
Surveillance of Antimicrobial Resistance in Hospital Wastewater: Identification of Carbapenemase-Producing Klebsiella spp.

 , , ,
, , ,
Abstract
1. Introduction
2. Results
2.1. KPC Isolates
2.2. Antimicrobial Susceptibility
2.3. Detection of Carbapenem-Resistance Genes
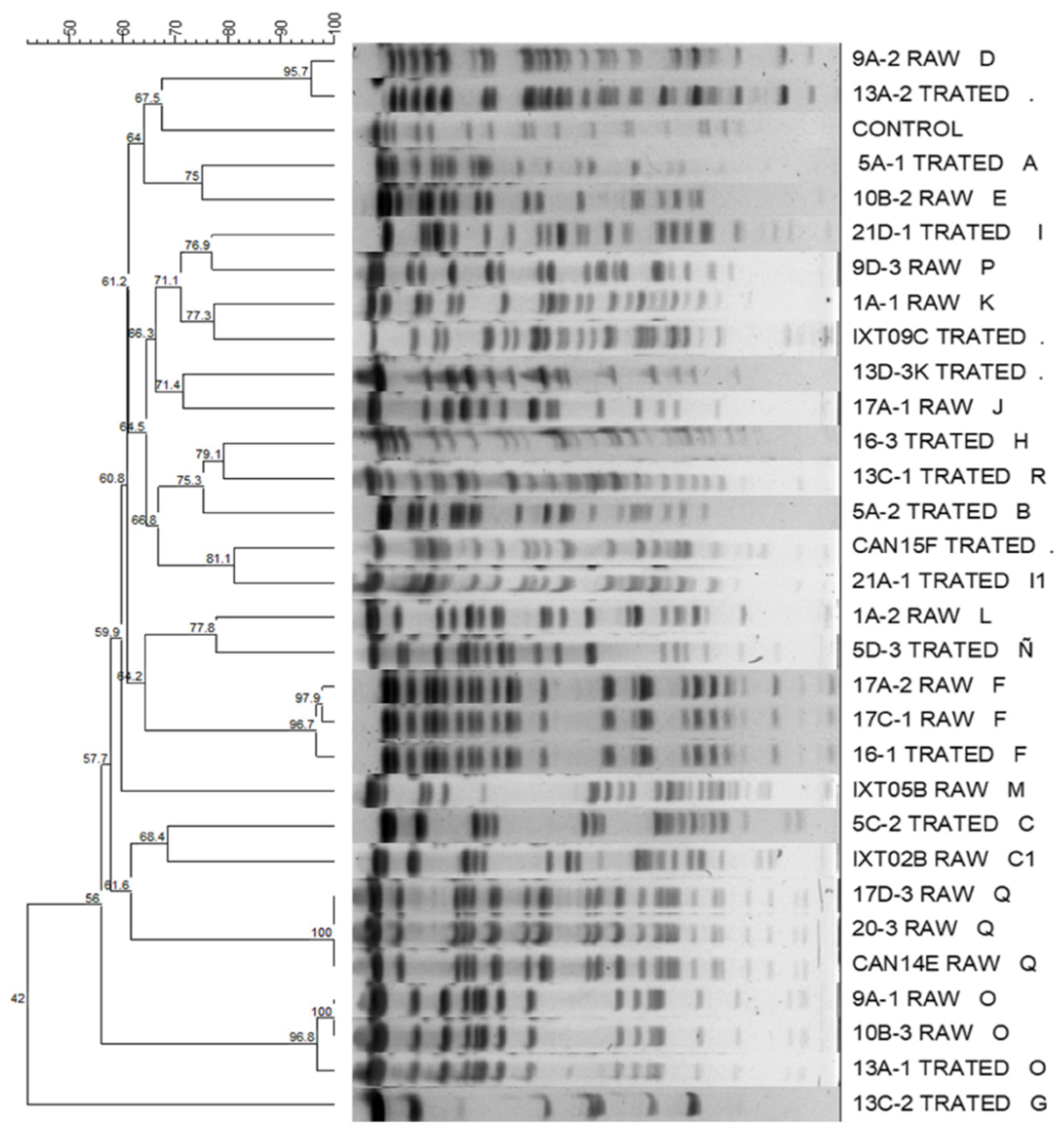
2.4. Molecular Typing of Pulsed-Field Gel Electrophoresis (PFGE)
3. Discussion
4. Materials and Methods
4.1. Study Sites and Sample Collection
4.2. Microbial Culturing and Identification
4.3. Antimicrobial Susceptibility Testing
4.4. Detection of Carbapenem-Resistance Genes
4.5. Molecular Typing of PFGE
4.6. Computer Fingerprint Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alpuche-Aranda, C.M. Infecciones emergentes el gran reto de la salud global: COVID-19. Salud Publica Mex. 2020, 62, 123. [Google Scholar] [CrossRef] [PubMed]
- McArthur, D.B. Emerging Infectious Diseases. Nurs. Clin. N. Am. 2019, 54, 297–311. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.E.; Patel, N.G.; Levy, M.A.; Storeygard, A.; Balk, D.; Gittleman, J.L.; Daszak, P. Global trends in emerging infectious diseases. Nature 2008, 451, 990–993. [Google Scholar] [CrossRef] [PubMed]
- Heymann, D.L.; Brilliant, L. Surveillance in eradication and elimination of infectious diseases: A progression through the years. Vaccine 2011, 29, D141–D144. [Google Scholar] [CrossRef] [PubMed]
- Gardy, J.L.; Loman, N.J. Towards a genomics-informed, real-time, global pathogen surveillance system. Nat. Rev. Genet. 2018, 19, 9–20. [Google Scholar] [CrossRef]
- Daughton, C.G. Wastewater surveillance for population-wide COVID-19: The present and future. Sci. Total Environ. 2020, 736, 139631. [Google Scholar] [CrossRef]
- La Rosa, G.; Iaconelli, M.; Mancini, P.; Bonanno Ferraro, G.; Veneri, C.; Bonadonna, L.; Lucentini, L.; Suffredini, E. First detection of SARS-CoV-2 in untreated wastewaters in Italy. Sci. Total Environ. 2020, 736, 139652. [Google Scholar] [CrossRef]
- Logan, L.K.; Weinstein, R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J. Infect. Dis. 2017, 215, S28–S36. [Google Scholar] [CrossRef]
- Bartsch, S.M.; McKinnell, J.A.; Mueller, L.E.; Miller, L.G.; Gohil, S.K.; Huang, S.S.; Lee, B.Y. Potential economic burden of carbapenem-resistant Enterobacteriaceae (CRE) in the United States. Clin. Microbiol. Infect. 2017, 23, 48.e9–48.e16. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention CRE Technical Information. Available online: https://www.cdc.gov/hai/organisms/cre/technical-info.html#Definition (accessed on 5 May 2020).
