevention. Expert Rev. Anti-Infect. Ther. 2020, 18, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann-Struzek, C.; Goldfarb, D.; Schlattmann, P.; Schlapbach, L.J.; Reinhart, K.; Kissoon, N. The global burden of paediatric and neonatal sepsis: A systematic review. Lancet Respir. Med. 2018, 6, 223–230. [Google Scholar] [CrossRef]
- Glaser, M.A.; Hughes, L.M.; Jnah, A.; Newberry, D. Neonatal sepsis: A review of pathophysiology and current management strategies. Adv. Neonatal. Care 2021, 21, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Shane, A.L.; Sánchez, P.J.; Stoll, B.J. Neonatal sepsis. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef]
- Hartman, S.J.F.; Brüggemann, R.J.; Orriëns, L.; Dia, N.; Schreuder, M.; De Wildt, S.N. Pharmacokinetics and Target Attainment of Antibiotics in Critically Ill Children: A Systematic Review of Current Literature. Clin. Pharmacokinet. 2020, 59, 173–205. [Google Scholar] [CrossRef] [Green Version]
- Hassan, H.E.; Ivaturi, V.; Gobburu, J.; Green, T.P. Dosage Regimens for Meropenem in Children with Pseudomonas Infections Do Not Meet Serum Concentration Targets. Clin. Transl. Sci. 2019, 13, 301–308. [Google Scholar] [CrossRef]
- Shabaan, A.E.; Nour, I.; Elsayed Eldegla, H.; Nasef, N.; Shouman, B.; Abdel-Hady, H. Conventional versus prolonged infusion of meropenem in neonates with gram-negative late-onset sepsis: A randomized controlled trial. Pediatr. Infect Dis. J. 2017, 36, 358–363. [Google Scholar] [CrossRef]
- Yu, Z.; Pang, X.; Wu, X.; Shan, C.; Jiang, S. Clinical outcomes of prolonged infusion (extended infusion or continuous infusion) versus intermittent bolus of meropenem in severe infection: A meta-analysis. PLoS ONE 2018, 13, e0201667. [Google Scholar]
- Abdul-Aziz, M.H.; Sulaiman, H.; Nor, M.B.M.; Rai, V.; Wong, K.K.; Hasan, M.S.; Rahman, A.N.A.; Jamal, J.A.; Wallis, S.C.; Lipman, J.; et al. Beta-Lactam Infusion in Severe Sepsis (BLISS): A prospective, two-centre, open-labelled randomised controlled trial of continuous versus intermittent beta-lactam infusion in critically ill patients with severe sepsis. Intensiv. Care Med. 2016, 42, 1535–1545. [Google Scholar] [CrossRef]
- Lorente, L.; Lorenzo, L.; Martín, M.M.; Jiménez-Sosa, A.; Mora, M.L. Meropenem by Continuous Versus Intermittent Infusion in Ventilator-Associated Pneumonia due to Gram-Negative Bacilli. Ann. Pharmacother. 2006, 40, 219–223. [Google Scholar] [CrossRef]
- Zhou, P.; Zhang, Y.; Wang, Z.; Ying, Y.; Xing, Y.; Tong, X.; Zhai, S. Extended or Continuous Infusion of Carbapenems in Children with Severe Infections: A Systematic Review and Narrative Synthesis. Antibiotics 2021, 10, 1088. [Google Scholar] [CrossRef] [PubMed]
- McGovern, M.; Infection, I.O.B.O.T.; Giannoni, E.; Kuester, H.; Turner, M.A.; Hoogen, A.V.D.; Bliss, J.M.; Koenig, J.M.; Keij, F.M.; Mazela, J.; et al. Challenges in developing a consensus definition of neonatal sepsis. Pediatr. Res. 2020, 88, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Wynn, J.L. Defining neonatal sepsis. Curr. Opin. Pediatr. 2016, 28, 135–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tam, P.-Y.I.; Bendel, C. Diagnostics for neonatal sepsis: Current approaches and future directions. Pediatr. Res. 2017, 82, 574–583. [Google Scholar]
- Dong, Y.; Basmaci, R.; Titomanlio, L.; Sun, B.; Mercier, J.-C. Neonatal sepsis: Within and beyond China. Chin. Med. J. 2020, 133, 2219–2228. [Google Scholar] [CrossRef]
- Puopolo, K.M.; Benitz, W.E.; Zaoutis, T.E. Management of neonates born at ≤ 34 6/7 weeks’ gestation with suspected or proven early-onset bacterial sepsis. Pediatrics 2018, 142, e20182896. [Google Scholar] [CrossRef] [Green Version]