- Chea, N.; Bulens, S.N.; Kongphet-Tran, T.; Lynfield, R.; Shaw, K.M.; Vagnone, P.S.; Kainer, M.A.; Muleta, D.B.; Wilson, L.; Vaeth, E.; et al. Improved Phenotype-Based Definition for Identifying Carbapenemase Producers among Carbapenem-Resistant Enterobacteriaceae. Emerg. Infect. Dis. 2015, 21, 1611–1616. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. M100: Performance Standards for Antimicrobial Susceptibility Testing, 31st ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2021; ISBN 9781684400331. [Google Scholar]
- Bonardi, S.; Pitino, R. Carbapenemase-producing bacteria in food-producing animals, wildlife and environment: A challenge for human health. Ital. J. Food Saf. 2019, 8, 7956. [Google Scholar] [CrossRef] [PubMed]
- Köck, R.; Daniels-Haardt, I.; Becker, K.; Mellmann, A.; Friedrich, A.W.; Mevius, D.; Schwarz, S.; Jurke, A. Carbapenem-resistant Enterobacteriaceae in wildlife, food-producing, and companion animals: A systematic review. Clin. Microbiol. Infect. 2018, 24, 1241–1250. [Google Scholar] [CrossRef] [PubMed]
- Von Wintersdorff, C.J.H.; Penders, J.; Van Niekerk, J.M.; Mills, N.D.; Majumder, S.; Van Alphen, L.B.; Savelkoul, P.H.M.; Wolffs, P.F.G. Dissemination of antimicrobial resistance in microbial ecosystems through horizontal gene transfer. Front. Microbiol. 2016, 7, 173. [Google Scholar] [CrossRef] [PubMed]
- Vera-Leiva, A.; Barría-Loaiza, C.; Carrasco-Anabalón, S.; Lima, C.; Aguayo-Reyes, A.; Domínguez, M.; Bello-Toledo, H.; González-Rocha, G. KPC: Klebsiella pneumoniae carbapenemasa, principal carbapenemasa en enterobacterias. Rev. Chil. Infectol. 2017, 34, 476–484. [Google Scholar] [CrossRef]
- López, V.J.A.; Echeverri, T.L.M. K. pneumoniae: ¿la nueva “superbacteria”? Patogenicidad, epidemiología y mecanismos de resistencia. Iatreia 2010, 23, 157–165. [Google Scholar]
- Queenan, A.M.; Bush, K. Carbapenemases: The Versatile β-Lactamases. Clin. Microbiol. Rev. 2007, 20, 440–458. [Google Scholar] [CrossRef] [PubMed]
- Yigit, H.; Queenan, A.M.; Anderson, G.J.; Domenech-Sanchez, A.; Biddle, J.W.; Steward, C.D.; Alberti, S.; Bush, K.; Tenover, F.C. Novel carbapenem-hydrolyzing β-lactamase, KPC-1, from a carbapenem-resistant strain of Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2001, 45, 1151–1161. [Google Scholar] [CrossRef]
- Naas, T.; Nordmann, P.; Vedel, G.; Poyart, C. Plasmid-mediated carbapenem-hydrolyzing β-lactamase KPC in a Klebsiella pneumoniae isolate from France. Antimicrob. Agents Chemother. 2005, 49, 4423–4424. [Google Scholar] [CrossRef]
- Villegas, M.V.; Lolans, K.; Correa, A.; Suarez, C.J.; Lopez, J.A.; Vallejo, M.; Quinn, J.P. First detection of the plasmid-mediated class a carbapenemase KPC-2 in clinical isolates of Klebsiella pneumoniae from South America. Antimicrob. Agents Chemother. 2006, 50, 2880–2882. [Google Scholar] [CrossRef]
- de León Rosales, S.P. Plan Universitario de Control de la Resistencia Antimicrobiana; Universidad Nacional Autónoma de México: Mexico City, Mexico, 2018; Volume 53, ISBN 9788578110796. [Google Scholar]
- Garza-González, E.; Franco-Cendejas, R.; Morfín-Otero, R.; Echaniz-Aviles, G.; Rojas-Larios, F.; Bocanegra-Ibarias, P.; Flores-Treviño, S.; Ponce-De-León, A.; Rodríguez-Noriega, E.; Alavez-Ramírez, N.; et al. The Evolution of Antimicrobial Resistance in Mexico during the Last Decade: Results from the INVIFAR Group. Microb. Drug Resist. 2020, 26, 1372–1382. [Google Scholar] [CrossRef]
- Garza-González, E.; Bocanegra-Ibarias, P.; Bobadilla-del-Valle, M.; Alfredo Ponce-de-León-Garduño, L.; Esteban-Kenel, V.; Silva-Sánchez, J.; Garza-Ramos, U.; Barrios-Camacho, H.; López-Jácome, L.E.; Colin-Castro, C.A.; et al. Drug resistance phenotypes and genotypes in Mexico in representative gram-negative species: Results from the infivar network. PLoS ONE 2021, 16, e0248614. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Zulueta, P.; Silva-Sánchez, J.; Barrios, H.; Reyes-Mar, J.; Vélez-Pérez, F.; Arroyo-Escalante, S.; Ochoa-Carrera, L.; Delgado-Sapien, G.; Morales-Espinoza, M.D.R.; Tamayo-Legorreta, E.; et al. First Outbreak of KPC-3-Producing Klebsiella pneumoniae (ST258) Clinical Isolates in a Mexican Medical Center. Antimicrob. Agents Chemother. 2013, 57, 4086–4088. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Islam, M.A.; Islam, M.; Hasan, R.; Hossain, M.I.; Nabi, A.; Rahman, M.; Goessens, W.H.F.; Endtz, H.P.; Boehm, A.B.; Faruque, S.M. Environmental Spread of New Delhi Metallo-β-Lactamase-1-Producing Multidrug-Resistant Bacteria in Dhaka, Bangladesh. Appl. Environ. Microbiol. 2017, 83, e00793-17. [Google Scholar] [CrossRef] [PubMed]
- Moges, F.; Endris, M.; Belyhun, Y.; Worku, W. Isolation and characterization of multiple drug resistance bacterial pathogens from waste water in hospital and non-hospital environments, Northwest Ethiopia. BMC Res. Notes 2014, 7, 215. [Google Scholar] [CrossRef]
- Partridge, S.R.; Kwong, S.M.; Firth, N.; Jensen, S.O. Mobile Genetic Elements Associated with Antimicrobial Resistance. Clin. Microbiol. Rev. 2018, 31, e00088-17. [Google Scholar] [CrossRef]
- Berendonk, T.U.; Manaia, C.M.; Merlin, C.; Fatta-Kassinos, D.; Cytryn, E.; Walsh, F.; Bürgmann, H.; Sørum, H.; Norström, M.; Pons, M.-N.; et al. Tackling antibiotic resistance: The environmental framework. Nat. Rev. Microbiol. 2015, 13, 310–317. [Google Scholar] [CrossRef]
- World Health Organization (WHO); Food and Agricultura Organization of the United Nations (FAO); World Organisation or Animal Health (OIE). Technical Brief on Water, Sanitation, Hygiene and Wastewater Management to Prevent Infections and Reduce the Spread of Antimicrobial Resistance; WHO: Geneva, Switzerland, 2020; ISBN 9789240006416.