- Zakariya, B.P.; Bhat, B.V.; Harish, B.N.; Babu, T.A.; Joseph, N.M. Risk Factors and Predictors of Mortality in Culture Proven Neonatal Sepsis. Indian J. Pediatr. 2011, 79, 358–361. [Google Scholar] [CrossRef]
- Bhongade, S.D.; Meshram, R.M.; Gajimwar, V.S. Predictors of mortality in outborns with neonatal sepsis: A prospective observational study. Niger. Postgrad. Med. J. 2019, 26, 216–222. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Wiebe, R.; Dilay, L.; Thomson, K.; Rubinstein, E.; Hoban, D.J.; Noreddin, A.M.; Karlowsky, J.A. Comparative Review of the Carbapenems. Drugs 2007, 67, 1027–1052. [Google Scholar] [CrossRef]
- Heil, E.L.; Nicolau, D.P.; Farkas, A.; Roberts, J.A.; Thom, K.A. Pharmacodynamic Target Attainment for Cefepime, Meropenem, and Piperacillin-Tazobactam Using a Pharmacokinetic/Pharmacodynamic-Based Dosing Calculator in Critically Ill Patients. Antimicrob. Agents Chemother. 2018, 62, 62. [Google Scholar] [CrossRef] [Green Version]
- MacVane, S.H.; Kuti, J.L.; Nicolau, D.P. Prolonging β-lactam infusion: A review of the rationale and evidence, and guidance for implementation. Int. J. Antimicrob. Agents 2014, 43, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Pacifici, G.M.; Allegaert, K. Clinical pharmacology of carbapenems in neonates. J. Chemother. 2013, 26, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Viaene, E.; Chanteux, H.; Servais, H.; Mingeot-Leclercq, M.P.; Tulkens, P.M. Comparative stability studies of antipseudomonal beta-lactams for potential administration through portable elastomeric pumps (home therapy for cystic fibrosis patients) and motor-operated syringes (intensive care units). Antimicrob. Agents Chemother. 2002, 46, 2327–2332. [Google Scholar] [CrossRef] [Green Version]
- Nicolau, D.P. Carbapenems: A potent class of antibiotics. Expert Opin. Pharmacother. 2007, 9, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Costenaro, P.; Minotti, C.; Cuppini, E.; Barbieri, E.; Giaquinto, C.; Donà, D. Optimizing Antibiotic Treatment Strategies for Neonates and Children: Does Implementing Extended or Prolonged Infusion Provide any Advantage? Antibiotics 2020, 9, 329. [Google Scholar] [CrossRef]
- Germovsek, E.; Lutsar, I.; Kipper, K.; Karlsson, M.O.; Planche, T.; Chazallon, C.; Meyer, L.; Trafojer, U.M.T.; Metsvaht, T.; Fournier, I.; et al. Plasma and CSF pharmacokinetics of meropenem in neonates and young infants: Results from the Neo, Mero studies. J. Antimicrob. Chemother. 2018, 73, 1908–1916. [Google Scholar] [CrossRef] [Green Version]
- Padari, H.; Metsvaht, T.; Kõrgvee, L.-T.; Germovsek, E.; Ilmoja, M.-L.; Kipper, K.; Herodes, K.; Standing, J.F.; Oselin, K.; Lutsar, I. Short versus Long Infusion of Meropenem in Very-Low-Birth-Weight Neonates. Antimicrob. Agents Chemother. 2012, 56, 4760–4764. [Google Scholar] [CrossRef] [Green Version]
- Vesoulis, Z.A.; El Ters, N.M.; Wallendorf, M.; Mathur, A.M. Empirical estimation of the normative blood pressure in infants. J. Perinatol. 2016, 36, 291–295. [Google Scholar] [CrossRef] [Green Version]
- Batton, B.; Li, L.; Newman, N.S.; Das, A.; Watterberg, K.L.; Yoder, B.A.; Faix, R.G.; Laughon, M.M.; Stoll, B.J.; Higgins, R.D.; et al. Evolving blood pressure dynamics for extremely preterm infants. J. Perinatol. 2014, 34, 301–305. [Google Scholar] [CrossRef] [Green Version]
- Dionne, J.; Abitbol, C.L.; Flynn, J.T. Hypertension in infancy: Diagnosis, management and outcome. Pediatr. Nephrol. 2012, 27, 17–32. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | EI Group (n = 127) | STI Group (n = 129) | p-Values |
|---|---|---|---|
| Age (weeks), mean (SD) | 31.1 (3.49) | 30.5 (3.05) | 0.166 |
| Weight (grams), mean (SD) | 1460 (722) | 1340 (608) | 0.228 |
| Poor response | 110 (86.6%) | 103 (79.8%) | 0.147 |
| Antibiotics upgrade | 39 (30.7%) | 52 (40.3%) | 0.109 |