- Samanta, A.; Mahanti, A.; Chatterjee, S.; Joardar, S.N.; Bandyopadhyay, S.; Sar, T.K.; Mandal, G.P.; Dutta, T.K.; Samanta, I. Pig farm environment as a source of beta-lactamase or AmpC-producing Klebsiella pneumoniae and Escherichia coli. Ann. Microbiol. 2018, 68, 781–791. [Google Scholar] [CrossRef]
- Sharma, M.; Chetia, P.; Puzari, M.; Neog, N.; Borah, A. Menace to the ultimate antimicrobials among common Enterobacteriaceae clinical isolates in part of North-East India. bioRxiv 2019, 610923. [Google Scholar] [CrossRef]
- King, T.L.B.; Schmidt, S.; Essack, S.Y. Antibiotic resistant Klebsiella spp. from a hospital, hospital effluents and wastewater treatment plants in the uMgungundlovu District, KwaZulu-Natal, South Africa. Sci. Total Environ. 2020, 712, 135550. [Google Scholar] [CrossRef]
- Ebomah, K.E.; Okoh, A.I. Detection of carbapenem-resistance genes in Klebsiella species recovered from selected environmental niches in the Eastern Cape Province, South Africa. Antibiotics 2020, 9, 425. [Google Scholar] [CrossRef]
- Peneş, N.O.; Muntean, A.A.; Moisoiu, A.; Muntean, M.M.; Chirca, A.; Bogdan, M.A.; Popa, M.I. An overview of resistance profiles ESKAPE pathogens from 2010–2015 in a tertiary respiratory center in Romania. Rom. J. Morphol. Embryol. 2017, 58, 909–922. [Google Scholar] [PubMed]
- Abderrahim, A.; Djahmi, N.; Pujol, C.; Nedjai, S.; Bentakouk, M.C.; Kirane-Gacemi, D.; Dekhil, M.; Sotto, A.; Lavigne, J.P.; Pantel, A. First Case of NDM-1-Producing Klebsiella pneumoniae in Annaba University Hospital, Algeria. Microb. Drug Resist. 2017, 23, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Al-Agamy, M.H.; Aljallal, A.; Radwan, H.H.; Shibl, A.M. Characterization of carbapenemases, ESBLs, and plasmid-mediated quinolone determinants in carbapenem-insensitive Escherichia coli and Klebsiella pneumoniae in Riyadh hospitals. J. Infect. Public Health 2018, 11, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Perilli, M.; Bottoni, C.; Pontieri, E.; Segatore, B.; Celenza, G.; Setacci, D.; Bellio, P.; Strom, R.; Amicosante, G. Emergence of blaKPC-3-Tn4401a in Klebsiella pneumoniae ST512 in the municipal wastewater treatment plant and in the university hospital of a town in central Italy. J. Glob. Antimicrob. Resist. 2013, 1, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Obasi, A.; Nwachukwu, S.; Ugoji, E.; Kohler, C.; Göhler, A.; Balau, V.; Pfeifer, Y.; Steinmetz, I. Extended-Spectrum β-Lactamase-Producing Klebsiella pneumoniae from Pharmaceutical Wastewaters in South-Western Nigeria. Microb. Drug Resist. 2017, 23, 1013–1018. [Google Scholar] [CrossRef] [PubMed]
- Teban-Man, A.; Farkas, A.; Baricz, A.; Hegedus, A.; Szekeres, E.; Pârvu, M.; Coman, C. Wastewaters, with or without hospital contribution, harbour MDR, carbapenemase-producing, but not hypervirulent Klebsiella pneumoniae. Antibiotics 2021, 10, 361. [Google Scholar] [CrossRef]
- Guo, L.; An, J.; Ma, Y.; Ye, L.; Luo, Y.; Tao, C.; Yang, J. Nosocomial outbreak of oxa-48-producing Klebsiella pneumoniae in a Chinese hospital: Clonal transmission of st147 and st383. PLoS ONE 2016, 11, e0160754. [Google Scholar] [CrossRef]
- Cuzon, G.; Ouanich, J.; Gondret, R.; Naas, T.; Nordmann, P. Outbreak of OXA-48-positive carbapenem-resistant Klebsiella pneumoniae isolates in France. Antimicrob. Agents Chemother. 2011, 55, 2420–2423. [Google Scholar] [CrossRef]
- Nazik, H.; Ongen, B.; Ilktac, M.; Aydin, S.; Kuvat, N.; Sahin, A.; Yemisen, M.; Mete, B.; Durmus, M.S.; Balkan, I.I.; et al. Carbapenem resistance due to blaOXA-48 among ESBL-producing scherichia coli and Klebsiella pneumoniae isolates in a univesity hospital, Turkey. Southeast Asian J. Trop. Med. Public Health 2012, 43, 1178–1185. [Google Scholar]
- Shibl, A.; Al-Agamy, M.; Memish, Z.; Senok, A.; Khader, S.A.; Assiri, A. The emergence of OXA-48- and NDM-1-positive Klebsiella pneumoniae in Riyadh, Saudi Arabia. Int. J. Infect. Dis. 2013, 17, e1130–e1133. [Google Scholar] [CrossRef]
- Gibbon, M.J.; Couto, N.; David, S.; Barden, R.; Standerwick, R.; Jagadeesan, K.; Birkwood, H.; Dulyayangkul, P.; Avison, M.B.; Kannan, A.; et al. A high prevalence of blaOXA-48 in Klebsiella (Raoultella) ornithinolytica and related species in hospital wastewater in South West England. Microb. Genom. 2021, 7, 000509. [Google Scholar] [CrossRef]
- Sheppard, A.E.; Stoesser, N.; Wilson, D.J.; Sebra, R.; Kasarskis, A.; Anson, L.W.; Giess, A.; Pankhurst, L.J.; Vaughan, A.; Grim, C.J.; et al. Nested Russian doll-like genetic mobility drives rapid dissemination of the carbapenem resistance gene blaKPC. Antimicrob. Agents Chemother. 2016, 60, 3767–3778. [Google Scholar] [CrossRef] [PubMed]
- Stoesser, N.; Sheppard, A.E.; Peirano, G.; Anson, L.W.; Pankhurst, L.; Sebra, R.; Phan, H.T.T.; Kasarskis, A.; Mathers, A.J.; Peto, T.E.A.; et al. Genomic epidemiology of global Klebsiella pneumoniae carbapenemase (KPC)-producing Escherichia coli. Sci. Rep. 2017, 7, 5917. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, E.; Ribeiro, R.; Silva, C.J.C.; Alves, R.; Baptista, R.; Condinho, S.; Rosa, M.J.; Perdigão, J.; Caneiras, C.; Duarte, A. An update on wastewater multi-resistant bacteria: Identification of clinical pathogens such as Escherichia coli o25b:H4-b2-st131-producing ctx-m-15 esbl and kpc-3 carbapenemase-producing Klebsiella oxytoca. Microorganisms 2021, 9, 576. [Google Scholar] [CrossRef]
- de Oliveira, D.V.; Nunes, L.S.; Barth, A.L.; Van Der Sand, S.T. Genetic Background of β-Lactamases in Enterobacteriaceae Isolates from Environmental Samples. Microb. Ecol. 2017, 74, 599–607. [Google Scholar] [CrossRef]
- Daoud, Z.; Farah, J.; Sokhn, E.S.; El Kfoury, K.; Dahdouh, E.; Masri, K.; Afif, C.; Abdel-Massih, R.M.; Matar, G.M. Multidrug-Resistant Enterobacteriaceae in Lebanese Hospital Wastewater: Implication in the One Health Concept. Microb. Drug Resist. 2018, 24, 166–174. [Google Scholar] [CrossRef]
- Shahcheraghi, F.; Aslani, M.M.; Mahmoudi, H.; Karimitabar, Z.; Solgi, H.; Bahador, A.; Alikhani, M.Y. Molecular study of carbapenemase genes in clinical isolates of Enterobacteriaceae resistant to carbapenems and determining their clonal relationship using pulsed-field gel electrophoresis. J. Med. Microbiol. 2017, 66, 570–576. [Google Scholar] [CrossRef]