| CRT extension | 11 (8.7%) | 18 (14.0%) | 0.182 |
| Hypothermia | 23 (18.1%) | 15 (11.6%) | 0.145 |
| Apnea | 60 (47.2%) | 66 (51.2%) | 0.531 |
| Dyspnea | 67 (52.8%) | 71 (55.0%) | 0.714 |
| Abdominal distention | 39 (30.7%) | 31 (24.0%) | 0.231 |
| Vomiting | 4 (3.1%) | 5 (3.9%) | 1.000 |
| Heart rate increase | 45 (35.4%) | 43 (33.3%) | 0.724 |
| Hypotension | 7 (5.5%) | 10 (7.8%) | 0.472 |
| Cool extremities | 12 (9.4%) | 17 (13.2%) | 0.347 |
| Jaundice | 19 (15.0%) | 16 (12.4%) | 0.551 |
| Scleroderma | 6 (4.7%) | 4 (3.1%) | 0.728 |
| Pale or gray complexion | 60 (47.2%) | 51 (39.5%) | 0.213 |
| Convulsions | 0 (0%) | 3 (2.3%) | 0.251 |
| Outcomes | EI Group (n = 127) | STI Group (n = 129) | p-Values |
|---|---|---|---|
| 3-day clinical effectiveness rate | 104 (81.9%) | 77 (59.7%) | <0.001 |
| 3-day microbial clearance | 120 (94.5%) | 110 (85.3%) | 0.015 |
| 3-day CRP recovery rate | 30 (23.6%) | 21 (16.3%) | 0.141 |
| 3-day WBC recovery rate | 67 (52.8%) | 55 (42.6%) | 0.105 |
| Predictive Factors | Odds Ratio [95% CI] | p-Values | Odds Ratio [95% CI] | p-Values |
|---|---|---|---|---|
| Outcomes | 3-day clinical effectiveness rate | 3-day microbial clearance | ||
| Infusion time | 0.34 (0.18,0.62) | 0.001 | 4.13 (1.24, 13.78) | 0.021 |
| Age | 0.96 (0.82, 1.13) | 0.628 | 0.65 (0.47, 0.90) | 0.010 |
| Weight | 1.00 (1.00, 1.00) | 0.227 | 1.00 (1.00, 1.00) | 0.081 |
| Poor response | 0.47 (0.20, 1.13) | 0.092 | 2.29 (0.39, 13.49) | 0.361 |
| Antibiotics upgrade | 0.56 (0.29, 1.08) | 0.082 | 0.45 (0.13, 1.54) | 0.202 |
| CRT extension | 0.67 (0.20, 2.23) | 0.512 | 10.89 (1.50, 79.02) | 0.018 |
| Hypothermia | 1.36 (0.45, 4.09) | 0.585 | 1.14 (0.16, 8.08) | 0.894 |
| Apnea | 0.67 (0.36, 1.26) | 0.219 | 0.56 (0.18, 1.73) | 0.316 |
| Dyspnea | 0.69 (0.37, 1.29) | 0.243 | 0.62 (0.18, 2.11) | 0.447 |
| Abdominal distention | 2.06 (0.95, 4.46) | 0.069 | 1.85 (0.49, 6.96) | 0.361 |
| Vomiting | 0.42 (0.08, 2.27) | 0.315 | 10.24 (1.15, 91.56) | 0.037 |
| Heart rate increase | 0.67 (0.35, 1.29) | 0.233 | 1.43 (0.45, 4.59) | 0.543 |
| Hypotension | 4.75 (0.88, 25.62) | 0.070 | 5.79 (1.31, 25.58) | 0.020 |
| Cool extremities | 0.61 (0.21, 1.78) | 0.364 | 1.06 (0.16, 7.14) | 0.956 |
| Jaundice | 1.09 (0.42, 2.84) | 0.856 | 0.32 (0.05, 2.26) | 0.254 |
| Scleroderma | 0.28 (0.06, 1.25) | 0.094 | 40.15 (5.66, 284.83) | <0.001 |
| Pale or gray complexion | 1.30 (0.68, 2.49) | 0.424 | 0.87 (0.27, 2.8) | 0.812 |
| Convulsions | 0.24 (0.02, 3.59) | 0.300 | 0.68 (0.01, 35.67) | 0.846 |
| Outcomes | EI Group (n = 127) | STI Group (n = 129) | p-Values |
|---|---|---|---|
| 3-day BUN abnormality | 50 (39.4%) | 44 (34.1%) | 0.383 |
| 3-day creatinine abnormality | 49 (38.6%) | 39 (30.2%) | 0.160 |
| 3-day ALT abnormality | 44 (34.6%) | 42 (32.6%) | 0.724 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, G.; Zhou, P.; Zhang, H.; Sun, B.; Tong, X.; Xing, Y. Extended Infusion of Meropenem in Neonatal Sepsis: A Historical Cohort Study. Antibiotics 2022, 11, 341. https://doi.org/10.3390/antibiotics11030341
Cao G, Zhou P, Zhang H, Sun B, Tong X, Xing Y. Extended Infusion of Meropenem in Neonatal Sepsis: A Historical Cohort Study. Antibiotics. 2022; 11(3):341. https://doi.org/10.3390/antibiotics11030341
Chicago/Turabian StyleCao, Guangna, Pengxiang Zhou, Hua Zhang, Bangkai Sun, Xiaomei Tong, and Yan Xing. 2022. "Extended Infusion of Meropenem in Neonatal Sepsis: A Historical Cohort Study" Antibiotics 11, no. 3: 341. https://doi.org/10.3390/antibiotics11030341
APA StyleCao, G., Zhou, P., Zhang, H., Sun, B., Tong, X., & Xing, Y. (2022). Extended Infusion of Meropenem in Neonatal Sepsis: A Historical Cohort Study. Antibiotics, 11(3), 341. https://doi.org/10.3390/antibiotics11030341