- Hashemizadeh, Z.; Hosseinzadeh, Z.; Azimzadeh, N.; Motamedifar, M. Dissemination pattern of multidrug resistant carbapenemase producing Klebsiella pneumoniae isolates using pulsed-field gel electrophoresis in southwestern Iran. Infect. Drug Resist. 2020, 13, 921–929. [Google Scholar] [CrossRef]
- Siddiqui, M.T.; Mondal, A.H.; Sultan, I.; Ali, A.; Haq, Q.M.R. Co-occurrence of ESBLs and silver resistance determinants among bacterial isolates inhabiting polluted stretch of river Yamuna, India. Int. J. Environ. Sci. Technol. 2019, 16, 5611–5622. [Google Scholar] [CrossRef]
- Siddiqui, M.T.; Mondal, A.H.; Gogry, F.A.; Husain, F.M.; Alsalme, A.; Haq, Q.M.R. Plasmid-mediated ampicillin, quinolone, and heavy metal co-resistance among esbl-producing isolates from the Yamuna River, New Delhi, India. Antibiotics 2020, 9, 826. [Google Scholar] [CrossRef]
- Gogry, F.A.; Siddiqui, M.T.; Haq, Q.M.R. Emergence of mcr-1 conferred colistin resistance among bacterial isolates from urban sewage water in India. Environ. Sci. Pollut. Res. 2019, 26, 33715–33717. [Google Scholar] [CrossRef] [PubMed]
- Aarestrup, F.M.; Woolhouse, M.E.J. Using sewage for surveillance of antimicrobial resistance. Science 2020, 367, 630–632. [Google Scholar] [CrossRef] [PubMed]
- Dogonchi, A.A.; Ghaemi, E.A.; Ardebili, A.; Yazdansetad, S.; Pournajaf, A. Metallo-β-lactamase-mediated resistance among clinical carbapenem-resistant Pseudomonas aeruginosa isolates in northern Iran: A potential threat to clinical therapeutics. Tzu Chi Med. J. 2018, 30, 90–96. [Google Scholar] [CrossRef]
- Aubron, C.; Poirel, L.; Ash, R.J.; Nordmann, P. Carbapenemase-producing Enterobacteriaceae, U.S. rivers. Emerg. Infect. Dis. 2005, 11, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Bradford, P.A.; Bratu, S.; Urban, C.; Visalli, M.; Mariano, N.; Landman, D.; Rahal, J.J.; Brooks, S.; Cebular, S.; Quale, J. Emergence of carbapenem-resistant Klebsiella species possessing the class A carbapenem-hydrolyzing KPC-2 and inhibitor-resistant TEM-30 β-lactamases in New York City. Clin. Infect. Dis. 2004, 39, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Poirel, L.; Héritier, C.; Tolün, V.; Nordmann, P. Emergence of Oxacillinase-Mediated Resistance to Imipenem in Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2004, 48, 15–22. [Google Scholar] [CrossRef]
- Han, H.; Zhou, H.; Li, H.; Gao, Y.; Lu, Z.; Hu, K.; Xu, B. Optimization of pulse-field gel electrophoresis for subtyping of Klebsiella pneumoniae. Int. J. Environ. Res. Public Health 2013, 10, 2720–2731. [Google Scholar] [CrossRef]
- Tenover, F.C.; Arbeit, R.D.; Goering, R.V.; Mickelsen, P.A.; Murray, B.E.; Persing, D.H.; Swaminathan, B. Interpreting chromosomal DNA restriction patterns produced by pulsed- field gel electrophoresis: Criteria for bacterial strain typing. J. Clin. Microbiol. 1995, 33, 2233–2239. [Google Scholar] [CrossRef]


{kind=link}
| Hospital | Sample Site | Code | Isolated | Genes | AMP | TZP | FOX | CAZ | CTX | CEF | DOR | ERT | IPM | MEM | AMK | GEN | CIP | TIG |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HRAEI | Raw Wastewater | 1A-1 | K. pneumoniae | 16 | <4 | <4 | 4 | 16 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | 1 | <0.025 | <0.5 | |
| 1A-2 | K. pneumoniae | 4 | <4 | <4 | <1 | <1 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | 1 | <0.025 | <0.5 | |||
| IXT02B | K. pneumoniae | blaKPC, blaOXA | >32 | >128 | 16 | >64 | 16 | 2 | >8 | >8 | 8 | >16 | 2 | 1 | 1 | <0.5 | ||
| IXT05B | K. oxytoca | 4 | <4 | <4 | <1 | <1 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | 1 | <0.025 | <0.5 | |||
| Treated Wastewater | 5A-1 | K. pneumoniae | blaKPC | >32 | >128 | 16 | >64 | >64 | >64 | >8 | >8 | >16 | >16 | <2 | >16 | 2 | 2 | |
| 5A-2 | K. pneumoniae | >32 | 8 | <4 | 4 | >64 | 2 | <0.12 | <0.5 | <0.25 | <0.25 | 4 | <1 | 2 | 2 | |||
| 5C-2 | K. pneumoniae | blaKPC | >32 | >128 | 16 | 64 | 16 | 2 | >8 | >8 | 8 | >16 | 2 | 1 | 2 | <0.5 | ||
| 5D-3 | K. pneumoniae | >32 | >128 | >64 | >64 | >64 | >64 | >8 | >8 | >16 | >16 | >64 | 16 | >4 | <0.5 | |||
| IXT09C | K. oxytoca | >32 | >128 | >64 | >64 | >64 | >64 | >8 | >8 | >16 | >16 | 16 | 1 | 1 | <0.5 | |||
| INCAN | Raw Wastewater | 9A-1 | K. pneumoniae | 4 | <4 | <4 | <1 | <1 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | 1 | <0.025 | 1 | |
| 9A-2 | K. pneumoniae | blaKPC | >32 | >128 | 16 | 64 | 16 | 2 | >8 | >8 | 8 | >16 | >64 | 8 | 1 | 1 | ||
| 9D-3 | K. pneumoniae | 4 | <4 | <4 | <1 | <1 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | 1 | <0.025 | 1 | |||
| 10B-2 | K. pneumoniae | 2 | <4 | <4 | <1 | <1 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | 1 | <0.025 | 1 | |||
| 10B-3 | K. pneumoniae | 4 | <4 | <4 | <1 | <1 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | <1 | <0.025 | 1 | |||
| 17A-1 | K. pneumoniae | 4 | <4 | <4 | <1 | <1 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | 1 | <0.025 | <0.5 | |||
| 17A-2 | K. pneumoniae | blaKPC | >32 | >128 | 8 | >64 | 16 | 2 | >8 | >8 | >16 | >16 | 2 | 1 | 1 | <0.5 | ||
| 17C-1 | K. pneumoniae | blaKPC | >32 | >128 | 4 | >64 | 8 | 2 | >8 | >8 | >16 | >16 | 2 | 1 | 1 | <0.5 | ||
| 17D-3 | K. pneumoniae | 4 | <4 | <4 | <1 | <1 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | 1 | <0.025 | <0.5 | |||
| 20-Mar | K. pneumoniae | 4 | <4 | <4 | <1 | <1 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | 1 | <0.025 | <0.5 | |||
| CAN14E | K. pneumoniae | 4 | <4 | <4 | <1 | <1 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | 1 | <0.025 | <0.5 | |||
| Treated Wastewater | 13A-1 | K. pneumoniae | 4 | <4 | <4 | <1 | <1 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | <1 | <0.025 | 1 | ||
| 13A-2 | K. pneumoniae | blaKPC | >32 | >128 | 16 | >64 | 16 | 2 | >8 | >8 | >16 | >16 | >64 | 8 | 0.5 | 1 | ||
| 13C-1 | K. oxytoca | blaKPC | >32 | >128 | 4 | >64 | 16 | 2 | >8 | >8 | >16 | >16 | 2 | 1 | >4 | <0.5 | ||
| 13C-2 | K. pneumoniae | blaKPC | >32 | >128 | >64 | >64 | 32 | 8 | >8 | >8 | 8 | >16 | <2 | 8 | 1 | 1 | ||
| 16-ene | K. pneumoniae | blaKPC | >32 | >128 | 8 | >64 | >64 | 2 | >8 | >8 | 8 | >16 | 2 | 1 | 1 | <0.5 | ||
| 16-Mar | K. oxytoca | blaKPC | >32 | >128 | >64 | >64 | >64 | 32 | >8 | >8 | >16 | >16 | 8 | 1 | 2 | 2 | ||
| 21A-1 | K. pneumoniae | blaKPC | >32 | >128 | 8 | >64 | 8 | 2 | >8 | 4 | 8 | >16 | 2 | 8 | 2 | 1 | ||
| 21D-1 | K. pneumoniae | blaKPC | >32 | >128 | 8 | >64 | 16 | 2 | >8 | >8 | >16 | >16 | 2 | >16 | >4 | 1 | ||
| CAN15F | K. pneumoniae | blaKPC | >32 | >128 | 8 | 64 | 8 | 2 | >8 | 4 | 8 | >16 | <2 | >16 | >4 | 1 | ||
| 13D-3-k | K. pneumoniae | 4 | <4 | <4 | <1 | <1 | <1 | <0.12 | <0.5 | <0.25 | <0.25 | <2 | 1 | <0.025 | 1 |
| Target Gene | Primer Sequence (5’-3’) | Amplicon Size (bp) | PCR Cycling Condition | References |
|---|---|---|---|---|
| blaNDM-1 | F: GGTTTGGCGATCTGGTTTTC R: GGAATGGCTCATCACGATC | 621 | Initial denaturation 10 min at 94 °C. Denaturation at 94 °C for 30 s, annealing at 52 °C for 40 s, extension at 72 °C for 50 s, by 36 cycles, and final extension at 72 °C for 10 min. | Dogonchi AA, et al. [57] |
| blaIMP | F: ATAGCCATCCTTGTTTAGCTC R: TCTGCGATTACTTTATCCTC | 818 | Initial denaturation 10 min at 94 °C. Denaturation at 94 °C for 30 s, annealing at 58 °C for 30 s, extension at 72 °C for 1 min by 30 cycles, and final extension at 72 °C for 10 min. | Aubron, CL, et al. [58] |
| blaKPC | F: ATGTCACTGTATCGCCGTCT R: TTTTCAGAGCCTTACTGCCC | 893 | Initial denaturation 15 min at 95 °C. Denaturation at 94 °C for 1 min, annealing at 62 °C for 1 min, extension at 72 °C for 1 min by 38 cycles, and final extension at 72 °C for 10 min. | Bradford, PA, et al. [59] |
| blaOXA-48-like | F: TTGGTGGCATCGATTATCGG R: GAGCACTTCTTTTGTGATGGC | 744 | Initial denaturation 5 min at 94 °C. Denaturation at 94 °C for 1 min, annealing at 60 °C for 1 min, extension at 72 °C for 1 min by 30 cycles, and final extension at 72 °C for 10 min. | Poirel, LC, et al. [60] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galarde-López, M.; Velazquez-Meza, M.E.; Bobadilla-del-Valle, M.; Carrillo-Quiroz, B.A.; Cornejo-Juárez, P.; Ponce-de-León, A.; Sassoé-González, A.; Alpuche-Aranda, C.M. Surveillance of Antimicrobial Resistance in Hospital Wastewater: Identification of Carbapenemase-Producing Klebsiella spp. Antibiotics 2022, 11, 288. https://doi.org/10.3390/antibiotics11030288
Galarde-López M, Velazquez-Meza ME, Bobadilla-del-Valle M, Carrillo-Quiroz BA, Cornejo-Juárez P, Ponce-de-León A, Sassoé-González A, Alpuche-Aranda CM. Surveillance of Antimicrobial Resistance in Hospital Wastewater: Identification of Carbapenemase-Producing Klebsiella spp. Antibiotics. 2022; 11(3):288. https://doi.org/10.3390/antibiotics11030288
Chicago/Turabian StyleGalarde-López, Miguel, Maria Elena Velazquez-Meza, Miriam Bobadilla-del-Valle, Berta Alicia Carrillo-Quiroz, Patricia Cornejo-Juárez, Alfredo Ponce-de-León, Alejandro Sassoé-González, and Celia Mercedes Alpuche-Aranda. 2022. "Surveillance of Antimicrobial Resistance in Hospital Wastewater: Identification of Carbapenemase-Producing Klebsiella spp." Antibiotics 11, no. 3: 288. https://doi.org/10.3390/antibiotics11030288
APA StyleGalarde-López, M., Velazquez-Meza, M. E., Bobadilla-del-Valle, M., Carrillo-Quiroz, B. A., Cornejo-Juárez, P., Ponce-de-León, A., Sassoé-González, A., & Alpuche-Aranda, C. M. (2022). Surveillance of Antimicrobial Resistance in Hospital Wastewater: Identification of Carbapenemase-Producing Klebsiella spp. Antibiotics, 11(3), 288. https://doi.org/10.3390/antibiotics11030288